
Developing a Novel Prosthetic Hand with Wireless Wearable Sensor Technology Based on User Perspectives: A Pilot Study
 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Novel Hand Based on Users’ Perspectives
2.1.1. Users’ Perspectives
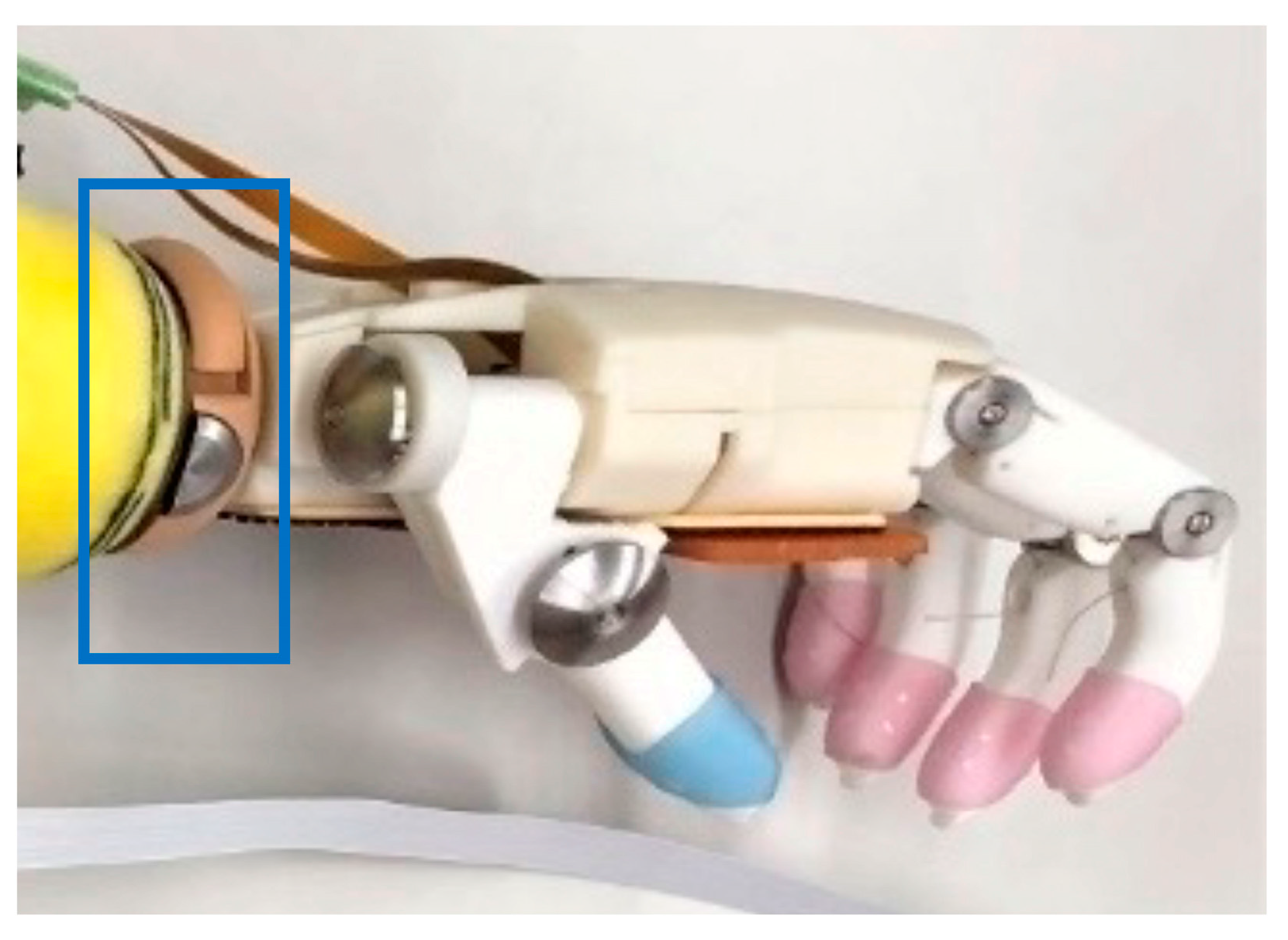
2.1.2. Prosthetic Hand Design
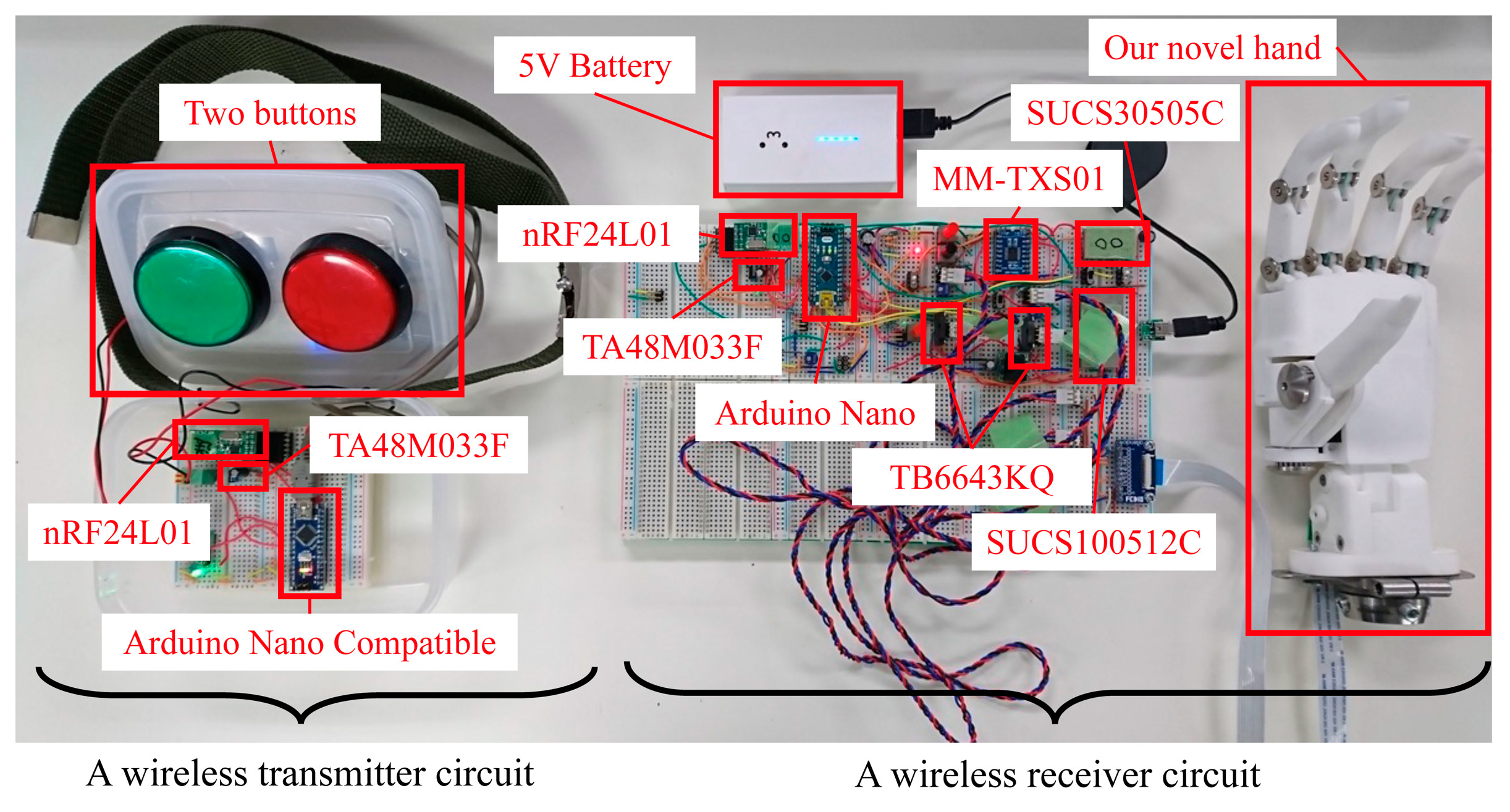
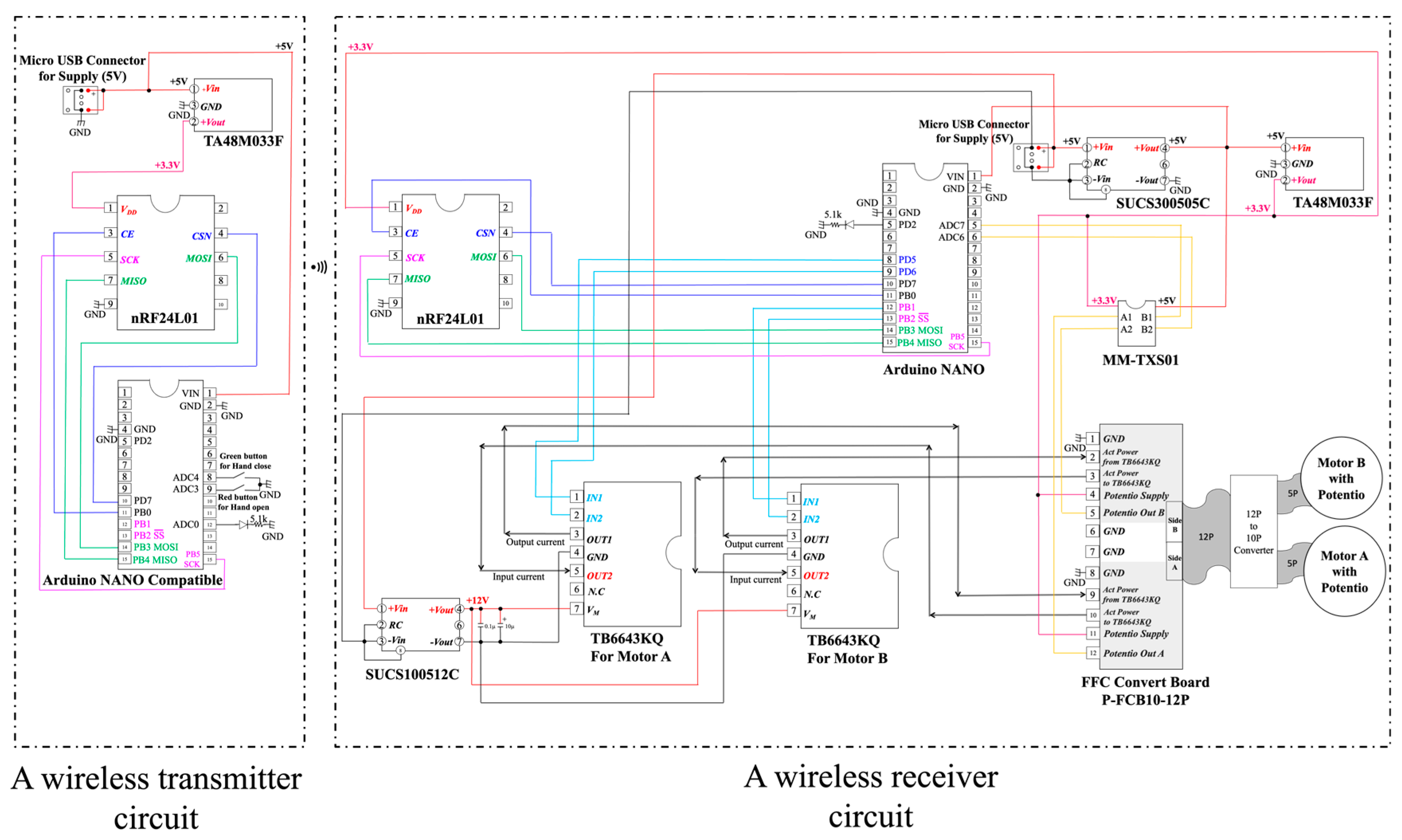
2.2. Wireless Button Sensor
2.3. Participants and Method
2.3.1. Participants
2.3.2. Materials
2.3.3. Clinical Evaluation
Upper-Limb Function
Fatigue While Using the Simulator Hand
2.3.4. Statistical Analysis
3. Results
3.1. ARAT
3.2. STEF
3.3. Modified Borg Scale
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Yamamoto, M.; Chung, K.C.; Sterbenz, J.; Shauver, M.J.; Tanaka, H.; Nakamura, T.; Oba, J.; Chin, T.; Hirata, H. Cross-sectional international multicenter study on quality of life and reasons for abandonment of upper limb prostheses. Plast. Reconstr. Surg. Glob. Open 2019, 7, e2205. [Google Scholar] [CrossRef] [PubMed]
- Biddiss, E.; Beaton, D.; Chau, T. Consumer design priorities for upper limb prosthetics. Disabil. Rehabil. Assist. Technol. 2007, 2, 346–357. [Google Scholar] [CrossRef] [PubMed]
- Østlie, K.; Lesjø, I.M.; Franklin, R.J.; Garfelt, B.; Skjeldal, O.H.; Magnus, P. Prosthesis rejection in acquired major upper-limb amputees: A population-based survey. Disabil. Rehabil. Assist. Technol. 2012, 7, 294–303. [Google Scholar] [CrossRef]
- Resnik, L.; Borgia, M. User ratings of prosthetic usability and satisfaction in VA study to optimize DEKA arm. J. Rehabil. Res. Dev. 2014, 51, 15–26. [Google Scholar] [CrossRef]
- Resnik, L.; Ekerholm, S.; Borgia, M.; Clark, M.A. A national study of veterans with major upper limb amputation: Survey methods, participants, and summary findings. PLoS ONE 2019, 14, e0213578. [Google Scholar] [CrossRef]
- Resnik, L.; Borgia, M.; Biester, S.; Clark, M.A. Longitudinal study of prosthesis use in veterans with upper limb amputation. Prosthet. Orthot. Int. 2021, 45, 26–35. [Google Scholar] [CrossRef]
- Biddiss, E.; McKeever, P.; Lindsay, S.; Chau, T. Implications of prosthesis funding structures on the use of prostheses: Experiences of individuals with upper limb absence. Prosthet. Orthot. Int. 2011, 35, 215–224. [Google Scholar] [CrossRef] [PubMed]
- Cordella, F.; Ciancio, A.L.; Sacchetti, R.; Davalli, A.; Cutti, A.G.; Guglielmelli, E.; Zollo, L. Literature review on needs of upper limb prosthesis users. Front. Neurosci. 2016, 10, 209. [Google Scholar] [CrossRef]
- O’Keeffe, B. Prosthetic rehabilitation of the upper limb amputee. Indian J. Plast. Surg. 2011, 44, 246–252. [Google Scholar] [CrossRef]
- Carey, S.L.; Lura, D.J.; Highsmith, M.J. Differences in myoelectric and body-powered upper-limb prostheses: Systematic literature review. J. Rehabil. Res. Dev. 2015, 52, 247–262. [Google Scholar] [CrossRef]
- Yabuki, Y.; Tanahashi, K.; Mouri, Y.; Murai, Y.; Togo, S.; Kato, R.; Jiang, Y.; Yokoi, H. Development of new cosmetic gloves for myoelectric prosthetic hand using superelastic rubber. Robot. Auton. Syst. 2019, 111, 31–43. [Google Scholar] [CrossRef]
- Yoshikawa, M.; Ogawa, K.; Yamanaka, S.; Kawashima, N. Finch: Prosthetic arm with three opposing fingers controlled by a muscle bulge. IEEE Trans. Neural. Syst. Rehabil. Eng. 2023, 31, 377–386. [Google Scholar] [CrossRef] [PubMed]
- Espinosa, M.; Nathan-Roberts, D. Understanding prosthetic abandonment. Proc. Human Factors Ergonomics Soc. Annu. Meet. 2019, 63, 1644–1648. [Google Scholar] [CrossRef]
- Baumann, M.F.; Frank, D.; Kulla, L.-C.; Stieglitz, T. Obstacles to prosthetic care—Legal and ethical aspects of access to upper and lower limb prosthetics in Germany and the improvement of prosthetic care from a social perspective. Societies 2020, 10, 10. [Google Scholar] [CrossRef]
- Webster, J.B.; Webster, N.; Borgia, M.; Resnik, L. Frequency, severity, and implications of shoulder pain in people with major upper limb amputation who use prostheses: Results of a national study. PM&R 2022, 14, 901–912. [Google Scholar] [CrossRef] [PubMed]
- Lyons, K.R.; Joshi, S.S.; Joshi, S.S.; Lyons, K.R. Upper limb prosthesis control for high-level amputees via myoelectric recognition of leg gestures. IEEE Trans. Neural. Syst. Rehabil. Eng. 2018, 26, 1056–1066. [Google Scholar] [CrossRef] [PubMed]
- Mori, T.; Tanaka, Y.; Yoshikawa, K.; Katane, D.; Torishima, H.; Shimizu, Y.; Hara, Y. Proposal of bioinstrumentation using shape deformation of the amputated upper limb. In Proceedings of the 2013 35th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Osaka, Japan, 3–7 July 2013; pp. 882–885. [Google Scholar] [CrossRef]
- Mori, T.; Tanaka, Y.; Mito, M.; Yoshikawa, K.; Katane, D.; Torishima, H.; Shimizu, Y.; Hara, Y. Proposal of bioinstrumentation using flex sensor for amputated upper limb. In Proceedings of the 2014 36th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Chicago, IL, USA, 26–30 August 2014; pp. 1218–1221. [Google Scholar] [CrossRef]
- Japan Platform for Patent Information (JP,6953007,B). Available online: https://www.j-platpat.inpit.go.jp/p0200 (accessed on 1 April 2024).
- Nordic. Semiconductor. nRF24LU1+ Single Chip 2.4-GHz Transceiver with USB Microcontroller and Flash Memory Product Specification v1.1. Available online: https://infocenter.nordicsemi.com/pdf/nRF24LU1P_PS_v1.1.pdf (accessed on 1 April 2024).
- Actuonix Motion Devices, PQ12-100-12-P Linear Actuator. Available online: https://www.actuonix.com/pq12-100-12-p (accessed on 10 April 2024).
- Platz, T.; Pinkowski, C.; van Wijck, F.; Kim, I.H.; di Bella, P.; Johnson, G. Reliability and validity of arm function assessment with standardized guidelines for the Fugl-Meyer Test, Action Research Arm Test and Box and Block Test: A multicentre study. Clin. Rehabil. 2005, 19, 404–411. [Google Scholar] [CrossRef] [PubMed]
- Kita, K.; Otaka, Y.; Takeda, K.; Sakata, S.; Ushiba, J.; Kondo, K.; Liu, M.; Osu, R. A pilot study of sensory feedback by transcutaneous electrical nerve stimulation to improve manipulation deficit caused by severe sensory loss after stroke. J. Neuroeng. Rehabil. 2013, 10, 55. [Google Scholar] [CrossRef] [PubMed]
- Carpinella, I.; Cattaneo, D.; Ferrarin, M. Quantitative assessment of upper limb motor function in Multiple Sclerosis using an instrumented Action Research Arm Test. J. Neuroeng. Rehabil. 2014, 11, 67. [Google Scholar] [CrossRef]
- Lee, J.H.; Park, J.H.; Kim, Y.J. Sensitivity of the accelerometer as a measurement tool for upper extremity movement by stroke patients: A comparison with the action research arm test. J. Phys. Ther. Sci. 2015, 27, 1053–1054. [Google Scholar] [CrossRef]
- Borg, G.A. Psychophysical bases of perceived exertion. Med. Sci. Sports Exerc. 1982, 14, 377–381. [Google Scholar] [CrossRef] [PubMed]
- Muza, S.R.; Silverman, M.T.; Gilmore, G.C.; Hellerstein, H.K.; Kelsen, S.G. Comparison of scales used to quantitate the sense of effort to breathe in patients with chronic obstructive pulmonary disease. Am. Rev. Respir. Dis. 1990, 141 Pt 1, 909–913. [Google Scholar] [CrossRef] [PubMed]
- Bouwsema, H.; van der Sluis, C.K.; Bongers, R.M. Learning to control opening and closing a myoelectric hand. Arch. Phys. Med. Rehabil. 2010, 91, 1442–1446. [Google Scholar] [CrossRef] [PubMed]
- Bouwsema, H.; Kyberd, P.J.; Hill, W.; van der Sluis, C.K.; Bongers, R.M. Determining skill level in myoelectric prosthesis use with multiple outcome measures. J. Rehabil. Res. Dev. 2012, 49, 1331–1348. [Google Scholar] [CrossRef] [PubMed]
- Huinink, L.H.; Bouwsema, H.; Plettenburg, D.H.; van der Sluis, C.K.; Bongers, R.M. Learning to use a body-powered prosthesis: Changes in functionality and kinematics. J. Neuroeng. Rehabil. 2016, 13, 90. [Google Scholar] [CrossRef] [PubMed]
- Stavdahl, Ø.; Mugaas, T.; Ottermo, M.V.; Magne, T.; Kyberd, P. Mechanisms of sporadic control failure related to the skin-electrode interface in myoelectric hand prostheses. J. Prosthet. Orthot. 2020, 32, 38–51. [Google Scholar] [CrossRef]
- Available online: https://www.ottobock.com/en-us/product/8E500 (accessed on 28 January 2024).
- Jones, H.; Dupan, S.; Dyson, M.; Krasoulis, A.; Kenney, L.P.J.; Donovan-Hall, M.; Memarzadeh, K.; Day, S.; Coutinho, M.; Nazarpour, K. Co-creation and user perspectives for upper limb prosthetics. Front. Neurorobot. 2012, 15, 689717. [Google Scholar] [CrossRef]
- Ossur. i-Limb® Quantum Bionic Hand. Available online: https://www.ossur.com/en-us/prosthetics/arms/i-limb-quantum (accessed on 28 January 2024).
- Ku, I.; Lee, G.K.; Park, C.Y.; Lee, J.; Jeong, E. Clinical outcomes of a low-cost single-channel myoelectric-interface three-dimensional hand prosthesis. Arch. Plast. Surg. 2019, 46, 303–310. [Google Scholar] [CrossRef]
- Kyberd, P.J. The influence of passive wrist joints on the functionality of prosthetic hands. Prosthet. Orthot. Int. 2012, 36, 33–38. [Google Scholar] [CrossRef]
- Wright, V. Prosthetic Outcome measures for use with upper limb amputees: A systematic review of the peer-reviewed literature, 1970 to 2009. J. Prosthet. Orthot. 2009, 21, 3–63. [Google Scholar] [CrossRef]
- Kyberd, P.J. The influence of control format and hand design in single axis myoelectric hands: Assessment of functionality of prosthetic hands using the Southampton hand assessment procedure. Prosthet. Orthot. Int. 2011, 35, 285–293. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| User | 1 | 2 | 3 | 4 | 5 |
|---|---|---|---|---|---|
| Age group | 40s | 20s | 30s | 30s | 40s |
| Level | Humerus | Forearm | Forearm | Forearm | Humerus |
| Right/left | Right | Left | Right | Left | Left |
| Necessity | Yes | Yes | Yes | Yes | Yes |
| Hesitation in using a prosthesis | No | No | No | No | No |
| Type of prosthesis | Body-powered, | Body-powered, | Body-powered, | Body-powered, | Body-powered, |
| cosmetic, myoelectric | cosmetic, hooked | cosmetic, myoelectric | cosmetic, myoelectric | cosmetic, hooked | |
| Myoelectric hand problem | Malfunction, | Increased weight, cost | Cost | Cost | Malfunction, |
| increased weight, cost | increased weight, cost | ||||
| Objectives | Daily life, | Daily life, | Daily life, | Daily life, | Daily life, |
| light work, office work | carrying heavy loads | light work, Calligraphy | light work, office work | light work | |
| Priority | 1. Appearance | 1. Function | 1. Function | 1. Function | 1. Function |
| 2. Function | 2. Appearance | 2. Weight | 1. Appearance | 1. Appearance | |
| 3. Cost | 3. Cost | 3. Appearance | 3.Weight | 3. Cost | |
| Priority in hand function | 1. Wrist angle adjustment | 1. Wrist angle adjustment | 1. Wrist angle adjustment | 1. Grip | 1. Wrist angle adjustment |
| 2. Grip | 2. Grip | 2.Pinch | 2. Wrist angle adjustment | 2. Grip | |
| 3. Pinch | 3. Pinch | 3. Grip | 3. Pinch | 3. Pinch | |
| Grasp | Grip | Pinch | Gross motor | Total | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| OH | NW | OH | NW | OH | NW | OH | NW | OH | NW | |
| Median | 15 | 15 | 12 | 12 | 6 | 3 | 9 | 9 | 71 | 66 |
| IQR | 14.5–15 | 14–15 | 11–12 | 12 | 4–6 | 3 | 9 | 9 | 67–75 | 63–66 |
| p = 1.00 | p = 0.75 | ※ p = 0.0039 | p = 1.00 | p = 0.29 | ||||||
| 1 | 2 | 3 | 4 | 5 | ||||||
| Five large balls | Six middle-sized balls | Five large | Six middle-sized cubes | Six wooden | ||||||
| cuboids | circular disks | |||||||||
| OH | NW | OH | NW | OH | NW | OH | NW | OH | NW | |
| Median | 1 | 1 | 1 | 2 | 0 | 0.5 | 0 | 0 | 0 | 0.5 |
| IQR | 0.75 –3.5 | 0.75–1.0 | 0–2 | 0–2.25 | 0–1 | 0–1 | 0–0.25 | 0–1 | 0 | 0–2 |
| p = 0.13 | p = 0.57 | p = 0.53 | p = 0.81 | p = 0.063 | ||||||
| 6 | 7 | 8, 9, 10 | Total | |||||||
| Six small cubes | Six pieces of clothes | Seven metallic circular disks, | ||||||||
| Six small balls, eight pins | ||||||||||
| OH | NW | OH | NW | OH | NW | OH | NW | |||
| Median | 0 | 0 | 0 | 0.3 | 0 | 0 | 3 | 5 | ||
| IQR | 0 | 0–1.25 | 0.1 | 0–1 | 0 | 0 | 1.5–6.25 | 1–8.5 | ||
| p = 0.13 | p = 0.50 | p = 1.00 | p = 1.00 | p = 0.26 | ||||||
| ARAT | STEF | Change of Borg Scale | ||||
|---|---|---|---|---|---|---|
| OH | NW | OH | NW | OH | NW | |
| Median | 71 | 66 | 3 | 5 | 1 | 1 |
| IQR | 67–75 | 63–66 | 1.5–6.25 | 1–8.5 | 1–1.375 | 0–2.125 |
| p = 0.29 | p = 0.26 | ※ p = 0.045 | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shimizu, Y.; Mori, T.; Yoshikawa, K.; Katane, D.; Torishima, H.; Hara, Y.; Yozu, A.; Yamazaki, M.; Hada, Y.; Mutsuzaki, H. Developing a Novel Prosthetic Hand with Wireless Wearable Sensor Technology Based on User Perspectives: A Pilot Study. Sensors 2024, 24, 2765. https://doi.org/10.3390/s24092765
Shimizu Y, Mori T, Yoshikawa K, Katane D, Torishima H, Hara Y, Yozu A, Yamazaki M, Hada Y, Mutsuzaki H. Developing a Novel Prosthetic Hand with Wireless Wearable Sensor Technology Based on User Perspectives: A Pilot Study. Sensors. 2024; 24(9):2765. https://doi.org/10.3390/s24092765
Chicago/Turabian StyleShimizu, Yukiyo, Takahiko Mori, Kenichi Yoshikawa, Daisuke Katane, Hiroyuki Torishima, Yuki Hara, Arito Yozu, Masashi Yamazaki, Yasushi Hada, and Hirotaka Mutsuzaki. 2024. "Developing a Novel Prosthetic Hand with Wireless Wearable Sensor Technology Based on User Perspectives: A Pilot Study" Sensors 24, no. 9: 2765. https://doi.org/10.3390/s24092765