An IoT Based Architecture for Enhancing the Effectiveness of Prototype Medical Instruments Applied to Neurodegenerative Disease Diagnosis

 , , , ,
, , , , 
Abstract
:1. Motivation and Introduction
- the proposal of a novel IoT-based architecture addressing requirements of prototype medical instruments, with the following characteristics: low-cost; based on well-accepted, secure, open and interoperable message oriented solutions; and able to include other information coming from ancillary sensors;
- the identification and selection of formal performance metrics for the characterization of the real-time behavior of the proposed architecture;
- the implementation of a testbed with both local and cloud servers, in order to provide close-to-reality results;
- an experimental measurement campaign for the characterization of the real-time behavior varying the location of the servers and the size of the exchanged information.
2. Early Neurodegenerative Disease Diagnosis
2.1. Transcranial Magnetic Stimulation for Early Neurodegenerative Disease Diagnosis
2.2. Diagnosis Protocol with Transcranical Magnetic Stimulation
- NMM: the number of distinct values of TISI that should be used in each cycle of the diagnosis phase associated with MM trains;
- a set of NMM TISI;
- NEM: the number of distinct values of TISI that should be used in each cycle of the diagnosis phase associated with EM trains;
- a set of NEM TISI;
- NREF: the number of reference stimuli, i.e., REF trains, that should be issued in each cycle of the diagnosis phase;
- TITI,MIN, TITI,MAX: the range of TITI to use in the diagnosis phase, to ensure aperiodic stimulation for optimal patient response;
- NC: the number of times that each cycle should be repeated in the diagnosis phase.
2.3. Advantages Offered by Cloud Services
3. The Proposed Cloud Architecture
3.1. The MQTT and AMQP Protocols
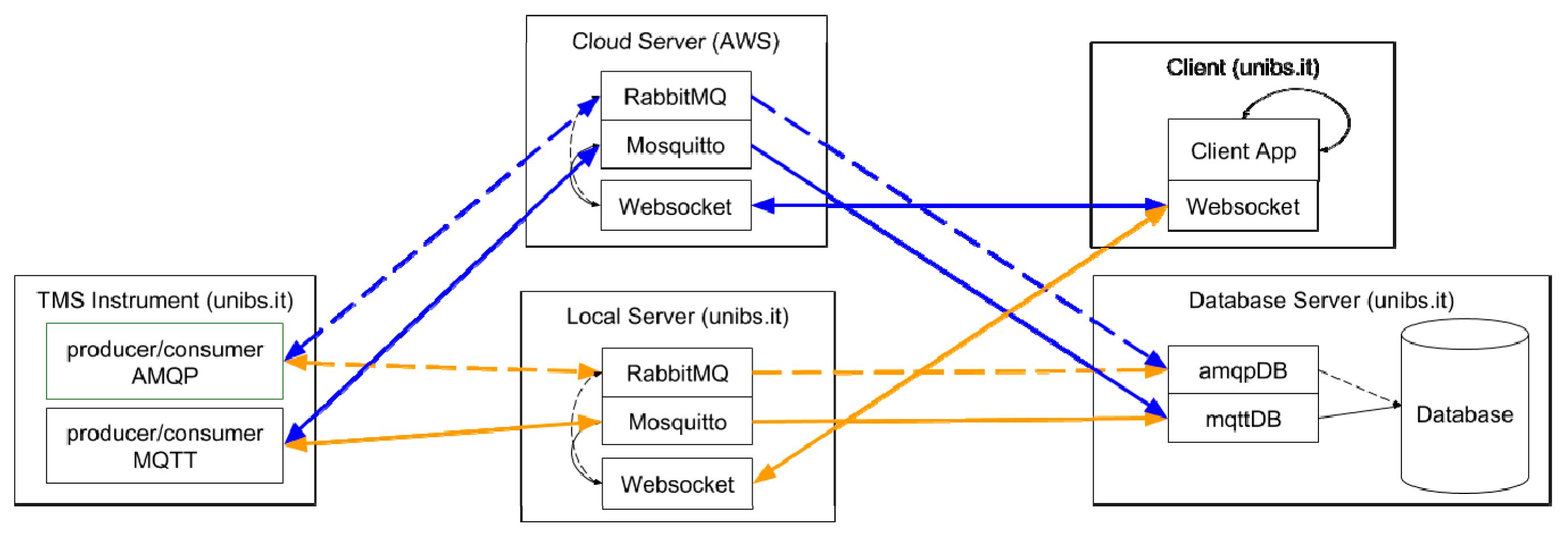
3.2. The Proposed Architecture
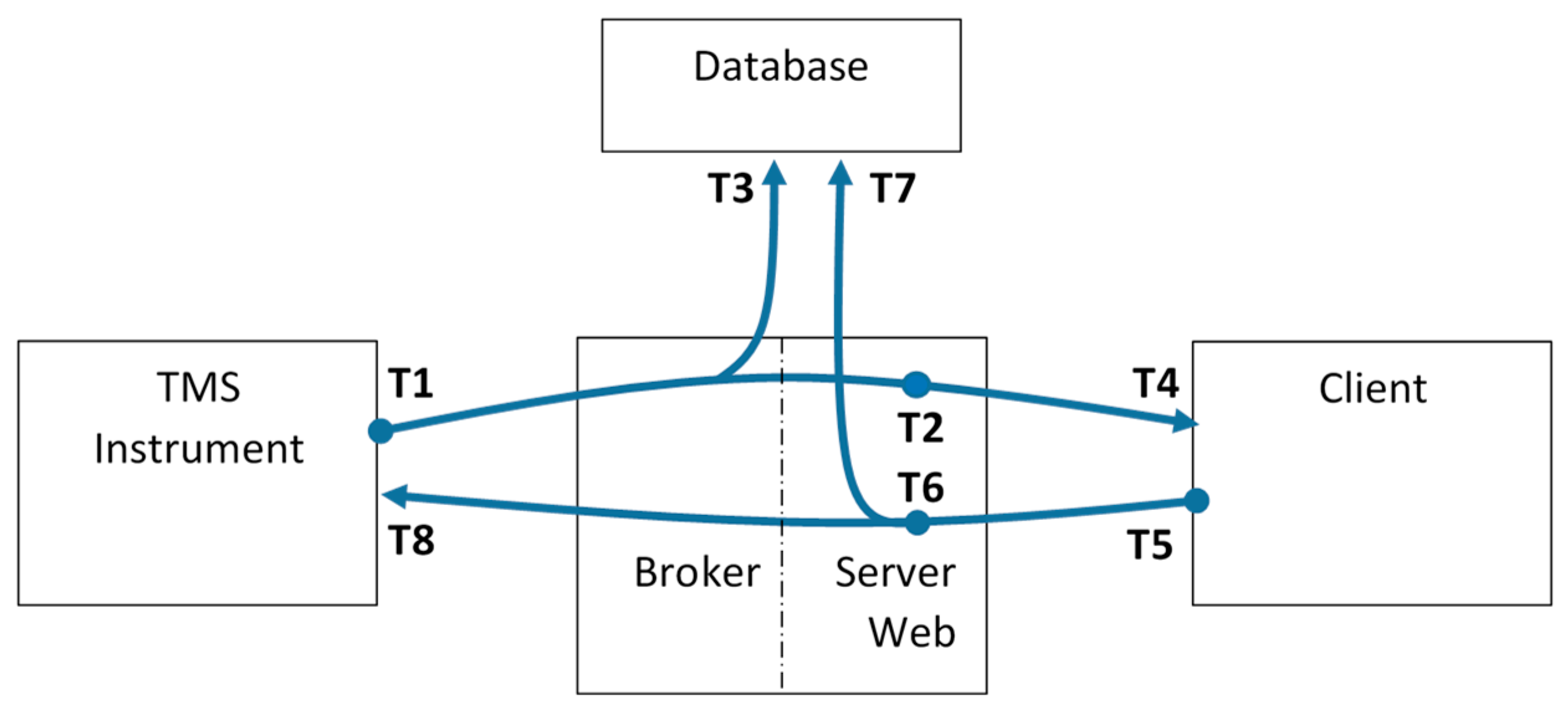
3.3. The Proposed Metrics for Performance Evaluation
- T1: this timestamp is assigned by the instruments when a new set of data is ready to be sent to the architecture.
- T2: this timestamp is assigned by the architecture when a new set of data arrives to the Web Server coming from the instrument.
- T3: this timestamp is assigned by the database when a new set of data coming from the instruments is permanently stored in its data table.
- T4: this timestamp is assigned by the Client when a new set of data arrives through the websocket.
- T5: this timestamp is assigned by the Client when a new command leaves the Client addressed to the architecture.
- T6: this timestamp is assigned by the architecture when a new set of data arrives to the Web Server coming from the Client.
- T7: this timestamp is assigned by the database when a new set of data coming from the Client is permanently stored in its data table.
- T8: this timestamp is assigned by the instrument when a command arrives through the architecture.
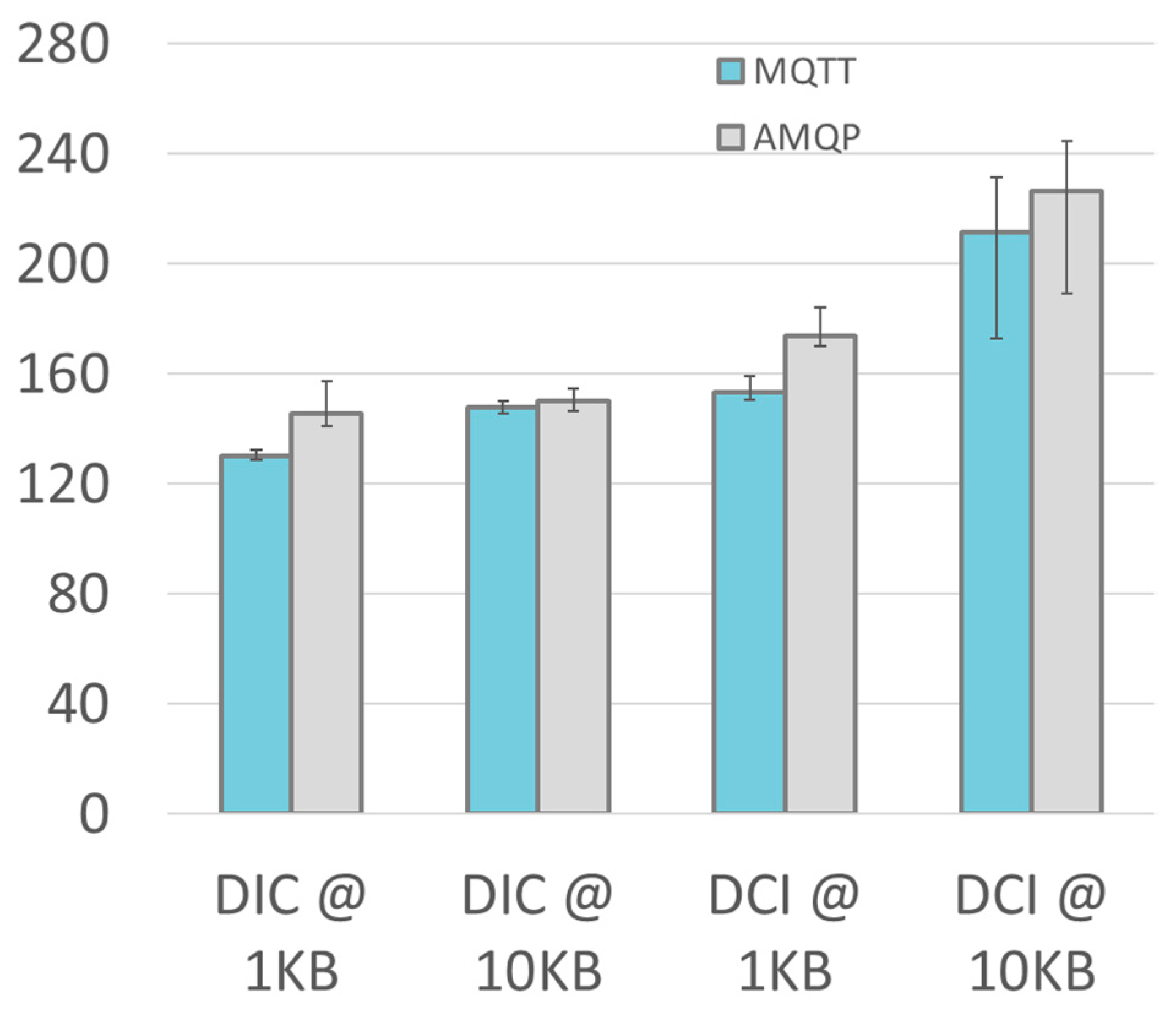
- DIC = T4–T1: the overall end-to-end delay from the TMS instrument to the remote Client.
- DIS = T2–T1: the end-to-end delay from the TMS instrument to the Web Server.
- DID = T3–T1: the end-to-end delay from the TMS instruments to the Database.
- DCI = T8–T5: the reverse overall end-to-end delay from the remote Client to the TMS instrument.
- DCS = T6–T5: the end-to end delay from the Client to the Web Server.
- DCD = T7–T5: the end-to-end delay from the Client to the Database.
4. Validation and Experimental Results
4.1. The Prototype Medical Instrument for Neurodegenerative Disease Diagnosis
- protocol invariant data, as the amplitude of the stimuli, AmTS, AmCS, AeCS; each of which is one byte wide;
- an array of NTOT records, each of which specifying the stimulus type (1 byte), the TISI value (1 byte), the TITI value (1 byte), and the calculated MEP value (2 byte).
4.2. Experimental Setup
- The TMS Instrument is based on a Raspberry Pi 2 single board computer, as described in Section 4.1. The raspberry Pi 2 hosts a quad-core 64 bit ARM processor (clock frequency 1.2 GHz), 1 GB of RAM, four USB ports, a LAN interface and HDMI video connection; it runs the Linux-based Raspbian OS. The TMS Instrument role is to initiate the experiment, sending the first data message. It also terminate the experiment, receiving the Client command. A custom transport layer abstracting the communication libraries for both AMQP and MQTT has been implemented in Python; in particular, the transport layer uses the Paho library for MQTT and the Pika library for AMQP.
- The Client represents the remote operator that needs to interact with the prototype TMS Instrument. In this experiment, the simple Client role is to receive data from the instrument and loopback them into a command for the instrument. It has been implemented with an embedded device to introduce the minimum overhead. The device is a Siemens IOT2040 (based on an Intel Quark × 1020 (+Secure Boot) processor and hosting 1 GB of RAM, two Ethernet ports and two RS232/485 interfaces, and a battery-backed Real Time Calendar. It runs a customized Yocto Linux distribution. The entire software at client side is written in Javascript and runs in Node.Js, a well-accepted approach in IoT solutions that ensures portability on different platforms. The Client is located inside the domain of the University of Brescia.
- The Local Server is a machine specifically created for the experiments. It is located inside the domain of the University of Brescia. It is a VMware (ESXi 6.5) virtual machine (VM); the VM is hosted on a DELL PowerEdge R630 (Intel Xeon E5–2 core, 128 GB RAM, 4 × 1 Gbps Ethernet), one of the facility available in the University of Brescia eLUX laboratory [40]. The VM has a single CPU, 2 GB of RAM and has CentOS7 as guest operating System (OS). It hosts the RabbitMQ AMQP broker, with the HTTP management plugin enabled, and the Mosquitto MQTT broker. The local server hosts also the websocket server, which is a simple Python 3.6 program. It uses the Tornado web server websocket implementation to communicate with the Client and it runs the same custom transport layer used in the TMS Instrument (which, as previously stated, leverages the Paho library for MQTT and the Pika library for AMQP).
- The Cloud Server is an instance of the Amazon AWS EC2 t2.micro virtual machine with a single CPU and 1 GB of RAM. The Cloud Server is hosted by the US East (Ohio) Amazon Web Service (AWS) data center and it has been specifically created for the experiments. The software configuration of the Cloud Server is identical to the Local Server one; a minimal effort is required for migration from Local to cloud Server.
- The Database Server is located inside the domain of the University of Brescia. It is a VMware (ESXi 6.5) VM; it is hosted on a Syneto Ultra 205 hyperconverged system (Intel Xeon E5–6-core, 64 GB RAM, 4 × 1 Gbps Ethernet), another facility available in the eLUX laboratory. The VM has 4 CPU, 16 GB RAM and has CentOS7 as guest OS. It hosts the different databases (including MariaDB, Influxdb, PosgreSQL) that collect the laboratory data. For the experiments of this work, the Influxdb, an open-source database purposely-designed for time series storage, has been chosen.
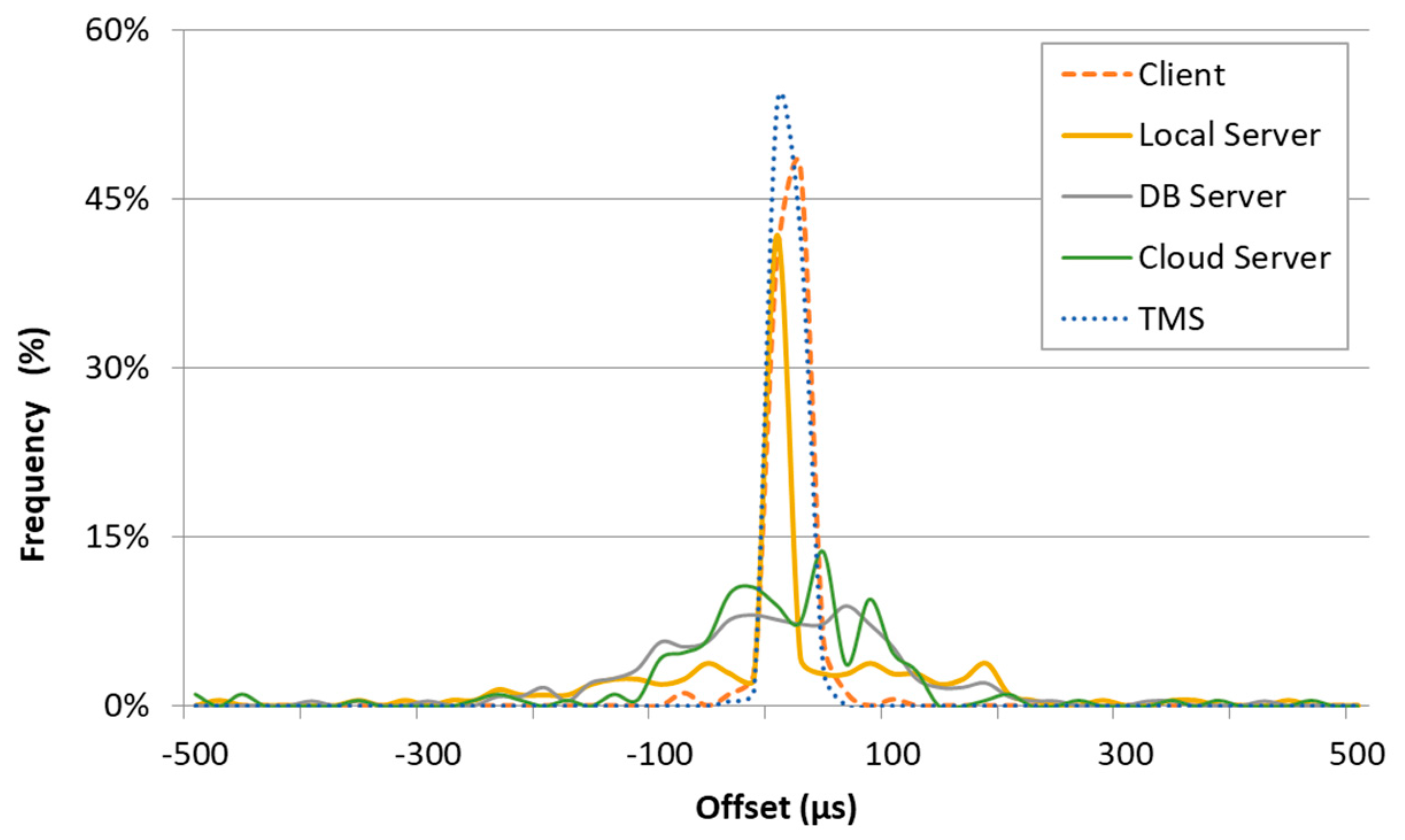
4.3. Estimation of Measurement Uncertainty
4.4. Experimental Results
- interval between data transfer (1 s or 10 s);
- location of Broker and Web Server (Local Server or Cloud Server);
- the used message protocol (AMQP or MQTT).
5. Conclusions and Future Development
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Khaitan, S.K.; McCalley, J.D. Design Techniques and Applications of Cyberphysical Systems: A Survey. IEEE Syst. J. 2015, 9, 350–365. [Google Scholar] [CrossRef]
- Al-Fuqaha, A.; Guizani, M.; Mohammadi, M.; Aledhari, M.; Ayyash, M. Internet of Things: A Survey on Enabling Technologies, Protocols, and Applications. IEEE Commun. Surv. Tutor. 2015, 17, 2347–2376. [Google Scholar] [CrossRef]
- Crema, C.; Depari, A.; Flammini, A.; Sisinni, E.; Vezzoli, A.; Bellagente, P. Virtual Respiratory Rate Sensors: An Example of a Smartphone-Based Integrated and Multiparametric mHealth Gateway. IEEE Trans. Instrum. Meas. 2017, 66, 2456–2463. [Google Scholar] [CrossRef]
- Depari, A.; Flammini, A.; Sisinni, E.; Vezzoli, A. A wearable smartphone-based system for electrocardiogram acquisition. In Proceedings of the Medical Measurements and Applications (MeMeA) 2014 IEEE International Symposium, Lisbon, Portugal, 11–12 June 2014; pp. 1–6. [Google Scholar]
- Zhang, X.; Li, J.; Liu, Y.; Zhang, Z.; Wang, Z.; Luo, D.; Zhou, X.; Zhu, M.; Salman, W.; Hu, G.; et al. Design of a Fatigue Detection System for High-Speed Trains Based on Driver Vigilance Using a Wireless Wearable EEG. Sensors 2017, 17, 486. [Google Scholar] [CrossRef] [PubMed]
- Zia ur Rehman, M.; Waris, A.; Gilani, S.O.; Jochumsen, M.; Niazi, I.K.; Jamil, M.; Farina, D.; Kamavuako, E.N. Multiday EMG-Based Classification of Hand Motions with Deep Learning Techniques. Sensors 2018, 18, 2497. [Google Scholar] [CrossRef] [PubMed]
- Ivanov, R.; Weimer, J.; Lee, I. Context-Aware Detection in Medical Cyber-Physical Systems. In Proceedings of the International Conference on Cyber-Physical Systems (ICCPS), Porto, Portugal, 11–13 April 2018. [Google Scholar]
- Jezewski, J.; Pawlak, A.; Wróbel, J.; Horoba, K.; Penkala, P. Towards a medical cyber-physical system for home telecare of high-risk pregnancy. IFAC-PapersOnLine 2015, 48, 466–473. [Google Scholar] [CrossRef]
- Lee, I.; Sokolsky, O.; Chen, S.; Hatcliff, J.; Jee, E.; Kim, B.; King, A.L.; Mullen-Fortino, M.; Park, S.; Roederer, A.; et al. Challenges and Research Directions in Medical Cyber–Physical Systems. Proc. IEEE 2012, 100, 75–90. [Google Scholar]
- Kocabas, O.; Soyata, T.; Aktas, M.K. Emerging Security Mechanisms for Medical Cyber Physical Systems. IEEE/ACM Trans. Comput. Biol. Bioinform. 2016, 13, 401–416. [Google Scholar] [CrossRef] [PubMed]
- Dey, N.; Ashour, A.S.; Shi, F.; Fong, S.J.; Tavares, J.; Manuel, R.S. Medical cyber-physical systems: A survey. J. Med. Syst. 2018, 42, 74. [Google Scholar] [CrossRef]
- Li, T.; Cao, J.; Liang, J.; Zheng, J. Towards context-aware medical cyber-physical systems: Design methodology and a case study. Cyber Phys. Syst. 2015, 1, 5–23. [Google Scholar] [CrossRef]
- Padovani, A.; Benussi, A.; Cantoni, V.; Dell’Era, V.; Cotelli, M.S.; Caratozzolo, S.; Turrone, R.; Rozzini, L.; Alberici, A.; Altomare, D.; et al. Diagnosis of Mild Cognitive Impairment Due to Alzheimer’s Disease with Transcranial Magnetic Stimulation. J. Alzheimer’s Dis. 2018, 65, 221–230. [Google Scholar] [CrossRef]
- Crema, C.; Depari, A.; Sisinni, E.; Benussi, A.; Borroni, B.; Padovani, A. Embedded platform-based system for early detection of Alzheimer disease through transcranial magnetic stimulation. In Proceedings of the 2018 IEEE Sensors Applications Symposium (SAS), Seoul, Korea, 12–14 March 2018; pp. 350–355. [Google Scholar]
- Francis, P.T.; Palmer, A.M.; Snape, M.; Wilcock, G.K. The cholinergic hypothesis of Alzheimer’s disease: A review of progress. J. Neurol. Neurosurg. Psychiatry 1999, 66, 137–147. [Google Scholar] [CrossRef] [PubMed]
- Levenga, J.; Krishnamurthy, P.; Rajamohamedsait, H.; Wong, H.; Franke, T.F.; Cain, P.; Sigurdsson, E.M.; Hoeffer, C.A. Tau pathology induces loss of GABAergic interneurons leading to altered synaptic plasticity and behavioral impairments. Acta Neuropathol. Commun. 2013, 1, 34. [Google Scholar] [CrossRef] [PubMed]
- Tokimura, H.; Di Lazzaro, V.; Tokimura, Y.; Oliviero, A.; Profice, P.; Insola, A.; Mazzone, P.; Tonali, P.; Rothwell, J.C. Short latency inhibition of human hand motor cortex by somatosensory input from the hand. J. Physiol. 2000, 523, 503–513. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kujirai, T.; Caramia, M.D.; Rothwell, J.C.; Day, B.L.; Thompson, P.D.; Ferbert, A.; Wroe, S.; Asselman, P.; Marsden, C.D. Corticocortical inhibition in human motor cortex. J. Physiol. 1993, 471, 501–519. [Google Scholar] [CrossRef]
- Ziemann, U.; Rothwell, J.C.; Ridding, M.C. Interaction between intracortical inhibition and facilitation in human motor cortex. J. Physiol. 1996, 496, 873–881. [Google Scholar] [CrossRef]
- Benussi, A.; Di Lorenzo, F.; Dell’Era, V.; Cosseddu, M.; Alberici, A.; Caratozzolo, S.; Cotelli, M.S.; Micheli, A.; Rozzini, L.; Depari, A.; et al. Transcranial magnetic stimulation distinguishes Alzheimer’s disease from Frontotemporal Dementia. Neurology 2017, 89, 665–672. [Google Scholar] [CrossRef]
- Blumrosen, G.; Avisdris, N.; Kupfer, R.; Rubinsky, B. C-SMART: Efficient seamless cellular phone based patient monitoring system. In Proceedings of the 2011 IEEE International Symposium on a World of Wireless, Mobile and Multimedia Networks, Lucca, Italy, 20–24 June 2011; pp. 1–16. [Google Scholar]
- Bellagente, P.; Depari, A.; Ferrari, P.; Flammini, A.; Rinaldi, S.; Sisinni, E. M3IoT-Message-oriented middleware for M-health Internet of Things: Design and validation. In Proceedings of the 2018 IEEE International Instrumentation and Measurement Technology Conference (I2MTC), Houston, TX, USA, 14–17 May 2018; pp. 1213–1218. [Google Scholar]
- Larson, B.R.; Zhang, Y.; Barrett, S.C.; Hatcliff, J.; Jones, P.L. Enabling Safe Interoperation by Medical Device Virtual Integration. IEEE Des. Test 2015, 32, 74–88. [Google Scholar] [CrossRef]
- Plourde, J.; Arney, D.; Goldman, J.M. OpenICE: An open, interoperable platform for medical cyber-physical systems. In Proceedings of the 2014 ACM/IEEE International Conference on Cyber-Physical Systems (ICCPS), Berlin, Germany, 14–17 April 2014; p. 221. [Google Scholar]
- Ivanov, R.; Nguyen, H.; Weimer, J.; Sokolsky, O.; Lee, I. OpenICE-lite: Towards a Connectivity Platform for the Internet of Medical Things. In Proceedings of the 2018 IEEE 21st International Symposium on Real-Time Distributed Computing (ISORC), Singapore, 29–31 May 2018; pp. 103–106. [Google Scholar]
- Mahadevan, P.; Krioukov, D.; Fomenkov, M.; Huffaker, B.; Dimitropoulos, X.; Claffy, K.; Vahdat, A. The Internet AS-Level Topology: Three Data Sources and One Definitive Metric. ACM SIGCOMM Comput. Commun. Rev. 2006, 36, 17–26. [Google Scholar] [CrossRef]
- Tramarin, F.; Narduzzi, C.; Vitturi, S.; Bertocco, M. A Calibrated Test-Set for Measurement of Access-Point Time Specifications in Hybrid Wired/Wireless Industrial Communication. Information 2018, 9, 122. [Google Scholar] [CrossRef]
- De Vito, L.; Rapuano, S.; Tomaciello, L. One-Way Delay Measurement: State of the Art. IEEE Trans. Instrum. Meas. 2008, 57, 2742–2750. [Google Scholar] [CrossRef]
- Ferrari, P.; Sisinni, E.; Brandao, D.; Rocha, M. Evaluation of communication latency in industrial IoT applications. In Proceedings of the 2017 IEEE International Workshop on Measurements and Networking (M&N), Naples, Italy, 27–29 September 2017; pp. 17–22. [Google Scholar]
- Ferrari, P.; Flammini, A.; Rinaldi, S.; Sisinni, E. Evaluation of Communication Delay in IoT Applications Based on OPC UA. In Proceedings of the 2018 Workshop on Metrology for Industry 4.0 and IoT, Brescia, Italy, 16–18 April 2018; pp. 225–230. [Google Scholar]
- Fernandes Carvalho, D.; Ferrari, P.; Flammini, A.; Sisinni, E. A Test Bench for Evaluating Communication Delays in LoRaWAN Applications. In Proceedings of the 2018 Workshop on Metrology for Industry 4.0 and IoT, Brescia, Italy, 16–18 April 2018; pp. 249–254. [Google Scholar]
- Silva, D.; Oliveira, G.; Silva, I.; Ferrari, P.; Sisinni, E. Latency Evaluation for MQTT and WebSocket Protocols: An Industry 4.0 Perspective. In Proceedings of the 2018 IEEE Symposium on Computers and Communications (ISCC), Natal, Brazil, 25–28 June 2018; pp. 1–6. [Google Scholar]
- Ferrari, P.; Flammini, A.; Rinaldi, S.; Sisinni, E.; Maffei, D.; Malara, M. Impact of Quality of Service on Cloud Based Industrial IoT Applications with OPC UA. Electronics 2018, 7, 109. [Google Scholar] [CrossRef]
- Ferrari, P.; Flammini, A.; Sisinni, E.; Rinaldi, S.; Brandao, D.; Rocha, M. Delay Estimation of Industrial IoT Applications Based on Messaging Protocols. IEEE Trans. Instrum. Meas. 2018, 67, 2188–2199. [Google Scholar] [CrossRef]
- Tobagi, F.A.; Markopoulou, A.P.; Karam, M.J. Is the Internet ready for VoIP? In Proceedings of the IWDC 2002, Calcutta, India, 28–31 December 2002; pp. 49–57. [Google Scholar]
- Collina, M.; Bartolucci, M.; Vanelli-Coralli, A.; Corazza, G.E. Internet of Things application layer protocol analysis over error and delay prone links. In Proceedings of the 7th Advanced Satellite Multimedia Systems Conference and the 13th Signal Processing for Space Communications Workshop (ASMS/SPSC), Livorno, Italy, 8–10 September 2014; pp. 398–404. [Google Scholar]
- Govindan, K.; Azad, A.P. End-to-end service assurance in IoT MQTT-SN. In Proceedings of the 12th Annual IEEE Consumer Communications and Networking Conference (CCNC), Las Vegas, NV, USA, 9–12 January 2015; pp. 290–296. [Google Scholar]
- Mijovic, S.; Shehu, E.; Buratti, C. Comparing application layer protocols for the Internet of Things via experimentation. In Proceedings of the IEEE 2nd International Forum on Research and Technologies for Society and Industry Leveraging a better tomorrow (RTSI), Bologna, Italy, 7–9 September 2016; pp. 1–5. [Google Scholar]
- Pereira, C.; Pinto, A.; Ferreira, D.; Aguiar, A. Experimental Characterisation of Mobile IoT Application Latency. IEEE Internet Things J. 2017, PP, 1. [Google Scholar]
- Rinaldi, S.; Pasetti, M.; Sisinni, E.; Bonafini, F.; Ferrari, P.; Rizzi, M.; Flammini, A. On the Mobile Communication Requirements for the Demand-Side Management of Electric Vehicles. Energies 2018, 11, 1220. [Google Scholar] [CrossRef]
- Sherman, J.A.; Levine, J. Usage Analysis of the NIST Internet Time Service. J. Res. Natl. Inst. Stand. Technol. Gaithersburg 2016, 121, 33–46. [Google Scholar] [CrossRef]
- Angrisani, L.; Capriglione, D.; Ferrigno, L.; Miele, G. Internet Protocol Packet Delay Variation measurements in communication networks: How to evaluate measurement uncertainty? Meas. J. Int. Meas. Conf. 2013, 46, 2099–2109. [Google Scholar] [CrossRef]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Device | usn | ||
|---|---|---|---|
| TMS Instrument | 0.009 | 0.000 | 0.009 |
| Local Server | 0.172 | 0.007 | 0.172 |
| Cloud Server | 0.278 | 0.013 | 0.278 |
| DB Server | 0.126 | 0.011 | 0.125 |
| Client | 0.018 | 0.001 | 0.018 |
| Device | utn | ||
|---|---|---|---|
| TMS Instrument | 1.0 | 1.4 | 0.2 |
| Local Server | 0.7 | 1.0 | 0.1 |
| Cloud Server | 0.8 | 1.1 | 0.3 |
| DB Server | 0.8 | 1.0 | 0.3 |
| Client | 3.1 | 4.3 | 0.9 |
| Metric | Device A | Device B | ||
|---|---|---|---|---|
| Local | TMS to Client | TMS Instrument | Client | 3.3 |
| TMS to Server | TMS Instrument | Local Server | 1.2 | |
| TMS to Database | TMS Instrument | DB Server | 1.3 | |
| Client to TMS | Client | TMS Instrument | 3.3 | |
| Client to Server | Client | Local Server | 3.2 | |
| Client to Database | Client | DB Server | 3.2 | |
| Cloud | TMS to Client | TMS Instrument | Client | 3.3 |
| TMS to Server | TMS Instrument | AWS Server | 1.3 | |
| TMS to Database | TMS Instrument | DB Server | 1.3 | |
| Client to TMS | Client | TMS Instrument | 3.3 | |
| Client to Server | Client | Cloud Server | 3.2 | |
| Client to Database | Client | DB Server | 3.2 |
| Metric | MQTT @ 1 s | AMQP @ 1 s | MQTT @ 10 s | AMQP @ 10 s | |||||
|---|---|---|---|---|---|---|---|---|---|
| Mean | 95 perc. | Mean | 95 perc. | Mean | 95 perc. | Mean | 95 perc. | ||
| Local | DIC | 4.8 | 5.4 | 7.0 | 7.6 | 6.3 | 6.3 | 6.2 | 6.5 |
| DIS | 0.5 | 0.9 | 2.0 | 2.3 | 1.7 | 1.8 | 2.0 | 2.3 | |
| DID | 2.3 | 3.5 | 3.8 | 4.3 | 3.4 | 4.1 | 3.8 | 4.4 | |
| DCI | 25.7 | 30.9 | 27.8 | 34.6 | 26.2 | 33.5 | 25.0 | 29.8 | |
| DCS | 22.1 | 25.4 | 24.1 | 30.6 | 22.7 | 26.4 | 21.2 | 25.2 | |
| DCD | 25.4 | 30.7 | 28.6 | 35.5 | 28.2 | 37.3 | 25.9 | 30.8 | |
| Cloud | DIC | 144.6 | 158.9 | 132.5 | 134.6 | 145.0 | 164.3 | 141.8 | 143.0 |
| DIS | 71.4 | 71.9 | 59.8 | 60.3 | 71.9 | 72.9 | 72.0 | 72.7 | |
| DID | 141.9 | 147.7 | 128.1 | 129.0 | 141.1 | 148.9 | 140.3 | 141.9 | |
| DCI | 164.3 | 189.4 | 168.5 | 176.7 | 165.9 | 186.3 | 164.0 | 183.3 | |
| DCS | 93.7 | 111.8 | 97.5 | 103.8 | 94.1 | 110.6 | 94.5 | 115.3 | |
| DCD | 164.3 | 189.5 | 169.3 | 178.2 | 165.8 | 186.8 | 166.5 | 185.5 | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Depari, A.; Fernandes Carvalho, D.; Bellagente, P.; Ferrari, P.; Sisinni, E.; Flammini, A.; Padovani, A. An IoT Based Architecture for Enhancing the Effectiveness of Prototype Medical Instruments Applied to Neurodegenerative Disease Diagnosis. Sensors 2019, 19, 1564. https://doi.org/10.3390/s19071564
Depari A, Fernandes Carvalho D, Bellagente P, Ferrari P, Sisinni E, Flammini A, Padovani A. An IoT Based Architecture for Enhancing the Effectiveness of Prototype Medical Instruments Applied to Neurodegenerative Disease Diagnosis. Sensors. 2019; 19(7):1564. https://doi.org/10.3390/s19071564
Chicago/Turabian StyleDepari, Alessandro, Dhiego Fernandes Carvalho, Paolo Bellagente, Paolo Ferrari, Emiliano Sisinni, Alessandra Flammini, and Alessandro Padovani. 2019. "An IoT Based Architecture for Enhancing the Effectiveness of Prototype Medical Instruments Applied to Neurodegenerative Disease Diagnosis" Sensors 19, no. 7: 1564. https://doi.org/10.3390/s19071564