Situation Awareness-Oriented Patient Monitoring with Visual Patient Technology: A Qualitative Review of the Primary Research


 , ,
, ,  ,
, 
Abstract

1. Introduction
1.1. Situation Awareness
1.2. State-of-the-Art Patient Monitoring
1.2.1. Scope of the Area of Application
1.2.2. Limitations of Current Patient Monitors
1.2.3. Patient Monitoring in Clinical Reality
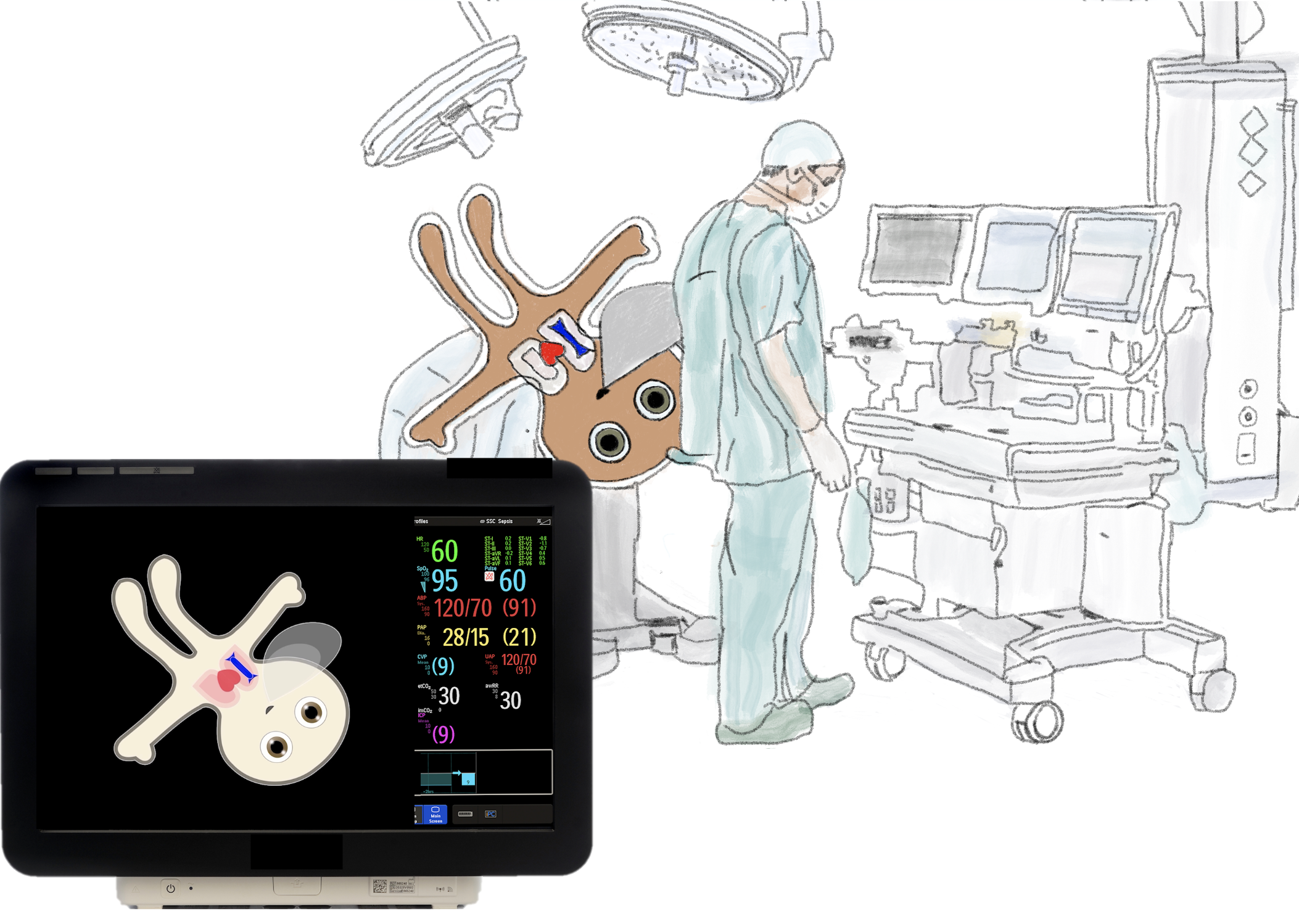
1.3. Visual Patient Technology
1.4. Synthetic Vision, Aviation, and Visual Patient
1.5. Design Philosophy and Scientific Context
2. Characteristics of the Visual Patient Technology
2.1. Display of High-Order Information Synthesized in One Picture (Multiple-Sensor-Multiple-Indicator Philosophy)
2.2. Preprocessing (Simplification) of Data
2.3. Direct (Logical) Presentation of Information
2.4. Parallel Information Transfer
2.5. Peripheral Vision Monitoring
2.6. Limitations of Visual Patient
3. Qualitative Review of the Studies Conducted to Date
3.1. Data Collection Tool
3.2. Visual Patient Series 1
3.2.1. Development and Validation of the Visual Patient Design
3.2.2. Visual Patient Versus Conventional Monitor
3.2.3. User Perceptions
3.2.4. Eye Tracking
3.3. Visual Patient Series 2
3.3.1. Peripheral Vision
3.3.2. Distractions
3.3.3. Monitoring Multiple Patients
3.3.4. Individual Versus Class Instruction in an Auditorium
4. Discussion
4.1. Vital Sign Perception
4.2. Perceived Workload
4.3. Perceived Diagnostic Certainty
4.4. Learnability
4.5. Visual Patient and Relevant Patient Monitoring Aspects
4.5.1. Alarm Fatigue
4.5.2. Artifacts
4.5.3. Trend Monitoring
4.5.4. Pattern Recognition
4.5.5. Event Monitoring
4.6. Impressions from Performing Studies with the Technology
4.7. Strengths and Limitations of the Reviewed Studies
4.8. Overview of Other Studies
5. Conclusions
6. Patents
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Ethical Statements
References
- Tscholl, D.W.; Handschin, L.; Neubauer, P.; Weiss, M.; Seifert, B.; Spahn, D.R.; Noethiger, C.B. Using an animated patient avatar to improve perception of vital sign information by anaesthesia professionals. Br. J. Anaesth. 2018, 121, 662–671. [Google Scholar] [CrossRef] [PubMed]
- Tscholl, D.W.; Weiss, M.; Handschin, L.; Spahn, D.R.; Nothiger, C.B. User perceptions of avatar-based patient monitoring: A mixed qualitative and quantitative study. BMC Anesthesiol. 2018, 18, 188. [Google Scholar] [CrossRef] [PubMed]
- Tscholl, D.W.; Rössler, J.; Handschin, L.; Seifert, B.; Spahn, D.R.; Nöthiger, C.B. The mechanisms responsible for improved information transfer in avatar-based patient monitoring: A Multicenter Comparative Eye-Tracking Study. J. Med. Internet Res. 2020. [Google Scholar] [CrossRef] [PubMed]
- Pfarr, J.; Ganter, M.T.; Spahn, D.R.; Noethiger, C.B.; Tscholl, D.W. Avatar-Based Patient Monitoring With Peripheral Vision: A Multicenter Comparative Eye-Tracking Study. J. Med. Internet Res. 2019, 21, e13041. [Google Scholar] [CrossRef]
- Garot, O.; Rössler, J.; Pfarr, J.; Ganter, M.T.; Spahn, D.R.; Nöthiger, C.B.; Tscholl, D.W. Avatar-based versus conventional vital sign display in a central monitor for monitoring multiple patients: A multicenter computer-based laboratory study. BMC Med. Inform. Decis Mak. 2020, 20, 26. [Google Scholar] [CrossRef]
- Pfarr, J.; Ganter, M.T.; Spahn, D.R.; Noethiger, C.B.; Tscholl, D.W. Effects of a standardized distraction on caregivers’ perceptive performance with avatar-based and conventional patient monitoring: A multicenter comparative study. J. Clin. Monit. Comput. 2019, 25. [Google Scholar] [CrossRef]
- Rössler, J.; Kaserer, A.; Albiez, B.; Braun, J.; Breckwoldt, J.; Spahn, D.R.; Nöthiger, C.B.; Tscholl, D.W. Comparing classroom instruction to individual instruction as a teaching approach to avatar-based monitoring system with the “Visual Patient”: An experimental study. JMIR Med. Educ. 2020. [Google Scholar] [CrossRef]
- Endsley, M.R. Designing for Situation Awareness: An. Approach to User-Centered Design, 2nd ed.; CRC Press Inc.: Boca Raton, FL, USA, 2011. [Google Scholar]
- Schulz, C.M.; Endsley, M.R.; Kochs, E.F.; Gelb, A.W.; Wagner, K.J. Situation awareness in anesthesia: Concept and research. Anesthesiology 2013, 118, 729–742. [Google Scholar] [CrossRef]
- Fioratou, E.; Flin, R.; Glavin, R.; Patey, R. Beyond monitoring: Distributed situation awareness in anaesthesia. Br. J. Anaesth. 2010, 105, 83–90. [Google Scholar] [CrossRef]
- Gaba, D.M.; Howard, S.K.; Small, S.D. Situation awareness in anesthesiology. Hum. Factors 1995, 37, 20–31. [Google Scholar] [CrossRef]
- Schulz, C.M.; Krautheim, V.; Hackemann, A.; Kreuzer, M.; Kochs, E.F.; Wagner, K.J. Situation awareness errors in anesthesia and critical care in 200 cases of a critical incident reporting system. BMC Anesthesiol. 2016, 16, 4. [Google Scholar] [CrossRef] [PubMed]
- Schulz, C.M.; Burden, A.; Posner, K.L.; Mincer, S.L.; Steadman, R.; Wagner, K.J.; Domino, K.B. Frequency and Type of Situational Awareness Errors Contributing to Death and Brain Damage: A Closed Claims Analysis. Anesthesiology 2017, 127, 326–337. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Guidelines for Safe Surgery 2009: Safe Surgery Saves Lives; World Health Organization: Geneva, Switzerland, 2009; Available online: https://www.who.int/patientsafety/safesurgery/tools_resources/9789241598552/en/ (accessed on 29 February 2020).
- Moller, J.T.; Jensen, P.F.; Johannessen, N.W.; Espersen, K. Hypoxaemia is reduced by pulse oximetry monitoring in the operating theatre and in the recovery room. Br. J. Anaesth. 1992, 68, 146–150. [Google Scholar] [CrossRef]
- Moller, J.T.; Johannessen, N.W.; Espersen, K.; Ravlo, O.; Pedersen, B.D.; Jensen, P.F.; Rasmussen, N.H.; Rasmussen, L.S.; Pedersen, T.; Cooper, J.B.; et al. Randomized evaluation of pulse oximetry in 20;802 patients: II. Perioperative events and postoperative complications. Anesthesiology 1993, 78, 445–453. [Google Scholar] [CrossRef] [PubMed]
- Coté, C.J.; Rolf, N.; Liu, L.M.; Goudsouzian, N.G.; Ryan, J.F.; Zaslavsky, A.; Gore, R.; Todres, T.D.; Vassallo, S.; Polaner, D.; et al. A single-blind study of combined pulse oximetry and capnography in children. Anesthesiology 1991, 74, 980–987. [Google Scholar] [CrossRef] [PubMed]
- Weiser, T.G.; Haynes, A.B.; Molina, G.; Lipsitz, S.R.; Esquivel, M.M.; Uribe-Leitz, T.; Fu, R.; Azad, T.; Chao, T.E.; Berry, W.R.; et al. Size and distribution of the global volume of surgery in 2012. Bull. World Health Organ. 2016, 94, 201–209F. [Google Scholar] [CrossRef] [PubMed]
- Michard, F.; Sessler, D.I. Ward monitoring 3.0. Br. J. Anaesth. 2018, 121, 999–1001. [Google Scholar] [CrossRef]
- Schlosser, P.D.; Grundgeiger, T.; Sanderson, P.M.; Happel, O. An exploratory clinical evaluation of a head-worn display based multiple-patient monitoring application: Impact on supervising anesthesiologists’ situation awareness. J. Clin. Monit. Comput. 2019, 33, 1119–1127. [Google Scholar] [CrossRef]
- Downey, C.L.; Brown, J.M.; Jayne, D.G.; Randell, R. Patient attitudes towards remote continuous vital signs monitoring on general surgery wards: An interview study. Int. J. Med. Inform. 2018, 114, 52–56. [Google Scholar] [CrossRef]
- Boer, C.; Touw, H.R.; Loer, S.A. Postanesthesia care by remote monitoring of vital signs in surgical wards. Curr. Opin Anaesthesiol. 2018, 31, 716–722. [Google Scholar] [CrossRef]
- Yilmaz, T.; Foster, R.; Hao, Y. Detecting vital signs with wearable wireless sensors. Sensors 2010, 10, 10837–10862. [Google Scholar] [CrossRef] [PubMed]
- Drews, F.A.; Westenskow, D.R. The right picture is worth a thousand numbers: Data displays in anesthesia. Hum. Factors 2006, 48, 59–71. [Google Scholar] [CrossRef] [PubMed]
- Rayner, K. Eye movements in reading and information processing: 20 years of research. Psychol. Bull. 1998, 124, 372–422. [Google Scholar] [CrossRef] [PubMed]
- Miller, G.A. The magical number seven plus or minus two: Some limits on our capacity for processing information. Psychol. Rev. 1956, 63, 81–97. [Google Scholar] [CrossRef] [PubMed]
- Holmqvist, K. Eye Tracking: A Comprehensive Guide to Methods and Measures; Oxford University Press: Oxford, UK, 2011. [Google Scholar]
- Ford, S.; Birmingham, E.; King, A.; Lim, J.; Ansermino, J.M. At-a-glance monitoring: Covert observations of anesthesiologists in the operating room. Anesth. Analg. 2010, 111, 653–658. [Google Scholar] [CrossRef]
- Loeb, R.G. Monitor surveillance and vigilance of anesthesia residents. Anesthesiology 1994, 80, 527–533. [Google Scholar] [CrossRef]
- Rock, I.; Linnett, C.M.; Grant, P.; Mack, A. Perception without attention: Results of a new method. Cogn. Psychol. 1992, 24, 502–534. [Google Scholar] [CrossRef]
- Mack, A.; Pappas, Z.; Silverman, M.; Gay, R. What we see: Inattention and the capture of attention by meaning. Conscious. Cogn. 2002, 11, 488–506. [Google Scholar] [CrossRef]
- Simons, D.J. Attentional capture and inattentional blindness. Trends Cogn. Sci. 2000, 4, 147–155. [Google Scholar] [CrossRef]
- Simons, D.J.; Chabris, C.F. Gorillas in Our Midst: Sustained Inattentional Blindness for Dynamic Events. Perception 1999, 28, 1059–1074. [Google Scholar] [CrossRef]
- Broom, M.A.; Capek, A.L.; Carachi, P.; Akeroyd, M.A.; Hilditch, G. Critical phase distractions in anaesthesia and the sterile cockpit concept. Anaesthesia 2011, 66, 175–179. [Google Scholar] [CrossRef] [PubMed]
- Campbell, G.; Arfanis, K.; Smith, A.F. Distraction and interruption in anaesthetic practice. Br. J. Anaesth. 2012, 109, 707–715. [Google Scholar] [CrossRef] [PubMed]
- Crockett, C.J.; Donahue, B.S.; Vandivier, D.C. Distraction-Free Induction Zone: A Quality Improvement Initiative at a Large Academic Children’s Hospital to Improve the Quality and Safety of Anesthetic Care for Our Patients. Anesth. Analg. 2019, 129, 794–803. [Google Scholar] [CrossRef]
- Jenkins, A.; Wilkinson, J.V.; Akeroyd, M.A.; Broom, M.A. Distractions during critical phases of anaesthesia for caesarean section: An observational study. Anaesthesia 2015, 70, 543–548. [Google Scholar] [CrossRef] [PubMed]
- Van Pelt, M.; Weinger, M.B. Distractions in the Anesthesia Work Environment: Impact on Patient Safety? Report of a Meeting Sponsored by the Anesthesia Patient Safety Foundation. Anesth. Analg. 2017. [Google Scholar] [CrossRef]
- Slagle, J.M.; Porterfield, E.S.; Lorinc, A.N.; Afshartous, D.; Shotwell, M.S.; Weinger, M.B. Prevalence of Potentially Distracting Noncare Activities and Their Effects on Vigilance; Workload; and Nonroutine Events during Anesthesia Care. Anesthesiology 2018, 128, 44–54. [Google Scholar] [CrossRef]
- McGowan, G.; Jawaheer, L.; Young, D.; Yorston, D. QUIET PLEASE! Effect of distraction on simulated posterior segment surgical performance. Graefes Arch. Clin. Exp. Ophthalmol. 2018, 256, 519–523. [Google Scholar] [CrossRef]
- Craik, F.I. Effects of distraction on memory and cognition: A commentary. Front. Psychol. 2014, 5, 841. [Google Scholar] [CrossRef]
- Tscholl, D.W.; Handschin, L.; Rossler, J.; Weiss, M.; Spahn, D.R.; Nothiger, C.B. It’s not you; it’s the design—common problems with patient monitoring reported by anesthesiologists: A mixed qualitative and quantitative study. BMC Anesthesiol. 2019, 19, 87. [Google Scholar] [CrossRef]
- Knox, C.E.; Leavitt, J. NASA Technical Memorandum 74057: Description of Path-in-the-Sky Contact Analog Piloting Display; NASA Langley Research Center: Hampton, VA, USA, 1977.
- Way, T.; Hornsby, M.; Gilmour, J.; Edwards, R.; Hobbs, R. Pictorial Format Display Evaluation; Flight Dynamics Laboratory: Wright-Patterson Airforce Base, OH, USA, 1984. [Google Scholar]
- Wittgenstein, L. Tractatus Logico-Philosophicus; Routledge & Kegan Paul: London, UK, 1922. [Google Scholar]
- Degani, A.; Jorgensen, D.; Iverson, D.L.; Shafto, M.; Olson, L. On Organization of Information: Approach and Early Work; NASA Ames Research Center: Moffet Field, CA, USA, 2009.
- Tscholl, D.W.; Weiss, M.; Spahn, D.R.; Noethiger, C.B. How to Conduct Multimethod Field Studies in the Operating Room: The iPad Combined With a Survey App as a Valid and Reliable Data Collection Tool. JMIR Res. Protoc. 2016, 5, e4. [Google Scholar] [CrossRef]
- Tscholl, D.W.; Weiss, M.; Kolbe, M.; Staender, S.; Seifert, B.; Landert, D.; Grande, B.; Spahn, D.R.; Noethiger, C.B. An Anesthesia Preinduction Checklist to Improve Information Exchange; Knowledge of Critical Information; Perception of Safety; and Possibly Perception of Teamwork in Anesthesia Teams. Anesth. Analg. 2015, 121, 948–956. [Google Scholar] [CrossRef] [PubMed]
- Kandler, L.; Tscholl, D.W.; Kolbe, M.; Seifert, B.; Spahn, D.R.; Noethiger, C.B. Using educational video to enhance protocol adherence for medical procedures. Br. J. Anaesth. 2016, 116, 662–669. [Google Scholar] [CrossRef] [PubMed]
- Hart, S.G. Nasa-Task Load Index (NASA-TLX); 20 Years Later. Proc. Hum. Factors Ergon. Soc. Annu. Meet. 2006, 50, 904–908. [Google Scholar] [CrossRef]
- Mazur, L.M.; Mosaly, P.R.; Moore, C.; Comitz, E.; Yu, F.; Falchook, A.D.; Eblan, M.J.; Hoyle, L.M.; Tracton, G.; Chera, B.S.; et al. Toward a better understanding of task demands; workload; and performance during physician-computer interactions. J. Am. Med. Inform. Assoc. 2016, 23, 1113–1120. [Google Scholar] [CrossRef]
- Finomore, V.S., Jr.; Shaw, T.H.; Warm, J.S.; Matthews, G.; Boles, D.B. Viewing the workload of vigilance through the lenses of the NASA-TLX and the MRQ. Hum. Factors 2013, 55, 1044–1063. [Google Scholar] [CrossRef]
- Wheelock, A.; Suliman, A.; Wharton, R.; Babu, E.D.; Hull, L.; Vincent, C.; Sevdalis, N.; Arora, S. The Impact of Operating Room Distractions on Stress; Workload; and Teamwork. Ann. Surg. 2015, 261, 1079–1084. [Google Scholar] [CrossRef]
- Tombaugh, T.N. A comprehensive review of the Paced Auditory Serial Addition Test (PASAT). Arch. Clin. Neuropsychol. 2006, 21, 53–76. [Google Scholar] [CrossRef]
- Prottengeier, J.; Petzoldt, M.; Jess, N.; Moritz, A.; Gall, C.; Schmidt, J.; Breuer, G. The effect of a standardised source of divided attention in airway management: A randomised; crossover; interventional manikin study. Eur. J. Anaesthesiol. 2016, 33, 195–203. [Google Scholar] [CrossRef]
- Lee, K.; Kim, M.J.; Park, J.; Park, J.M.; Kim, K.H.; Shin, D.W.; Kim, H.; Jeon, W.; Kim, H. The effect of distraction by dual work on a CPR practitioner’s efficiency in chest compression: A randomized controlled simulation study. Medicine 2017, 96, e8268. [Google Scholar] [CrossRef]
- Yang, C.; Heinze, J.; Helmert, J.; Weitz, J.; Reissfelder, C.; Mees, S.T. Impaired laparoscopic performance of novice surgeons due to phone call distraction: A single-centre; prospective study. Surg Endosc. 2017, 31, 5312–5317. [Google Scholar] [CrossRef]
- Bauer, M.S.; Damschroder, L.; Hagedorn, H.; Smith, J.; Kilbourne, A.M. An introduction to implementation science for the non-specialist. BMC Psychol. 2015, 3, 32. [Google Scholar] [CrossRef] [PubMed]
- Blackler, A.; Popovic, V.; Mahar, D. Investigating users’ intuitive interaction with complex artefacts. Appl. Ergon. 2010, 41, 72–92. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, R.; Karahanna, E. Time flies when you’re having fun: Cognitive absorption and beliefs about information technology usage. MIS Q. 2000, 24, 665–694. [Google Scholar] [CrossRef]
- Haynes, A.B.; Weiser, T.G.; Berry, W.R.; Lipsitz, S.R.; Breizat, A.H.; Dellinger, E.P.; Herbosa, T.; Joseph, S.; Kibatala, P.L.; Lapitan, M.C.; et al. A surgical safety checklist to reduce morbidity and mortality in a global population. N. Engl. J. Med. 2009, 360, 491–499. [Google Scholar] [CrossRef] [PubMed]
- Arriaga, A.F.; Bader, A.M.; Wong, J.M.; Lipsitz, S.R.; Berry, W.R.; Ziewacz, J.E.; Hepner, D.L.; Boorman, D.J.; Pozner, C.N.; Smink, D.S.; et al. Simulation-based trial of surgical-crisis checklists. N. Engl. J. Med. 2013, 368, 246–253. [Google Scholar] [CrossRef] [PubMed]
- Mehta, N.; Amaranathan, A.; Jayapal, L.; Kundra, P.; Ramakrishnaiah, V.P.N. Effect of Comprehensive Surgical Safety System on Patients’ Outcome: A Prospective Clinical Study. Cureus 2018, 10, e2601. [Google Scholar] [CrossRef]
- Huggins, A.; Claudio, D. A performance comparison between the subjective workload analysis technique and the NASA-TLX in a healthcare setting. IISE Trans. Healthc. Syst. Eng. 2018, 8, 59–71. [Google Scholar] [CrossRef]
- Tubbs-Cooley, H.L.; Mara, C.A.; Carle, A.C.; Gurses, A.P. The NASA Task Load Index as a measure of overall workload among neonatal; paediatric and adult intensive care nurses. Intensive Crit Care Nurs. 2018, 46, 64–69. [Google Scholar] [CrossRef]
- Casner, S.M.; Gore, F.B. Measuring and Evaluating Workload: A Primer; Ames Research Center: Moffet Field, CA, USA, 2010.
- Endsley, M.; Jones, W. Situation Awareness Information Dominance & Information Warfare; United States Airforce: Wright-Patterson Air Force Base, OH, USA, 1997. [Google Scholar]
- Schmid, F.; Goepfert, M.S.; Kuhnt, D.; Eichhorn, V.; Diedrichs, S.; Reichenspurner, H.; Goetz, A.E.; Reuter, D.A. The wolf is crying in the operating room: Patient monitor and anesthesia workstation alarming patterns during cardiac surgery. Anesth. Analg. 2011, 112, 78–83. [Google Scholar] [CrossRef]
- Lawless, S.T. Crying wolf: False alarms in a pediatric intensive care unit. Crit Care Med. 1994, 22, 981–985. [Google Scholar] [CrossRef]
- Schmid, F.; Goepfert, M.S.; Reuter, D.A. Patient monitoring alarms in the ICU and in the operating room. Crit Care 2013, 17, 216. [Google Scholar] [CrossRef] [PubMed]
- Lynn, L.A.; Curry, J.P. Patterns of unexpected in-hospital deaths: A root cause analysis. Patient Saf. Surg. 2011, 5, 3. [Google Scholar] [CrossRef] [PubMed]
- Sangkachand, P.; Sarosario, B.; Funk, M. Continuous ST-segment monitoring: Nurses’ attitudes, practices, and quality of patient care. Am. J. Crit Care. 2011, 20, 226–237. [Google Scholar] [CrossRef]
- Giuliano, K.K.; Jahrsdoerfer, M.; Case, J.; Drew, T.; Raber, G. The role of clinical decision support tools to reduce blood pressure variability in critically ill patients receiving vasopressor support. Comput. Inform. Nurs. 2012, 30, 204–209. [Google Scholar] [CrossRef] [PubMed]
- Agutter, J.; Drews, F.; Syroid, N.; Westneskow, D.; Albert, R.; Strayer, D.; Bermudez, J.; Weinger, M.B. Evaluation of graphic cardiovascular display in a high-fidelity simulator. Anesth. Analg. 2003, 97, 1403–1413. [Google Scholar] [CrossRef] [PubMed]
- Wachter, S.B.; Agutter, J.; Syroid, N.; Drews, F.; Weinger, M.B.; Westenskow, D. The employment of an iterative design process to develop a pulmonary graphical display. J. Am. Med. Inform. Assoc. 2003, 10, 363–372. [Google Scholar] [CrossRef]
- Kheterpal, S.; Shanks, A.; Tremper, K.K. Impact of a Novel Multiparameter Decision Support System on Intraoperative Processes of Care and Postoperative Outcomes. Anesthesiology 2018, 128, 272–282. [Google Scholar] [CrossRef]
- Jungk, A.; Thull, B.; Hoeft, A.; Rau, G. Ergonomic Evaluation of an Ecological Interface and a Profilogram Display for Hemodynamic Monitoring. J. Clin. Monit. Comput. 1999, 15, 469–479. [Google Scholar] [CrossRef]
- Jungk, A.; Thull, B.; Hoeft, A.; Rau, G. Evaluation of two new ecological interface approaches for the anesthesia workplace. J. Clin. Monit. Comput. 2000, 16, 243–258. [Google Scholar] [CrossRef]
- Drews, F.A.; Doig, A. Evaluation of a Configural Vital Signs Display for Intensive Care Unit Nurses. Hum. Factors 2014, 56, 569–580. [Google Scholar] [CrossRef]
- Wright, M.C.; Borbolla, D.; Waller, R.G.; Del Fiol, G.; Reese, T.; Nesbitt, P.; Segall, N. Critical care information display approaches and design frameworks: A systematic review and meta-analysis. J. Biomed. Inform. X 2019, 3. [Google Scholar] [CrossRef]
- Wachter, S.B.; Johnson, K.; Albert, R.; Syroid, N.; Drews, F.; Westenskow, D. The evaluation of a pulmonary display to detect adverse respiratory events using high resolution human simulator. J. Am. Med. Inform. Assoc. 2006, 13, 635–642. [Google Scholar] [CrossRef] [PubMed]
- Rössler, J.; Meybohm, P.; Spahn, D.R.; Zacharowski, K.; Braun, J.; Nöthiger, C.B.; Tscholl, D.W. Improving decision making through presentation of viscoelastic tests as a 3D animated blood clot: The Visual Clot. Anaesthesia 2020. [Google Scholar] [CrossRef] [PubMed]
- Roche, T.R.; Said, S.; Rössler, J.; Godzik, M.; Meybohm, P.; Zacharowski, K.; Spahn, D.R.; Nöthiger, C.B.; Tscholl, D.W. Physician perceptions of Visual Clot—A situation awareness-oriented visualization technology for viscoelastic tests: A mixed methods study. JMIR Preprints 2020, 19036. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
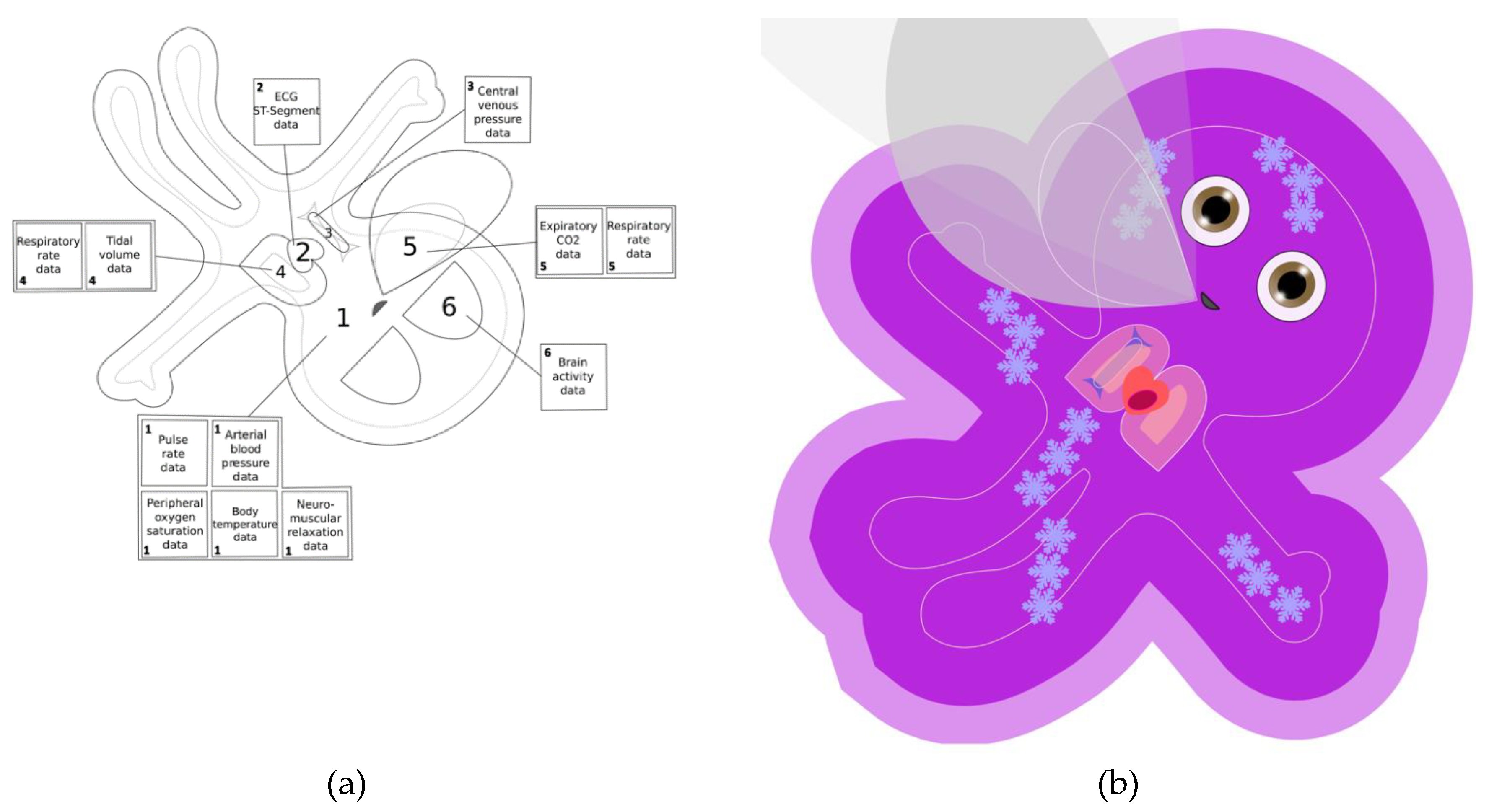
| Vital Sign | Visualization on the Avatar 1 | Phenomenon in the Patient the Visualization is Modeled on |
|---|---|---|
| 1. Pulse rate | The pulsation rate of the body (element #1) of the avatar. Example: The avatar’s body pulsates with a slow, normal, or fast frequency. | The pulsation of the arteries as visible, for example, under a microscope or palpable as a pulse. |
| 2. Arterial blood pressure | The pulsation intensity of the body (element #1) of the avatar. Example: The avatar’s body pulsates just barely normally (i.e., reaching the white line designating the normal pulsation extension) or very intensely, extending far beyond the white “normal” line. | The strength of the pulse in the arteries depending on the arterial blood pressure as visible, for example, under a microscope or palpable as a pulse. |
| 3. Central venous pressure | The area of the vena cava (element #3) of the avatar. Example: The size of the avatar’s vena cava is very small, normal (i.e., reaching the white line designating the normal extension), or very large, far beyond the white “normal line.” | The filling volume of the vena cava depending on central venous pressure. |
| 4. Respiratory rate | The breathing frequency of the lungs (element #4) of the avatar and the corresponding exhalation frequency of the carbon dioxide (CO2) cloud (element #5). Example: The avatar’s lungs breathe with a slow, normal, or high frequency and (if data from a CO2 sensor is available) synchronous slow, normal, or quick exhalation of the CO2 cloud. | The breathing synchronous volume change of the lungs and the breathing synchronous invisible exhalation of a volume of CO2. |
| 5. Tidal volume | The extension size of the lungs (element #4) of the avatar during the breathing cycle. Example: The avatar’s lungs extend just barely, normally (i.e., reaching the white line designating the normal breathing extension) or very far, noticeably beyond the white “normal” line. | The volume change of the lungs depending on tidal volume. |
| 6. Expiratory CO2 concentration | The extension size of the CO2 cloud (element #5) of the avatar during the breathing cycle. Example: The CO2 cloud is just barely visible, reaches a normal extension (i.e., reaching the white line designating the normal breathing extension), or extends very wide, far beyond the white “normal” line. | The volume change of CO2 exhaled into the air. |
| 7. Body temperature | The presence or absence of temperature indicators on the body (element #1) of the avatar. Example: Heat waves are rising from the avatar or ice crystals are visible on its skin. | Hyperthermia: The heat radiation from the skin. Hypothermia: The skin cold to the touch. |
| 8. Brain activity | The form of the eyes (element #6) of the avatar. Example: The eyes of the avatar are open or closed. | High: Eyes open; pupils middle wide as in sympathetic activation. Low: Eyelids completely closed as in a sleeping patient. |
| 9. Peripheral oxygen saturation | The color of the body (element # 1) of the avatar. Example: The avatar has a healthy skin color or a purple skin color. | Normal: Light-brown skin color according to Fitzpatrick skin type III. Hypoxia: Dark purple skin color as in cyanosis. |
| 10. Neuromuscular function | The form of the body (element #1) of the avatar. Example: The avatar has extended extremities and an extended thumb or the extremities appear floppy. | Normal neuromuscular function: Extended extremities and thumb (healthy muscle tone in the adductor policis muscle, where care providers frequently measure relaxation). Neuromuscular block: Floppy limbs. |
| 11. Electrocardiography ST segment | The presence or absence of a hypoxia indicator over the heart (element #2) of the avatar. Example: The heart muscle of the avatar has a homogenous red color or a dark purple spot on the heart. | Normal: Light red color of healthy myocardium. Hypoxia: Purple color of hypoxic myocardium. |
| Study (Year) | Study Type 1 | Participants 2 | Task | Method | Results |
|---|---|---|---|---|---|
| Tscholl et al. (2018) [1] | Within-subject, computer-based | Calibration and validation of avatar: 150 Comparative study: 32 | Interpreting patient monitoring scenarios with Visual Patient and conventional patient monitoring | Iterative development Delphi process Rating of vital signs Rating of diagnostic certainty NASA Task Load Index | Visual Patient showed high high interrater reliability, improved vital sign perception, increased diagnostic confidence, and lowered perceived workload. |
| Tscholl et al. (2018) [2] | Qualitative and quantitative study | Interview part: 128 Quantitative part: 36 | Providing user feedback about Visual Patient | Qualitative analysis of interviews followed by quantitative rating of statements | Visual Patient provided quick situation overview and was easy to learn |
| Pfarr et al. (2019) [4] | Within-subject, computer-based, eye tracking | 30 | Interpreting patient monitoring scenarios with Visual Patient and conventional patient monitoring with peripheral vision | Rating of vital signs Rating of diagnostic certainty Eye-tracking analysis | Visual Patient improved vital sign perception, and increased diagnostic confidence with peripheral vision |
| Pfarr et al. (2019) [6] | Within-subject, computer-based | 38 | Interpreting patient monitoring scenarios with Visual Patient and conventional patient monitoring under distraction | Rating of vital signs NASA Task Load Index | Visual Patient improved vital sign perception and reduced workload under distraction |
| Garot et al. (2020) [5] | Within-subject, computer-based | 38 | Interpreting multiple-patient monitoring scenarios with Visual Patient and conventional patient monitoring | Rating of vital signs NASA Task Load Index | Visual Patient improved vital sign perception and reduced workload under distraction except in 30 s scenarios |
| Tscholl et al. (2020) [3] | Within-subject, computer-based, eye-tracking | 30 | Interpreting patient monitoring scenarios with Visual Patient and conventional patient monitoring | Eye-tracking analysis | Visual Patient enabled parallel perception of vital signs as a result of its visual design |
| Rössler et al. (2020) [7] | Between-subject, computer-based | 42 | Interpreting patient monitoring scenarios with Visual Patient and conventional patient monitoring | Rating of vital signs | Class-based and individual instruction both feasible for Visual Patient training |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tscholl, D.W.; Rössler, J.; Said, S.; Kaserer, A.; Spahn, D.R.; Nöthiger, C.B. Situation Awareness-Oriented Patient Monitoring with Visual Patient Technology: A Qualitative Review of the Primary Research. Sensors 2020, 20, 2112. https://doi.org/10.3390/s20072112
Tscholl DW, Rössler J, Said S, Kaserer A, Spahn DR, Nöthiger CB. Situation Awareness-Oriented Patient Monitoring with Visual Patient Technology: A Qualitative Review of the Primary Research. Sensors. 2020; 20(7):2112. https://doi.org/10.3390/s20072112
Chicago/Turabian StyleTscholl, David Werner, Julian Rössler, Sadiq Said, Alexander Kaserer, Donat Rudolf Spahn, and Christoph Beat Nöthiger. 2020. "Situation Awareness-Oriented Patient Monitoring with Visual Patient Technology: A Qualitative Review of the Primary Research" Sensors 20, no. 7: 2112. https://doi.org/10.3390/s20072112
APA StyleTscholl, D. W., Rössler, J., Said, S., Kaserer, A., Spahn, D. R., & Nöthiger, C. B. (2020). Situation Awareness-Oriented Patient Monitoring with Visual Patient Technology: A Qualitative Review of the Primary Research. Sensors, 20(7), 2112. https://doi.org/10.3390/s20072112