Acoustic Sensing and Ultrasonic Drug Delivery in Multimodal Theranostic Capsule Endoscopy

 ,
,
Abstract
:1. Introduction
2. Capsule Endoscopy
2.1. Video Capsule Endoscopy for Diagnosis
2.2. Therapeutic Capsule Endoscopy
2.3. Ultrasound Capsule Endoscopy
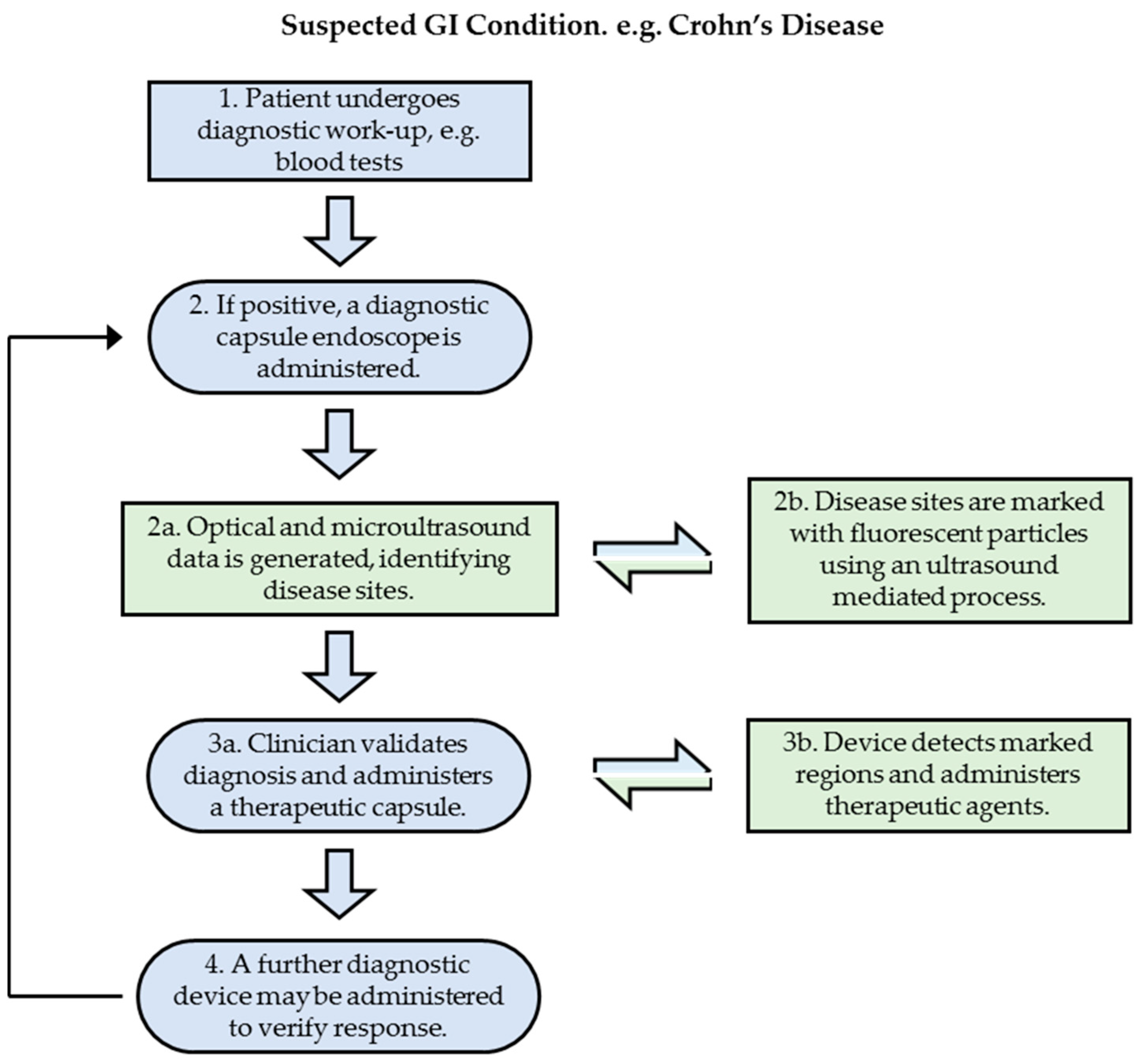
3. Proposed Theranostic Patient Pathway
4. Results
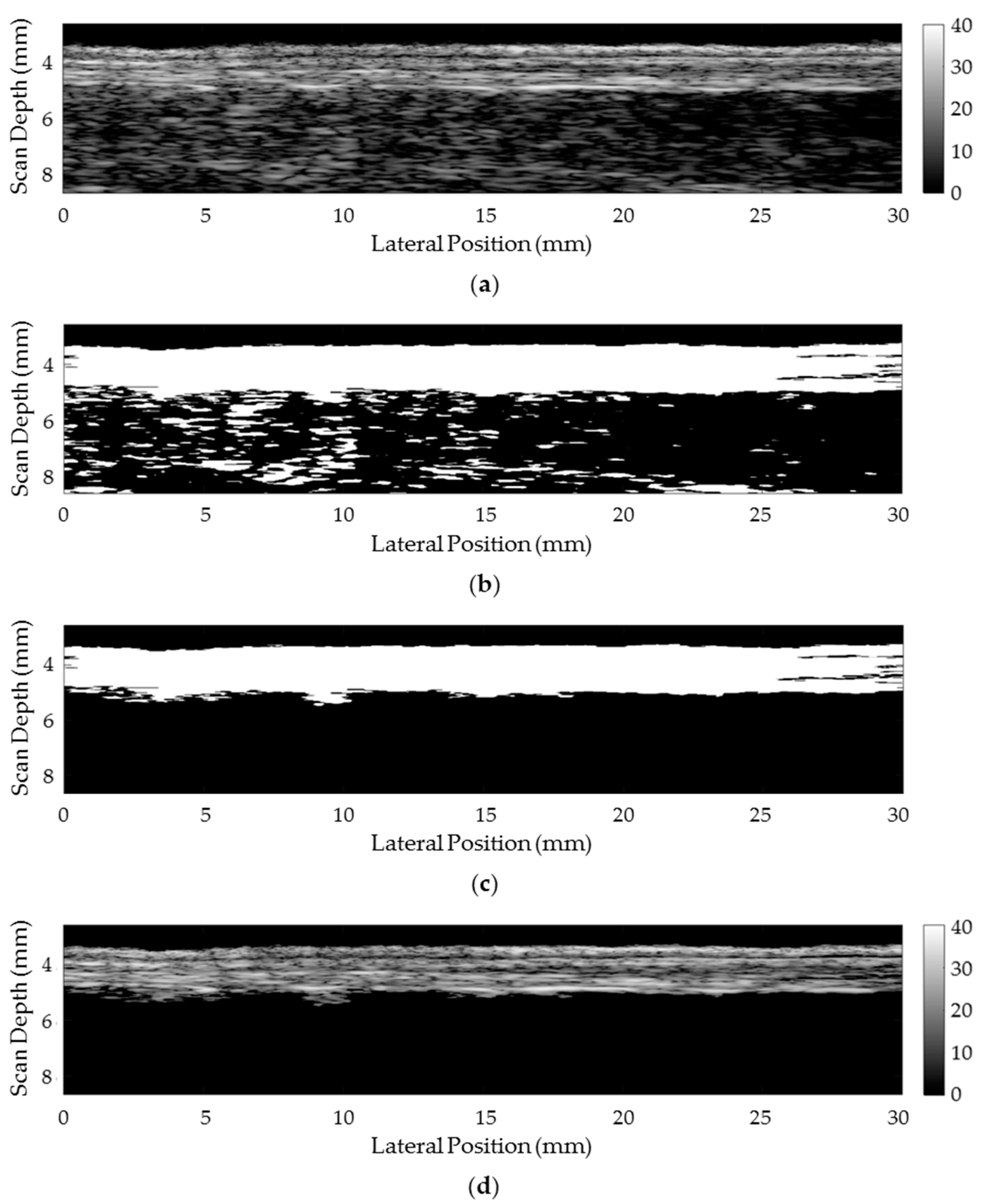
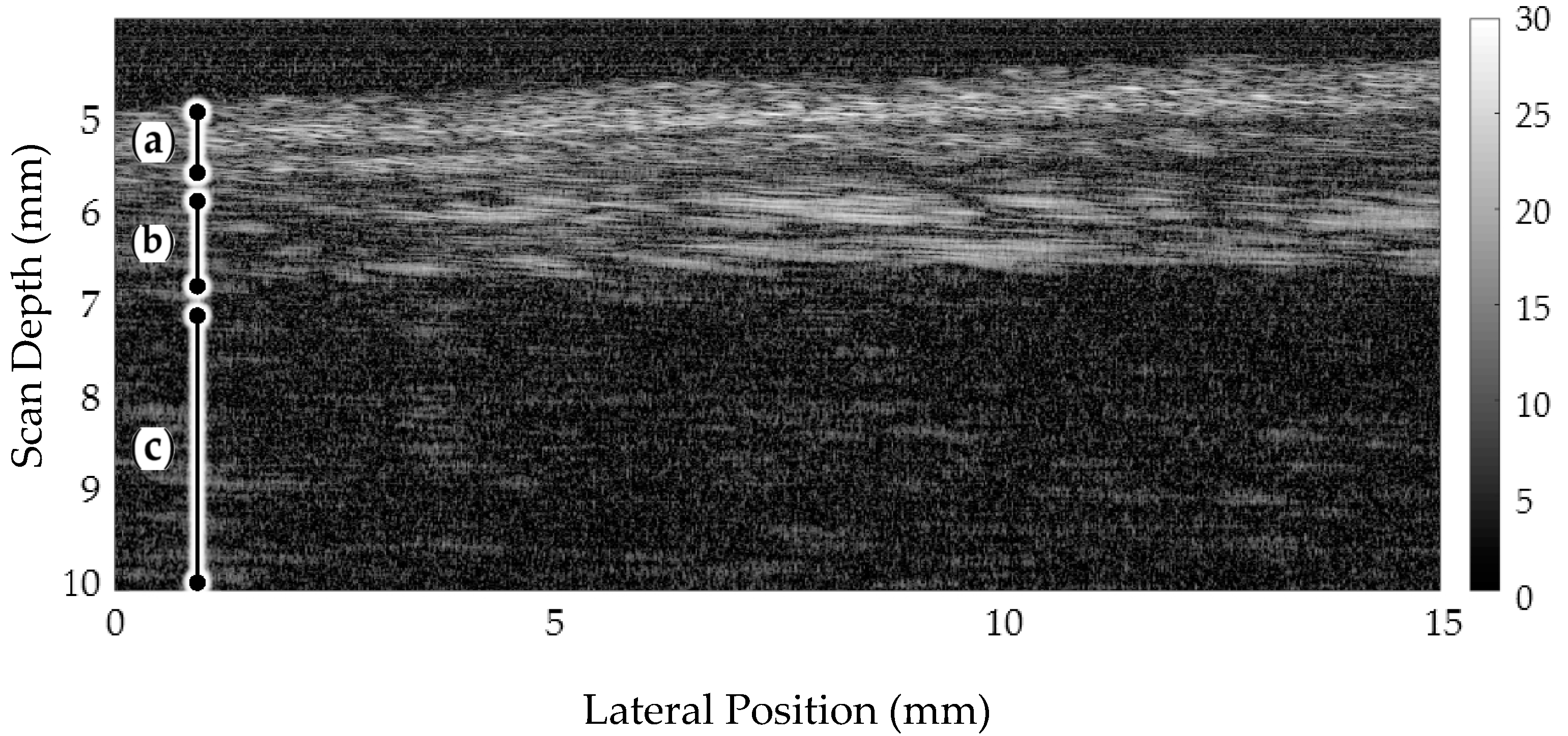
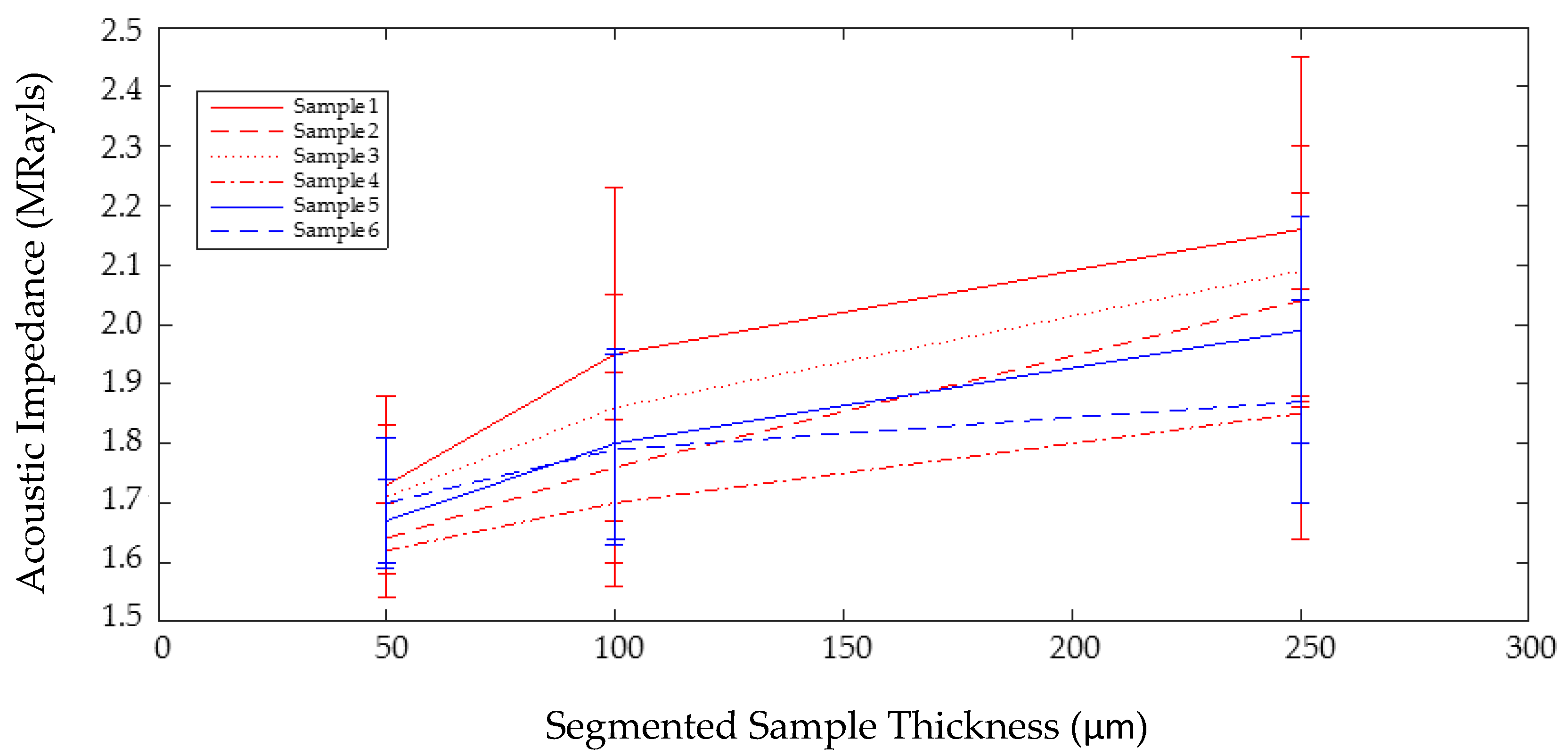
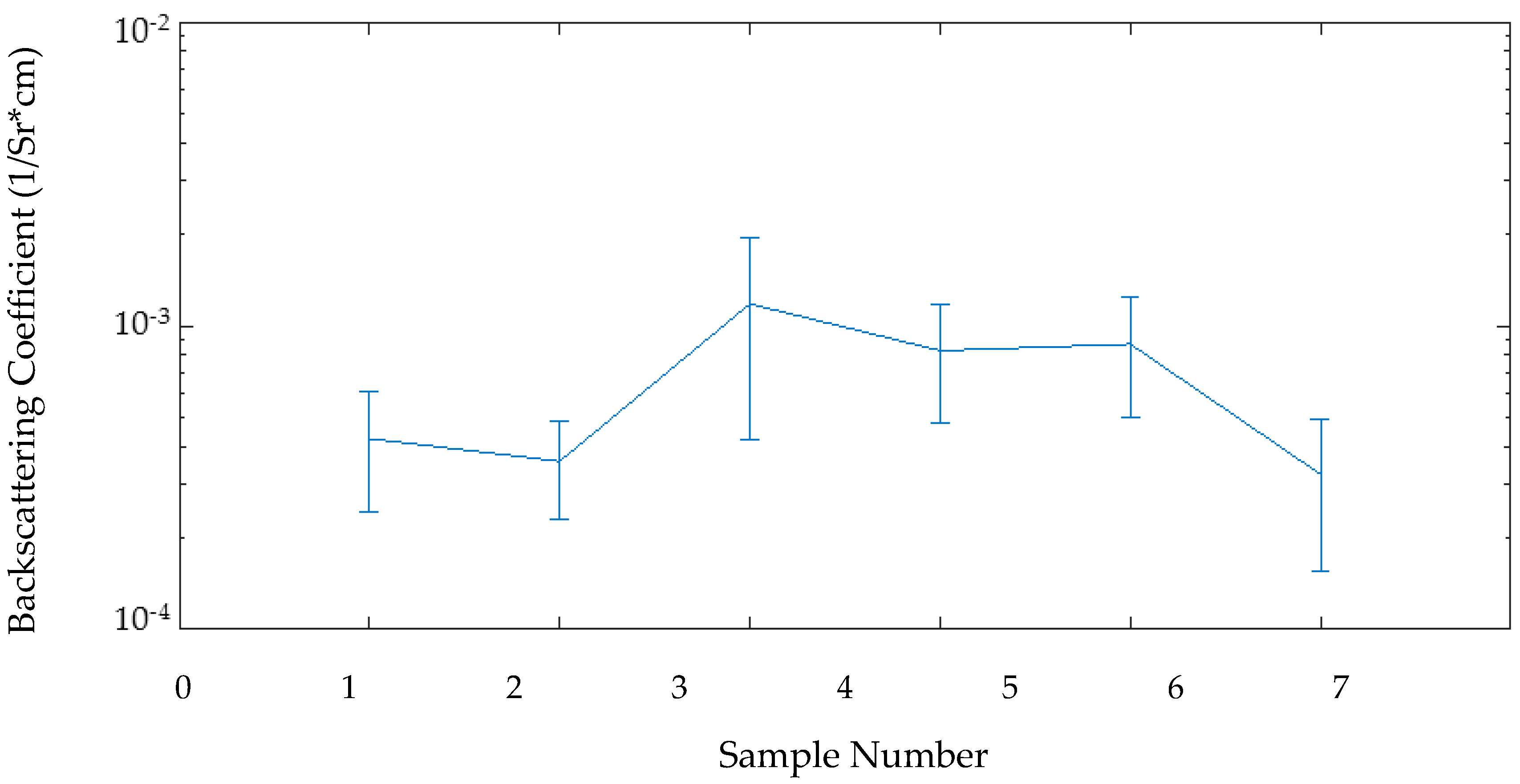
4.1. Microultrasound Diagnosis and Quantitative Analysis
4.1.1. Tissue Characterization Techniques
4.1.2. Experimental Tissue Preparation
4.1.3. Results
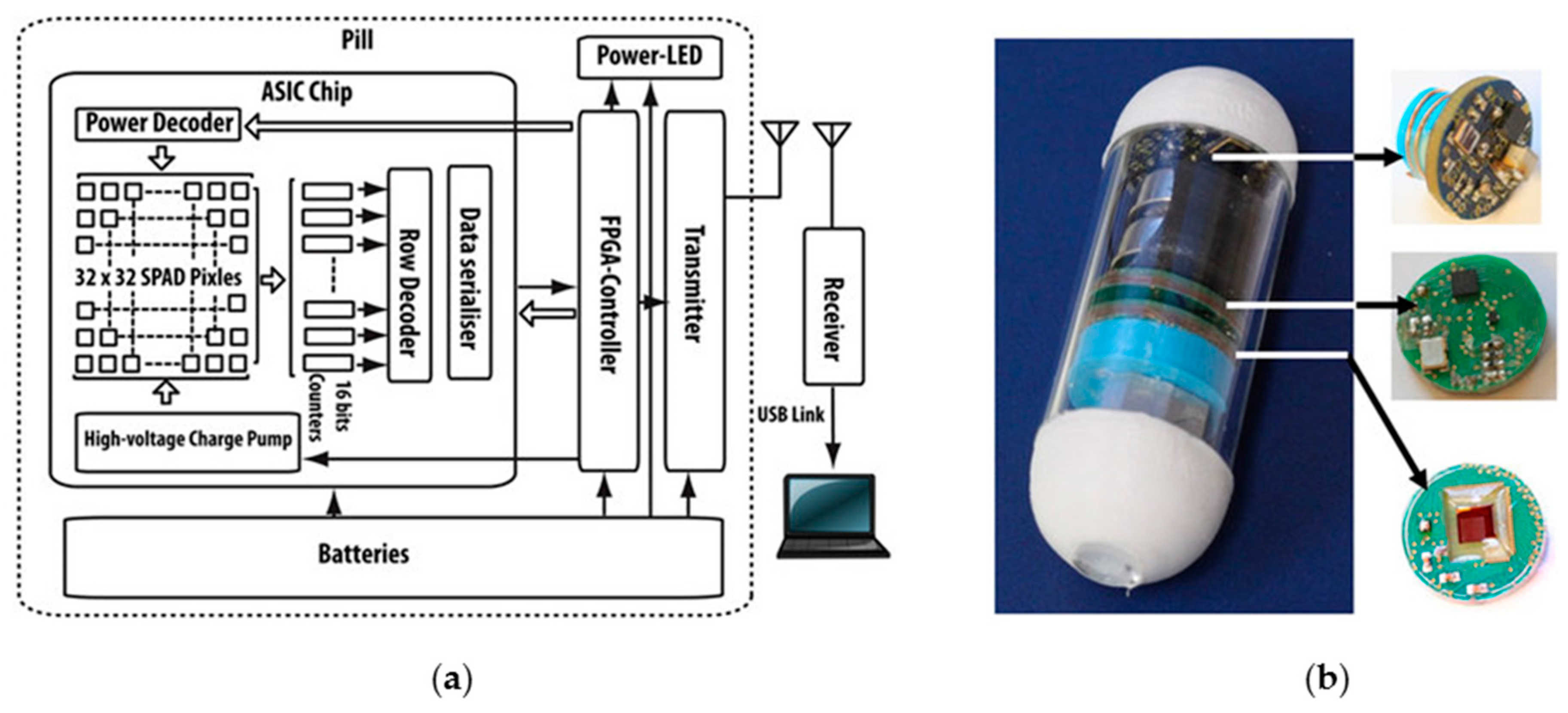
4.2. Fluorescent Nanoparticle Marking and Imaging
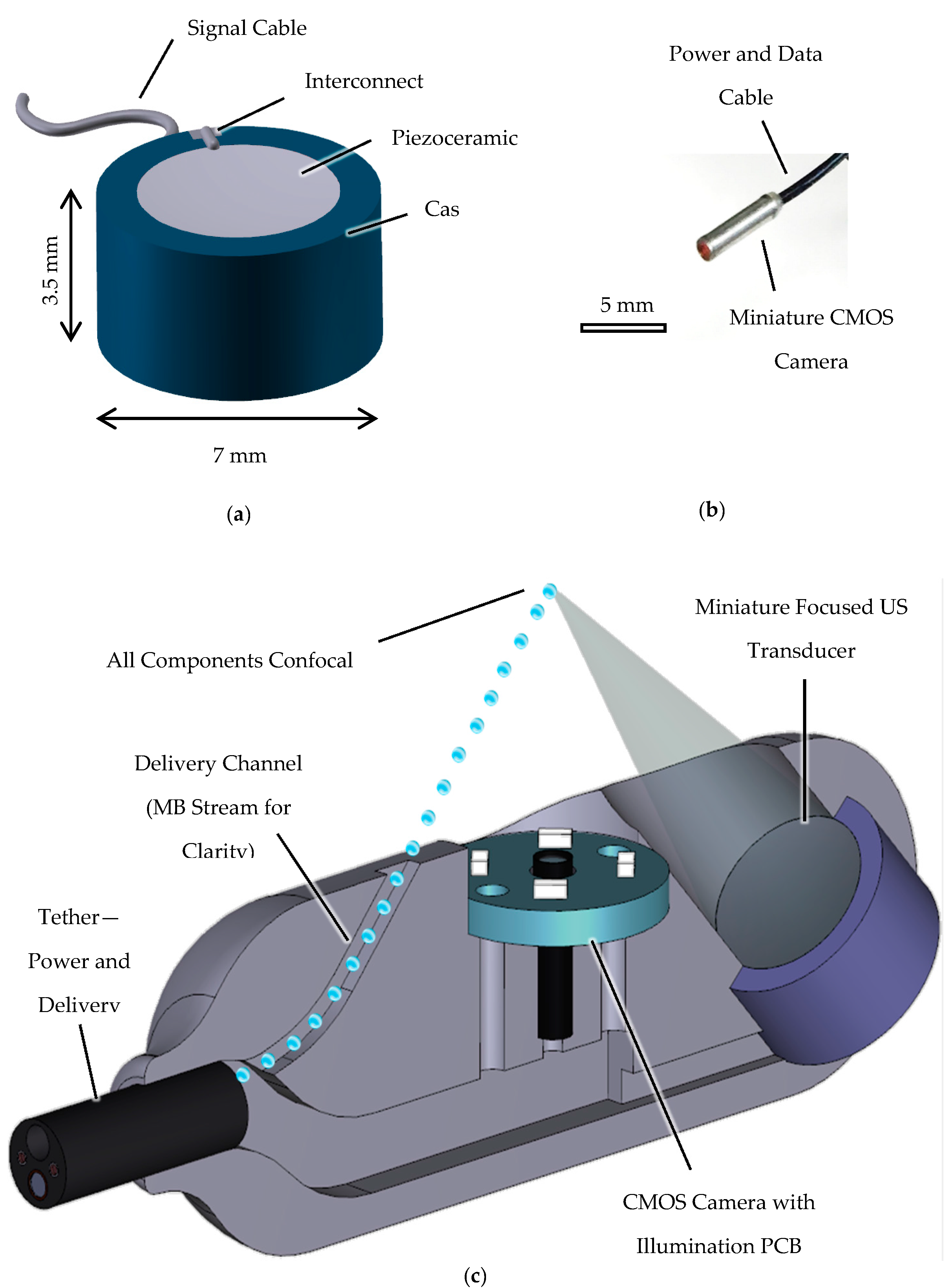
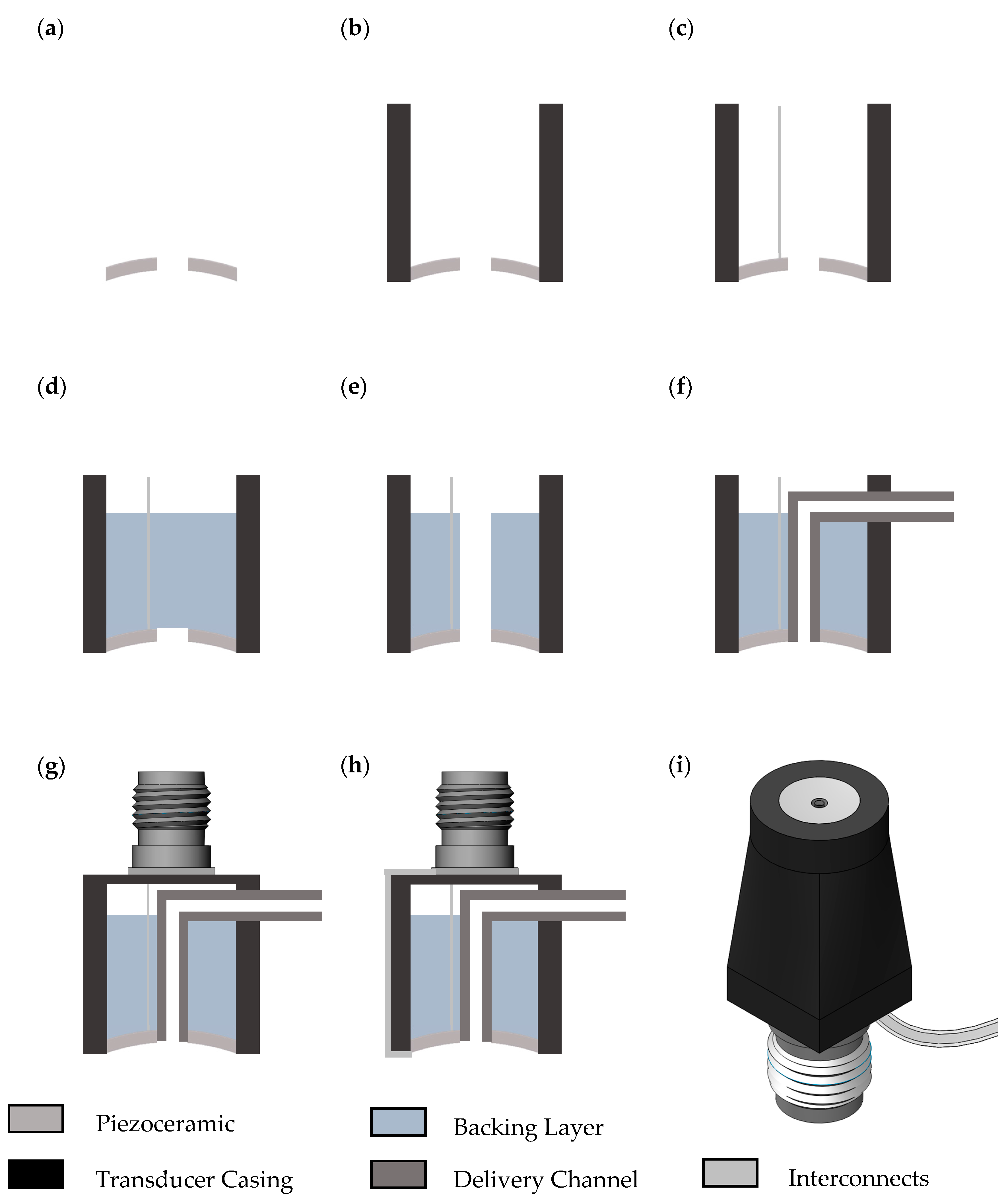
4.3. Feasibility of Therapeutic Capsule Endoscopy
Capsule Fabrication and Functional Testing
4.4. Ultrasound-Mediated Targeted Drug Delivery
4.4.1. Epithelial Cell Model of the Small Intestine
4.4.2. Transducers for Insonation
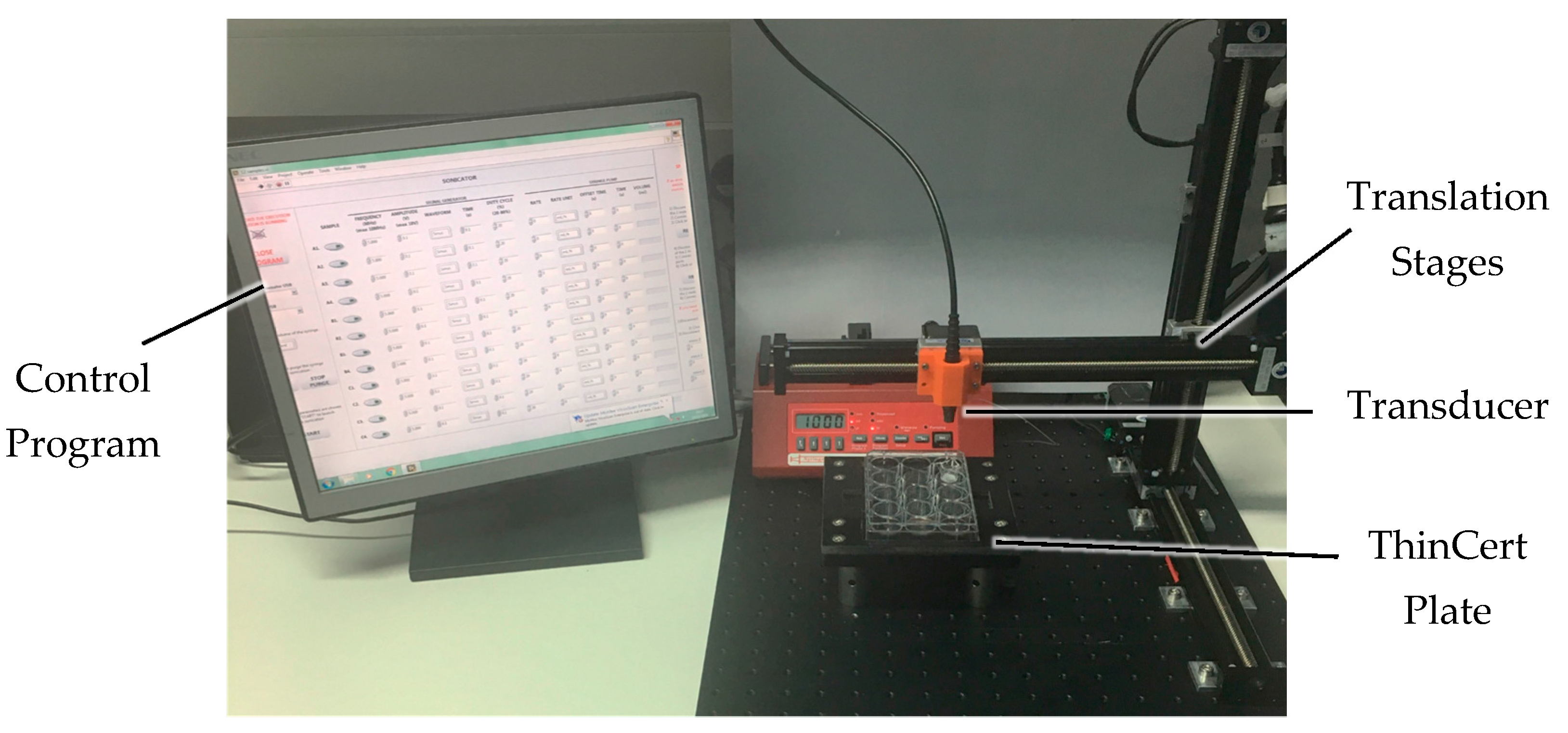
4.4.3. Fully Automated Insonation System
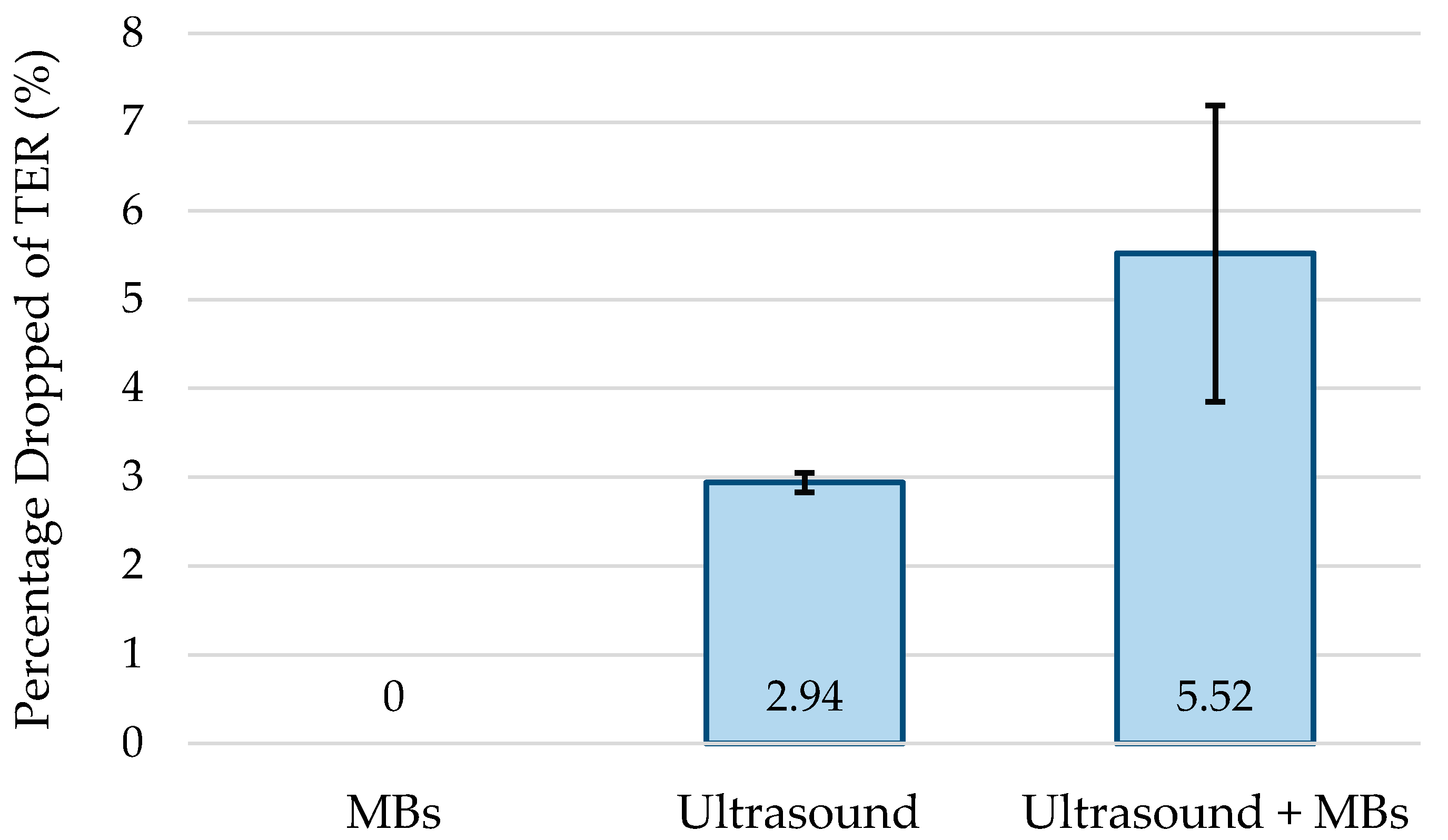
4.4.4. Barrier Function Measurements during Insonation
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Kaplan, G.G. The global burden of ibd: From 2015 to 2025. Nat. Rev. Gastroenterol. Hepatol. 2015, 12, 720–727. [Google Scholar] [CrossRef] [PubMed]
- Jemal, A.; Bray, F.; Center, M.M.; Ferlay, J.; Ward, E.; Forman, D. Global cancer statistics. CA Cancer J. Clin. 2011, 61, 69–90. [Google Scholar] [CrossRef] [PubMed]
- Iddan, G.; Meron, G.; Glukhovsky, A.; Swain, P. Wireless capsule endoscopy. Nature 2000, 405, 417. [Google Scholar] [CrossRef] [PubMed]
- Sivak, M. Gastrointestinal endoscopy: Past and future. Gut 2006, 55, 1061–1064. [Google Scholar] [CrossRef] [PubMed]
- Cox, B.F.; Stewart, F.; Lay, H.; Cummins, G.; Newton, I.P.; Desmulliez, M.P.; Steele, R.J.; Nthkeä, I.; Cochran, S. Ultrasound capsule endoscopy: Sounding out the future. Ann. Trans. Med. 2017, 5, 201. [Google Scholar] [CrossRef] [PubMed]
- Cummins, G.; Lay, H.; Cox, B.; Seetohul, V.; Qiu, Y.; Stewart, F.; Faerber, J.; Mitrakos, V.; Al Rawhani, M.; Beeley, J. Sonopill: A platform for gastrointestinal disease diagnosis and therapeutics. In Proceedings of the 6th Joint Workshop on New Technologies for Computer/Robot Assisted Surgery, Pisa, Italy, 12–14 September 2016. [Google Scholar]
- Lay, H.; Qiu, Y.; Al-Rawhani, M.; Beeley, J.; Poltarjonoks, R.; Seetohul, V.; Cumming, D.; Cochran, S.; Cummins, G.; Desmulliez, M. Progress towards a multi-modal capsule endoscopy device featuring microultrasound imaging. In Proceedings of the 2016 IEEE International Ultrasonics Symposium (IUS), Tours, France, 18–21 September 2016; IEEE: Piscataway, NJ, USA, 2016; pp. 1–4. [Google Scholar]
- Al-Rawhani, M.A.; Beeley, J.; Cumming, D.R. Wireless fluorescence capsule for endoscopy using single photon-based detection. Sci. Rep. 2015, 5, 18591. [Google Scholar] [CrossRef] [PubMed]
- Stewart, F. Sonocait: Proof-of-concept ultrasound-enabled therapeutic capsule endoscope. J. Med. Robot. Res. 2017, 26, 1238–1246. [Google Scholar]
- Stewart, F.; Cox, B.; Vorstius, J.; Verbeni, A.; Qiu, Y.; Cochran, S. Capsule-based ultrasound-mediated targeted gastrointestinal drug delivery. In Proceedings of the 2015 IEEE International Ultrasonics Symposium (IUS), Taipei, Taiwan, 21–24 October 2015; IEEE: Piscataway, NJ, USA, 2015; pp. 1–4. [Google Scholar]
- Moglia, A.; Menciassi, A.; Schurr, M.O.; Dario, P. Wireless capsule endoscopy: From diagnostic devices to multipurpose robotic systems. Biomed. Microd. 2007, 9, 235–243. [Google Scholar] [CrossRef] [PubMed]
- Ciuti, G.; Caliò, R.; Camboni, D.; Neri, L.; Bianchi, F.; Arezzo, A.; Koulaouzidis, A.; Schostek, S.; Stoyanov, D.; Oddo, C. Frontiers of robotic endoscopic capsules: A review. J. Micro-Bio Robot. 2016, 11, 1–18. [Google Scholar] [CrossRef]
- Koulaouzidis, A.; Iakovidis, D.K.; Karargyris, A.; Rondonotti, E. Wireless endoscopy in 2020: Will it still be a capsule? World J. Gastroenterol. 2015, 21, 5119. [Google Scholar] [CrossRef] [PubMed]
- Mc Caffrey, C.; Chevalerias, O.; O’Mathuna, C.; Twomey, K. Swallowable-capsule technology. IEEE Pervasive Comput. 2008, 7. [Google Scholar] [CrossRef]
- Caunedo-Álvarez, Á.; Romero-Vazquez, J.; Herrerias-Gutierrez, J.M. Patency© and agile© capsules. World J. Gastroenterol. 2008, 14, 5269–5273. [Google Scholar] [CrossRef] [PubMed]
- Wang, A.; Banerjee, S.; Barth, B.A.; Bhat, Y.M.; Chauhan, S.; Gottlieb, K.T.; Konda, V.; Maple, J.T.; Murad, F.; Pfau, P.R. Wireless capsule endoscopy. Gastrointest. Endosc. 2013, 78, 805–815. [Google Scholar] [CrossRef] [PubMed]
- Fisher, L.R.; Hasler, W.L. New vision in video capsule endoscopy: Current status and future directions. Nat. Rev. Gastroenterol. Hepatol. 2012, 9, 392–405. [Google Scholar] [CrossRef] [PubMed]
- Koulaouzidis, A.; Rondonotti, E.; Karargyris, A. Small-bowel capsule endoscopy: A ten-point contemporary. World J. Gastroenterol. 2013, 19, 3726–3746. [Google Scholar] [CrossRef] [PubMed]
- Basar, M.R.; Malek, F.; Juni, K.M.; Idris, M.S.; Saleh, M.I.M. Ingestible wireless capsule technology: A review of development and future indication. Int. J. Antennas Propag. 2012, 2012, 14. [Google Scholar] [CrossRef]
- Toennies, J.L.; Tortora, G.; Simi, M.; Valdastri, P.; Webster, R.J. Swallowable medical devices for diagnosis and surgery: The state of the art. Proc. Inst. Mech. Eng. Part C J. Mech. Eng. Sci. 2010, 224, 1397–1414. [Google Scholar] [CrossRef]
- Ciuti, G.; Menciassi, A.; Dario, P. Capsule endoscopy: From current achievements to open challenges. IEEE Rev. Biomed. Eng. 2011, 4, 59–72. [Google Scholar] [CrossRef] [PubMed]
- Jinshan Science & Technology. OMOM Capsule Endoscopy System I, Product specifications. Available online: http://www.jinshangroup.com/products_17.html (accessed on 15 May 2017).
- Li, C.-Y.; Zhang, B.-L.; Chen, C.-X.; Li, Y.-M. Omom capsule endoscopy in diagnosis of small bowel disease. J. Zhejiang Univers.-Sci. B 2008, 9, 857–862. [Google Scholar] [CrossRef] [PubMed]
- Medtronic. A Complete Suite of Capsule Endoscopy Solutions within a Single Platform. Available online:http://www.medtronic.com/covidien/products/capsule-endoscopy (accessed on 15 May 2017).
- Yung, D.E.; Rondonotti, E.; Koulaouzidis, A. Review: Capsule colonoscopy—A concise clinical overview of current status. Ann. Trans. Med. 2016, 4, 398. [Google Scholar] [CrossRef] [PubMed]
- Moglia, A.; Menciassi, A.; Dario, P. Recent patents on wireless capsule endoscopy. Recent Pat. Biomed. Eng. 2008, 1, 24–33. [Google Scholar] [CrossRef]
- Gao, M.; Hu, C.; Chen, Z.; Zhang, H.; Liu, S. Design and fabrication of a magnetic propulsion system for self-propelled capsule endoscope. IEEE Trans. Biomed. Eng. 2010, 57, 2891–2902. [Google Scholar] [PubMed]
- Mosse, C.A.; Mills, T.N.; Appleyard, M.N.; Kadirkamanathan, S.S.; Swain, C.P. Electrical stimulation for propelling endoscopes. Gastrointest. Endosc. 2001, 54, 79–83. [Google Scholar] [CrossRef] [PubMed]
- Kim, B.; Lee, S.; Park, J.H.; Park, J.-O. Design and fabrication of a locomotive mechanism for capsule-type endoscopes using shape memory alloys (smas). IEEE/ASME Trans. Mechatron. 2005, 10, 77–86. [Google Scholar] [CrossRef]
- Carpi, F.; Pappone, C. Magnetic maneuvering of endoscopic capsules by means of a robotic navigation system. IEEE Trans. Biomed. Eng. 2009, 56, 1482–1490. [Google Scholar] [CrossRef] [PubMed]
- Ishiyama, K.; Arai, K.; Sendoh, M.; Yamazaki, A. Spiral-type micro-machine for medical applications. J. Micromechatron. 2002, 2, 77–86. [Google Scholar] [CrossRef]
- Valdastri, P.; Webster, R.J., III; Quaglia, C.; Quirini, M.; Menciassi, A.; Dario, P. A new mechanism for mesoscale legged locomotion in compliant tubular environments. IEEE Trans. Robot. 2009, 25, 1047–1057. [Google Scholar] [CrossRef]
- Quirini, M.; Scapellato, S.; Valdastri, P.; Menciassi, A.; Dario, P. An approach to capsular endoscopy with active motion. In Proceedings of the 29th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, 2007 (EMBS 2007), Lyon, France, 23–26 August 2007; IEEE: Piscataway, NJ, USA, 2007; pp. 2827–2830. [Google Scholar]
- Simi, M.; Valdastri, P.; Quaglia, C.; Menciassi, A.; Dario, P. Design, fabrication, and testing of a capsule with hybrid locomotion for gastrointestinal tract exploration. IEEE/ASME Trans. Mechatron. 2010, 15, 170–180. [Google Scholar] [CrossRef]
- Wang, K.; Yan, G.; Ma, G.; Ye, D. An earthworm-like robotic endoscope system for human intestine: Design, analysis, and experiment. Ann. Biomed. Eng. 2009, 37, 210–221. [Google Scholar] [CrossRef] [PubMed]
- Kim, B.; Park, S.; Jee, C.Y.; Yoon, S.-J. An earthworm-like locomotive mechanism for capsule endoscopes. In Proceedings of the 2005 IEEE/RSJ International Conference on Intelligent Robots and Systems (IROS 2005), Edmonton, AB, Canada, 2–6 August 2005; IEEE: Piscataway, NJ, USA, 2005; pp. 2997–3002. [Google Scholar]
- Valdastri, P. Mesoscale mobile robots for gastrointestinal minimally invasive surgery (mis). Med. Robot. Minim. Invasive Surg. 2012, 224–251. [Google Scholar] [CrossRef]
- Fischer, D.; Schreiber, R.; Levi, D.; Eliakim, R. Capsule endoscopy: The localization system. Gastrointest. Endosc. Clin. N. Am. 2004, 14, 25–31. [Google Scholar] [CrossRef] [PubMed]
- Jacob, H.; Frisch, M.; Levy, D.; Glukhovsky, A.; Shreiber, R.; Adler, S. Localization of the given m2a® ingestible capsule in the given® diagnostic imaging system. Am. J. Gastroenterol. 2001, 96, S106–S107. [Google Scholar] [CrossRef]
- Woods, S.P.; Constandinou, T.G. Wireless capsule endoscope for targeted drug delivery: Mechanics and design considerations. IEEE Trans. Biomed. Eng. 2013, 60, 945–953. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Meng, M.Q.-H.; Hu, C. A localization method using 3-axis magnetoresistive sensors for tracking of capsule endoscope. In Proceedings of the 28th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, 2006 (EMBS’06), New York, NY, USA, 30 August–3 September 2006; IEEE: Piscataway, NJ, USA, 2006; pp. 2522–2525. [Google Scholar]
- Andrä, W.; Danan, H.; Kirmße, W.; Kramer, H.-H.; Saupe, P.; Schmieg, R.; Bellemann, M.E. A novel method for real-time magnetic marker monitoring in the gastrointestinal tract. Phys. Med. Biol. 2000, 45, 3081–3093. [Google Scholar] [CrossRef] [PubMed]
- Arshak, K.; Adepoju, F. Capsule tracking in the gi tract: A novel microcontroller based solution. In Proceedings of the 2006 IEEE Sensors Applications Symposium, Houston, TX, USA, 7–9 February 2006; IEEE: Piscataway, NJ, USA, 2006; pp. 186–191. [Google Scholar]
- Kuth, R.; Reinschke, J.; Rockelein, R. Method for Determining the Position and Orientation of an Endoscopy Capsule Guided through an Examination Object by Using a Navigating Magnetic Field Generated by Means of a Navigation Device. Patent US 20070038063, 2006. [Google Scholar]
- Wilding, I.; Hirst, P.; Connor, A. Development of a new engineering-based capsule for human drug absorption studies. Pharm. Sci. Technol. Today 2000, 3, 385–392. [Google Scholar] [CrossRef]
- Moglia, A.; Menciassi, A.; Dario, P.; Cuschieri, A. Capsule endoscopy: Progress update and challenges ahead. Nat. Rev. Gastroenterol. Hepatol. 2009, 6, 353–361. [Google Scholar] [CrossRef] [PubMed]
- Jia, Z.; Yan, G.; Shi, Y.; Zhu, B. A wireless power transmission system for an active capsule endoscope for colon inspection. J. Med. Eng. Technol. 2012, 36, 235–241. [Google Scholar] [CrossRef] [PubMed]
- Nadeau, P.; El-Damak, D.; Glettig, D.; Kong, Y.L.; Mo, S.; Cleveland, C.; Booth, L.; Roxhed, N.; Langer, R.; Chandrakasan, A.P. Prolonged energy harvesting for ingestible devices. Nat. Biomed. Eng. 2017, 1, 0022. [Google Scholar] [CrossRef] [PubMed]
- Oostendorp, R.L.; Beijnen, J.H.; Schellens, J.H. The biological and clinical role of drug transporters at the intestinal barrier. Cancer Treat. Rev. 2009, 35, 137–147. [Google Scholar] [CrossRef] [PubMed]
- Munoz, F.; Alici, G.; Li, W. A review of drug delivery systems for capsule endoscopy. Adv. Drug Deliv. Rev. 2014, 71, 77–85. [Google Scholar] [CrossRef] [PubMed]
- Iakovidis, D.K.; Koulaouzidis, A. Software for enhanced video capsule endoscopy: Challenges for essential progress. Nat. Rev. Gastroenterol. Hepatol. 2015, 12, 172–186. [Google Scholar] [CrossRef] [PubMed]
- Swain, P. The future of wireless capsule endoscopy. World J. Gastroenterol. 2008, 14, 4142–4145. [Google Scholar] [CrossRef] [PubMed]
- Zou, H.; Shimizu, J.; Iordanov, V.; Dijksman, F. Regional drug absorption study in canines with intelligent pill system. In Proceedings of the 37th Annual Meeting Controlled Release Society, Portland, OR, USA, 10–14 July 2010. [Google Scholar]
- Çolak, B.; Şakalak, H.; Çavuşoğlu, H.; Yavuz, M.S. Novel capsules for potential theranostics of obscure gastrointestinal bleedings. Med. Hypotheses 2016, 94, 99–102. [Google Scholar] [CrossRef] [PubMed]
- Glass, P.; Cheung, E.; Sitti, M. A legged anchoring mechanism for capsule endoscopes using micropatterned adhesives. IEEE Trans. Biomed. Eng. 2008, 55, 2759–2767. [Google Scholar] [CrossRef] [PubMed]
- Yim, S.; Sitti, M. Design and rolling locomotion of a magnetically actuated soft capsule endoscope. IEEE Trans. Robot. 2012, 28, 183–194. [Google Scholar] [CrossRef]
- Yim, S.; Sitti, M. 3-D localization method for a magnetically actuated soft capsule endoscope and its applications. IEEE Trans. Robot. 2013, 29, 1139–1151. [Google Scholar] [CrossRef] [PubMed]
- Rasouli, M.; Lin, L.; Prima Kencana, A.; Wong, K.-J.; Tan, S.-L.; Ho, K.Y.; Phee, S.J. Therapeutic capsule endoscopy: Opportunities and challenges. J. Healthc. Eng. 2011, 2, 459–471. [Google Scholar] [CrossRef]
- Valdastri, P.; Quaglia, C.; Susilo, E.; Menciassi, A.; Dario, P.; Ho, C.; Anhoeck, G.; Schurr, M. Wireless therapeutic endoscopic capsule: In vivo experiment. Endoscopy 2008, 40, 979–982. [Google Scholar] [CrossRef] [PubMed]
- Kong, K.-C.; Cha, J.; Jeon, D.; Cho, D.-I.D. A rotational micro biopsy device for the capsule endoscope. In Proceedings of the 2005 IEEE/RSJ International Conference on Intelligent Robots and Systems (IROS 2005), Edmonton, AB, Canada, 2–6 August 2005; IEEE: Piscataway, NJ, USA, 2005; pp. 1839–1843. [Google Scholar]
- Kong, K.; Yim, S.; Choi, S.; Jeon, D. A robotic biopsy device for capsule endoscopy. J. Med. Dev. 2012, 6, 031004. [Google Scholar] [CrossRef]
- Park, S.; Koo, K.-I.; Bang, S.M.; Park, J.Y.; Song, S.Y. A novel microactuator for microbiopsy in capsular endoscopes. J. Micromech. Microeng. 2008, 18, 025032. [Google Scholar] [CrossRef]
- Wang, T.D.; Van Dam, J. Optical biopsy: A new frontier in endoscopic detection and diagnosis. Clin. Gastroenterol. Hepatol. 2004, 2, 744–753. [Google Scholar] [CrossRef]
- Chak, A. Eus in submucosal tumors. Gastrointest. Endosc. 2002, 56, S43–S48. [Google Scholar] [CrossRef]
- Gheorghe, C.; Iacob, R.; Bancila, I. Olympus capsule endoscopy for small bowel examination. J. Gastrointest. Liver Dis. 2007, 16, 309. [Google Scholar]
- Yuan, Y.; Yang, S.; Xing, D. Preclinical photoacoustic imaging endoscope based on acousto-optic coaxial system using ring transducer array. Opt. Lett. 2010, 35, 2266–2268. [Google Scholar] [CrossRef] [PubMed]
- CORDIS. Troy Report Summary. Available online: http://cordis.europa.eu/result/rcn/48767_en.html (accessed on 15 May 2017).
- Memon, F.; Touma, G.; Wang, J.; Baltsavias, S.; Moini, A.; Chang, C.; Rasmussen, M.F.; Nikoozadeh, A.; Choe, J.W.; Olcott, E. Capsule ultrasound device: Further developments. In Proceedings of the 2016 IEEE International Ultrasonics Symposium (IUS), Tours, France, 18–21 September 2016; IEEE: Piscataway, NJ, USA, 2016; pp. 1–4. [Google Scholar]
- Lee, J.H.; Traverso, G.; Schoellhammer, C.M.; Blankschtein, D.; Langer, R.; Thomenius, K.E.; Boning, D.S.; Anthony, B.W. Towards wireless capsule endoscopic ultrasound (WCEU). In Proceedings of the 2014 IEEE International Ultrasonics Symposium (IUS), Chicago, IL, USA, 3–6 September 2014; IEEE: Piscataway, NJ, USA, 2014; pp. 734–737. [Google Scholar]
- Arneson, M.; Bandy, W.; Shanks, W. Ultrasound Scanning Capsule Endoscope (USCE). Patent US 8647259 B2, 11 February 2014. [Google Scholar]
- Iddan, G.J. Ultrasonic Capsule. Patent US 20110130658 A1, 22 March 2008. [Google Scholar]
- Taniguchi, Y. Intracoelomic mobile body, and capsule-type ultrasonic endoscope. Patent US 7452338 B2, 18 November 2008. [Google Scholar]
- Wang, X.; Seetohul, V.; Chen, R.; Qian, M.; Wang, C.; Huang, Z.; Zhou, Q.; Zheng, H.; Cochran, S.; Qiu, W. Development of a mechanical scanning device with high-frequency ultrasound transducer for ultrasonic capsule endoscopy. IEEE Trans. Med. Imaging 2017. [Google Scholar] [CrossRef] [PubMed]
- Gourevich, D.; Volovick, A.; Dogadkin, O.; Wang, L.; Mulvana, H.; Medan, Y.; Melzer, A.; Cochran, S. In vitro investigation of the individual contributions of ultrasound-induced stable and inertial cavitation in targeted drug delivery. Ultrasound Med. Biol. 2015, 41, 1853–1864. [Google Scholar] [CrossRef] [PubMed]
- Gourevich, D.; Dogadkin, O.; Volovick, A.; Wang, L.; Gnaim, J.; Cochran, S.; Melzer, A. Ultrasound-mediated targeted drug delivery with a novel cyclodextrin-based drug carrier by mechanical and thermal mechanisms. J. Controll. Release 2013, 170, 316–324. [Google Scholar] [CrossRef] [PubMed]
- Huang, S.-L. Liposomes in ultrasonic drug and gene delivery. Adv. Drug Deliv. Rev. 2008, 60, 1167–1176. [Google Scholar] [CrossRef] [PubMed]
- Rapoport, N. Physical stimuli-responsive polymeric micelles for anti-cancer drug delivery. Prog. Polym. Sci. 2007, 32, 962–990. [Google Scholar] [CrossRef]
- Antipina, M.N.; Sukhorukov, G.B. Remote control over guidance and release properties of composite polyelectrolyte based capsules. Adv. Drug Deliv. Rev. 2011, 63, 716–729. [Google Scholar] [CrossRef] [PubMed]
- Medtronic. Pillcam Colon. Available online: ous.pillcamcolon.com (accessed on 8 May 2017).
- Anbarasan, T.; Demore, C.; Lay, H.; Sunoqrot, M.; Poltarjonoks, R.; Cochran, S.; Cox, B. Development of small bowel tissue phantom for microultrasound investigation. J. Crohns Colitis 2016, 10, S103–S104. [Google Scholar]
- Lay, H.; Cox, B.; Sunoqrot, M.; Démoré, C.; Näthke, I.; Gomez, T.; Cochran, S. Microultrasound characterisation of ex vivo porcine tissue for ultrasound capsule endoscopy. J. Phys. Conf. Ser. 2017, 797, 012003. [Google Scholar] [CrossRef]
- Cox, B.; Stewart, F.; Huang, Z.; Nathke, I.; Cochran, S. Ultrasound facilitated marking of gastrointestinal tissue with fluorescent material. In Proceedings of the 2016 IEEE International Ultrasonics Symposium (IUS), Tours, France, 18–21 September 2016; IEEE: Piscataway, NJ, USA, 2016; pp. 1–4. [Google Scholar]
- Stewart, F. Theranostics in the gut. In Theranostics and Image Guided Drug Delivery; Thanou, M., Ed.; Royal Society of Chemistry: London, UK, 2017; in press. [Google Scholar]
- Stewart, F.; Cox, B.; Wang, G.; Huang, Z.; Newton, I.; Nathke, I.; Thanou, M.; Cochran, S. An in vitro sonication system for applications in ultrasound-mediated targeted drug delivery. In Proceedings of the 2016 IEEE International Ultrasonics Symposium (IUS), Tours, France, 18–21 September 2016; IEEE: Piscataway, NJ, USA, 2016; pp. 1–4. [Google Scholar]
- Ødegaard, S.; Nesje, L.B.; Lærum, O.D.; Kimmey, M.B. High-frequency ultrasonographic imaging of the gastrointestinal wall. Expert Rev. Med. Dev. 2012, 9, 263–273. [Google Scholar] [CrossRef] [PubMed]
- Fatehullah, A.; Sharma, S.; Newton, I.; Langlands, A.; Lay, H.; Nelson, S.; McMahon, R.; McIlvenny, N.; Appleton, P.; Cochran, S. Increased variability in apcmin/+ intestinal tissue can be measured with microultrasound. Sci. Rep. 2016, 6. [Google Scholar] [CrossRef] [PubMed]
- Saha, R.K.; Kolios, M.C. Effects of cell spatial organization and size distribution on ultrasound backscattering. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2011, 58, 2118–2131. [Google Scholar] [CrossRef] [PubMed]
- Oelze, M.L.; Zachary, J.F.; O’Brien, W.D., Jr. Characterization of tissue microstructure using ultrasonic backscatter: Theory and technique for optimization using a gaussian form factor. J. Acoust. Soc. Am. 2002, 112, 1202–1211. [Google Scholar] [CrossRef] [PubMed]
- Feleppa, E.J.; Liu, T.; Kalisz, A.; Shao, M.C.; Fleshner, N.; Reuter, V.; Fair, W.R. Ultrasonic spectral-parameter imaging of the prostate. Int. J. Imaging Syst. Technol. 1997, 8, 11–25. [Google Scholar] [CrossRef]
- Gregerson, H.; Jensen, S.L.; Moody, F.; Shokouh-Amiri, M. Essentials of Experimental Surgery: Gastroenterology; CRC Press: Boca Raton, FL, USA, 1996. [Google Scholar]
- Salzer, R. Biomedical Imaging: Principles and Applications; John Wiley & Sons: Hoboken, NJ, USA, 2012. [Google Scholar]
- Jankowski, J.; Barr, H.; Wang, K.; Delaney, B. Diagnosis and management of barrett’s oesophagus. BMJ 2010, 341, c4551. [Google Scholar] [CrossRef] [PubMed]
- Moran, C.; Bush, N.; Bamber, J. Ultrasonic propagation properties of excised human skin. Ultrasound Med. Biol. 1995, 21, 1177–1190. [Google Scholar] [CrossRef]
- Ye, S.; Harasiewicz, K.; Pavlin, C.; Foster, F. Ultrasound characterization of normal ocular tissue in the frequency range from 50 mhz to 100 mhz. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 1995, 42, 8–14. [Google Scholar] [CrossRef]
- Aristizábal, O.; Turnbull, D.H.; Ketterling, J.A.; Mamou, J. In vivo 3d quantitative analysis of the mouse embryonic brain with a 38 mhz annular array and coded excitation. In Proceedings of the 2010 IEEE Ultrasonics Symposium (IUS), San Diego, CA, USA, 11–14 October 2010; IEEE: Piscataway, NJ, USA, 2010; pp. 794–797. [Google Scholar]
- Fink, M.; Hottier, F.; Cardoso, J. Ultrasonic signal processing for in vivo attenuation measurement: Short time fourier analysis. Ultrason. Imaging 1983, 5, 117–135. [Google Scholar] [CrossRef] [PubMed]
- Azhari, H. Basics of Biomedical Ultrasound for Engineers; John Wiley & Sons: Hoboken, NJ, USA, 2010. [Google Scholar]
- Qiu, Z. Development of Mri-Compatible Transducer Array for Focused Ultrasound Surgery: The Use of Relaxor-Based Piezocrystals; University of Dundee: Dundee, UK, 2014. [Google Scholar]
- Meunier, V.; Bourrié, M.; Berger, Y.; Fabre, G. The human intestinal epithelial cell line caco-2; pharmacological and pharmacokinetic applications. Cell Biol. Toxicol. 1995, 11, 187–194. [Google Scholar] [CrossRef] [PubMed]
- US Department of Health and Human Services, F.a.D.A.; Center for Drug Evaluation and Research (CDER). Guidance for industry. Waiver of in Vivo Bioavailability and Bioequivalence Studies for Immediate-Release Solid Oral Dosage Forms Based on a Biopharmaceutics Classification System. Available online: http://www.fda.gov/downloads/Drugs/GuidanceComplianceRegulatoryInformation/Guidances/UCM070246.pdf (accessed on 16 May 2017).
- Srinivasan, B.; Kolli, A.R.; Esch, M.B.; Abaci, H.E.; Shuler, M.L.; Hickman, J.J. Teer measurement techniques for in vitro barrier model systems. J. Lab. Autom. 2015, 20, 107–126. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.; Einspanier, R.; Schoen, J. Transepithelial electrical resistance (teer): A functional parameter to monitor the quality of oviduct epithelial cells cultured on filter supports. Histochem. Cell Biol. 2015, 144, 509–515. [Google Scholar] [CrossRef] [PubMed]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Device | Company | Size (mm) | Weight (g) | Imaging Sensor (Pixel Res.) | Frame Rate (fps) | Angle of View (°) | Image Display | Battery Lifetime (h) |
|---|---|---|---|---|---|---|---|---|
| PillCam® SB3 | Medtronic Inc., Dublin, Ireland. | Ø11.4 × 26.2 | 3.0 | CMOS (256 × 256) | 2–6 | 156 | Offline | 8 |
| PillCam® COLON2 | Ø11.6 × 32.8 | 3.0 | CMOS × 2 (256 × 256) | 4–35 | 172 | Real Time | 10 | |
| PillCam® UGI | Ø11.6 × 32.8 | 3.0 | CMOS × 2 (256 × 256) | 18–35 | 172 | Real Time | 1.5 | |
| PillCam® PATENCY | Ø11 × 26 | 3.3 | N/A 1 | |||||
| Endo-Capsule | Olympus, Tokyo, Japan | Ø11 × 26 | 3.8 | CCD (1920 × 1080) | 2 | 145 | Real Time | 8–10 |
| OMOM System I | Jinshan Sci. & Tech., Chongqing, China | Ø11 × 25.4 | ≤6.0 | CMOS (640 × 480) | 2 | 140 | Real Time | 12 |
| MiroCam | IntroMedic, Seoul, Korea | Ø10.8 × 24 | 3.3 | CMOS (320 × 320) | 3 | 150 | Offline | 10–12 |
| CapsoCam Plus | CapsoVision, Saratoga, CA, USA | Ø11 × 31 | 4.0 | CCD × 4 (221 × 884) | 20 | 360 | Offline | 15 |
| CE-Relevant Step in Patient Pathway | Required Technical Capability | Present Status of Research | Results Presented in This Paper | Relevant References |
|---|---|---|---|---|
| 2a/4 | µUS Imaging, Video Imaging, CADx | VCE established. US CE in development. Bench tests performed | Bench testing, QUS analysis | [5,6,7,80,81] |
| 2b | US tissue marking | Proof of concept capsule developed. Tissue marking with nanoparticles demonstrated | Proof of concept capsule. Tissue marking | [9,10,82] |
| 3a/b | UmTDD Capsule. Fluorescence Imaging | Proof of concept capsule developed and bench tested. Fluorescence imaging capsule developed; requires miniaturization. | Development of therapeutic capsule. Fluorescence capsule | [8,9,10,83,84] |
| Input Voltage (Vpp) | Winput (mW) | Woutput (mW) | Efficiency (%) | Pressure (kPa) | Beam Diam. (mm) | Intensity (W/cm2) | Mech. Index |
|---|---|---|---|---|---|---|---|
| 1 | 2.54 | N/A 1 | N/A 1 | 11.0 | 2.70 | N/A 1 | 0.005 |
| 2 | 10.2 | N/A 1 | N/A 1 | 22.9 | 2.70 | N/A 1 | 0.011 |
| 3 | 22.8 | 8.50 | 37.2 | 34.7 | 2.70 | 0.15 | 0.017 |
| 4 | 40.6 | 19.9 | 49.0 | 53.7 | 2.70 | 0.35 | 0.026 |
| 5 | 63.4 | 34.8 | 54.8 | 61.5 | 2.70 | 0.61 | 0.030 |
| 6 | 91.4 | 51.0 | 55.8 | 77.4 | 2.70 | 0.89 | 0.038 |
| 7 | 124 | 71.3 | 57.4 | 93.3 | 2.70 | 1.25 | 0.046 |
| 8 | 162 | 93.6 | 57.6 | 117 | 2.70 | 1.64 | 0.058 |
| 9 | 206 | 123 | 59.8 | 136 | 2.70 | 2.15 | 0.067 |
| 10 | 254 | 153 | 60.3 | 153 | 2.70 | 2.67 | 0.076 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stewart, F.R.; Qiu, Y.; Lay, H.S.; Newton, I.P.; Cox, B.F.; Al-Rawhani, M.A.; Beeley, J.; Liu, Y.; Huang, Z.; Cumming, D.R.S.; et al. Acoustic Sensing and Ultrasonic Drug Delivery in Multimodal Theranostic Capsule Endoscopy. Sensors 2017, 17, 1553. https://doi.org/10.3390/s17071553
Stewart FR, Qiu Y, Lay HS, Newton IP, Cox BF, Al-Rawhani MA, Beeley J, Liu Y, Huang Z, Cumming DRS, et al. Acoustic Sensing and Ultrasonic Drug Delivery in Multimodal Theranostic Capsule Endoscopy. Sensors. 2017; 17(7):1553. https://doi.org/10.3390/s17071553
Chicago/Turabian StyleStewart, Fraser R., Yongqiang Qiu, Holly S. Lay, Ian P. Newton, Benjamin F. Cox, Mohammed A. Al-Rawhani, James Beeley, Yangminghao Liu, Zhihong Huang, David R. S. Cumming, and et al. 2017. "Acoustic Sensing and Ultrasonic Drug Delivery in Multimodal Theranostic Capsule Endoscopy" Sensors 17, no. 7: 1553. https://doi.org/10.3390/s17071553