1. Introduction
Total knee arthroplasty (TKA) is a common orthopedic procedure, representing 1.5 million procedures per year in countries part of the organization for economic cooperation and development alone, and expected to further increase by 2030 [
1]. However, TKA still fails in 2–8% of the cases [
2,
3] and 35% of these failures has been attributed to ligament imbalance, which is associated with excessive stiffness or instability of the knee joint [
4]. Nonetheless, current ligament balancing procedures applied during TKA primarily rely on indirect assessments of ligament strains, e.g., bony distances or intra-articular distances, and/or subjective intra-operative opinions of the surgeon [
5,
6,
7]. The two main ligaments targeted by such ligament balancing procedures are the medial collateral ligament (MCL) and lateral collateral ligament (LCL) because they are the primary frontal-plane knee stabilizers post-TKA [
8,
9]. Therefore, direct assessment of functionally relevant in-situ biomechanical properties, e.g., ligament tension and strain in response to a given varus or valgus stress, could be of great value. Indeed, these properties could provide surgeons with currently unavailable objective data to further improve both the pre-operative surgical planning and intra-operative ligament balancing procedures, thereby reducing the above TKA failures related to ligament imbalance. Additionally, robot-assisted TKA, which already displayed improved stability compared to conventional TKA [
10,
11], are currently primarily based on soft-tissue properties extracted from the scarce literature available. As a result, they could also benefit from subject-specific biomechanical properties to improve the accuracy of their underlying ligament balancing procedure [
12,
13].
Ultrasound (US) imaging is a common imaging modality to non-invasively assess dynamic biomechanical properties of soft-tissues such as tendons and ligaments in-situ. Indeed, dedicated ultrasound imaging methodologies, i.e., speckle tracking, have already been developed and successfully applied on large energy-storing tendons, e.g., patellar tendon and Achilles tendon [
14,
15,
16]. However, only a limited number of studies applied these techniques on knee collateral ligaments, primarily due to their inherently complex geometry and dynamic behavior during clinically relevant functional assessments of the knee joint [
17]. Additionally, currently available studies were either performed ex-situ on isolated ligaments [
18], hence preventing extrapolation to the above clinically relevant functional assessments, or were lacking ground-truth data to thoroughly validate the process [
17]. Recently, a study aiming to overcome these limitations was performed by our group [
19]. Herein, a US speckle tracking approach was developed to specifically measure in-situ collateral ligament strain, and was successfully validated through the acquisition of reference data using digital image correlation (DIC) during varus–valgus loading, indicating the potential of ultrasound-based ligament strain estimation to non-invasively assess collateral ligament behavior in the knee joint and improved ligament balancing in knee arthroplasty, for example through its integration in computer-based pre-operative planning. Nevertheless, partly due to the novelty of this research area, the impact of residual errors associated with this technique on the in-silico estimation of functionally-relevant knee arthroplasty outcomes have never been tested, thereby hindering the potential clinical applications of that study.
Therefore, this project investigated the sensitivity of model-based predictions of post-TKA tibiofemoral (TF) kinematics to residual errors in US-based collateral ligament strain estimations. In addition, the resulting sensitivity in terms of tibiofemoral kinematics was compared to the effect of the current clinical variability in terms of implant positioning on post-operative TF kinematics. We hypothesized that the sensitivity of model-based predictions associated with the existing US-based strain assessment of in-situ collateral ligaments would be less than the sensitivity to current surgical inaccuracies in terms of implant positioning.
4. Discussion
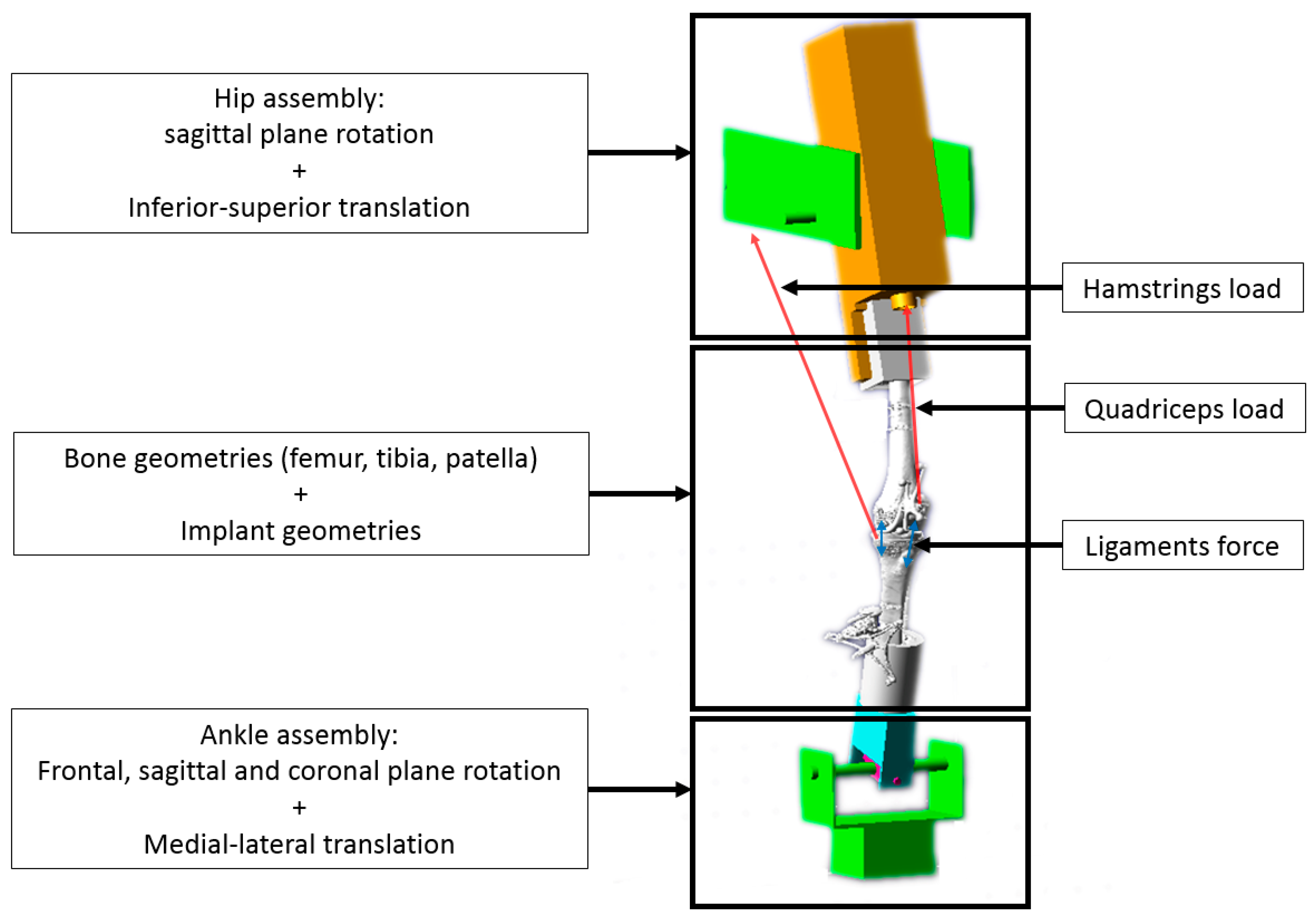
This study investigated the sensitivity of predicted kinematic behavior post-total knee arthroplasty to previously reported errors in US-based collateral ligament strain estimations. Thereto, a virtual simulator with an integrated knee joint model was created to simulate experimental squatting of two specimens and was validated by comparing simulated TF kinematics and muscle loads with experimental in-vitro results. These validated reference models were then used to compare the sensitivity of these models to previously reported errors in US-based collateral ligament strain estimations with their sensitivity to clinical accuracy in terms of implant positioning. The goal thereof was to assess whether the current accuracy of US-based collateral ligament strains suffices to inform computer-based pre-operative planning of TKA.
Our results showed that the knee simulator models can accurately predict tibiofemoral kinematics and loads with RMSE ranging from 0.4° to 3.8° for knee joint rotations and ranging from 0.5 mm to 2.62 mm for the translations (
Table 4). For both specimens, large differences were primarily observed in anterior–posterior translation, as previously reported in the literature [
29]. This is likely due to a lack of surrounding stabilizing structures in the model, such as the joint capsule, antero-lateral ligament or popliteus tendon. Nevertheless, the predicted TF kinematics displayed an overall excellent correlation and small RMSE, which compares well to prior studies using similar experimental set-ups and validation designs [
29,
36]. It should be noted that larger simulation errors were found with the model of specimen 2. This is probably due to the important post-TKA laxity that was observed during the ex-vivo experiments in this specimen, as displayed in
Table 1, likely associated with a poorly balanced and lax LCL during the whole range of motion. Indeed, in the squatting simulation, the LCL length was found to be continuously shorter than the initial length (
L0), leading to a ligament force equal to zero during the whole cycle. Because other posterolateral stabilizing structures such as the popliteofibular ligament and popliteus tendon, were not modeled, no soft-tissue structures were present to functionally contribute to the model’s lateral knee stability [
37]. As a result, the model of specimen 2 displayed excessive medial laxity compared to the experimental results. Besides TF kinematics, kinetics were also compared. For both specimens, ankle and quadriceps loads were close to experimental results with RMSE percentages of the experimentally obtained forces ranging from 20% to 50% for the ankle load and ranging from 8% to 28% for the quadriceps load. For similar reasons, slightly larger differences were again observed for specimen 2. Therefore, it can be concluded that both models reproducing realistic TF kinematics and loads and can be considered valid to perform the intended sensitivity analyses.
This sensitivity analysis of the models to residual errors in US-based collateral ligament strain estimation displayed an overall limited impact on TF kinematics. Indeed, for all TF kinematics except internal–external tibial rotation, the applied alterations in MCL and LCL stiffness led to absolute variations below 0.08° and 0.1 mm, in terms of rotations and translations respectively (
Table 6). The most important variations were indeed observed for the internal–external tibial rotation with values ranging from −0.61° to 0.73°. Considering the role of collateral ligaments as internal rotational stabilizers post-TKA [
8], such an impact on internal–external tibial rotation was to be expected. Nevertheless, an even higher impact was expected on varus–valgus and medial–lateral translations because the collateral ligaments are the primary frontal-plane knee stabilizers post-TKA [
8,
9]. Likely, the impact of the stiffness perturbations is to an extent mitigated by the post and cam successfully providing medio-lateral stability in the posterior-stabilized implant design used in this study [
38]. This interplay between the implant design and the soft-tissue structures in providing stability is assumed to also explain the overall smaller impact of MCL stiffness variations in specimen 2 (
Table 5). Here, the excessive laxity of the second specimen likely reduced the relative importance of the collateral ligaments within this interplay. Nevertheless, the combination of these two specimens uniquely illustrates the robustness of our model with US-based collateral ligament properties to clinically occurring variations in terms of ligament balancing.
Interestingly, our models displayed a larger sensitivity of predicted TF kinematics to the current clinical inaccuracies in terms of implant positioning, more precisely to variations in internal–external rotation of the tibial baseplate of ±3.2° [
34]. Once again, and as expected, the largest impact was observed on the internal–external tibial rotation with values ranging from −1.86° to 1.95°, i.e., a factor 3 times larger than the above sensitivity to errors in US-based collateral ligament strain estimation (
Table 6). Interestingly, the medial–lateral translation was also found to be up to ten times more sensitive to variations in implant positioning, with values ranging from −0.70 mm to 0.70 mm (
Table 6). For specimen 1, the sensitivity of varus–valgus rotation, anterior–posterior and inferior–superior translations were all very similar to the sensitivity to errors in US-based collateral ligament strain estimation. For specimen 2, increased sensitivity was also observed for varus–valgus and anterior–posterior translation. This observation further supports our hypothesis that, due to the high laxity and poor balancing of specimen 2, the implant design has a more important contribution to knee stability. By consequence, perturbations in terms of implant positioning have a greater impact on TF kinematics. Secondly, it should be noted that the above sensitivities vary throughout the flexion range. For specimen 1, the sensitivity to errors in US-based strain estimation of the LCL exceeded the sensitivity to variations in implant positioning at low flexion angles (<40° of knee flexion), as displayed in
Figure 3B. This can be explained by the decreasing importance of the LCL as a medio-lateral stabilizer with increasing flexion observed in our model, because the LCL strain was found to reduce in the model. Finally, the model of specimen 1 also indicated a relatively larger sensitivity to errors in US-based strain estimation of the LCL compared to the MCL. This is a direct result of the fact that the error in US-based LCL strain estimation was also higher than in the MCLs [
19]).
The main limitation of this study is the limited number of specimens. Nevertheless, this is similar to other modeling studies of the knee making use of in-vitro knee-joint simulators for validation purposes [
26,
29,
36,
39]. The second limitation is the pre-experimental conditions of both specimens used in the study. Indeed, as mentioned previously, the second specimen was poorly balanced, leading to an excessively lax specimen (
Table 1). Most importantly, the fact that the LCL was inactive during squat motion rendered perturbations in LCL stiffness to reflect the errors in US-based collateral ligament strain estimation a priori useless. Nevertheless, this model was still performing well and results were deemed satisfactory to perform further sensitivity analyses to variations in MCL stiffness and implant positioning. Furthermore, as already indicated above, the combination of these two specimens allowed us to analyze the robustness of US-informed models to clinically occurring variations in terms of ligament balancing. Indeed, our model nicely reflected how well-balanced post-TKA knees rely more on collateral ligaments to guarantee functional stability during squatting, whereas poorly balanced TKA’s rely more on the implant design to ensure this stability. A third limitation is related to the definition of soft tissue structures in our computational model. Only a limited number of soft-tissue structures were included, of which insertions points were based on an anatomical atlas and not defined on a subject-specific basis. Additionally, ligaments were modeled with a limited number of straight lines only, not taking into account any wrapping of soft-tissues around the bones. Nevertheless, this generally represents a worst-case scenario in terms of the model’s sensitivity to errors in US-based collateral ligament strain estimation, and further improvements in terms of soft-tissue modelling are expected to further reduce these sensitivities. Another limitation is the optimization process, which cannot guarantee a global optimum of parameters α and β (
Table 1), as well as stiffness parameters (
Table 2). Nevertheless, as it was not the main goal of this study to develop optimal models but rather to study the effect within a window of variations on these parameters, this not expected to influence any of the study findings. A last limitation of this study is that only variations in internal–external rotation of the tibial baseplate of one single, cruciate sacrificing implant design were assessed. However, it should also be noted here that we opted for a worst-case scenario because we expect that adding variations in other degrees of freedom of the implant position, as well as the addition of one or both cruciate ligaments in the post-TKA model with even larger reported variations in implant malpositioning [
40], would rather further increase the relative sensitivity of predicted knee kinematics to implant malpositioning in favor of our main hypothesis.






{kind=link}
{kind=link}
{kind=link}
{kind=link}