
Thermal Ablation and High-Resolution Imaging Using a Back-to-Back (BTB) Dual-Mode Ultrasonic Transducer: In Vivo Results

 , , , , and
, , , , and 
Abstract
:1. Introduction
2. Materials and Methods
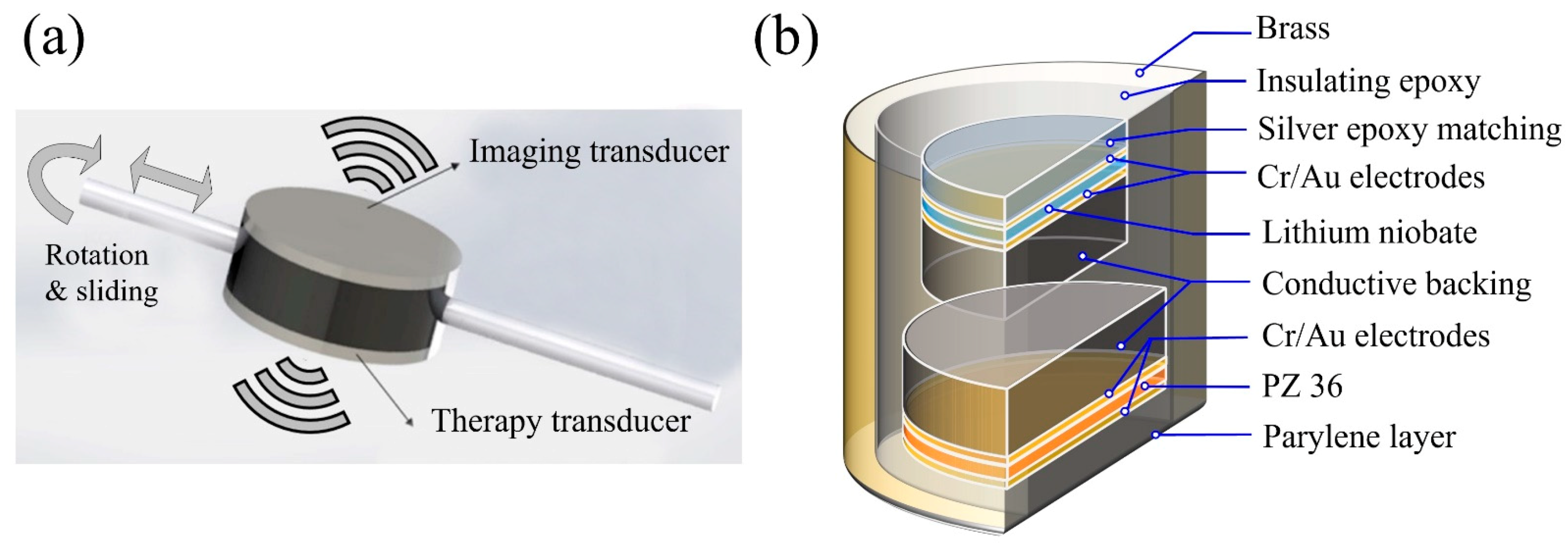
2.1. Fabrication of BTB Dual-Mode Transducer
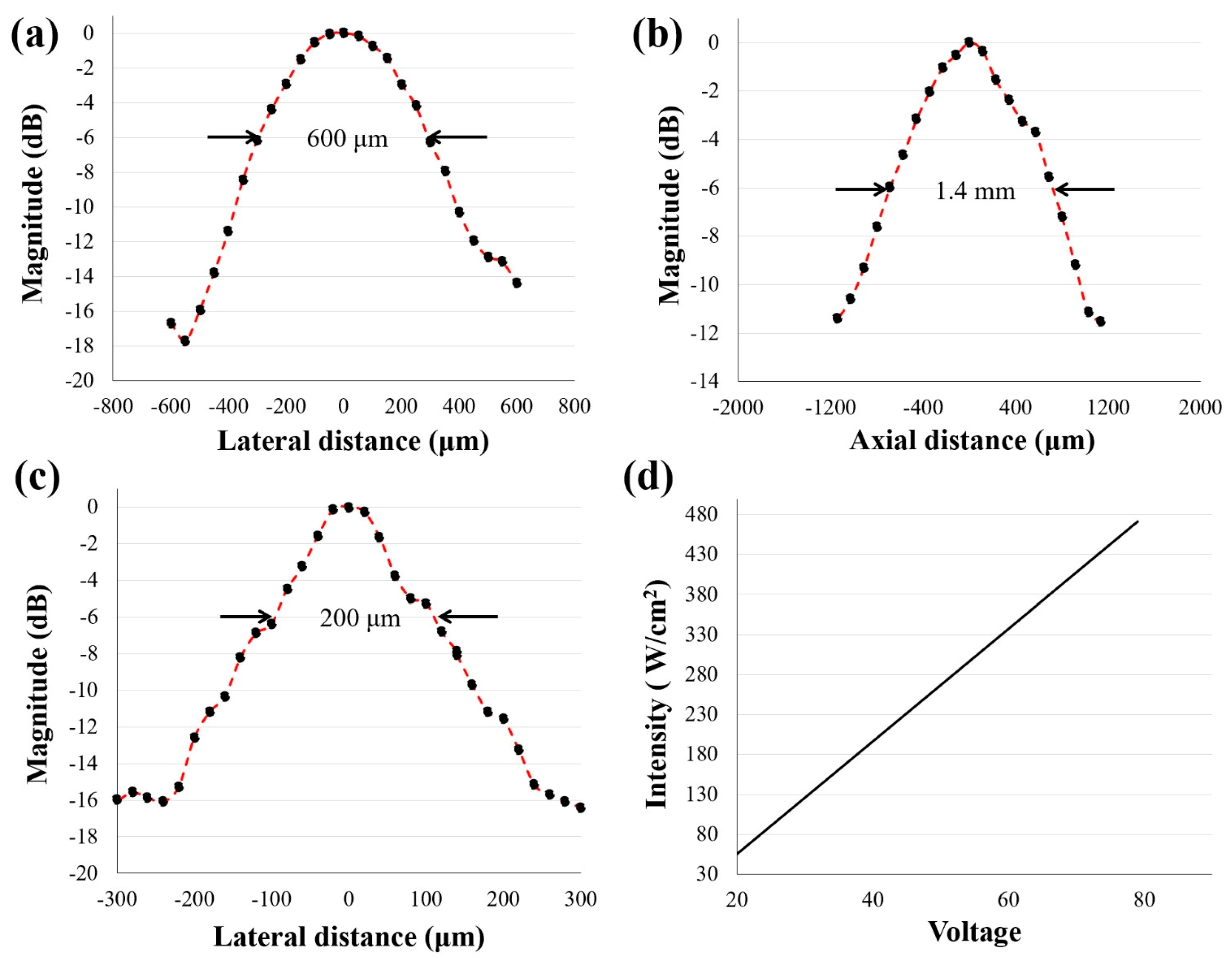
2.2. Transducer Performance Test
2.3. Transducer Performance Simulation
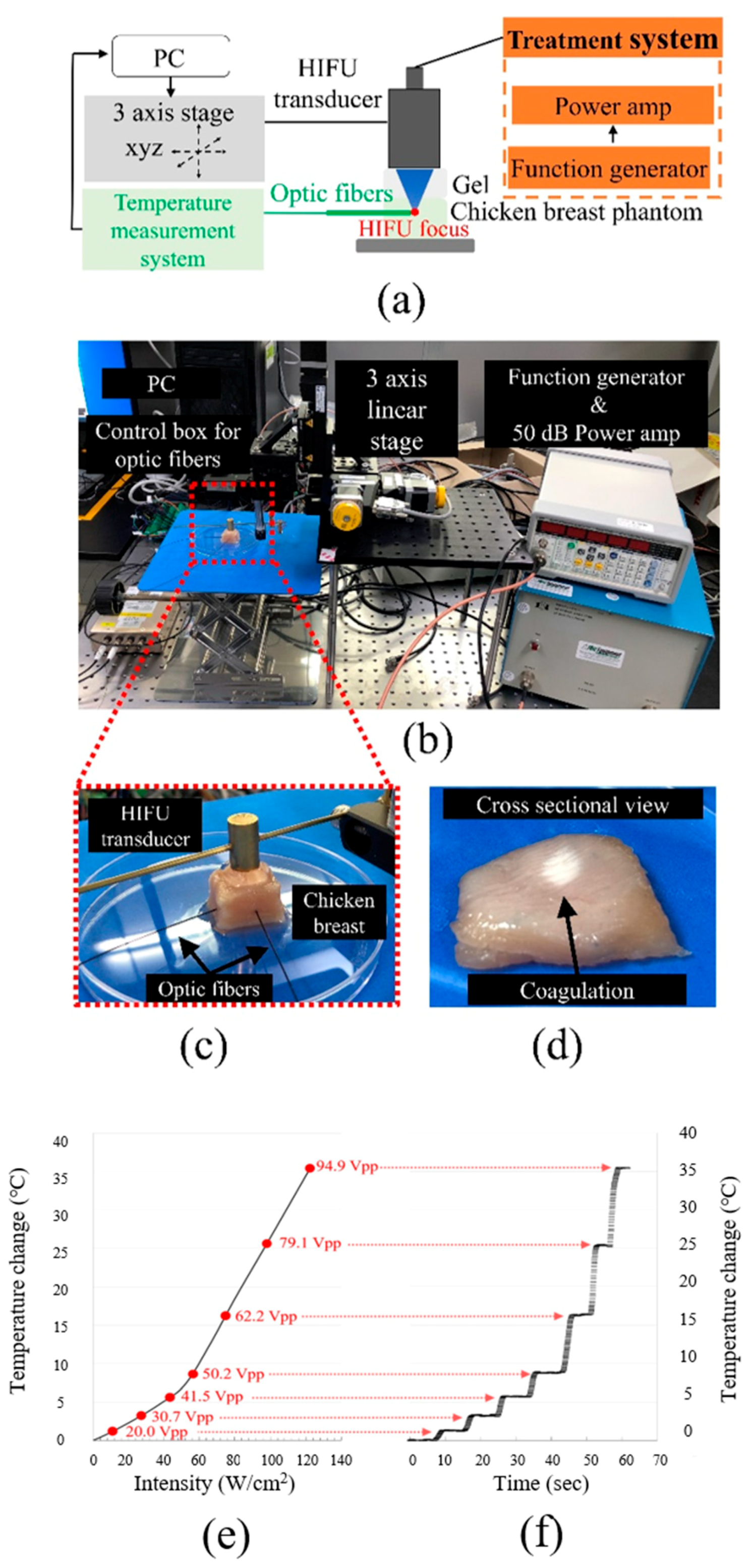
2.4. Ex Vivo Temperature Calibration
2.5. Phantom Imaging
2.6. In Vivo Experiment: Imaging and Treatment Using BTB Transducer
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
Patents
References
- Wu, F.; Wang, Z.B.; Chen, W.Z.; Wang, W.; Gui, Y.; Zhang, M.; Zheng, G.; Zhou, Y.; Xu, G.; Li, M.; et al. Extracorporeal high intensity focused ultrasound ablation in the treatment of 1038 patients with solid carcinomas in China: An overview. Ultrason. Sonochem. 2004, 11, 149–154. [Google Scholar] [CrossRef] [PubMed]
- Eisele, R.M.; Denecke, T.; Glanemann, M.; Chopra, S.S. Minimal-invasive microwave coagulation therapy for liver tumours: Laparoscopic and percutaneous access. Zentralbl. Chir. 2014, 139, 235–243. [Google Scholar] [CrossRef]
- Li, D.; Kang, J.; Golas, B.J.; Yeung, V.W.; Madoff, D.C. Minimally invasive local therapies for liver cancer. Cancer Biol. Med. 2014, 11, 217–236. [Google Scholar] [CrossRef] [PubMed]
- Rozenblum, N.; Zeira, E.; Scaiewicz, V.; Bulvik, B.; Gourevitch, S.; Yotvat, H.; Galun, E.; Goldberg, S.N. Oncogenesis: An “Off-Target” Effect of Radiofrequency Ablation. Radiology 2015, 276, 426–432. [Google Scholar] [CrossRef]
- Cavagnaro, M.; Amabile, C.; Bernardi, P.; Pisa, S.; Tosoratti, N. A minimally invasive antenna for microwave ablation therapies: Design, performances, and experimental assessment. IEEE Trans. Biomed. Eng. 2011, 58, 949–959. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.K.; Rhim, H.; Kim, Y.S.; Koh, B.H.; Cho, O.K.; Seo, H.S.; Kim, Y. Radiofrequency thermal ablation of hepatic tumors: Pitfalls and challenges. Abdom. Imaging 2005, 30, 727–733. [Google Scholar] [CrossRef]
- Hinshaw, J.L.; Littrup, P.J.; Durick, N.; Leung, W.; Lee, F.T., Jr.; Sampson, L.; Brace, C.L. Optimizing the protocol for pulmonary cryoablation: A comparison of a dual- and triple-freeze protocol. Cardiovasc. Interv. Radiol. 2010, 33, 1180–1185. [Google Scholar] [CrossRef] [Green Version]
- Choudhary, S.; Tang, J.; Elsaie, M.L.; Nouri, K. Lasers in the treatment of nonmelanoma skin cancer. Dermatol. Surg. 2011, 37, 409–425. [Google Scholar] [CrossRef] [PubMed]
- Sartori, S.; Di Vece, F.; Ermili, F.; Tombesi, P. Laser ablation of liver tumors: An ancillary technique, or an alternative to radiofrequency and microwave? World J. Radiol. 2017, 9, 91–96. [Google Scholar] [CrossRef] [PubMed]
- Pillai, K.; Akhter, J.; Chua, T.C.; Shehata, M.; Alzahrani, N.; Al-Alem, I.; Morris, D.L. Heat sink effect on tumor ablation characteristics as observed in monopolar radiofrequency, bipolar radiofrequency, and microwave, using ex vivo calf liver model. Medicine 2015, 94, e580. [Google Scholar] [CrossRef] [PubMed]
- Fabi, S.G. Noninvasive skin tightening: Focus on new ultrasound techniques. Clin. Cosmet. Investig. Dermatol. 2015, 8, 47–52. [Google Scholar] [CrossRef] [Green Version]
- Sanghvi, N. Non-invasive surgery using high intensity focused ultrasound (HIFU). Med. Phys. 2004, 31, 1805. [Google Scholar]
- Shaw, C.J.; Rivens, I.; Civale, J.; Botting, K.J.; Giussani, D.A.; ter Haar, G.; Lees, C.C. High Intensity Focused Ultrasound (HIFU): A method of non-invasive placental vascular occlusion. Bjog-Int. J. Obstet. Gy 2017, 124, 5. [Google Scholar]
- Ko, E.J.; Hong, J.Y.; Kwon, T.R.; Choi, E.J.; Jang, Y.J.; Choi, S.Y.; Yoo, K.H.; Kim, S.Y.; Kim, B.J. Efficacy and safety of non-invasive body tightening with high-intensity focused ultrasound (HIFU). Skin Res. Technol. 2017, 23, 558–562. [Google Scholar] [CrossRef]
- Guan, L.M.; Xu, G. Damage effect of high-intensity focused ultrasound on breast cancer tissues and their vascularities. World J. Surg. Oncol. 2016, 14, 1–17. [Google Scholar] [CrossRef] [Green Version]
- Kennedy, J.E.; Ter Haar, G.R.; Cranston, D. High intensity focused ultrasound: Surgery of the future? Br. J. Radiol. 2003, 76, 590–599. [Google Scholar] [CrossRef] [PubMed]
- Sung, H.H.; Jeong, B.C.; Seo, S.I.; Jeon, S.S.; Choi, H.Y.; Lee, H.M. Seven years of experience with high-intensity focused ultrasound for prostate cancer: Advantages and limitations. Prostate 2012, 72, 1399–1406. [Google Scholar] [CrossRef]
- He, P.; Shou, W.; Duan, S.; Xia, R. Dual-frequency High Intensity Focused Ultrasound (HIFU) Accelerating Therapy. In Proceedings of the 2005 IEEE Engineering in Medicine and Biology 27th Annual Conference, Shanghai, China, 17–18 January 2006; pp. 213–216. [Google Scholar] [CrossRef]
- Illing, R.O.; Kennedy, J.E.; Wu, F.; Ter Haar, G.R.; Protheroe, A.S.; Friend, P.J.; Gleeson, F.V.; Cranston, D.W.; Phillips, R.R.; Middleton, M.R. The safety and feasibility of extracorporeal high-intensity focused ultrasound (HIFU) for the treatment of liver and kidney tumours in a Western population. Br. J. Cancer 2005, 93, 890–895. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, S.; Wu, P.H. Magnetic resonance image-guided versus ultrasound-guided high-intensity focused ultrasound in the treatment of breast cancer. Chin. J. Cancer 2013, 32, 441–452. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.D.; Huang, C.H.; Yang, S.T.; Chu, Y.H.; Shieh, Y.Y.; Chen, J.W.; Lin, K.J. MRI/SPECT-based diagnosis and CT-guided high-intensity focused-ultrasound treatment system in MPTP mouse model of Parkinson’s disease. Med. Eng. Phys. 2013, 35, 222–230. [Google Scholar] [CrossRef] [PubMed]
- Owen, N.R.; Chapelon, J.Y.; Bouchoux, G.; Berriet, R.; Fleury, G.; Lafon, C. Dual-mode transducers for ultrasound imaging and thermal therapy. Ultrasonics 2010, 50, 216–220. [Google Scholar] [CrossRef]
- Hasebroock, K.M.; Serkova, N.J. Toxicity of MRI and CT contrast agents. Expert Opin. Drug Metab. Toxicol. 2009, 5, 403–416. [Google Scholar] [CrossRef]
- Ansari, T.; Yousef, A.; El Gamassy, A.; Fayez, M. Ultrasound-guided spinal anaesthesia in obstetrics: Is there an advantage over the landmark technique in patients with easily palpable spines? Int. J. Obstet. Anesth. 2014, 23, 213–216. [Google Scholar] [CrossRef] [PubMed]
- Chan, V.W.S.; Perlas, A.; Rawson, R.; Odukoya, O. Ultrasound-guided supraclavicular brachial plexus block. Anesth. Analg. 2003, 97, 1514–1517. [Google Scholar] [CrossRef] [PubMed]
- Brenner, K.; Ergun, A.S.; Firouzi, K.; Rasmussen, M.F.; Stedman, Q.; Khuri-Yakub, B.P. Advances in Capacitive Micromachined Ultrasonic Transducers. Micromachines 2019, 10, 152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanghvi, N.T.; Chen, W.H.; Carlson, R.; Weis, C.; Seip, R.; Uchida, T.; Marberger, M. Clinical validation of real-time tissue change monitoring during prostate tissue ablation with high intensity focused ultrasound. J. Ther. Ultrasound 2017, 5, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pak, C.S.; Lee, Y.K.; Jeong, J.H.; Kim, J.H.; Seo, J.D.; Heo, C.Y. Safety and efficacy of ulthera in the rejuvenation of aging lower eyelids: A pivotal clinical trial. Aesthet. Plast Surg. 2014, 38, 861–868. [Google Scholar] [CrossRef]
- Qi, W.J.; Li, R.; Ma, T.; Shung, K.K.; Zhou, Q.F.; Chen, Z.P. Confocal acoustic radiation force optical coherence elastography using a ring ultrasonic transducer. Appl. Phys. Lett. 2014, 104, 123702. [Google Scholar] [CrossRef] [Green Version]
- Shin, E.J.; Kang, B.; Chang, J.H. Real-Time HIFU Treatment Monitoring Using Pulse Inversion Ultrasonic Imaging. Appl. Sci. 2018, 8, 2219. [Google Scholar] [CrossRef] [Green Version]
- Mlosek, R.K.; Malinowska, S.; Sikora, M.; Debowska, R.; Stepien, A.; Czekaj, K.; Dabrowska, A. The use of high frequency ultrasound imaging in skin moisturization measurement. Skin Res. Technol. 2013, 19, 169–175. [Google Scholar] [CrossRef]
- Schuetzenberger, K.; Pfister, M.; Messner, A.; Froehlich, V.; Garhoefer, G.; Hohenadl, C.; Schmetterer, L.; Werkmeister, R.M. Comparison of optical coherence tomography and high frequency ultrasound imaging in mice for the assessment of skin morphology and intradermal volumes. Sci. Rep. 2019, 9, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Saijo, Y.; Kobayashi, K.; Okada, N.; Hozumi, N.; Hagiwara, Y.; Tanaka, A.; Iwamoto, T. High Frequency Ultrasound Imaging of Surface and Subsurface Structures of Fingerprints. In Proceedings of the 2008 30th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Vancouver, BC, Canada, 20–25 August 2008. [Google Scholar] [CrossRef]
- Lim, H.G.; Li, Y.; Lin, M.Y.; Yoon, C.; Lee, C.; Jung, H.; Chow, R.H.; Shung, K.K. Calibration of Trapping Force on Cell-Size Objects from Ultrahigh-Frequency Single-Beam Acoustic Tweezer. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2016, 63, 1988–1995. [Google Scholar] [CrossRef] [PubMed]
- Lim, H.G.; Shung, K.K. Quantification of Inter-Erythrocyte Forces with Ultra-High Frequency (410 MHz) Single Beam Acoustic Tweezer. Ann. Biomed. Eng. 2017, 45, 2174–2183. [Google Scholar] [CrossRef] [PubMed]
- Lim, H.G.; Kim, H.H.; Yoon, C. Evaluation method for acoustic trapping performance by tracking motion of trapped microparticle. Jpn. J. Appl. Phys. 2018, 57, 057202. [Google Scholar] [CrossRef]
- Lim, H.G.; Liu, H.C.; Yoon, C.W.; Jung, H.; Kim, M.G.; Yoon, C.; Kim, H.H.; Shung, K.K. Investigation of cell mechanics using single-beam acoustic tweezers as a versatile tool for the diagnosis and treatment of highly invasive breast cancer cell lines: An in vitro study. Microsyst. Nanoeng. 2020, 6, 1–12. [Google Scholar] [CrossRef]
- Lim, H.G.; Lee, O.J.; Shung, K.K.; Kim, J.T.; Kim, H.H. Classification of Breast Cancer Cells Using the Integration of High-Frequency Single-Beam Acoustic Tweezers and Convolutional Neural Networks. Cancers 2020, 12, 1212. [Google Scholar] [CrossRef]
- Soneson, J.E. A User-Friendly Software Package for HIFU Simulation. In Proceedings of the 8th International Symposium on Therapeutic Ultrasound, Aix-en-Provence, France, 23–26 September 2009; Volume 1113, pp. 165–169. [Google Scholar]
- Soneson, J.E. Extending the Utility of the Parabolic Approximation in Medical Ultrasound Using Wide-Angle Diffraction Modeling. IEEE Trans. Ultrason. Ferroelectr. Freq. Control. 2017, 64, 679–687. [Google Scholar] [CrossRef]
- Wang, Z.; Bai, J.; Li, F.; Du, Y.; Wen, S.; Hu, K.; Xu, G.; Ma, P.; Yin, N.; Chen, W.; et al. Study of a "biological focal region" of high-intensity focused ultrasound. Ultrasound Med. Biol. 2003, 29, 749–754. [Google Scholar] [CrossRef]
- Gill, I.S.; Hsu, T.H.; Fox, R.L.; Matamoros, A.; Miller, C.D.; Leveen, R.F.; Grune, M.T.; Sung, G.T.; Fidler, M.E. Laparoscopic and percutaneous radiofrequency ablation of the kidney: Acute and chronic porcine study. Urology 2000, 56, 197–200. [Google Scholar] [CrossRef]
- Corwin, T.S.; Lindberg, G.; Traxer, O.; Gettman, M.T.; Smith, T.G.; Pearle, M.S.; Cadeddu, J.A. Laparoscopic radiofrequency thermal ablation of renal tissue with and without hilar occlusion. J. Urol. 2001, 166, 281–284. [Google Scholar] [CrossRef]
- Nakada, S.Y.; Jerde, T.J.; Warner, T.F.; Lee, F.T., Jr. Comparison of radiofrequency ablation, cryoablation, and nephrectomy in treating implanted VX-2 carcinoma in rabbit kidneys. J. Endourol. 2004, 18, 501–506. [Google Scholar] [CrossRef]
- Kornstein, A.N. Ulthera for silicone lip correction. Plast Reconstr. Surg. 2012, 129, 1014e–1015e. [Google Scholar] [CrossRef] [PubMed]
- Friedmann, D.P.; Fabi, S.G.; Goldman, M.P. Combination of intense pulsed light, Sculptra, and Ultherapy for treatment of the aging face. J. Cosmet. Dermatol. 2014, 13, 109–118. [Google Scholar] [CrossRef] [PubMed]
- Ma, T.; Yu, M.; Li, J.; Munding, C.E.; Chen, Z.; Fei, C.; Shung, K.K.; Zhou, Q. Multi-frequency intravascular ultrasound (IVUS) imaging. IEEE Trans. Ultrason. Ferroelectr. Freq. Control. 2015, 62, 97–107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Munding, C.E.; Cherin, E.; Jourard, I.; Weyers, J.J.; Goertz, D.E.; Courtney, B.K.; Foster, F.S. Development of a 3 French Dual-Frequency Intravascular Ultrasound Catheter. Ultrasound Med. Biol. 2018, 44, 251–266. [Google Scholar] [CrossRef]
- Bove, T.; Zawada, T.; Serup, J.; Jessen, A.; Poli, M. High-frequency (20-MHz) high-intensity focused ultrasound (HIFU) system for dermal intervention: Preclinical evaluation in skin equivalents. Skin Res. Technol. 2019, 25, 217–228. [Google Scholar] [CrossRef]
- Xing, Y.; Lu, X.; Pua, E.C.; Zhong, P. The effect of high intensity focused ultrasound treatment on metastases in a murine melanoma model. Biochem. Biophys. Res. Commun. 2008, 375, 645–650. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, R.S.; Liu, L.X.; Gu, Y.H.; Lin, Q.F.; Guo, R.H.; Shu, Y.Q. The effect of endostatin and gemcitabine combined with HIFU on the animal xenograft model of human pancreatic cancer. Biomed. Pharmacother. 2010, 64, 309–312. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Layer | Water | Soft Tissue |
|---|---|---|
| Sound speed () | 1482 | 1629 |
| Mass density () | 1000 | 1000 |
| Attenuation at 1 MHz () | 0.217 | 58 |
| Fraction due to absorption | 0.0 | 0.9 |
| Exponent of attenuation power law | 2.0 | 1.0 |
| Nonlinear parameter | 3.5 | 4.5 |
| Heat capacity (J/kg/K) | 4180 | 4180 |
| Thermal conductivity (W/m/K) | 0.6 | 0.6 |
| Perfusion rate /s) | 0.0 | 20 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lim, H.G.; Kim, H.; Kim, K.; Park, J.; Kim, Y.; Yoo, J.; Heo, D.; Baik, J.; Park, S.-M.; Kim, H.H. Thermal Ablation and High-Resolution Imaging Using a Back-to-Back (BTB) Dual-Mode Ultrasonic Transducer: In Vivo Results. Sensors 2021, 21, 1580. https://doi.org/10.3390/s21051580
Lim HG, Kim H, Kim K, Park J, Kim Y, Yoo J, Heo D, Baik J, Park S-M, Kim HH. Thermal Ablation and High-Resolution Imaging Using a Back-to-Back (BTB) Dual-Mode Ultrasonic Transducer: In Vivo Results. Sensors. 2021; 21(5):1580. https://doi.org/10.3390/s21051580
Chicago/Turabian StyleLim, Hae Gyun, Hyunhee Kim, Kyungmin Kim, Jeongwoo Park, Yeonggeun Kim, Jinhee Yoo, Dasom Heo, Jinhwan Baik, Sung-Min Park, and Hyung Ham Kim. 2021. "Thermal Ablation and High-Resolution Imaging Using a Back-to-Back (BTB) Dual-Mode Ultrasonic Transducer: In Vivo Results" Sensors 21, no. 5: 1580. https://doi.org/10.3390/s21051580