Does the Presence of Cognitive Impairment Exacerbate the Risk of Falls in People with Peripheral Neuropathy? An Application of Body-Worn Inertial Sensors to Measure Gait Variability




Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Physiological, Psycho-Cognitive, and Functional Assessments
2.3. Walking Performance
2.4. Data Analysis
2.5. Statistical Analysis
3. Results
3.1. Participant Characteristics
3.2. Walking Performance between the Cognitively Intact and Impaired Groups
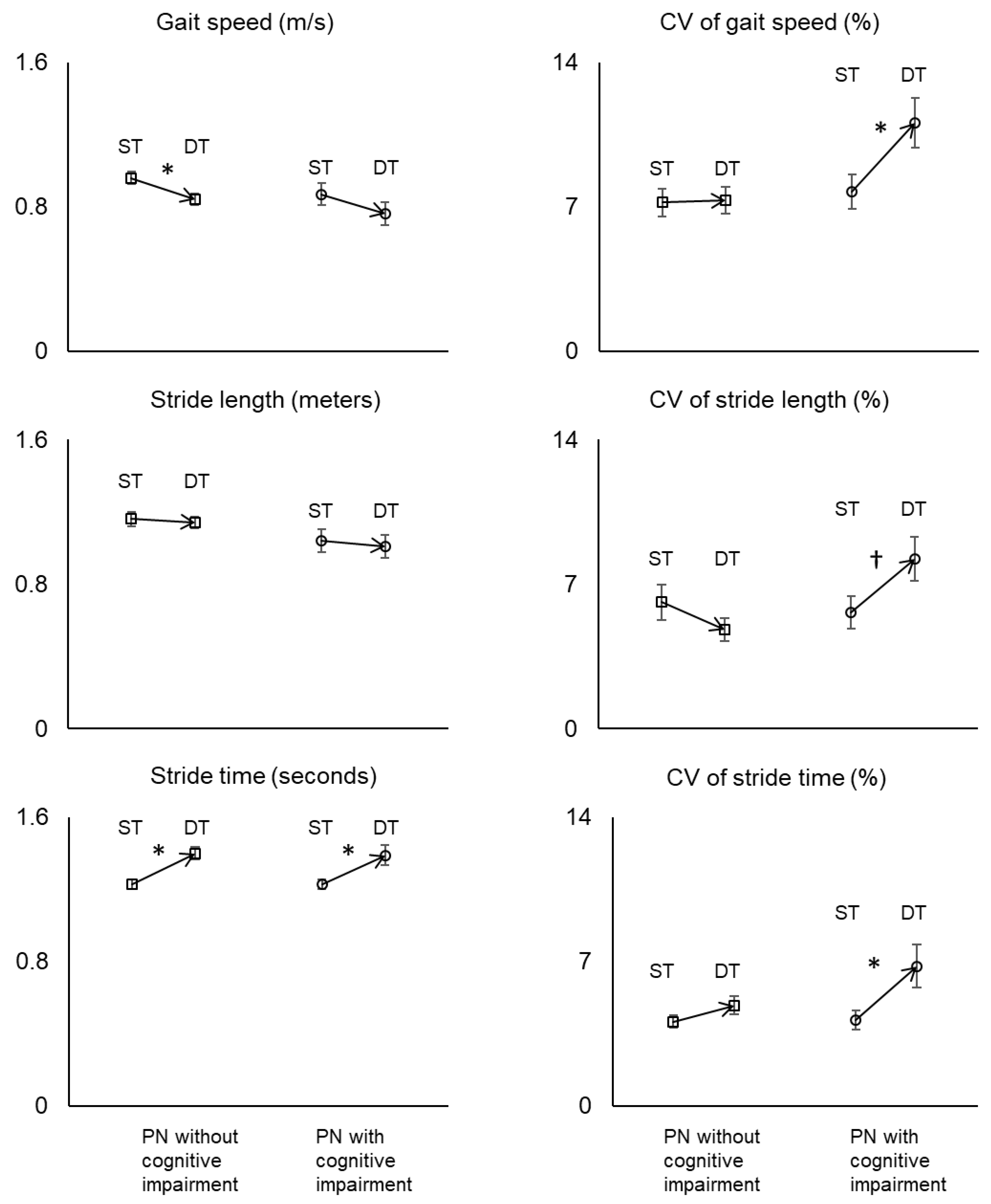
3.3. Walking Performance between Normal and Dual-Task Conditions
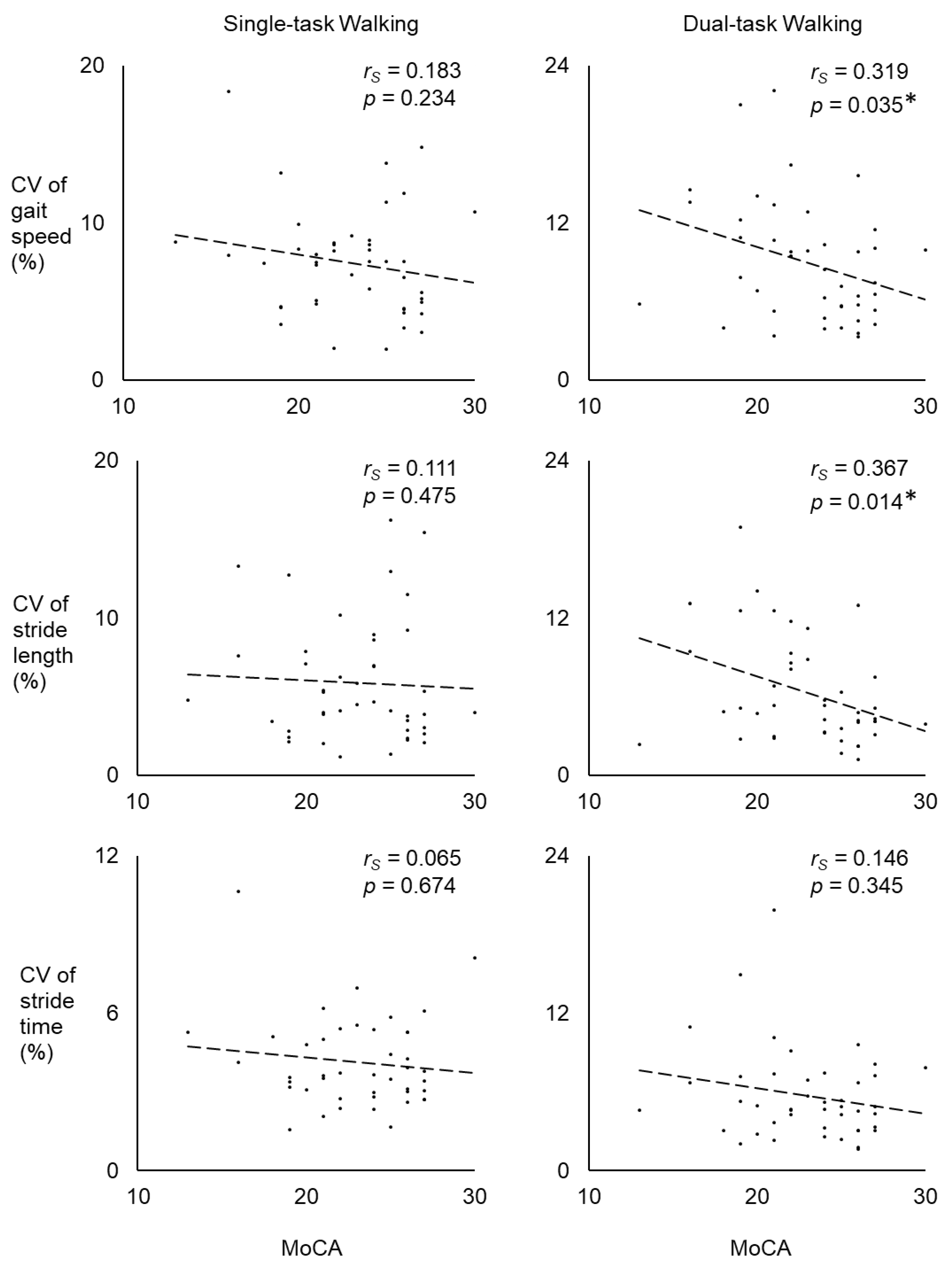
3.4. Correlations between Cognitive Function and Stride-to-Stride Variability
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- National Institute of Neurological Disorders and Stroke. Peripheral Neuropathy Fact Sheet. Available online: https://www.ninds.nih.gov/Disorders/Patient-Caregiver-Education/Fact-Sheets/Peripheral-Neuropathy-Fact-Sheet#3208_4 (accessed on 11 February 2020).
- Richardson, J.K.; Hurvitz, E.A. Peripheral neuropathy: A true risk factor for falls. J. Gerontol. Ser. A Biol. Sci. Med Sci. 1995, 50, M211–M215. [Google Scholar] [CrossRef] [PubMed]
- Gewandter, J.; Fan, L.; Magnuson, A.; Mustian, K.; Peppone, L.; Heckler, C.; Hopkins, J.; Tejani, M.; Morrow, G.; Mohile, S. Falls and functional impairments in cancer survivors with chemotherapy-Induced peripheral neuropathy (CIPN): A University of Rochester CCOP study. Supportive Care Cancer 2013, 21, 2059–2066. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benbow, S.; Wallymahmed, M.; MacFarlane, I. Diabetic peripheral neuropathy and quality of life. QJM Mon. J. Assoc. Physicians 1998, 91, 733–737. [Google Scholar] [CrossRef] [PubMed]
- Smith, E.M.L.; Pang, H.; Cirrincione, C.; Fleishman, S.; Paskett, E.D.; Ahles, T.; Bressler, L.R.; Fadul, C.E.; Knox, C.; Le-Lindqwister, N. Effect of duloxetine on pain, function, and quality of life among patients with chemotherapy-Induced painful peripheral neuropathy: A randomized clinical trial. JAMA 2013, 309, 1359–1367. [Google Scholar] [CrossRef] [PubMed]
- Cavanagh, P.; Derr, J.; Ulbrecht, J.; Maser, R.; Orchard, T. Problems with gait and posture in neuropathic patients with insulin-Dependent diabetes mellitus. Diabet. Med. 1992, 9, 469–474. [Google Scholar] [CrossRef] [PubMed]
- Richardson, J.K.; Ching, C.; Hurvitz, E.A. The relationship between electromyographically documented peripheral neuropatny and falls. J. Am. Geriatr. Soc. 1992, 40, 1008–1012. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DeMott, T.K.; Richardson, J.K.; Thies, S.B.; Ashton-Miller, J.A. Falls and gait characteristics among older persons with peripheral neuropathy. Am. J. Phys. Med. Rehabil. 2007, 86, 125–132. [Google Scholar] [CrossRef] [PubMed]
- Tofthagen, C.; Overcash, J.; Kip, K. Falls in persons with chemotherapy-Induced peripheral neuropathy. Supportive Care Cancer 2012, 20, 583–589. [Google Scholar] [CrossRef]
- Marshall, T.F.; Zipp, G.P.; Battaglia, F.; Moss, R.; Bryan, S. Chemotherapy-Induced-Peripheral neuropathy, gait and fall risk in older adults following cancer treatment. J. Cancer Res. Pract. 2017, 4, 134–138. [Google Scholar] [CrossRef]
- Hewston, P.; Deshpande, N. Falls and balance impairments in older adults with type 2 diabetes: Thinking beyond diabetic peripheral neuropathy. Can. J. Diabetes 2016, 40, 6–9. [Google Scholar] [CrossRef] [Green Version]
- Vaz, M.M.; Costa, G.C.; Reis, J.G.; Junior, W.M.; de Paula, F.J.A.; Abreu, D.C. Postural control and functional strength in patients with type 2 diabetes mellitus with and without peripheral neuropathy. Arch. Phys. Med. Rehabil. 2013, 94, 2465–2470. [Google Scholar] [CrossRef]
- Hutchinson, A.D.; Hosking, J.R.; Kichenadasse, G.; Mattiske, J.K.; Wilson, C. Objective and subjective cognitive impairment following chemotherapy for cancer: A systematic review. Cancer Treat. Rev. 2012, 38, 926–934. [Google Scholar] [CrossRef] [PubMed]
- Tannock, I.F.; Ahles, T.A.; Ganz, P.A.; van Dam, F.S. Cognitive impairment associated with chemotherapy for cancer: Report of a workshop. J. Clin. Oncol. 2004, 22, 2233–2239. [Google Scholar] [CrossRef] [PubMed]
- Gregg, E.W.; Yaffe, K.; Cauley, J.A.; Rolka, D.B.; Blackwell, T.L.; Narayan, K.V.; Cummings, S.R. Is diabetes associated with cognitive impairment and cognitive decline among older women? Arch. Intern. Med. 2000, 160, 174–180. [Google Scholar] [CrossRef] [Green Version]
- Luchsinger, J.A.; Reitz, C.; Patel, B.; Tang, M.-X.; Manly, J.J.; Mayeux, R. Relation of diabetes to mild cognitive impairment. Arch. Neurol. 2007, 64, 570–575. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Horak, F.B. Postural orientation and equilibrium: What do we need to know about neural control of balance to prevent falls? Age Ageing 2006, 35, ii7–ii11. [Google Scholar] [CrossRef] [Green Version]
- Delbaere, K.; Kochan, N.A.; Close, J.C.; Menant, J.C.; Sturnieks, D.L.; Brodaty, H.; Sachdev, P.S.; Lord, S.R. Mild cognitive impairment as a predictor of falls in community-Dwelling older people. Am. J. Geriatr. Psychiatry 2012, 20, 845–853. [Google Scholar] [CrossRef]
- Taylor, M.E.; Delbaere, K.; Mikolaizak, A.S.; Lord, S.R.; Close, J.C. Gait parameter risk factors for falls under simple and dual task conditions in cognitively impaired older people. Gait Posture 2013, 37, 126–130. [Google Scholar] [CrossRef]
- Woollacott, M.; Shumway-Cook, A. Attention and the control of posture and gait: A review of an emerging area of research. Gait Posture 2002, 16, 1–14. [Google Scholar] [CrossRef]
- Beauchet, O.; Dubost, V.; Herrmann, F.R.; Kressig, R.W. Stride-To-Stride variability while backward counting among healthy young adults. J. Neuroeng. Rehabil. 2005, 2, 26. [Google Scholar] [CrossRef]
- Bahureksa, L.; Najafi, B.; Saleh, A.; Sabbagh, M.; Coon, D.; Mohler, M.J.; Schwenk, M. The impact of mild cognitive impairment on gait and balance: A systematic review and meta-Analysis of studies using instrumented assessment. Gerontology 2017, 63, 67–83. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dubost, V.; Annweiler, C.; Aminian, K.; Najafi, B.; Herrmann, F.R.; Beauchet, O. Stride-To-Stride variability while enumerating animal names among healthy young adults: Result of stride velocity or effect of attention-Demanding task? Gait Posture 2008, 27, 138–143. [Google Scholar] [CrossRef]
- Buracchio, T.; Dodge, H.H.; Howieson, D.; Wasserman, D.; Kaye, J. The trajectory of gait speed preceding mild cognitive impairment. Arch. Neurol. 2010, 67, 980–986. [Google Scholar] [CrossRef] [PubMed]
- Montero-Odasso, M.; Muir, S.W.; Speechley, M. Dual-Task complexity affects gait in people with mild cognitive impairment: The interplay between gait variability, dual tasking, and risk of falls. Arch. Phys. Med. Rehabil. 2012, 93, 293–299. [Google Scholar] [CrossRef] [PubMed]
- Plummer-D′Amato, P.; Altmann, L.J.; Saracino, D.; Fox, E.; Behrman, A.L.; Marsiske, M. Interactions between cognitive tasks and gait after stroke: A dual task study. Gait Posture 2008, 27, 683–688. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kastavelis, D.; Mukherjee, M.; Decker, L.M.; Stergiou, N. The effect of virtual reality on gait variability. Nonlinear Dyn. Psychol. Life Sci. 2010, 14, 239–256. [Google Scholar]
- McAndrew, P.M.; Dingwell, J.B.; Wilken, J.M. Walking variability during continuous pseudo-Random oscillations of the support surface and visual field. J. Biomech. 2010, 43, 1470–1475. [Google Scholar] [CrossRef] [Green Version]
- Galna, B.; Lord, S.; Rochester, L. Is gait variability reliable in older adults and Parkinson’s disease? Towards an optimal testing protocol. Gait Posture 2013, 37, 580–585. [Google Scholar] [CrossRef]
- Paterson, K.L.; Lythgo, N.D.; Hill, K.D. Gait variability in younger and older adult women is altered by overground walking protocol. Age Ageing 2009, 38, 745–748. [Google Scholar] [CrossRef] [Green Version]
- Kang, G.E.; Gross, M.M. Concurrent validation of magnetic and inertial measurement units in estimating upper body posture during gait. Measurement 2016, 82, 240–245. [Google Scholar] [CrossRef]
- Najafi, B.; Helbostad, J.L.; Moe-Nilssen, R.; Zijlstra, W.; Aminian, K. Does walking strategy in older people change as a function of walking distance? Gait Posture 2009, 29, 261–266. [Google Scholar] [CrossRef] [PubMed]
- Najafi, B.; Crews, R.T.; Wrobel, J.S. A novel plantar stimulation technology for improving protective sensation and postural control in patients with diabetic peripheral neuropathy: A double-Blinded, randomized study. Gerontology 2013, 59, 473–480. [Google Scholar] [CrossRef] [PubMed]
- Kang, G.E.; Zahiri, M.; Lepow, B.; Saleem, N.; Najafi, B. The Effect of Daily Use of Plantar Mechanical Stimulation Through Micro-Mobile Foot Compression Device Installed in Shoe Insoles on Vibration Perception, Gait, and Balance in People With Diabetic Peripheral Neuropathy. J. Diabetes Sci. Technol. 2019, 13, 847–856. [Google Scholar] [CrossRef] [PubMed]
- Najafi, B.; Talal, T.K.; Grewal, G.S.; Menzies, R.; Armstrong, D.G.; Lavery, L.A. Using plantar electrical stimulation to improve postural balance and plantar sensation among patients with diabetic peripheral neuropathy: A randomized double blinded study. J. Diabetes Sci. Technol. 2017, 11, 693–701. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kang, G.E.; Zhou, H.; Varghese, V.; Najafi, B. Characteristics of the gait initiation phase in older adults with diabetic peripheral neuropathy compared to control older adults. Clin. Biomech. 2020, 72, 155–160. [Google Scholar] [CrossRef] [PubMed]
- Kang, G.E.; Najafi, B. Sensor-Based Daily Physical Activity: Towards Prediction of the Level of Concern about Falling in Peripheral Neuropathy. Sensors 2020, 20, 505. [Google Scholar] [CrossRef] [Green Version]
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A brief screening tool for mild cognitive impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef]
- Carson, N.; Leach, L.; Murphy, K.J. A re-Examination of Montreal Cognitive Assessment (MoCA) cutoff scores. Int. J. Geriatr. Psychiatry 2018, 33, 379–388. [Google Scholar] [CrossRef]
- Ehsani, H.; Mohler, M.J.; O′Connor, K.; Zamrini, E.; Tirambulo, C.; Toosizadeh, N. The association between cognition and dual-Tasking among older adults: The effect of motor function type and cognition task difficulty. Clin. Interv. Aging 2019, 14, 659–669. [Google Scholar] [CrossRef] [Green Version]
- Choi, J.S.; Seo, J.W.; Lee, J.S.; Kim, J.G.; Cho, J.H.; Tack, G.R. measurement system for delay-Time of gait event due to a dual-Task during walking. J. Mech. Med. Biol. 2019, 19, 1940064. [Google Scholar] [CrossRef]
- Radloff, L.S. The CES-D scale: A self-Report depression scale for research in the general population. Appl. Psychol. Meas. 1977, 1, 385–401. [Google Scholar] [CrossRef]
- Yardley, L.; Beyer, N.; Hauer, K.; Kempen, G.; Piot-Ziegler, C.; Todd, C. Development and initial validation of the Falls Efficacy Scale-International (FES-I). Age Ageing 2005, 34, 614–619. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Delbaere, K.; Close, J.C.; Heim, J.; Sachdev, P.S.; Brodaty, H.; Slavin, M.J.; Kochan, N.A.; Lord, S.R. A multifactorial approach to understanding fall risk in older people. J. Am. Geriatr. Soc. 2010, 58, 1679–1685. [Google Scholar] [CrossRef]
- Aminian, K.; Najafi, B.; Büla, C.; Leyvraz, P.-F.; Robert, P. Spatio-Temporal parameters of gait measured by an ambulatory system using miniature gyroscopes. J. Biomech. 2002, 35, 689–699. [Google Scholar] [CrossRef]
- Plummer, P.; Grewal, G.; Najafi, B.; Ballard, A. Instructions and skill level influence reliability of dual-Task performance in young adults. Gait Posture 2015, 41, 964–967. [Google Scholar] [CrossRef] [PubMed]
- Feld, J.A.; Zukowski, L.A.; Howard, A.G.; Giuliani, C.A.; Altmann, L.J.; Najafi, B.; Plummer, P. Relationship Between Dual-Task Gait Speed and Walking Activity Poststroke. Stroke 2018, 49, 1296–1298. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. A power primer. Psychol. Bull. 1992, 112, 155. [Google Scholar] [CrossRef] [PubMed]
- Najafi, B.; Horn, D.; Marclay, S.; Crews, R.T.; Wu, S.; Wrobel, J.S. Assessing Postural Control and Postural Control Strategy in Diabetes Patients Using Innovative and Wearable Technology. J. Diabetes Sci. Technol. 2010, 4, 780–791. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muir, S.W.; Speechley, M.; Wells, J.; Borrie, M.; Gopaul, K.; Montero-Odasso, M. Gait assessment in mild cognitive impairment and Alzheimer′s disease: The effect of dual-task challenges across the cognitive spectrum. Gait Posture 2012, 35, 96–100. [Google Scholar] [CrossRef]
- De Mettelinge, T.R.; Delbaere, K.; Calders, P.; Gysel, T.; Van Den Noortgate, N.; Cambier, D. The impact of peripheral neuropathy and cognitive decrements on gait in older adults with type 2 diabetes mellitus. Arch. Phys. Med. Rehabil. 2013, 94, 1074–1079. [Google Scholar] [CrossRef]
- Hausdorff, J.M.; Rios, D.A.; Edelberg, H.K. Gait variability and fall risk in community-Living older adults: A 1-Year prospective study. Arch. Phys. Med. Rehabil. 2001, 82, 1050–1056. [Google Scholar] [CrossRef] [PubMed]
- Ambrose, A.F.; Paul, G.; Hausdorff, J.M. Risk factors for falls among older adults: A review of the literature. Maturitas 2013, 75, 51–61. [Google Scholar] [CrossRef] [PubMed]
- Lundin-Olsson, L.; Nyberg, L.; Gustafson, Y. Stops walking when talking as a predictor of falls in elderly people. Lancet 1997, 349, 617. [Google Scholar] [CrossRef]
- Armstrong, D.G.; Najafi, B.; Shahinpoor, M. Potential applications of smart multifunctional wearable materials to gerontology. Gerontology 2017, 63, 287–298. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Measures | PN without Cognitive Impairment (N = 25) | PN with Cognitive Impairment (N = 19) | p-Value |
|---|---|---|---|
| Age, years | 66.5 ± 9.1 | 68.5 ± 9.1 | 0.324 |
| Body mass index, kg/m2 | 31.3 ± 5.9 | 29.0 ± 6.2 | 0.228 |
| Men:Women, N | 15:10 | 8:11 | 0.888 |
| VPT, volts | 26.3 ± 12.7 | 27.2 ± 12.1 | 0.813 |
| MoCA | 25.6 ± 1.6 | 19.6 ± 2.4 | <0.001 * |
| CES-D | 6.6 ± 8.2 | 9.1 ± 6.7 | 0.125 |
| Risk of depression, N | 2 | 4 | 0.184 |
| FES-I | 29.3 ± 14.7 | 35.2 ± 14.0 | 0.073 |
| Moderate to high fear of fall, N | 17 | 17 | 0.092 |
| People who fell in the past year, N | 8 | 7 | 0.737 |
| Number of falls in the past year, N | 0.9 ± 2.1 | 0.6 ± 1.1 | 0.866 |
| Measures | PN without Cognitive Impairment | PN with Cognitive Impairment | p-Value | Cohen’s d |
|---|---|---|---|---|
| Single-task walking | ||||
| Gait speed, m/s | 0.96 ± 0.18 | 0.87 ± 0.27 | 0.236 | 0.39 S |
| Stride length, meters | 1.16 ± 0.19 | 1.04 ± 0.28 | 0.160 | 0.50 M |
| Stride Time, seconds | 1.23 ± 0.13 | 1.23 ± 0.12 | 0.855 | 0.00 N |
| CV of gait speed, % | 7.21 ± 3.34 | 7.73 ± 3.63 | 0.804 | 0.15 N |
| CV of stride length, % | 6.12 ± 4.29 | 5.62 ± 3.48 | 0.615 | 0.13 N |
| CV of stride time, % | 4.10 ± 1.59 | 4.18 ±1.99 | 0.905 | 0.04 N |
| Dual-task walking | ||||
| Gait speed, m/s | 0.84 ± 0.16 | 0.76 ± 0.28 | 0.300 | 0.35 S |
| Stride length, m | 1.14 ± 0.16 | 1.01 ± 0.28 | 0.060 † | 0.57 M |
| Stride Time, s | 1.40 ± 0.17 | 1.39 ± 0.24 | 0.937 | 0.05 N |
| CV of gait speed, % | 7.31 ± 3.20 | 11.07 ± 5.22 | 0.014 * | 0.87 L |
| CV of stride length, % | 4.81 ± 2.80 | 8.23 ± 4.66 | 0.011 * | 0.89 L |
| CV of stride time, % | 4.89 ± 2.14 | 6.78 ± 4.60 | 0.119 | 0.53 M |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kang, G.E.; Yang, J.; Najafi, B. Does the Presence of Cognitive Impairment Exacerbate the Risk of Falls in People with Peripheral Neuropathy? An Application of Body-Worn Inertial Sensors to Measure Gait Variability. Sensors 2020, 20, 1328. https://doi.org/10.3390/s20051328
Kang GE, Yang J, Najafi B. Does the Presence of Cognitive Impairment Exacerbate the Risk of Falls in People with Peripheral Neuropathy? An Application of Body-Worn Inertial Sensors to Measure Gait Variability. Sensors. 2020; 20(5):1328. https://doi.org/10.3390/s20051328
Chicago/Turabian StyleKang, Gu Eon, Jacqueline Yang, and Bijan Najafi. 2020. "Does the Presence of Cognitive Impairment Exacerbate the Risk of Falls in People with Peripheral Neuropathy? An Application of Body-Worn Inertial Sensors to Measure Gait Variability" Sensors 20, no. 5: 1328. https://doi.org/10.3390/s20051328