Health Promotion for Childhood Obesity: An Approach Based on Self-Tracking of Data


 , ,
, , 
Abstract
1. Introduction
- RQ1. What is an appropriate multidimensional QS model for promoting healthy habits in children?
- RQ2. How might a recommender system complement the QS model to help the user select the appropriate actions and the time to do them?
- RQ3. How can the User eXperience (UX) of using a QS approach for children be improved?
- RQ4. How does a gamified technology-based intervention impact the health of children?
2. State of the Art
- Physical activities (distance, steps, calories, repetitions, etc.)
- Diet (calories consumed, satiety, fat, etc.)
- Psychological states (happiness, anxiety, depression, etc.)
- Mental and cognitive states (patience, creativity, reaction, memory, etc.)
- Environmental variables (location, noise, weather, etc.)
- Situational variables (context, time, date, etc.)
- Social variables (influence, charisma, status, etc.).
2.1. Quantified Self for Health
2.2. Wearables for Childen and Digital Biopedagogical Platforms
2.3. Quantified Self and User Modeling
- Attitudes: feelings, states of mind, and desires for a particular item, event, or tendency;
- Behaviors: activities that happen at a precise moment in time (like tasks or actions), or habits (series of repetitive acts);
- Emotions: moods (emotive trends over a prolonged period); emotions (over a short interval);
- Mental states: cognitive functions (for instance, memory, attention) regarding an instant and cognitive skills associated with their performance over time, such as an increase or decrease of memory health or spatial orientation.
3. Study on Enhancing Healthy Habits in Children
The PROVITAO Project
- -
- Inclusion criteria:
- *
- Children aged between 6 and 12 years with obesity, using as the criterion a BMI higher than PC95.
- *
- Children attending HUC’s pediatric outpatient clinics (Phase 1).
- *
- Students enrolled in the public school participating in this project (Phase 2)
- -
- Exclusion criteria:
- *
- Children who did not have the necessary networking technologies at home (computer and Internet) and television (experimental group only). The project provided the remainder of the technological tools required for the intervention at home (Kinect sensor, Wii console, and Wii balance board) and in the group sessions.
- *
- Children whose parents did not wish to participate in the project.
- *
- Children with cognitive impairment preventing them from participating in the project.
- *
- Participation during the preceding 12 months in a clinical trial.
4. Multidimensional QS Model for Promoting Healthy Habits
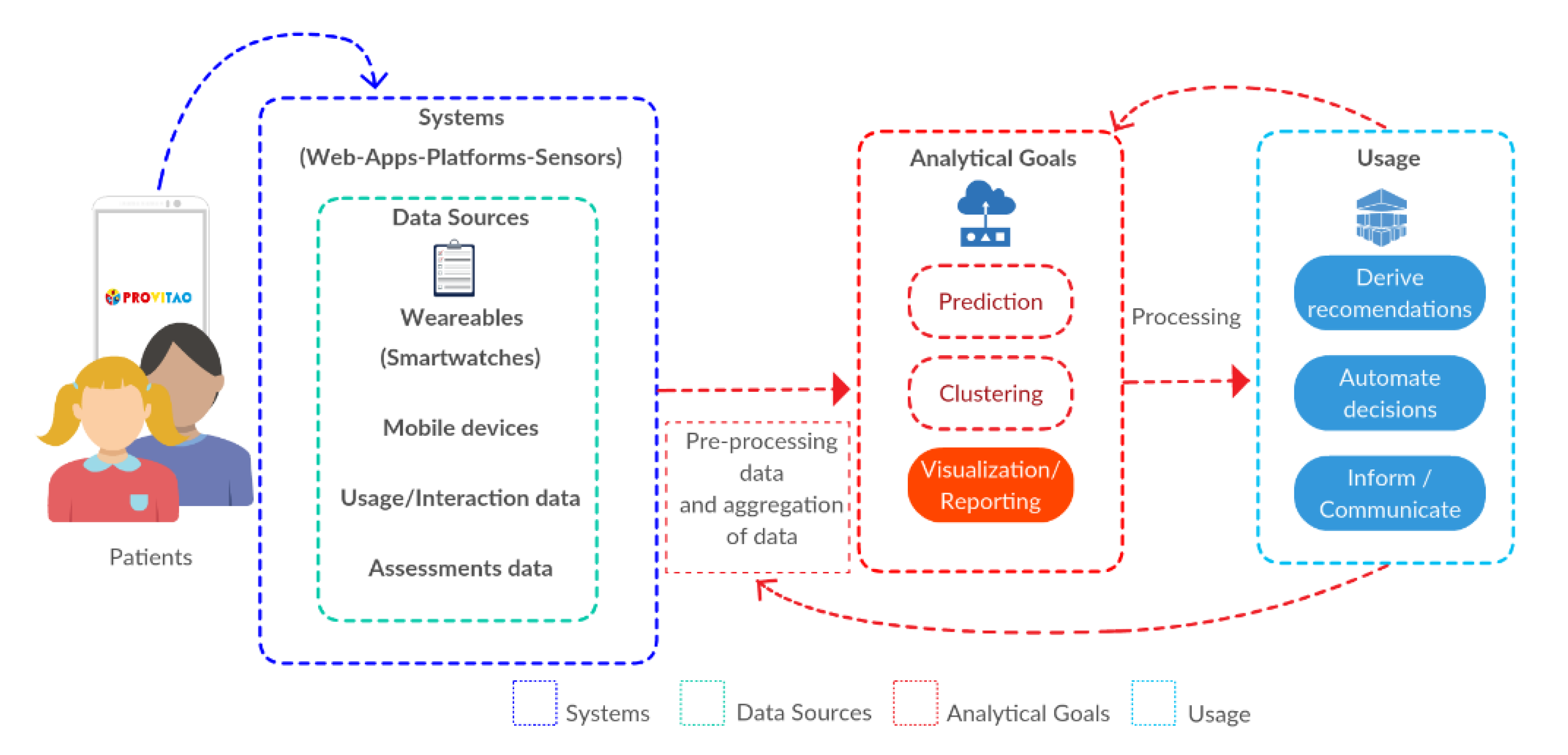
- Data sources (DS): We propose gathering data from multiple sources of information, including wearable sensors, mobile sensors, applications, digital activity records, and sentiment analysis applied to written communications.
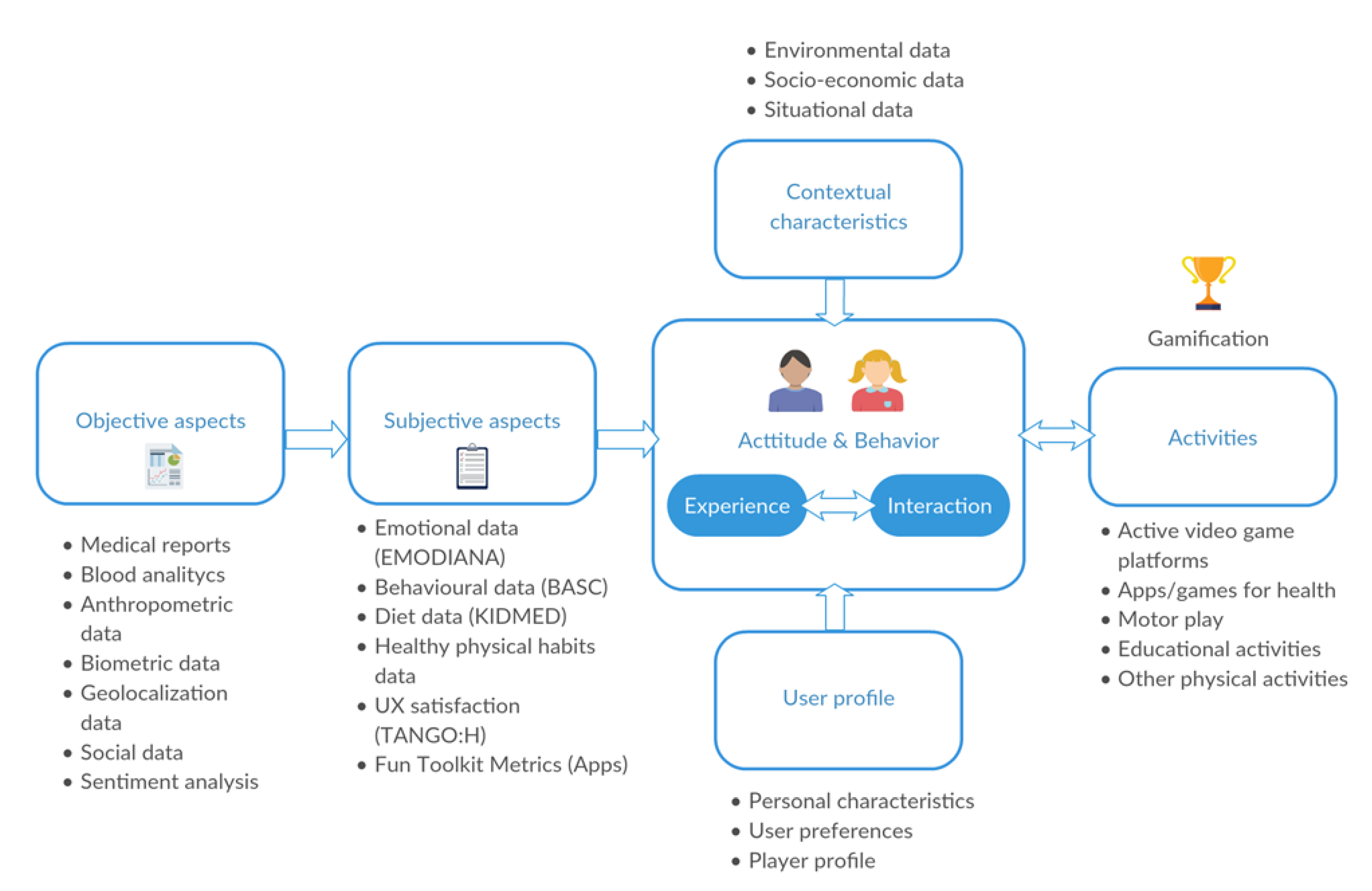
- QS user model (QSUM): We define a QS user model that is continuously updated using the information mentioned above. The QS user model includes variables grouped into several aspects, such as attitudes, behaviors, emotions, and cognitive functions.
- Activity recommender system (ARS): Given the QS user model and the contextual information gathered about the user, a recommendation can be selected at any time from a predefined set of actions. To build the recommendation system, advanced data mining and machine learning techniques are applied [50]. The actions include engaging in a particular sport, participating in an active game, learning and reinforcing knowledge about healthy habits, and motivation enhancement tasks.
- UX Module (UXM): We propose a design for motivation enhancement tasks, although this design is itself an open research problem. It has been shown that adults who have access to data collected during their physical exercise sessions improve their performance and adherence. Consequently, we propose a means to present progress data to children to maximize their response. Due to the large and varied sources of data used in this project (biometric and anthropometric data, interaction logs, tests, medical reports, etc.), we define a QS user model and other models to interact with the user.
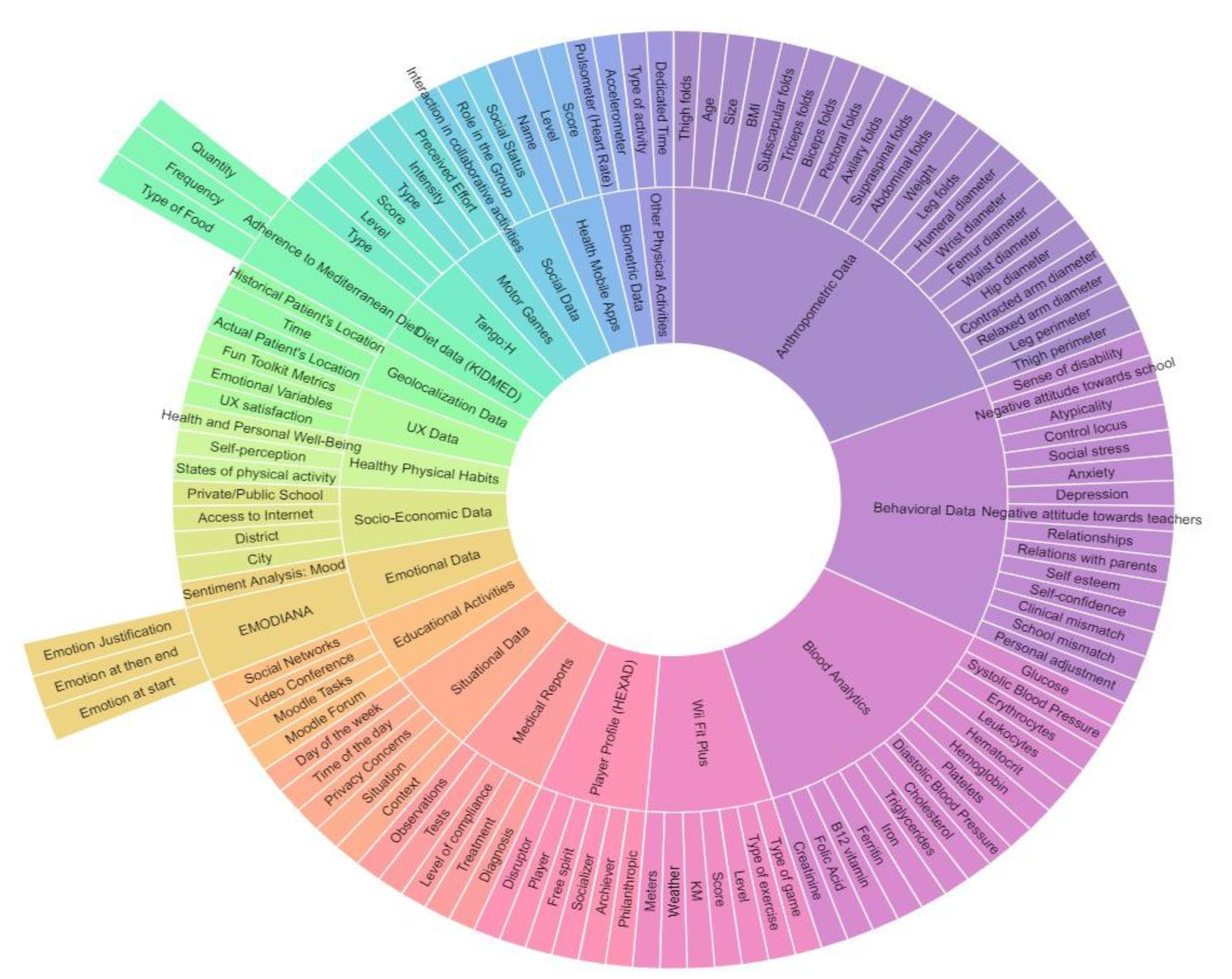
4.1. Data Sources
4.2. QS User Model (QSUM)
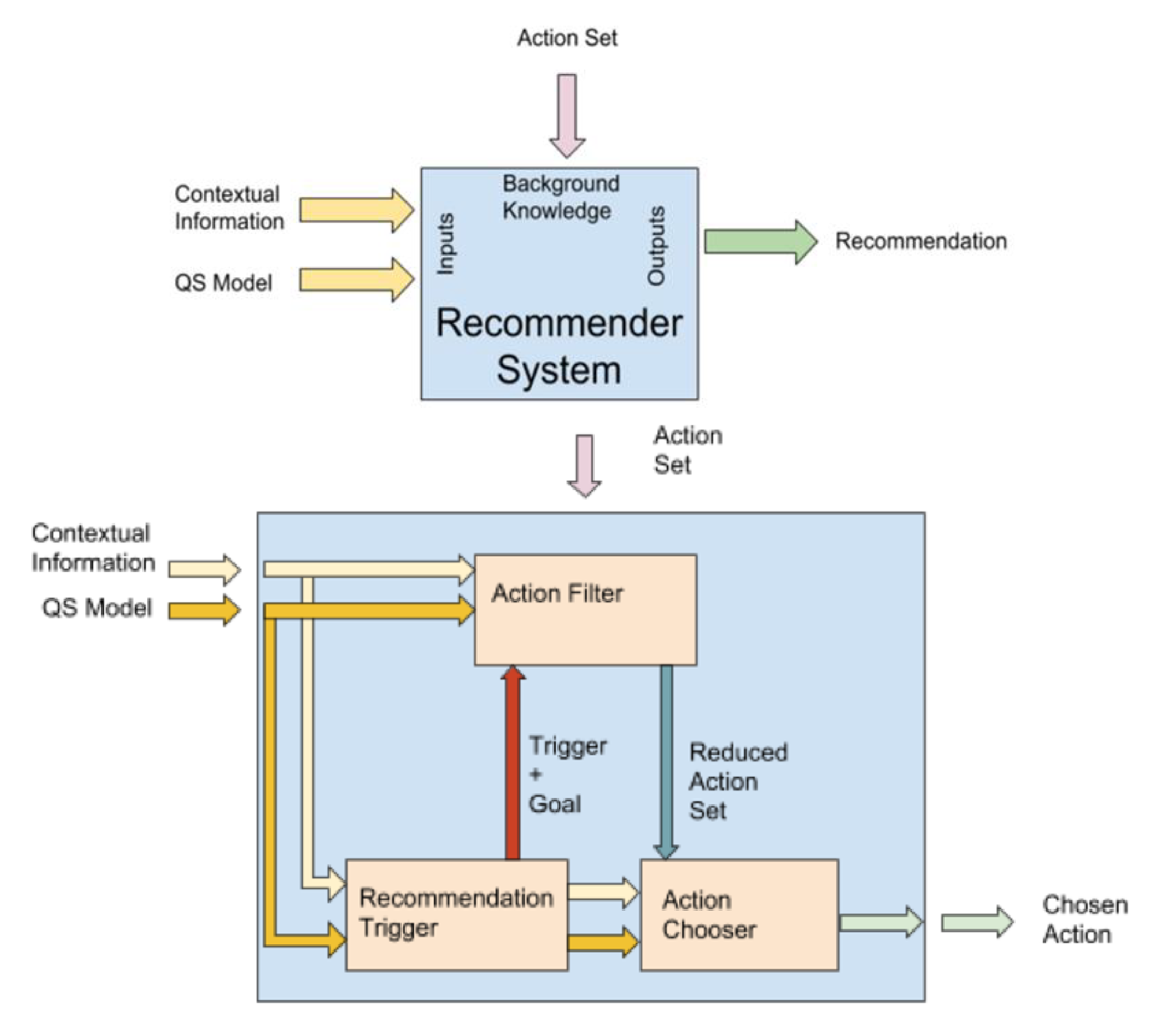
4.3. A Recommendation System to Complement the QS Model: The Activity Recommender System (ARS)
4.3.1. Recommendation Trigger
- Time and schedule: Depending on the time and the schedule of the users and actions, some actions are required to be scheduled. Reminder actions, weekly results summaries, scheduled physical activity sessions, etc., can be triggered within this aspect.
- Location: When the user visits specific locations, an action can be triggered. For example, if the user is walking near a sports center that offers activities the user might be interested in, a reminder can trigger this location.
- User model update: If the user’s QS model changes, an action can be triggered. Clear examples are the duration since the last physical activity session or time spent at a sedentary activity. When this time reaches a certain threshold, an activity recommendation is triggered.
4.3.2. Action Filter
4.3.3. Action Chooser
4.3.4. Recommendation Examples
- Healthy food restaurants and meals: At lunch or dinner time, the recommendation could be for a restaurant with a balanced menu based on your current location, or for a balanced meal at a specific restaurant.
- Healthy locations: When the system detects that the user is enjoying free time, it recommends places to visit nearby that have health benefits for the user.
- Physical activities: At the scheduled time for physical activity, a kind of activity is recommended, given the user preferences and the surrounding locations.
4.4. UX Model Using a QS Approach
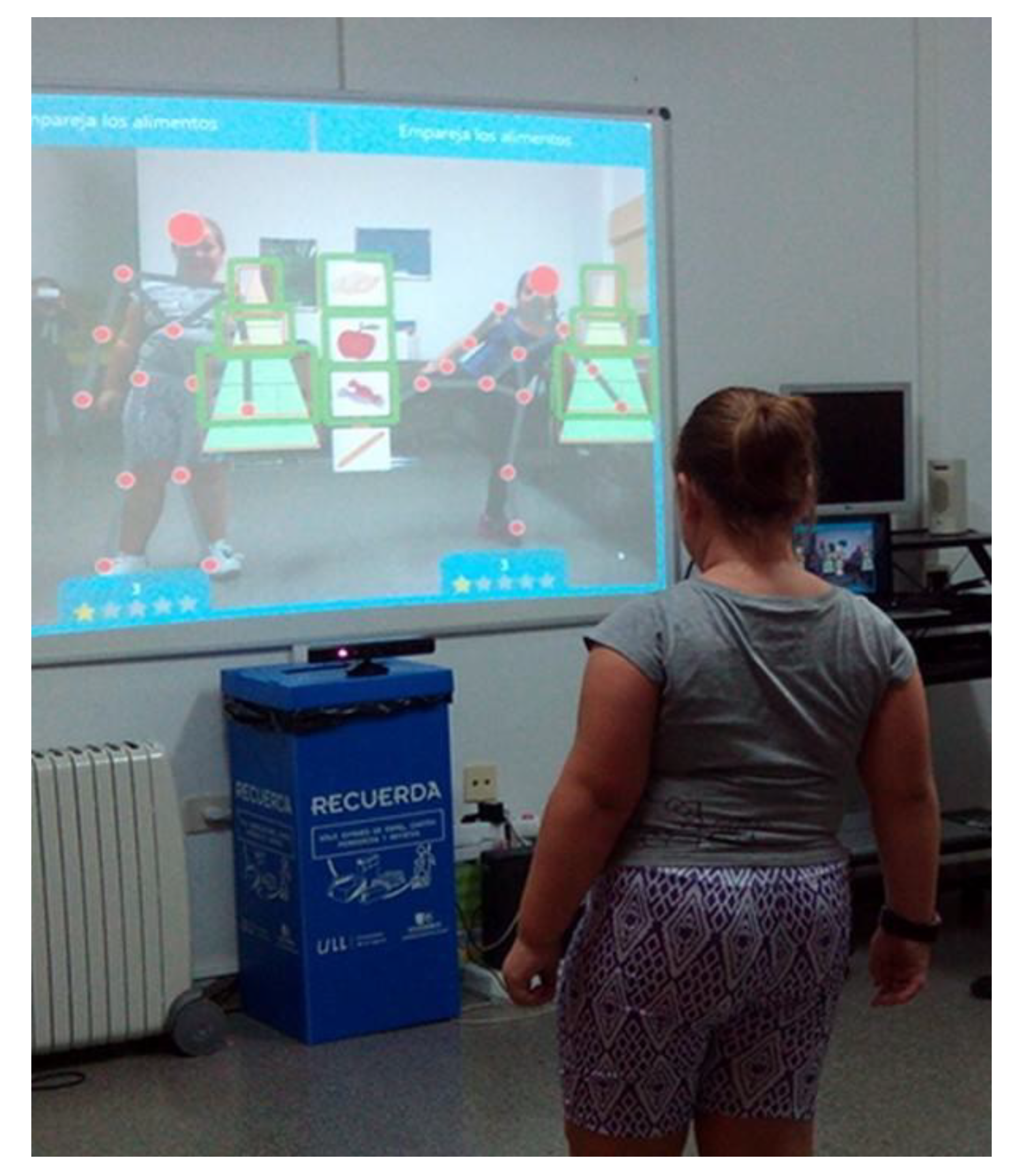
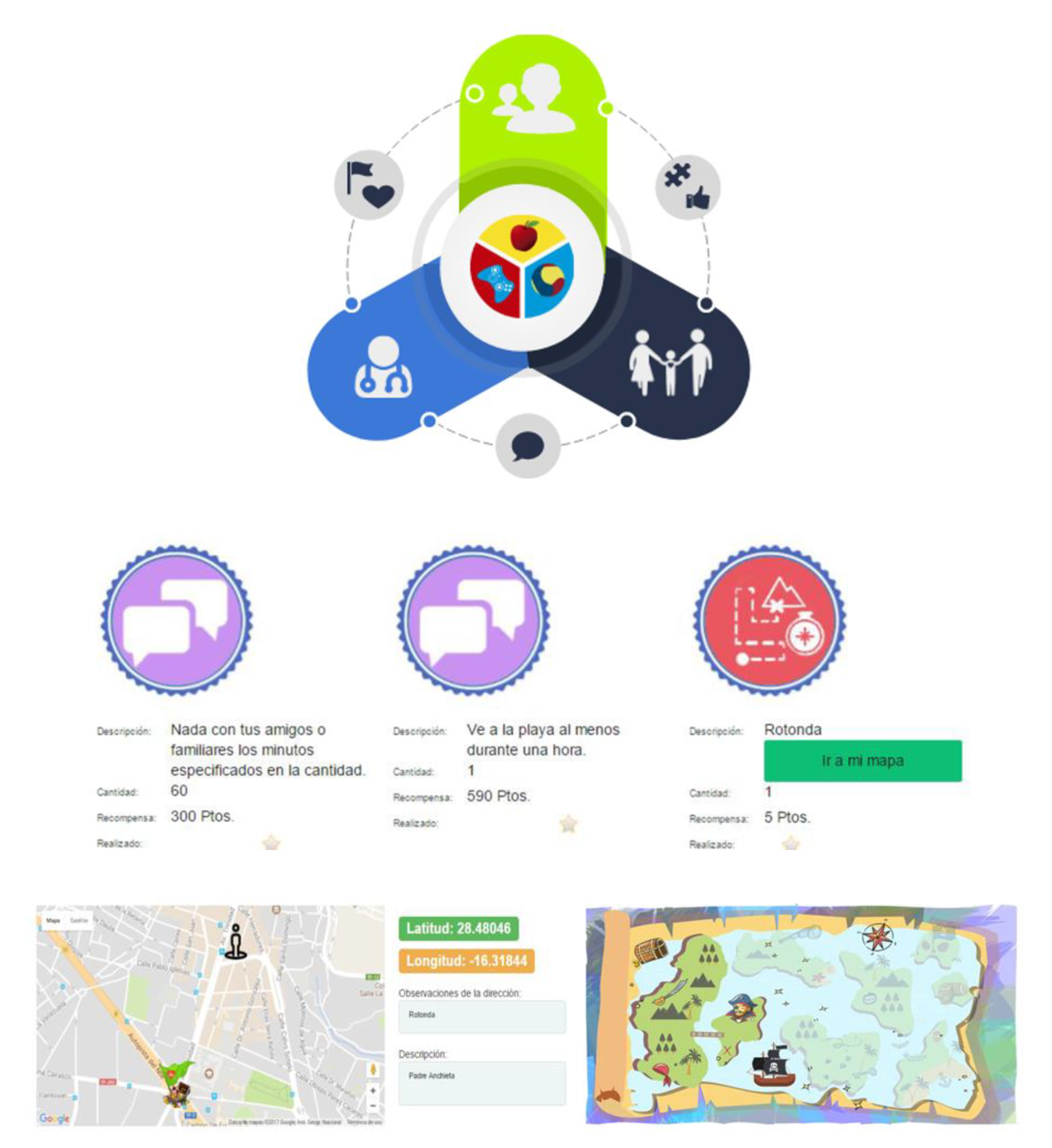
4.5. Gamified Technology-Based Intervention: The PROVITAO App Prototype
- Clinical support. Allows therapists to design an appropriate protocol for each patient, including follow-up, the activities experienced by the patient, and the control of their effects.
- Support at home. Allows communication between patient and therapist, enabling data of the process to be obtained and contributing to the child’s health education.
- Mobile support. Facilitates the child’s access to advice and therapeutic instructions, and carries out the different weekly activities to achieve a series of rewards, making the treatment attractive.
5. Validation
5.1. Validation of the Multidimensional QS Model
5.2. UX Validation
5.3. Validation of the Gamified Educational Intervention
6. Conclusions
- RQ1. What is an appropriate multidimensional QS model for promoting healthy habits in children? Many different data sources can be integrated into a QS model in the context proposed. These information sources were identified and integrated into a single QS model, which was defined and validated by experts after an iterative process in which the experts were classified by areas of expertise.
- RQ2. How might a recommender system complement the QS model to help the user select the appropriate actions and when to do them? A recommender system for a sophisticated QS model cannot be designed as a single system. This paper proposes a recommender system supported by three different modules. One module selects when a recommendation should be made based on contextual and user information in the QS model. The second module filters recommendations to provide only appropriate actions for the user and the context, using an automated planning strategy. The third module selects the most appropriate action based on the action’s content, the user filtering information, and a learning strategy that minimizes the selection of mismatched actions. These three modules combine to answer, first, the question of what to recommend and, second, of when to recommend it, to thus help children improve their healthy habits.
- RQ3. How can the UX of using a QS approach for children be improved? The PROVITAO App is the framework in which our recommender system was embedded. Improving the UX of the system was considered to be crucial. Consequently, a UX model was explicitly proposed. The PROVITAO App was validated by experts who highlighted usability issues of the application, and evaluation of average satisfaction based on heuristic categories identified areas where the application UX could be improved.
- RQ4. How does a gamified technology-based intervention impact the health of children? We presented a summary of the validation of the gamified program using different instruments and dimensions. The PROVITAO project created a game-based educational program for healthy habits using active games developed by the research group, such as TANGO: H, and commercial video games (Wii Fit Plus and apps). The project was carried out with 45 children suffering from childhood obesity, plus their caregivers. Various technological artifacts (exergames, serious games, web apps, sensorial libraries, wearable devices, etc.) have been developed as part of this project. Results of the project have not shown a significant immediate or general improvement in measures such as participants’ body mass composition or percentage of body fat. However, there is evidence of a positive impact on the children, which might lead to a long-term positive effect. These changes include better knowledge about healthy eating, improved behavior and greater sense of responsibility, control over issues such as social stress and depression, a tendency to favor positive emotions after the intervention, and an improvement in the children’s free-time habits. Furthermore, in a single case study with obesity and type II pre-diabetes, there were observed improvements in measurements of BMI, waist circumference, and percentage of body fat, and these improvements were maintained over time. For future interventions, it is recommended that the positive effects of the mentioned measures are analyzed during the process, rather than only the ultimate measures and BMI.
- A technological proposal based on a quantified-self user model to treat and prevent obesity in children was presented. These components were described in this paper (i.e., DS, QSUM, ASR, and UXM).
- An extensive list of data sources and the main mechanisms for data processing are provided in the DS component, which primarily uses the data to recommend healthy activities. In addition, the categories of DS and relationships are described in the QSUM component.
- A new approach for an activity recommender system is presented with the following characteristics:
- -
- A modular design comprising a recommendation trigger, an action filter working as a content-based recommender, and an action chooser as a collaborative filtering recommender.
- -
- Actions and action plans are built using an automated planning approach.
- -
- Action recommendation mismatches are minimized using a reinforcement learning strategy.
- -
- A multidimensional, goal-driven recommendation trigger is used that relies on the user’s location, time, and schedule, as well as user model changes, as its primary considerations.
- -
- The UX model for recommender systems is extended from the one proposed by Knijnenburg (2012) to consider the QS particularities and gamification aspects.
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Swinburn, B.A.; Sacks, G.; Hall, K.D.; McPherson, K.; Finegood, D.T.; Moodie, M.L.; Gortmaker, S.L. The global obesity pandemic: Shaped by global drivers and local environments. Lancet 2011, 378, 804–814. [Google Scholar] [CrossRef]
- Rimmer, J.H.; Vanderbom, K.A. A call to action: Building a translational inclusion team science in physical activity, nutrition, and obesity management for children with disabilities. Front. Public Health 2016, 4, 164. [Google Scholar] [CrossRef] [PubMed]
- Must, A.; Strauss, R.S. Risks and consequences of childhood and adolescent obesity. Int. J. Assoc. Study Obes. 1999, 23, 2–11. [Google Scholar] [CrossRef] [PubMed]
- Pulgaron, E.R.; Delamater, A.M. Obesity and type 2 diabetes in children: Epidemiology and treatment. Curr. Diabetes Rep. 2014, 14, 508. [Google Scholar] [CrossRef] [PubMed]
- Nesta. The NHS in 2030: A People-Powered and Knowledge-Powered Health System. 2015. Available online: https://www.nesta.org.uk/report/the-nhs-in-2030-a-people-powered-and-knowledge-powered-health-system/ (accessed on 31 July 2018).
- Nogueira, T.F.D.; Zambon, M.P. Reasons for non-adherence to obesity treatment in children and adolescents. Rev. Paul. Pediatr. 2013, 31, 338–343. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Nacke, L.E.; Deterding, C.S. The maturing of gamification research. Comput. Hum. Behav. 2017, 71, 450–454. [Google Scholar] [CrossRef]
- Gómez del Río, N.G.; González-González, C.S.; Gonzalez, R.M.; Adelantado, V.N.; Delgado, P.T.; Fleitas, Y.B. Gamified educational programme for childhood obesity. In Proceedings of the 2018 IEEE Global Engineering Education Conference (EDUCON), Santa Cruz de Tenerife, Canary Islands, Spain, 18–20 April 2018. [Google Scholar]
- Park, L.G.; Howie-Esquivel, J.; Dracup, K. A quantitative systematic review of the efficacy of mobile phone interventions to improve medication adherence. J. Adv. Nurs. 2014, 70, 1932–1953. [Google Scholar] [CrossRef]
- Pérez-Jover, V.; Sala-González, M.; Guilabert, M.; Mira, J.J. Mobile apps for increasing treatment adherence: Systematic review. J. Med. Internet Res. 2019, 21, e12505. [Google Scholar] [CrossRef]
- Ahmed, I.; Ahmad, N.S.; Ali, S.; Ali, S.; George, A.; Danish, H.S.; Uppal, E.; Soo, J.; Mobasheri, M.H.; King, D.; et al. Medication adherence apps: Review and content analysis. JMIR mHealth uHealth 2018, 6, e62. [Google Scholar] [CrossRef]
- Park, J.Y.E.; Li, J.; Howren, A.; Tsao, N.W.; A De Vera, M.; Jeong, E.; Patel, T. Mobile phone apps targeting medication adherence: Quality assessment and content analysis of user reviews. JMIR mHealth uHealth 2019, 7, e11919. [Google Scholar] [CrossRef]
- Lambert, E.; Harvey, L.A.; Avdalis, C.; Chen, L.W.; Jeyalingam, S.; Pratt, C.A.; Tatum, H.J.; Bowden, J.L.; Lucas, B.R. An app with remote support achieves better adherence to home exercise programs than paper handouts in people with musculoskeletal conditions: A randomised trial. J. Physiother. 2017, 63, 161–167. [Google Scholar] [CrossRef] [PubMed]
- Voth, E.C.; Oelke, N.D.; Jung, M.E. A theory-based exercise app to enhance exercise adherence: A pilot study. JMIR mHealth uHealth 2016, 4, e62. [Google Scholar] [CrossRef] [PubMed]
- Russo, C.R. The quantified self. HCI 2015, 15, 514–520. [Google Scholar]
- Marcengo, A.; Rapp, A. Visualization of human behavior data: The quantified self. In Innovative Approaches of Data Visualization and Visual Analytics; IGI GLOBAL: Hershey, PA, USA, 2013; pp. 236–265. [Google Scholar]
- Swan, M. Emerging patient-driven health care models: An examination of health social networks, consumer personalized medicine and quantified self-tracking. Int. J. Environ. Res. Public Health 2009, 6, 492–525. [Google Scholar] [CrossRef]
- Cena, F.; Likavec, S.; Rapp, A. Quantified self and modeling of human cognition. In Proceedings of the 2015 ACM International Joint Conference on Pervasive and Ubiquitous Computing and Proceedings of the 2015 ACM International Symposium on Wearable Computers, Osaka, Japan, 7–11 September 2015; ACM: New York, NY, USA, 2015; pp. 1021–1026. [Google Scholar]
- Maeyer, C.; Markopoulos, P. Exploring quantified self attitudes. In Proceedings of the HEALTHINF 2018, Funchal, Madeira, Portugal, 19–21 January 2018; pp. 253–260. [Google Scholar]
- De Vries, H.J.; Kooiman, T.J.M.; van Ittersum, M.W.; van Brussel, M.; de Groot, M. Do activity monitors increase physical activity in adults with overweight or obesity? A systematic review and meta-analysis. Obesity 2016, 24, 2078–2091. [Google Scholar] [CrossRef]
- Ledger, D.; McCaffrey, D. Inside Wearables: How the Science of Human Behavior Change Offers the Secret to Long-Term Engagement; Endeavour Partners LLC: Cambridge, MA, USA, 2014; pp. 1–17. [Google Scholar]
- Hammond, T. Wearables Have a Dirty Little Secret: 50% of Users Lose Interest. 2014. Available online: http://www.techrepublic.com/article/wearables-have-a-dirty-little-secret-most- (accessed on 3 March 2020).
- Sharon, T. Self-tracking for health and the quantified self: Re-articulating autonomy, solidarity, and authenticity in an age of personalized healthcare. Philos. Technol. 2017, 30, 93–121. [Google Scholar] [CrossRef]
- Choe, E.U.; Lee, N.B.; Lee, B.; Pratt, W.; Kientz, J. Understanding quantified-selfers’ practices in collecting and exploring personal data. In Proceedings of the CHI Conference on Human Factors in Computing Systems, Toronto, ON, Canada, 26 April–1 May 2014; pp. 1143–1152. [Google Scholar] [CrossRef]
- Swan, M. The quantified self: Fundamental disruption in big data science and biological discovery. Big Data 2013, 1, 85–99. [Google Scholar] [CrossRef]
- Hoogendoorn, M.; Funk, B. Machine Learning for the quantified self—On the art of learning from sensory data. In Cognitive Systems Monographs 35; Springer: Berlin/Heidelberg, Germany, 2018; pp. 1–221. ISBN 978-3-319-66307-4. [Google Scholar]
- Yang, R.; Shin, E.; Newman, M.W.; Ackerman, M.S. When fitness trackers don’t ‘fit’. In Proceedings of the 2015 ACM International Joint Conference on Pervasive and Ubiquitous Computing—UbiComp 15, Osaka, Japan, 7–11 September 2015. [Google Scholar]
- Gimpel, H.; Nißen, M.; Görlitz, R. Quantifying the quantified self: A study on the motivations of patients to track their own health. In Proceedings of the International Conference on Information Systems (ICIS 2013): Reshaping Society Through Information Systems Design, Milan, Italy, 15–18 December 2013. [Google Scholar]
- Bermingham-McDonogh, N. The Data Science of the Quantified Self; Vrije Universiteit Amsterdam: Amsterdam, The Nertherlands, 2015. [Google Scholar]
- Swan, M. Sensor mania! The internet of things, wearable computing, objective metrics, and the quantified self 2.0. J. Sens. Actuator Netw. 2012, 1, 217–253. [Google Scholar] [CrossRef]
- Shehab, A.; Ismail, A.; Osman, L.; Elhoseny, M.; El-Henawy, I.M. Quantified self using IoT wearable devices. In Proceedings of the AISI 2017, Cairo, Egypt, September 9–11 2017; pp. 820–831. [Google Scholar]
- Menychtas, A.; Papadimatos, D.; Tsanakas, P.; Maglogiannis, I. On the Integration of wearable sensors in IoT enabled mHealth and quantified-self applications. In Proceedings of the IMCL 2017, Thessaloníki, Greece, 30 November–1 December 2017; pp. 77–88. [Google Scholar]
- Chousiadas, D.; Menychtas, A.; Tsanakas, P.; Maglogiannis, I. Advancing quantified-self applications utilizing visual data analytics and the internet of things. In Proceedings of the AIAI (Workshops) 2018, Rhodes, Greece, 25–27 May 2018; pp. 263–274. [Google Scholar]
- Keskin, T. Introduction to the minitrack on internet of things: Providing services using smart devices, wearables, and quantified self. In Proceedings of the HICSS 2018, Hilton Waikoloa Village, HI, USA, 3–6 January 2018. [Google Scholar]
- Shin, D.; Biocca, F. Health experience model of personal informatics: The case of a quantified self. Comput. Hum. Behav. 2017, 69, 62–74. [Google Scholar] [CrossRef]
- Shin, H. Cross-platform user experience towards designing an inter-usable system. Int. J. Hum.-Comput. Interact. 2016, 32, 503–514. [Google Scholar] [CrossRef]
- Regnier, F.; Chauvel, L. Digital inequalities in the use of self-tracking diet and fitness apps: Interview study on the influence of social, economic, and cultural factors. JMIR mHealth uHealth 2018, 6, e101. [Google Scholar] [CrossRef] [PubMed]
- Williamson, B. The digitised future of physical education. In Transformative Learning and Teaching in Physical Education; Routledge: London, UK, 2017. [Google Scholar]
- Mehta, R. The self-quantification movement-implications for healthcare professionals. SelfCare 2011, 2, 87–92. [Google Scholar]
- Munson, S.A.; Consolvo, S. Exploring goal-setting, rewards, self-monitoring, and sharing to motivate physical activity. In Proceedings of the 6th International Conference on Pervasive Computing Technologies for Healthcare (PervasiveHealth) and Workshops, San Diego, CA, USA, 21–24 May 2012; pp. 25–32. [Google Scholar]
- Hamari, J.; Hassan, L.; Dias, A. Gamification, quantified-self or social networking? Matching users’ goals with motivational technology. User Model. User-Adapt. Interact. 2018, 28, 35–74. [Google Scholar] [CrossRef]
- Didžiokaitė, G.; Saukko, P.; Greiffenhagen, C. The mundane experience of everyday calorie trackers: Beyond the metaphor of quantified self. New Media Soc. 2017, 20, 1470–1487. [Google Scholar] [CrossRef]
- Schaefer, S.E.; Van Loan, M.; German, J.B. A feasibility study of wearable activity monitors for pre-adolescent school-age children. Prev. Chronic Dis. 2014, 11, E85. [Google Scholar] [CrossRef] [PubMed]
- Hswen, Y.; Murti, V.; Vormawor, A.A.; Bhattacharjee, R.; Naslund, J.A. Virtual avatars, gaming, and social media: Designing a mobile health app to help children choose healthier food options. J. Mob. Technol. Med. 2013, 2, 8–14. [Google Scholar] [CrossRef] [PubMed]
- Pluim, C.; Gard, M. Physical education’s grand convergence: Fitnessgram®, big-data and the digital commerce of children’s health. Crit. Stud. Educ. 2016, 1–18. [Google Scholar] [CrossRef]
- Nafus, D. (Ed.) Quantified: Biosensing Technologies in Everyday Life; MIT Press: Cambridge, MA, USA, 2016. [Google Scholar]
- Nafus, D.; Sherman, J. This one does not go up to 11: The quantified self movement as an alternative big data practice. Int. J. Commun. 2014, 8, 1784–1794. [Google Scholar]
- Whitson, J.R. Gaming the quantified self. Surveill. Soc. 2013, 11, 163–176. [Google Scholar] [CrossRef]
- Sarzotti, F.; Lombardi, I.; Rapp, A.; Marcengo, A.; Cena, F. Engaging users in self-reporting their data: A tangible interface for quantified self. In Proceedings of the International Conference on Universal Access in Human-Computer Interaction, Los Angeles, CA, USA, 2–7 August 2015; Springer: Cham, Switzerland, 2015; pp. 518–527. [Google Scholar]
- Marshall, T.; Champagne-Langabeer, T.; Castelli, D.; Hoelscher, D. Cognitive computing and eScience in health and life science research: Artificial intelligence and obesity intervention programs. Health Inf. Sci. Syst. 2017, 5, 13. [Google Scholar] [CrossRef]
- González, C.S.; Cairós-González, M.; Navarro-Adelantado, V. EMODIANA: Un instrumento para la evaluación subjetiva de emociones en niños y niñas. In Proceedings of the Actas Del XIV Congreso Internacional de Interacción Persona-Ordenador, Madrid, Spain, 17–20 September 2013; Volume 10. [Google Scholar]
- Reynolds, C.R.; Kamphaus, R.W. BASC: Sistema de Evaluación de la Conducta en Niños y Adolescentes; TEA: Madrid, Spain, 2004. [Google Scholar]
- Serra-Majem, L.; Ribas, L.; Ngo, J.; Ortega, R.M.; García, A.; Pérez-Rodrigo, C.; Aranceta-Bartrina, J. Food, youth and the Mediterranean diet in Spain. Development of KIDMED, Mediterranean Diet Quality Index in children and adolescents. Public Health Nutr. 2004, 7, 931–935. [Google Scholar] [CrossRef]
- Burke, R. Hybrid recommender systems: Survey and experiments. User Model. User-Adapt. Interact. 2002, 12, 331–370. [Google Scholar] [CrossRef]
- Hu, R.; Pu, P. Acceptance issues of personality-based recommender systems. In Proceedings of the Third ACM Conference on Recommender Systems, New York, NY, USA, 22–25 October 2009; ACM: New York, NY, USA, 2009; pp. 221–224. [Google Scholar]
- Pu, P.; Chen, L.; Hu, R. Evaluating recommender systems from the user’s perspective: Survey of the state of the art. User Model. User-Adapt. Interact. 2012, 22, 317–355. [Google Scholar] [CrossRef]
- Pu, P.; Chen, L.; Hu, R. A user-centric evaluation framework for recommender systems. In Proceedings of the Fifth ACM Conference on Recommender Systems, Chicago, IL, USA, 23–27 October 2011; ACM: New York, NY, USA, 2011; p. 157. [Google Scholar]
- Knijnenburg, B.P.; Willemsen, M.C.; Gantner, Z.; Soncu, H.; Newell, C. Explaining the user experience of recommender systems. User Model. User-Adapt. Interact. 2012, 22, 441–504. [Google Scholar] [CrossRef]
- Nielsen, J. Available online: https://www.nngroup.com/articles/how-to-conduct-a-heuristic-evaluation/ (accessed on 15 March 2020).
- Ledford, J.R.; Gast, D.L. Single Case Research Methodology: Applications in Special Education and Behavioral Sciences; Routledge: London, UK, 2018. [Google Scholar]
- Fasano, G.; Franceschini, A. A multidimensional version of the Kolmogorov–Smirnov test. Mon. Not. R. Astron. Soc. 1987, 225, 155–170. [Google Scholar] [CrossRef]
- Fernández, C.; Lorenzo, H.; Vrotsou, K.; Aresti, U.; Rica, I.; Sánchez, E. Estudio de Crecimiento de Bilbao. Curvas y Tablas de Crecimiento; Faustino Orbegozo Foundation, 2011; Available online: https://www.fundacionorbegozo.com/wp-content/uploads/pdf/estudios_2011.pdf (accessed on 15 March 2020).
- Gómez del Río, N.; González, C.S.G.; Martín, R.; Navarro-Adelantado, V.; Toledo, P.; Fleitas, Y.D.C.B.; Marrero-Gordillo, N.; Armas, H.; García-Peñalvo, F.J. Treatment of children obesity and diabetes through gamification: A case of study. In Proceedings of the Seventh International Conference on Technological Ecosystems for Enhancing Multiculturality, León, Spain,16–18 October 2019; ACM: New York, NY, USA, 2019; pp. 452–458. [Google Scholar]
- Reynolds, C.; Kamphaus, R.W. BASC-2. Behavior Assessment System for Children, 2nd ed.; Pearson: Bloomington, MN, USA, 2004. [Google Scholar]
- Del Río, N.G.; González-González, C.S.; Martín-González, R.; Navarro-Adelantado, V.; Delgado, P.A.T.; García-Peñalvo, F.J. Effects of a gamified educational program in the nutrition of children with obesity. J. Med Syst. 2019, 43, 198. [Google Scholar] [CrossRef]
- Fleiss, J.L.; Levin, B.; Paik, M.C. The measurement of interrater agreement. In Statistical Methods for Rates and Proportions; John Wiley & Sons, Inc: Hoboken, NJ, USA, 1981; Volume 2, pp. 22–23. [Google Scholar]
- Altman, D.G. Mathematics for kappa. In Practical Statistics for Medical Research; Chapman & Hall: London, UK, 1991; pp. 406–407. [Google Scholar]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Phase | Goal |
|---|---|
| 1: Pre-Intervention Phase |
|
| 2: Intervention |
|
| 3: Post-Intervention Phase |
|
| Type of Measurement | Data | When |
|---|---|---|
| Medical reports | Diagnosis Treatment Level of compliance Tests Observations | Periodical |
| Blood tests | Systolic blood pressure, Diastolic blood pressure, Erythrocytes Leukocytes, Hematocrit, Hemoglobin, Platelets, Glucose Cholesterol, Triglycerides, Iron, Ferritin, B12 vitamin, Folic acid, Creatinine, etc. | Pre-/Mid-/Post- Intervention |
| Anthropometric dataº | Age, weight, height, BMI, subscapular folds, triceps folds, biceps folds, pectoral folds, axillary folds, supraspinal folds, abdominal folds, thigh folds, leg folds, humeral diameter, wrist diameter, femur diameter, waist diameter, hip diameter, contracted arm diameter, relaxed arm diameter, leg perimeter, thigh perimeter | Pre-/Mid-/Post- Intervention |
| Biometric data from sensors | Pulsometer (Heart Rate) Accelerometer (Steps, Speed, Distance, Pace, etc.) | During session intervention/Diary |
| Geolocalization data | Patient’s physical location Timepoint Patient’s location history | Diary |
| Emotional data | Intervention (EMODIANA): -Input emotion (Positive, Negative, Neutral) -Exit emotion (Positive, Negative, Neutral) -Justification (Person, Structure, Context, Person-Structure, Person-Context, Structure-Context, Person-Structure-Context) Mood (sentiment analysis) | Per session (entrance and exit) Diary |
| Behavioral data (BASC) | Negative attitude toward school Negative attitude toward teachers Atypicality Control locus Social stress Anxiety Depression Sense of disability Relationships Relationship with parents Self-esteem Self-confidence Clinical mismatch School mismatch Personal adjustment | Pre-/Mid-/Post- Intervention |
| Diet data (KIDMED) | Adherence to Mediterranean Diet: Types of foods, Frequency, and Quantity | Pre-/Mid-/Post- Intervention |
| Data on healthy physical habits | States of physical activity Self-perception of motor competence and the usefulness of physical activity or sports Health and personal well-being | Pre-/Mid-/Post- Intervention |
| Social data | Level of interaction in collaborative activities/games Role in the group (gamification) Social status (gamification) | During session intervention |
| UX data | UX satisfaction (TANGO: H) Emotional variables Fun Toolkit Metrics (Apps) | During session intervention Home/Diary |
| Player Profile (HEXAD) | Philanthropic Achiever Socializer Free spirit Player Disruptor | Beginning of the intervention |
| Socio-economic data | City, District Internet access and connected devices School (Private–Public) | Beginning of the intervention |
| Situational data | Context Situation Privacy concerns Time of day Day of week | During intervention |
| Activities |
| Sessions designed for the group (weekly) Sessions designed for the home (weekly) Sessions designed for the group (weekly) Recommended activities to perform at home (weekly) |
| User Preferences | Favorite foods/drinks Favorite activities/games Favorite places | During intervention |
| Personal characteristics | Age Sex Educational level Attitudes and motivation | At the beginning of the intervention |
| Environmental data | Family environment School environment | At the beginning of the intervention |
| Medicine (Biomedical, Physiotherapy, Pediatrics, Nutrition and Endocrinology) | Leisure-Emotion (Physical Education and Psychology) | Interactivity (Computer Science, Psychology) | Psychology and Education (Psychology, Health Education, Educational Technology) | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Expert | E1 | E2 | E3 | E4 | E5 * | E6 | E7 | E8 | E9 | E10 | E11 | E12 | E13 * | E13 * | E5 * | E14 | E15 |
| Age | 40 | 58 | 50 | 60 | 25 | 58 | 44 | 43 | 28 | 34 | 43 | 33 | 29 | 29 | 25 | 25 | 26 |
| Sex | M | F | F | M | F | M | M | F | F | M | F | M | F | F | F | F | M |
| Title | ME | ME | ME | ME | NU | PE | PE | CS | PS | CS | CS | CS | PS | PS | NU | ED | CS |
| ## | Problem | Heuristic (s) | Severity | Detail |
|---|---|---|---|---|
| 1 | Navigation | #1 #3 | 2 | Users found difficulties in navigation and misunderstood the nav buttons. Lack of buttons to move between activities and to move back and forward. |
| 2 | Consistency and standards | #2 | 2 | Some words or symbols can be confused. For example, the gamification “star” symbol does not appear in health professional profiles. |
| 3 | Personalization | #7 #3 | 1 | Need more personalization features in user profiles. |
| 4 | Error messages | #5 #6 | 2 | Signs usually accompany some error messages at the beginning that divert attention from the error message. The corresponding solution should accompany error messages. |
| 5 | Help | #10 | 4 | Need to expand the help section and to write more instructions on some patient options. There should be a help section or, in its absence, instructions on each page, especially doctors. |
| ## | Success | Heuristic (s) | Detail |
|---|---|---|---|
| 1 | Language | #4 | Correct language adapted to children (in this case, patients). |
| 2 | Design | #8 | Nice, adequate, and minimalist design. The information displayed correctly. |
| 3 | Gamification | #7 | Good approach, especially the rewards map. |
| # | Category | Quantity Of Heuristics Evaluated | Average Satisfaction (Min:1–Max:5) |
|---|---|---|---|
| 1 | Visibility of system status | 19 | 2.3 |
| 2 | Match between system and the real world | 8 | 2.3 |
| 3 | User control and freedom | 8 | 3 |
| 4 | Consistency and standards | 14 | 2.1 |
| 5 | Error prevention | 9 | 2.4 |
| 6 | Recognition rather than recall | 4 | 2.8 |
| 7 | Flexibility and efficiency of use | 11 | 1.9 |
| 8 | Aesthetic and minimalist design | 2 | 3.4 |
| 9 | Help users recognize, diagnose, and recover from errors | 3 | 1.9 |
| 10 | Help and documentation | 4 | 2.9 |
| Group and Statistical Means and (Standard Deviations) of the Difference in Mean Scores in the Children’s Baseline Questionnaires | ||||||
| Control N = 20 | Experimental N = 25 | F(1.43) | p | η2p | P | |
| Self-perception of motor skills and the usefulness of physical activity or sports | 22.25 (3.40) | 20.36 (5.60) | 1.75 | 0.19 | 0.04 | 0.25 |
| Feeding | 27.00 (3.64) | 26.40 (2.66) | 0.41 | 0.52 | 0.01 | 0.10 |
| Personal Health and Wellness | 40.75 (5.73) | 39.32 (7.03) | 0.54 | 0.47 | 0.01 | 0.11 |
| Means and (Standard Deviations) of Questionnaire Rates Reported by the Two Groups of Children in the Follow-Up Assessments. | ||||||
| Short Term | Long Term | |||||
| Control N = 16 | Experimental N = 17 | Control N = 16 | Experimental N = 15 | |||
| Self-perception of motor skills and the usefulness of physical activity or sports | 22.69 (3.34) | 20.59 (4.99) | 20.81 (3.31) | 19.80 (5.71) | ||
| Feeding | 27.00 (2.88) | 28.71 (2.62) | 29.56 (2.50) | 30.87 (2.95) | ||
| Personal Health and Wellness | 40.25 (6.39) | 40.18 (8.06) | 40.63 (8.21) | 38.80 (7.01) | ||
| Control Group | ||||||||||||
| Year 1 | Year 2 | |||||||||||
| Pre-Test | Post-Test (Short Term) | Post-Test (Long Term) | Pre-Test | Post-Test (Short Term) | Post-Test (Long Term) | |||||||
| Median | SD | Median | SD | Median | SD | Median | SD | Median | SD | Median | SD | |
| Age (years) | 8.67 | 1.66 | 8.44 | 1.67 | 8.5 | 1.2 | 10.09 | 1.51 | 10.86 | 1.21 | 11.1 | 1.52 |
| Weight (kg) | 53 | 8.24 | 51.41 | 8.44 | 55 | 8.21 | 58.72 | 13.14 | 61.26 | 6.71 | 64.5 | 12.51 |
| Height (m) | 1.41 | 0.11 | 1.41 | 0.1 | 1.44 | 0.11 | 1.48 | 0.11 | 1.52 | 0.08 | 1.54 | 0.1 |
| BMI (Kg/m2) | 26.82 | 3.13 | 25.56 | 1.89 | 26.49 | 2.11 | 26.53 | 3 | 26.42 | 2.75 | 27.13 | 2.91 |
| W/H Ratio | 0.91 | 0.15 | 1.99 | 3.04 | 0.96 | 0.06 | 0.95 | 0.05 | 0.97 | 0.03 | 0.92 | 0.05 |
| Experimental Group | ||||||||||||
| Pre-Test | Post-Test (Short Term) | Post-Test (Long Term) | Pre-Test | Post-Test (Short Term) | Post-Test (Long Term) | |||||||
| Median | SD | Median | SD | Median | SD | Median | SD | Median | SD | Median | SD | |
| Age (years) | 9.38 | 1.85 | 9.46 | 1.9 | 10.25 | 1.66 | 9.17 | 1.64 | 9 | 2.16 | 9.71 | 1.8 |
| Weight (kg) | 63.65 | 14.39 | 64.4 | 14.72 | 72.09 | 11.89 | 57.58 | 13.51 | 53.43 | 8.15 | 60.82 | 11.44 |
| Height (m) | 1.41 | 0.11 | 1.44 | 0.09 | 1.49 | 0.08 | 1.44 | 0.12 | 1.43 | 0.14 | 1.47 | 0.12 |
| BMI (Kg/m2) | 31.72 | 5.87 | 30.49 | 5.06 | 32.52 | 4.07 | 27.52 | 3.59 | 26.1 | 1.96 | 27.98 | 2.37 |
| W/H Ratio | 1 | 0.05 | 0.99 | 0.06 | 0.99 | 0.08 | 0.96 | 0.06 | 1 | 0.08 | 0.93 | 0.06 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gómez-del-Río, N.; González-González, C.S.; Toledo-Delgado, P.A.; Muñoz-Cruz, V.; García-Peñalvo, F. Health Promotion for Childhood Obesity: An Approach Based on Self-Tracking of Data. Sensors 2020, 20, 3778. https://doi.org/10.3390/s20133778
Gómez-del-Río N, González-González CS, Toledo-Delgado PA, Muñoz-Cruz V, García-Peñalvo F. Health Promotion for Childhood Obesity: An Approach Based on Self-Tracking of Data. Sensors. 2020; 20(13):3778. https://doi.org/10.3390/s20133778
Chicago/Turabian StyleGómez-del-Río, Nazaret, Carina S. González-González, Pedro A. Toledo-Delgado, Vanesa Muñoz-Cruz, and Francisco García-Peñalvo. 2020. "Health Promotion for Childhood Obesity: An Approach Based on Self-Tracking of Data" Sensors 20, no. 13: 3778. https://doi.org/10.3390/s20133778
APA StyleGómez-del-Río, N., González-González, C. S., Toledo-Delgado, P. A., Muñoz-Cruz, V., & García-Peñalvo, F. (2020). Health Promotion for Childhood Obesity: An Approach Based on Self-Tracking of Data. Sensors, 20(13), 3778. https://doi.org/10.3390/s20133778