A Clinically Evaluated Interferometric Continuous-Wave Radar System for the Contactless Measurement of Human Vital Parameters

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Physiological Fundamentals
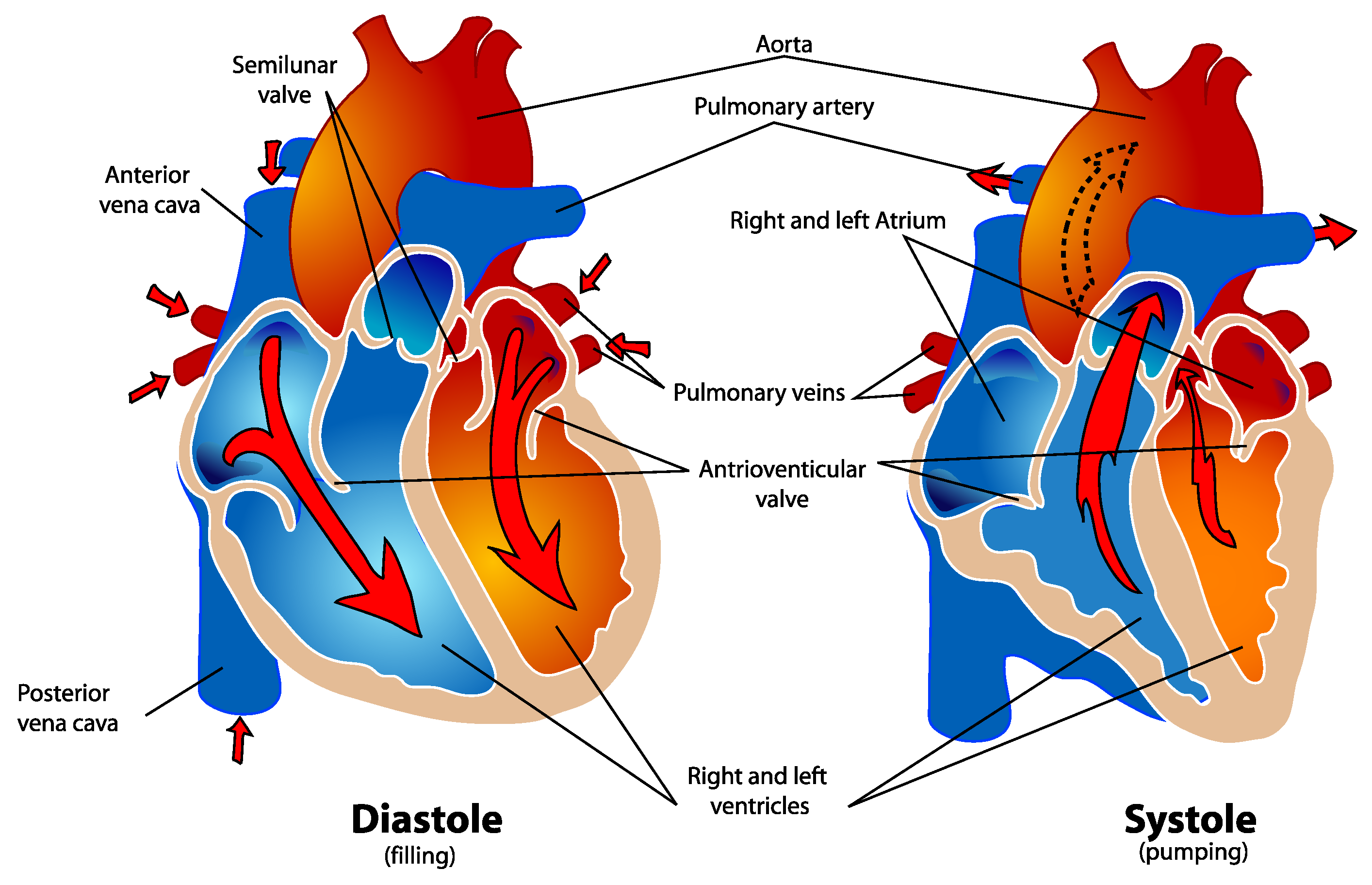
2.1. Cardiovascular Physiology
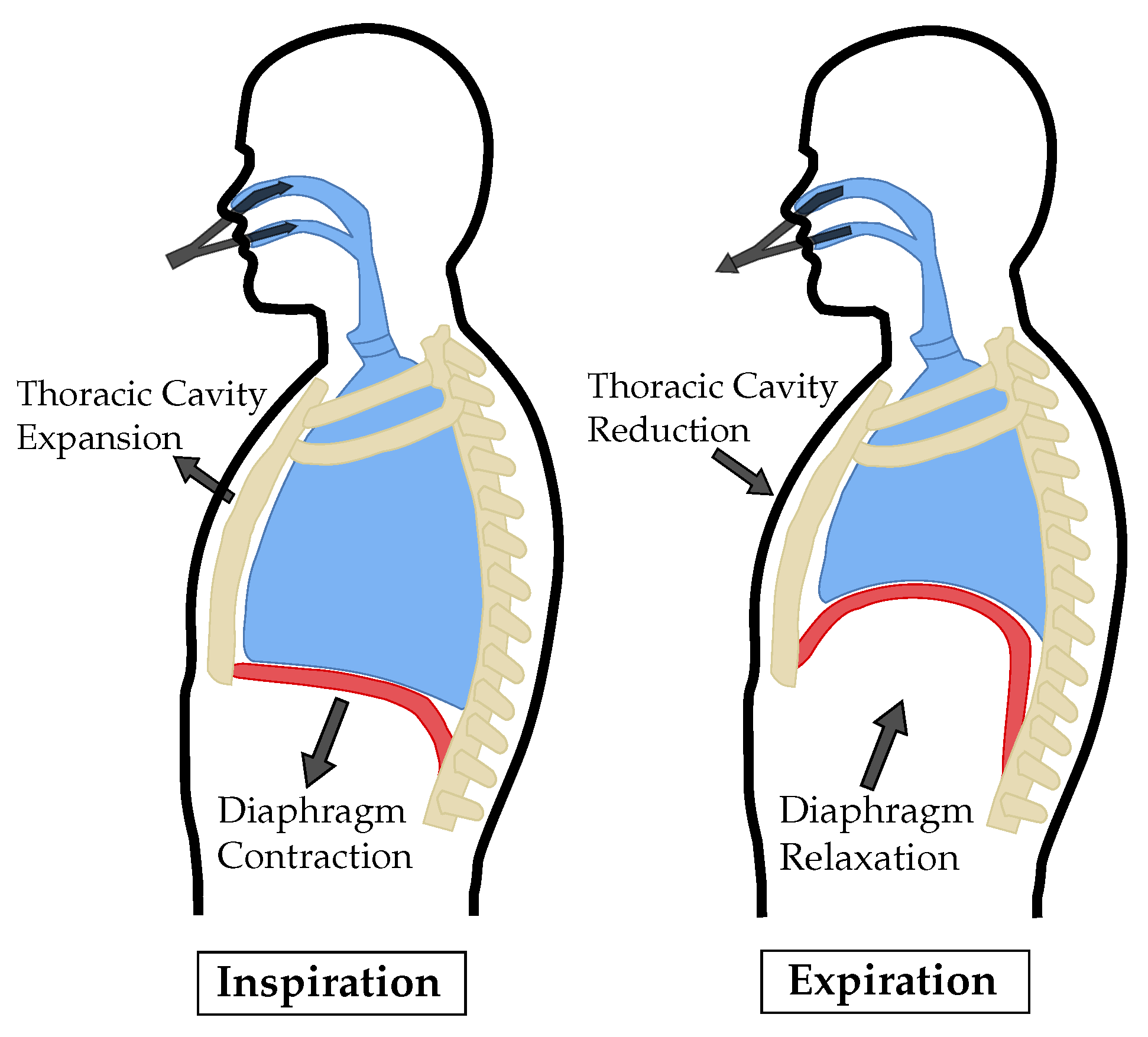
2.2. Respiration Physiology
3. System Concept
3.1. RF Concept and Design
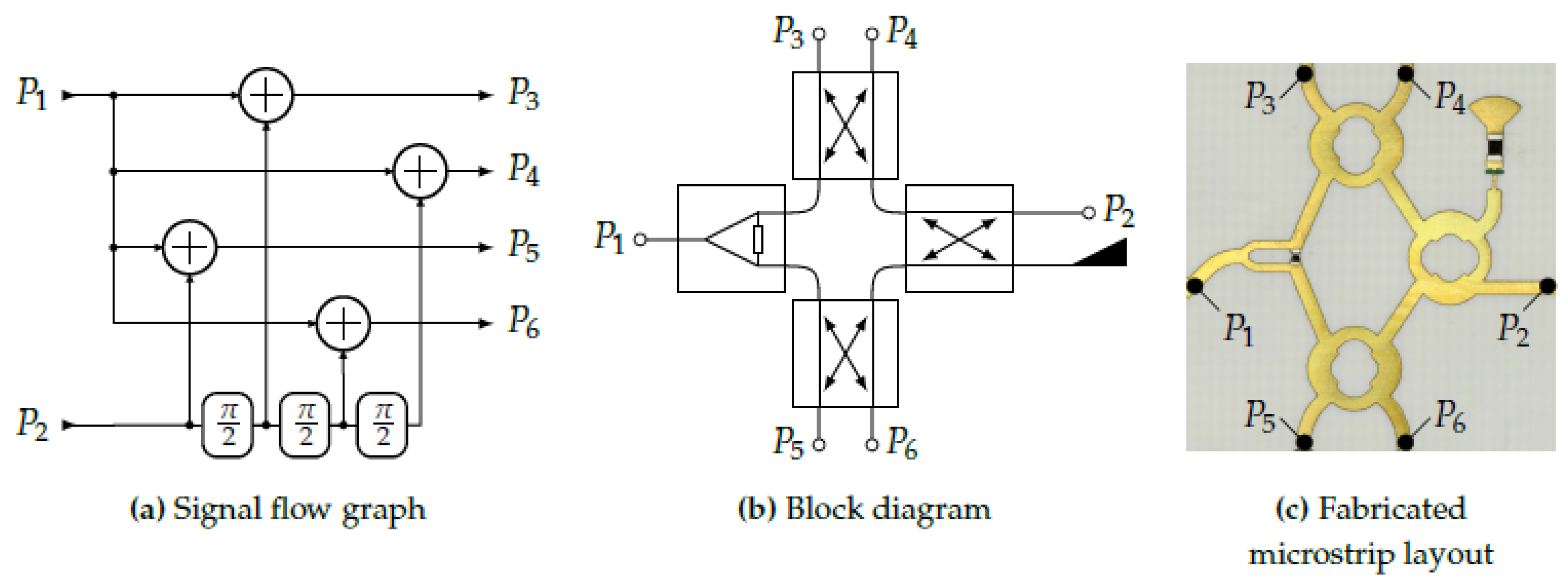
3.1.1. Six-Port Receiver
3.1.2. Antenna Design
3.1.3. Link Budget
3.1.4. Analog Baseband
3.2. Interface Board
3.3. Fabricated Prototype
4. Signal Processing
4.1. Distance Signal Reconstruction
4.2. Respiration Signal Analysis
- Autocorrelation: With the help of the autocorrelation (ACF) periodicity can be found in the respiration signal. After calculating the ACF, corresponds to:where x is the windowed breathing signal with length N. Subsequently, the respiration rate can be determined by selecting the largest peak in the range of possible respiration durations. In case of the filter limits selected here, the range spans from 3 s to 30 s, which is converted into points using the known sampling frequency. The extracted lag is then converted into the respiratory rate .
- Peaksearch: Using the Matlab internal function ’findpeaks’ with specifying a minimum peak distance and prominence all minima and maxima can be found. The minimum distance of two peaks has to include at least the highest respiration frequency. Therefore, a minimum distance of 3 s is chosen. By differentiation of the minima and maxima locations the durations for both extrema are calculated. Finally, the values are averaged and translated to the respiration rate .
- Zero crossing: Considering the bandpass filtered signal, the respiration is centered around zero. Therefore, the zero crossings (ZCs) can be determined by (5) in order to calculate the respiration rate:Saving all locations of ZC occurings in the given window, the respiration rate can be determined by converting twice the mean value of the differentiated locations into BrPM:
- Fast Fourier transform: The frequency components of a time signal can additionally be determined using the fast Fourier transform (FFT). Moreover, all signals are windowed with a Hann window of the same length before applying the FFT. The frequency spectrum is calculated for each window and the maximum of the spectrum in the range from 0.05 Hz to 0.5 Hz is determined. Afterwards it is converted to .
4.3. Heartbeat Signal Analysis
5. Validation Study
6. Results
6.1. Displacement Measurements
6.2. Respiration
6.3. Heart Rate
7. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Ethics Approval
References
- Hacke, W.; Kaste, M.; Olsen, T.S.; Bogousslavsky, J.; Orgogozo, J.M. Acute treatment of ischemic stroke. Cerebrovasc. Dis. 2000, 10, 22–33. [Google Scholar] [CrossRef] [PubMed]
- Cecconi, M.; De Backer, D.; Antonelli, M.; Beale, R.; Bakker, J.; Hofer, C.; Jaeschke, R.; Mebazaa, A.; Pinsky, M.R.; Teboul, J.L.; et al. Consensus on circulatory shock and hemodynamic monitoring. Task force of the European Society of Intensive Care Medicine. Intensive Care Med. 2014, 40, 1795–1815. [Google Scholar] [CrossRef]
- Cardona-Morrell, M.; Prgomet, M.; Turner, R.; Nicholson, M.; Hillman, K. Effectiveness of continuous or intermittent vital signs monitoring in preventing adverse events on general wards: a systematic review and meta-analysis. Int. J. Clin. Pract. 2016, 70, 806–824. [Google Scholar] [CrossRef]
- Katus, H.; Ziegler, A.; Ekinci, O.; Giannitsis, E.; Stough, W.G.; Achenbach, S.; Blankenberg, S.; Brueckmann, M.; Collinson, P.; Comaniciu, D.; et al. Early diagnosis of acute coronary syndrome. Eur. Heart J. 2017, 38, 3049–3055. [Google Scholar] [CrossRef]
- Heldeweg, M.L.A.; Liu, N.; Koh, Z.X.; Fook-Chong, S.; Lye, W.K.; Harms, M.; Ong, M.E.H. A novel cardiovascular risk stratification model incorporating ECG and heart rate variability for patients presenting to the emergency department with chest pain. Crit. Care 2016, 20, 179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keach, J.W.; Bradley, S.M.; Turakhia, M.P.; Maddox, T.M. Early detection of occult atrial fibrillation and stroke prevention. Heart 2015, 101, 1097–1102. [Google Scholar] [CrossRef] [PubMed]
- Le Gall, J.R.; Lemeshow, S.; Saulnier, F. A new simplified acute physiology score (SAPS II) based on a European/North American multicenter study. Jama 1993, 270, 2957–2963. [Google Scholar] [CrossRef]
- Zimmerman, J.E.; Kramer, A.A.; McNair, D.S.; Malila, F.M. Acute Physiology and Chronic Health Evaluation (APACHE) IV: hospital mortality assessment for today’s critically ill patients. Crit. Care Med. 2006, 34, 1297–1310. [Google Scholar] [CrossRef]
- McGloin, H.; Adam, S.K.; Singer, M. Unexpected deaths and referrals to intensive care of patients on general wards. Are some cases potentially avoidable? J. R. Coll. Phys. Lond. 1999, 33, 255–259. [Google Scholar]
- Solomon, M.D.; Yang, J.; Sung, S.H.; Livingston, M.L.; Sarlas, G.; Lenane, J.C.; Go, A.S. Incidence and timing of potentially high-risk arrhythmias detected through long term continuous ambulatory electrocardiographic monitoring. BMC Cardiovasc. Disord. 2016, 16, 35. [Google Scholar] [CrossRef] [PubMed]
- Bhangu, J.; McMahon, C.G.; Hall, P.; Bennett, K.; Rice, C.; Crean, P.; Sutton, R.; Kenny, R.A. Long-term cardiac monitoring in older adults with unexplained falls and syncope. Heart 2016, 102, 681–686. [Google Scholar] [CrossRef] [Green Version]
- Ziegler, P.D.; Koehler, J.L.; Mehra, R. Comparison of continuous versus intermittent monitoring of atrial arrhythmias. Heart Rhythm 2006, 3, 1445–1452. [Google Scholar] [CrossRef]
- Patil, S.P.; Schneider, H.; Schwartz, A.R.; Smith, P.L. Adult obstructive sleep apnea: pathophysiology and diagnosis. Chest 2007, 132, 325–337. [Google Scholar] [CrossRef]
- Mok, W.; Wang, W.; Cooper, S.; Ang, E.N.K.; Liaw, S.Y. Attitudes towards vital signs monitoring in the detection of clinical deterioration: scale development and survey of ward nurses. Int. J. Qual. Health Care 2015, 27, 207–213. [Google Scholar] [CrossRef] [Green Version]
- Yusif, S.; Soar, J.; Hafeez-Baig, A. Older people, assistive technologies, and the barriers to adoption: A systematic review. Int. J. Med. Inf. 2016, 94, 112–116. [Google Scholar] [CrossRef] [Green Version]
- Kabel, A.; McBee-Black, K.; Dimka, J. Apparel-related participation barriers: Ability, adaptation and engagement. Disabil. Rehabil. 2016, 38, 2184–2192. [Google Scholar] [CrossRef] [PubMed]
- Bassett, R.; Adams, K.M.; Danesh, V.; Groat, P.M.; Haugen, A.; Kiewel, A.; Small, C.; Van-Leuven, M.; Venus, S.; Ely, E.W. Rethinking critical care: decreasing sedation, increasing delirium monitoring, and increasing patient mobility. Joint Comm. J. Qual. Patient Saf. 2015, 41, 62–74. [Google Scholar] [CrossRef]
- Vincent, J.L.; Rubenfeld, G.D. Does intermediate care improve patient outcomes or reduce costs? Crit. Care 2015, 19, 89. [Google Scholar] [CrossRef]
- McGrath, S.P.; Taenzer, A.H.; Karon, N.; Blike, G. Surveillance Monitoring Management for General Care Units: Strategy, Design, and Implementation. Joint Comm. J. Qual. Patient Saf. 2016, 42, 293–302. [Google Scholar] [CrossRef]
- Poh, M.; McDuff, D.J.; Picard, R.W. Advancements in Noncontact, Multiparameter Physiological Measurements Using a Webcam. IEEE Trans. Biomed. Eng. 2011, 58, 7–11. [Google Scholar] [CrossRef] [PubMed]
- Garbey, M.; Sun, N.; Merla, A.; Pavlidis, I. Contact-free measurement of cardiac pulse based on the analysis of thermal imagery. IEEE Trans. Biomed. Eng. 2007, 54, 1418–1426. [Google Scholar] [CrossRef] [PubMed]
- Barbosa Pereira, C.; Czaplik, M.; Blazek, V.; Leonhardt, S.; Teichmann, D. Monitoring of Cardiorespiratory Signals Using Thermal Imaging: A Pilot Study on Healthy Human Subjects. Sensors 2018, 18, 1541. [Google Scholar] [CrossRef]
- EC57 A A. Testing and Reporting Performance Results of Cardiac Rhythm and ST Segment Measurement Algorithms; Association for the Advancement of Medical Instrumentation: Arlington, VA, USA, 2012. [Google Scholar]
- Gambi, E.; Agostinelli, A.; Belli, A.; Burattini, L.; Cippitelli, E.; Fioretti, S.; Pierleoni, P.; Ricciuti, M.; Sbrollini, A.; Spinsante, S. Heart rate detection using microsoft kinect: Validation and comparison to wearable devices. Sensors 2017, 17, 1776. [Google Scholar] [CrossRef]
- Procházka, A.; Schätz, M.; Vyšata, O.; Vališ, M. Microsoft kinect visual and depth sensors for breathing and heart rate analysis. Sensors 2016, 16, 996. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.J.; Hwang, S.H.; Yoon, H.N.; Lee, W.K.; Park, K.S. Heart rate variability monitoring during sleep based on capacitively coupled textile electrodes on a bed. Sensors 2015, 15, 11295–11311. [Google Scholar] [CrossRef] [PubMed]
- Lim, Y.G.; Kim, K.K.; Park, K.S. ECG Recording on a Bed During Sleep Without Direct Skin-Contact. IEEE Trans. Biomed. Eng. 2007, 54, 718–725. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Lubecke, V.M.; Boric-Lubecke, O.; Lin, J. A Review on Recent Advances in Doppler Radar Sensors for Noncontact Healthcare Monitoring. IEEE Trans. Microw. Theory Technol. 2013, 61, 2046–2060. [Google Scholar] [CrossRef]
- Will, C.; Shi, K.; Schellenberger, S.; Steigleder, T.; Michler, F.; Fuchs, J.; Weigel, R.; Ostgathe, C.; Koelpin, A. Radar-Based Heart Sound Detection. Sci. Rep. 2018, 8, 11551. [Google Scholar] [CrossRef]
- Braunwald, E.; Zipes, D.P.; Libby, P. Heart Disease: A Textbook of Cardiovascular Medicine, 6th ed.; WB Saunders: St. Louis, MO, USA, 2001. [Google Scholar]
- Yusuf, S.; Wood, D.; Ralston, J.; Reddy, K.S. The World Heart Federation’s vision for worldwide cardiovascular disease prevention. Lancet 2015, 386, 399–402. [Google Scholar] [CrossRef]
- Guyton, A.C.; Hall, J.E. Textbook of Medical Physiolgy; Elsevier Saunders: Philadelphia, PA, USA, 2006. [Google Scholar]
- van Opbergen, C.J.M.; van der Voorn, S.M.; Vos, M.A.; de Boer, T.P.; van Veen, T.A.B. Cardiac Ca2+ signalling in zebrafish: Translation of findings to man. Prog. Biophys. Mol. Biol. 2018, 138, 45–58. [Google Scholar] [CrossRef]
- Levitzky, M. Pulmonary Physiology, 7th ed.; LANGE Physiology Series; McGraw-Hill Education: New York, NY, USA, 2007. [Google Scholar]
- Yuan, G.; Drost, N.A.; McIvor, R.A. Respiratory rate and breathing pattern. MUMJ 2013, 7, 23–25. [Google Scholar]
- McGee, S. Evidence-Based Physical Diagnosis, 4th ed.; Elsevier: Philadelphia, PA, USA, 2018. [Google Scholar]
- Kaniusas, E. Biomedical Signals and Sensors I; Springer: Berlin/Heidelberg, Germany, 2012. [Google Scholar]
- Infineon Technologies AG. BGT24MTR11 Data Sheet. Available online: http://www.alldatasheet.com/datasheet-pdf/pdf/756319/INFINEON/BGT24MTR11.html (accessed on 30 May 2019).
- Koelpin, A.; Lurz, F.; Linz, S.; Mann, S.; Will, C.; Lindner, S. Six-Port Based Interferometry for Precise Radar and Sensing Applications. Sensors 2016, 16, 1556. [Google Scholar] [CrossRef]
- Linz, S.; Lurz, F.; Weigel, R.; Koelpin, A. A Review on Six-Port Radar and Its Calibration Techniques. In Proceedings of the 22nd International Microwave and Radar Conference (MIKON), Poznan, Poland, 14–17 May 2018; pp. 80–83. [Google Scholar] [CrossRef]
- Fortin, J.; Haitchi, G.; Bojic, A.; Habenbacher, W.; Grullenberger, R.; Heller, A.; Pacher, R.; Wach, P.; Skrabal, F. Validation and verification of the Task Force Monitor. Results Clin. Stud. FDA 2001, 510, 1–7. [Google Scholar]
- Will, C.; Shi, K.; Schellenberger, S.; Steigleder, T.; Michler, F.; Weigel, R.; Ostgathe, C.; Koelpin, A. Local Pulse Wave Detection using Continuous Wave Radar Systems. IEEE J. Electromagn. RF Microw. Med. Biol. 2017. [Google Scholar] [CrossRef]
- Springer, D.B.; Tarassenko, L.; Clifford, G.D. Logistic Regression-HSMM-Based Heart Sound Segmentation. IEEE Trans. Biomed. Eng. 2016, 63, 822–832. [Google Scholar] [CrossRef]
- Will, C.; Shi, K.; Lurz, F.; Weigel, R.; Koelpin, A. Instantaneous heartbeat detection using a cross-correlation based template matching for continuous wave radar systems. In Proceedings of the 2016 IEEE Topical Conference on Wireless Sensors and Sensor Networks (WiSNet), Austin, TX, USA, 24–27 January 2016; pp. 31–34. [Google Scholar] [CrossRef]
- Tomii, S.; Ohtsuki, T. Heartbeat detection by using Doppler radar with wavelet transform based on scale factor learning. In Proceedings of the 2015 IEEE International Conference on Communications (ICC), London, UK, 8–12 June 2015; pp. 483–488. [Google Scholar]
- Mogi, E.; Ohtsuki, T. Heartbeat detection with Doppler radar based on spectrogram. In Proceedings of the 2017 IEEE International Conference on Communications (ICC), Paris, France, 21–25 May 2017; pp. 1–6. [Google Scholar]
- Mogi, E.; Ohtsuki, T. Heartbeat detection with Doppler sensor using adaptive scale factor selection on learning. In Proceedings of the 2015 IEEE 26th Annual International Symposium on Personal, Indoor, and Mobile Radio Communications (PIMRC), Hong Kong, China, 30 August–2 September 2015; pp. 2166–2170. [Google Scholar]
- Lee, Y.S.; Pathirana, P.N.; Evans, R.J.; Steinfort, C.L. Noncontact detection and analysis of respiratory function using microwave Doppler radar. J. Sens. 2015, 2015, 548136. [Google Scholar] [CrossRef]
- Lee, Y.S.; Pathirana, P.N.; Steinfort, C.L. Respiration rate and breathing patterns from Doppler radar measurements. In Proceedings of the 2014 IEEE Conference on Biomedical Engineering and Sciences (IECBES), Sarawak, Malaysia, 8–10 December 2014; pp. 235–240. [Google Scholar]
- Wang, S.; Pohl, A.; Jaeschke, T.; Czaplik, M.; Köny, M.; Leonhardt, S.; Pohl, N. A novel ultra-wideband 80 GHz FMCW radar system for contactless monitoring of vital signs. In Proceedings of the 2015 37th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Milan, Italy, 25–29 August 2015; pp. 4978–4981. [Google Scholar]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ID | ||||||||
|---|---|---|---|---|---|---|---|---|
| 1 | 0.952 | 14 | 0.224 | 0.921 | 2.855 | 0.063 | 7.92 | 8.28 |
| 2 | 0.938 | –2 | 0.919 | 0.511 | 1.422 | 0.407 | 12.25 | 12.38 |
| 3 | 0.958 | 40 | 0.246 | 0.575 | 1.130 | 0.210 | 4.77 | 4.62 |
| 4 | 0.975 | 17 | 1.274 | 0.106 | 1.078 | 0.161 | 10.86 | 10.86 |
| 5 | 0.979 | –12 | 0.038 | 0.364 | 1.580 | 1.389 | 8.95 | 8.99 |
| 6 | 0.916 | 9 | 3.866 | 2.591 | 4.603 | 4.173 | 11.54 | 12.59 |
| 7 | 0.845 | 21 | 2.451 | 1.245 | 2.973 | 0.286 | 6.01 | 6.48 |
| 8 | 0.953 | 5 | 3.061 | 1.169 | 4.424 | 3.389 | 13.08 | 13.52 |
| 9 | 0.940 | 30 | 2.754 | 1.075 | 1.523 | 0.299 | 8.83 | 9.08 |
| 10 | 0.905 | 7 | 0.087 | 0.100 | 0.601 | 0.131 | 11.99 | 11.99 |
| 11 | 0.986 | 19 | 0.048 | 0.998 | 1.114 | 0.107 | 17.08 | 17.26 |
| 12 | 0.937 | 15 | 0.095 | 0.472 | 0.995 | 0.151 | 9.75 | 9.65 |
| 13 | 0.990 | -6 | 1.570 | 0.043 | 1.994 | 0.640 | 11.02 | 11.03 |
| 14 | 0.887 | 12 | 0.059 | 0.083 | 0.058 | 0.141 | 13.35 | 13.38 |
| 15 | 0.965 | 8 | 0.983 | 0.232 | 0.230 | 0.123 | 8.38 | 8.45 |
| 16 | 0.965 | 7 | 0.052 | 0.160 | 0.114 | 0.100 | 15.27 | 15.25 |
| 17 | 0.775 | 31 | 1.035 | 1.026 | 2.497 | 3.423 | 13.81 | 13.50 |
| 18 | 0.837 | 18 | 2.774 | 2.114 | 1.332 | 4.000 | 12.88 | 12.53 |
| 19 | 0.940 | 0 | 0.760 | 0.853 | 1.418 | 0.903 | 13.25 | 13.36 |
| 20 | 0.968 | 14 | 0.116 | 0.139 | 0.111 | 0.123 | 10.52 | 10.48 |
| 21 | 0.979 | 0 | 0.113 | 0.409 | 8.527 | 0.045 | 17.83 | 17.91 |
| 22 | 0.472 | 8 | 5.149 | 4.087 | 5.615 | 6.619 | 16.79 | 13.84 |
| 23 | 0.988 | 12 | 0.701 | 0.068 | 0.068 | 0.104 | 8.68 | 8.67 |
| 24 | 0.884 | 17 | 0.127 | 0.575 | 0.107 | 0.195 | 13.21 | 13.10 |
| 25 | 0.914 | 59 | 0.949 | 0.487 | 3.098 | 0.957 | 12.52 | 12.43 |
| 26 | 0.978 | 10 | 1.282 | 0.085 | 4.323 | 0.086 | 12.48 | 12.46 |
| 27 | 0.983 | 12 | 0.107 | 0.053 | 1.616 | 0.100 | 10.63 | 10.61 |
| 28 | 0.972 | 21 | 0.380 | 0.874 | 2.694 | 0.436 | 6.32 | 5.96 |
| 29 | 0.884 | 46 | 0.300 | 1.005 | 0.738 | 0.293 | 10.37 | 10.54 |
| 30 | 0.768 | 10 | 3.163 | 2.429 | 4.391 | 4.172 | 11.04 | 11.81 |
| Mean | 0.914 | 14.7 | 1.156 | 0.828 | 2.108 | 1.108 | 11.38 | 11.37 |
| Std. dev. | 0.103 | 14.9 | 1.352 | 0.919 | 1.971 | 1.722 | 3.15 | 3.03 |
| ID | F1 Score (%) | Sensitivity (%) | Precision (%) | TP | FP | FN | # R-Peaks ECG | # Pred. HB | Meas. Time (s) |
|---|---|---|---|---|---|---|---|---|---|
| 1 | 95.91 | 95.97 | 95.84 | 691 | 30 | 29 | 729 | 721 | 607.6 |
| 2 | 98.27 | 98.13 | 98.41 | 682 | 11 | 13 | 721 | 694 | 622.4 |
| 3 | 96.86 | 95.80 | 97.94 | 570 | 12 | 25 | 597 | 583 | 601.4 |
| 4 | 98.00 | 98.00 | 98.00 | 685 | 14 | 14 | 702 | 699 | 603.1 |
| 5 | 78.81 | 77.81 | 79.84 | 491 | 124 | 140 | 643 | 617 | 610.1 |
| 6 | 97.24 | 97.33 | 97.15 | 546 | 16 | 15 | 571 | 563 | 610.9 |
| 7 | 74.46 | 74.10 | 74.83 | 452 | 152 | 158 | 647 | 604 | 634.9 |
| 8 | 99.04 | 98.95 | 99.12 | 565 | 5 | 6 | 588 | 572 | 618.6 |
| 9 | 98.73 | 98.31 | 99.15 | 581 | 5 | 10 | 641 | 586 | 649.4 |
| 10 | 85.56 | 85.28 | 85.84 | 394 | 65 | 68 | 491 | 459 | 639.1 |
| 11 | 96.60 | 95.73 | 97.49 | 583 | 15 | 26 | 660 | 601 | 648.9 |
| 12 | 83.79 | 83.65 | 83.92 | 522 | 100 | 102 | 675 | 622 | 648.5 |
| 13 | 99.56 | 99.50 | 99.62 | 791 | 3 | 4 | 801 | 794 | 725.6 |
| 14 | 50.06 | 49.81 | 50.32 | 395 | 390 | 398 | 798 | 785 | 603.5 |
| 15 | 99.14 | 99.06 | 99.22 | 635 | 5 | 6 | 696 | 641 | 648.5 |
| 16 | 97.78 | 97.58 | 97.98 | 484 | 10 | 12 | 504 | 495 | 610.6 |
| 17 | 84.92 | 89.06 | 81.15 | 521 | 121 | 64 | 589 | 643 | 603.3 |
| 18 | 83.41 | 83.41 | 83.41 | 538 | 107 | 107 | 686 | 645 | 636.0 |
| 19 | 95.94 | 95.64 | 96.24 | 461 | 18 | 21 | 484 | 481 | 603.1 |
| 20 | 99.84 | 99.67 | 100.00 | 610 | 0 | 2 | 653 | 610 | 640.2 |
| 21 | 91.01 | 90.80 | 91.21 | 602 | 58 | 61 | 678 | 662 | 613.9 |
| 22 | 95.37 | 95.20 | 95.54 | 535 | 25 | 27 | 619 | 560 | 659.8 |
| 23 | 99.68 | 99.51 | 99.84 | 614 | 1 | 3 | 634 | 616 | 678.9 |
| 24 | 99.93 | 99.85 | 100.00 | 678 | 0 | 1 | 690 | 678 | 610.5 |
| 25 | 98.97 | 98.97 | 98.97 | 671 | 7 | 7 | 697 | 678 | 616.9 |
| 26 | 99.29 | 99.29 | 99.29 | 704 | 5 | 5 | 746 | 711 | 821.0 |
| 27 | 100.00 | 100.00 | 100.00 | 593 | 0 | 0 | 619 | 593 | 627.9 |
| 28 | 97.87 | 97.49 | 98.25 | 505 | 9 | 13 | 528 | 514 | 611.9 |
| 29 | 100.00 | 100.00 | 100.00 | 598 | 0 | 0 | 615 | 598 | 615.9 |
| 30 | 98.33 | 97.85 | 98.82 | 501 | 6 | 11 | 536 | 507 | 626.6 |
| Micro mean | 93.14% | 93.06% | 93.25% | 573.3 | 43.8 | 44.9 | 641.3 | 617.7 | 635.0 |
| Std. dev. | 10.74% | 10.72% | 10.82% | 94.1 | 78.8 | 79.1 | 82.3 | 82.2 | 44.2 |
| Macro mean | 92.82% | 92.73% | 92.90% |
| F1 Score (%) | Sensitivity (%) | Precision (%) | |
|---|---|---|---|
| Micro mean | 94.63 | 94.55 | 94.73 |
| Std. dev. | 7.14 | 7.07 | 7.29 |
| Macro mean | 94.72 | 94.65 | 94.79 |
| Number of Measured Subjects | Measured Time per Subject (min) | RMSE of Heart Rate (ms) | Correlation of Respiration Rate | |
|---|---|---|---|---|
| this work | 30 | 10 | 26.07 | 0.914 |
| [29] | 11 | >14 | 44.2 | – |
| [45] | 1 | 20 | >200 | – |
| [46] | 5 | 10 | 45 | – |
| [47] | 5 | 20 | >113.2 | – |
| [48] | 1 | 5 | – | 0.958 |
| [49] | 1 | 5 | – | 0.9198 |
| [50] | 10 | 1.7 | – | 0.45 a |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Michler, F.; Shi, K.; Schellenberger, S.; Steigleder, T.; Malessa, A.; Hameyer, L.; Neumann, N.; Lurz, F.; Ostgathe, C.; Weigel, R.; et al. A Clinically Evaluated Interferometric Continuous-Wave Radar System for the Contactless Measurement of Human Vital Parameters. Sensors 2019, 19, 2492. https://doi.org/10.3390/s19112492
Michler F, Shi K, Schellenberger S, Steigleder T, Malessa A, Hameyer L, Neumann N, Lurz F, Ostgathe C, Weigel R, et al. A Clinically Evaluated Interferometric Continuous-Wave Radar System for the Contactless Measurement of Human Vital Parameters. Sensors. 2019; 19(11):2492. https://doi.org/10.3390/s19112492
Chicago/Turabian StyleMichler, Fabian, Kilin Shi, Sven Schellenberger, Tobias Steigleder, Anke Malessa, Laura Hameyer, Nina Neumann, Fabian Lurz, Christoph Ostgathe, Robert Weigel, and et al. 2019. "A Clinically Evaluated Interferometric Continuous-Wave Radar System for the Contactless Measurement of Human Vital Parameters" Sensors 19, no. 11: 2492. https://doi.org/10.3390/s19112492