Domestic Water Service Delivery Indicators and Frameworks for Monitoring, Evaluation, Policy and Planning: A Review



Abstract
:1. Introduction
2. Frameworks for Monitoring Water Services: A History
2.1. Measuring and Ranking Water Services along Indicators (1991 and 1996)

2.2. Water Service Levels Introduced (2003)

| Service level | Access | Needs met | Level of health concern |
|---|---|---|---|
| No access (quantity collected often below 5 L/c/d) | More than 1,000 m or 30 min total collection time | Consumption—cannot be assured Hygiene—not possible (unless practiced at source) | Very high |
| Basic access (average quantity unlikely to exceed 20 L/c/d) | Between 100 and 1,000 m or 5 to 30 min total collection time | Consumption—should be assured Hygiene—hand washing and basic food hygiene possible; laundry/bathing difficult to assure unless carried out at source | High |
| Intermediate access (average quantity about 50 L/c/d) | Water delivered through one tap on plot (or within 100 m or 5 min total collection time | Consumption—assured Hygiene—all basic personal and food hygiene assured; laundry and bathing should also be assured | Low |
| Optimal access (average quantity 100 L/c/d and above) | Water supplied through multiple taps continuously | Consumption—all needs met Hygiene—all needs should be met | Very low |
2.3. A Human Rights Framework for Water (2003, 2010)
| Indicator | Definition |
|---|---|
| Availability | The water supply for each person must be sufficient and continuous for personal and domestic uses. These uses ordinarily include drinking, personal sanitation, washing of clothes, food preparation, personal and household hygiene. According to the WHO, between 50 and 100 L of water per person per day are needed to ensure basic needs are met and few health concerns arise [29]. |
| Quality | The water required for personal or domestic use must be safe, therefore free from micro-organisms, chemical substances and radiological hazards that constitute a threat to a person’s health. Measures of drinking-water safety are usually defined by national and/or local standards for drinking-water quality. The World Health Organization (WHO) Guidelines for Drinking-water Quality provide a basis for the development of national standards. |
| Accessibility | Water facilities must be accessible to everyone without discrimination. Accessibility has overlapping dimensions: physical, economic, and information. Sufficient and safe water must be accessible within the vicinity of the household and affordable. According to WHO, the water source has to be within 1,000 m of the home and collection time should not exceed 30 min. The United Nations Development Programme (UNDP) suggests that water costs should not exceed 3 per cent of household income. Accessibility includes the right to seek, receive and impart information concerning water issues. |
| Non-discrimination and equality | It is the obligation of States to guarantee that the right to water is enjoyed without discrimination and equally between men and women and proscribes any discrimination which has the effect of nullifying or impairing the equal enjoyment or exercise of the right to water. |
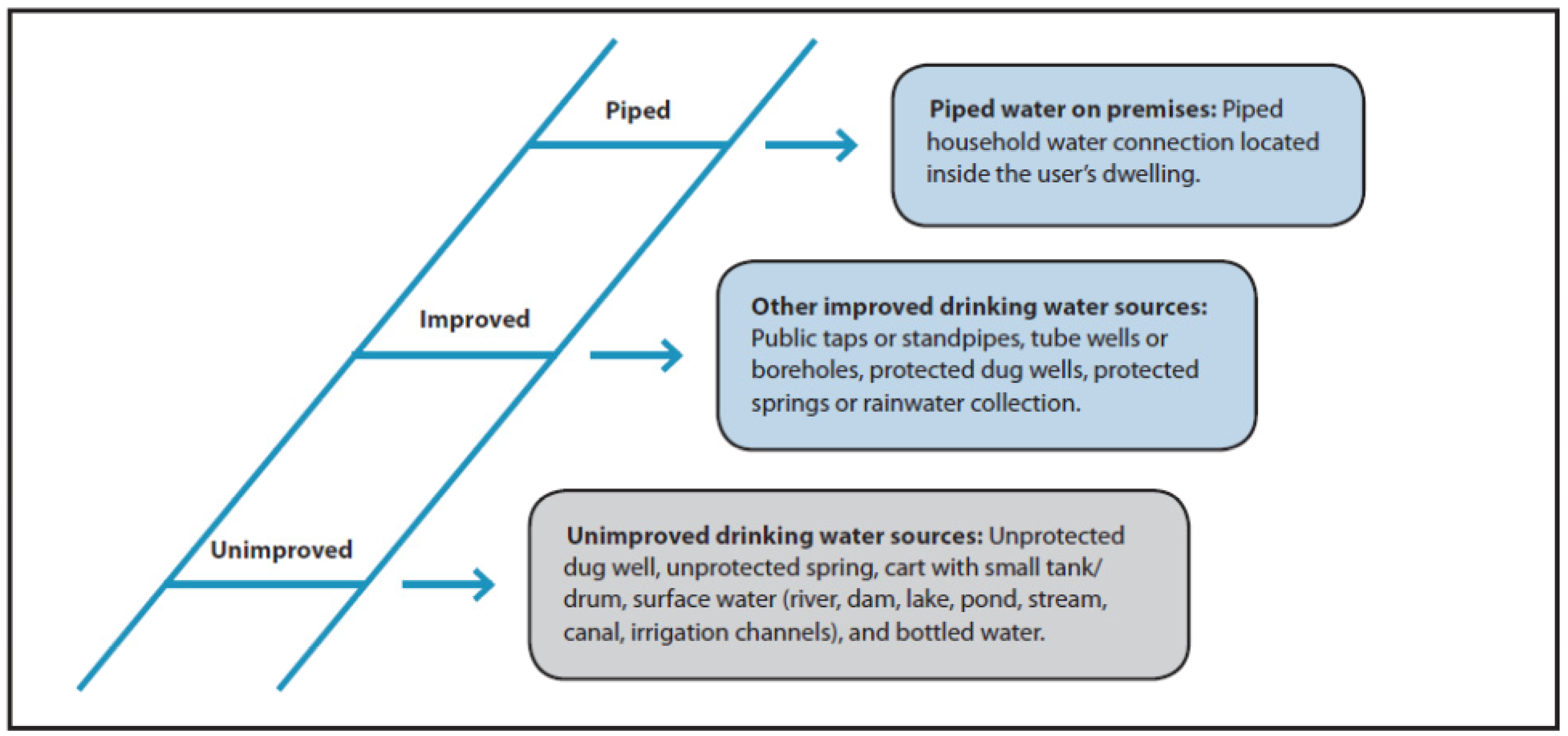
2.4. The WHO-UNICEF Framework (2008 et seq.)

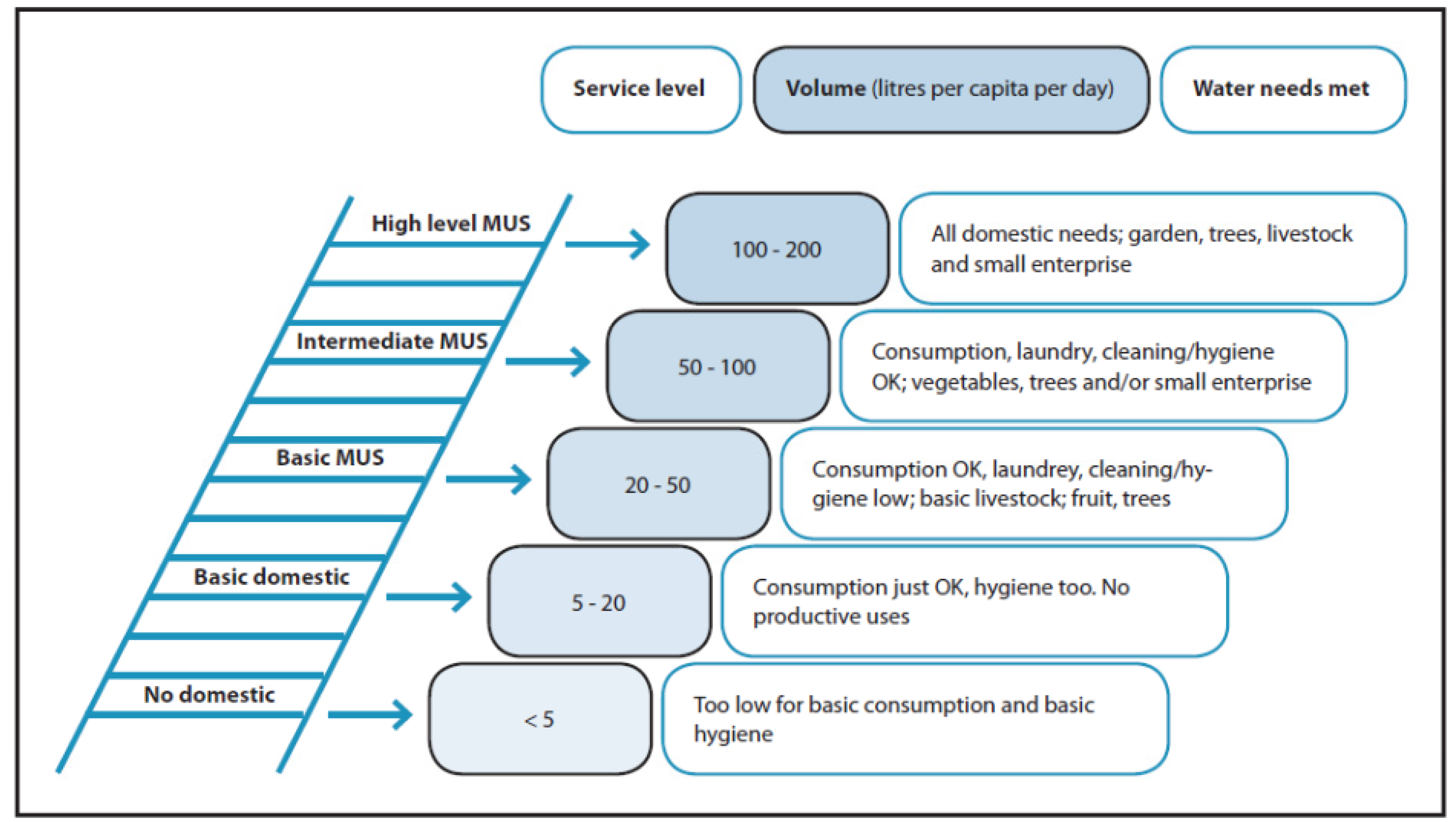
2.5. A Framework for Multiple Use Services (2007 and 2009)

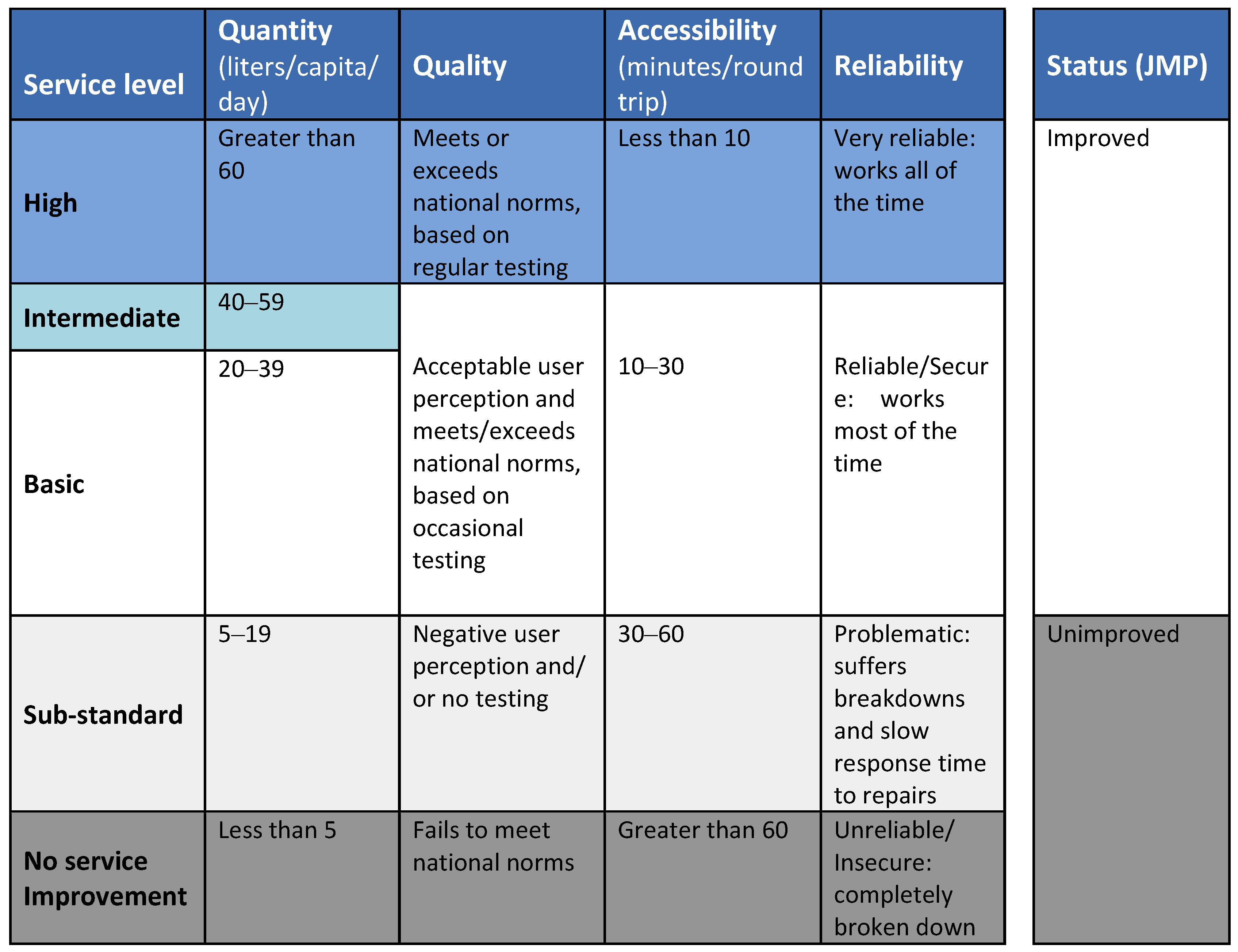
2.6. Water Service Ladders (2008 and 2009)

{kind=link}
{kind=link}
{kind=link}
{kind=link}
3. Water Service Indicators
3.1. Service Type (Infrastructure Classification)
3.2. Accessibility
3.3. Continuity and Reliability
3.4. Water Safety (Quality & Risk)
3.4.1. Measures of Drinking Water Quality
| WHO water quality risk levels | |
|---|---|
| Risk level | E. coli (CFU/100 mL) |
| Conformity | <1 |
| Low | 1–10 |
| Intermediate | 11–100 |
| High | 101–1,000 |
| Very High | >1,000 |
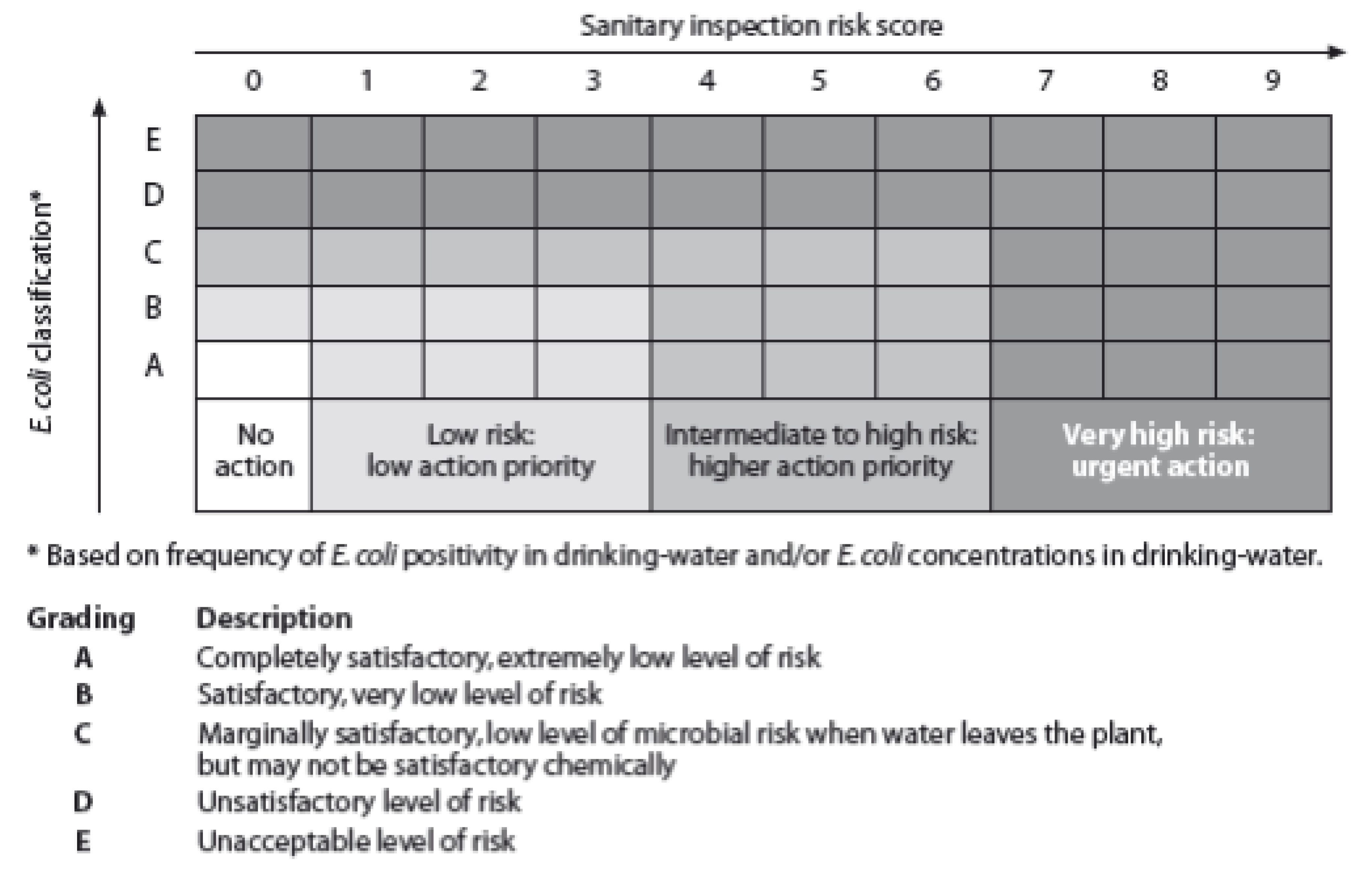
3.4.2. Sanitary Risk
3.4.3. Combined Analysis
3.5. Quantity
3.6. Equity, Non-Discrimination
3.7. Cost and Affordability
4. Water Service Delivery Indicators, Frameworks and Indices: Benefits and Challenges for Implementation, Policy, and Planning
4.1. A Scale for Each Indicator
4.2. Monitoring Framework Approaches
- The first is the use of service levels as a simple summary description for which the JMP approach provides a well-recognized example [2]. The value of its simplicity in communication is evident as it maximizes comparability over time and space. It is also easily collected across geographical settings. Its weakness is the counter-face of that simplicity; it does not provide the more nuanced analysis of the factors that influence public health, economic development, and fulfillment of human rights.
- The second is a “level platform” of a set of indicators that typically include service type, safety, quantity, accessibility, reliability or continuity of service, affordability, and more recently equity and non-discrimination. The level platform enables all concerns to be monitored and additional concerns to be included at limited risk to integrity. Many individual indicators are inter-dependent, however, and subsequent indicators are likely to have lesser impact on overall outcome. However these same factors are its weaknesses.
- The third attempts to take some account of inter-dependencies and is based on the concept that a limited number of indicators can be meaningfully distinguished because certain indicators are derivatives of others [26]. The “value” of each indicator category can be discounted by lesser degrees of quality or continuity/reliability. In its derivation it assumes for example that access and continuity/reliability determine quantity and thus there is no merit in inclusion of quantity as a separate parameter. This is important at the national and international level where limited resources are available for monitoring. It is also useful to provide some logical relationship among indicators. The evident weakness is that while this derivation is logical, the evidence for the specific inter-dependencies is weak and may to a greater or lesser extent be context-specific in practice.
- The fourth takes a single measure from all indicators measured. For example, the IRC water service framework takes the worst performing indicator’s level to measure the service delivered [20]. The advantage is twofold: there is a single value for a service and this value can be disaggregated and the value for each indicator revealed. The disadvantages of taking the worst valued indicator are that detail on all other indicators measured is lost and their benefits are ignored.
4.3. Combination of Indicators into an Index
4.4. Evaluating Monitoring Frameworks
5. Conclusions
Acknowledgements
Conflicts of Interest
References
- Bradley, D.; Bartram, J. Domestic water and sanitation as water security: Monitoring, concepts and strategy. Phil. Trans. R. Soc. Ser. A 2013, in press. [Google Scholar]
- WHO/UNICEF. Joint Monitoring Programme for Water Supply and Sanitation; Meeting the MDG Drinking Water and Sanitation Target: A Mid-Term Assessment of Progress, 2004; World Health Organization & United Nations Children’s Fund: Geneva, Switzerland, 2004. [Google Scholar]
- Onda, K.; LoBuglio, J.; Bartram, J. Global access to safe water: Accounting for water quality and the resulting impact on MDG progress. Int. J. Environ. Res. Public Health 2012, 93, 880–894. [Google Scholar]
- Lee, E.; Schwab, K. Deficiencies in drinking water distribution systems in developing countries. J. Water Health 2005, 3, 109–127. [Google Scholar]
- Bartram, J. Improving on haves and have-nots. Nature 2008, 452, 283–284. [Google Scholar] [CrossRef]
- Rizak, S.; Hrudey, S. Drinking-water safety—Challenges for community managed systems. J. Water Health 2008, 6, 33–41. [Google Scholar] [CrossRef]
- Albuquerque, C. Statement by Catarina de Albuquerque, Independent Expert on the Issue of Human Rights Obligations Related to Access to Safe Drinking Water and Sanitation. In Proceedings of the 65th session of the UN General Assembly, New York, NY, USA, 6 August 2010.
- Meier, B.; Kayser, G.L.; Amjad, U.; Bartram, J. Implementing an evolving human right through water & sanitation policy. Water Policy 2013, 15, 116–133. [Google Scholar] [CrossRef]
- Howard, G.; Bartram, J. Domestic Water Quantity, Service Level and Health; World Health Organization: Geneva, Switzerland, 2003. [Google Scholar]
- Moe, C.L.; Rheingans, R.D. Global challenges in water, sanitation and health. J. Water Health 2006, 4, 41–57. [Google Scholar]
- Haas, P.M. Epistemic communities and international policy coordination. Int. Organ. 1992, 46, 1–35. [Google Scholar] [CrossRef]
- Conca, K. Governing Water: Contentious Transnational Politics and Global Institution Building; MIT Press: Cambridge, UK, 2005. [Google Scholar]
- Albuquerque, C. Consultation on Post 2015 Indicators for Water and Sanitation; Keynote for the Office for the High Commissioner for Human Rights, United Nations: Geneva, Switzerland, May 2011. [Google Scholar]
- Albuquerque, C. The Human Right to Water and Sanitation: What, Why, How and Monitored by Whom? In Proceeding of the 1st Consultation on Post 2015 Indicators for Water and Sanitation, Berlin, Germany, 3–5 May 2011.
- Gruskin, S.; Ferguson, L. Using indicators to determine the contribution of human rights to public health efforts. Bull. World Health Organ. 2009, 87, 714–719. [Google Scholar] [CrossRef]
- Meier, B.; Kayser, G.L.; Amjad, U.; Kestenbaum, J.; Bartram, J. Practice of developing human rights indicators to facilitate accountability for the human right to water and sanitation. J. Human Rights Pract. 2013, in press. [Google Scholar]
- Rosga, A.; Satterthwaite, M. The trust in indicators: Measuring human rights. Berkeley J. Int. Law 2009, 27, 253–310. [Google Scholar]
- WHO; UNICEF. JMP Goals, Targets, Indicators: Post-2015 Global Monitoring. Available online: http://www.wssinfo.org/post-2015-monitoring/overview/ (accessed on 16 June 2013).
- Ostrom, E. Background on the institutional analysis and development framework. Policy Stud. J. 2011, 39, 7–27. [Google Scholar] [CrossRef]
- Moriarty, P.; Batchelor, C.; Fonseca, C.; Klutze, A.; Naafs, A.; Nyarko, A.; Pezon, K.; Potter, A.; Reddy, A.; Snehalatha, R. Ladders for Assessing and Costing Water Service Delivery, 2nd ed.; International Water and Sanitation Centre (IRC): The Hague, the Netherlands, 2011. [Google Scholar]
- Howard, G.; Bartram, J. Effective water supply surveillance in urban areas of developing countries. J. Water Health 2005, 31, 31–43. [Google Scholar]
- White, G.F.; Bradley, D.J.; White, A.U. Drawers of Water: Domestic Water Use in East Africa; University of Chicago Press: Chicago, IL, USA, 1972. [Google Scholar]
- Lloyd, B.J.; Bartram, J. Surveillance solutions to microbiological problems in water quality control in developing countries. Water Sci. Technol. 1991, 24, 61–75. [Google Scholar]
- WHO. Guidelines for Drinking-Water Quality: Surveillance and Control of Community Supplies; WHO: Geneva, Switzerland, 1997; Volume 3. [Google Scholar]
- UNICEF,WHO. Progress on Drinking Water and Sanitation, Special Focus on Sanitation; WHO: Geneva, Switzerland, 2008. [Google Scholar]
- Bartram, J. Optimizing the Monitoring and Assessment of Rural Water Supplies. Ph.D. Thesis, University of Surrey, Surrey, UK, 1996. [Google Scholar]
- Bradley, D.; Bartram, J. Domestic Water and Sanitation as Water Security: Monitoring, Concepts and Strategy. Unpublished work. 26 February 2013. [Google Scholar]
- Cairncross, S.; Feachman, R. Environmental Health Engineering in the Tropics: An Introductory Text; John Wiley & Sons: Chichester, UK, 1993. [Google Scholar]
- Gilman, R.; Marquis, G.; Ventura, G.; Campos, M.; Spira, W.; Diaz, F. Water cost and availability: Key determinants of family hygiene in a peruvian shantytown. Am. J. Public Health 1993, 83, 1554–1558. [Google Scholar] [CrossRef]
- Tompson, J.; Porras, I.T.; Tumwine, J.K.; Mukwahuzi, M.R.; Katui-Katua, M.; Johnson, N.; Wood, L. Drawers of Water II: 30 years of Change in Domestic Water Use and Environmental Health in East Africa; International Institute for Environment & Development: London, UK, 2001. [Google Scholar]
- United Nations. Resolution on Human Right to Water and Sanitation, UN General Assembly Research A/64/292; United Nations: New York, NY, USA, 2010. [Google Scholar]
- United Nations Committee on Economic, Social and Cultural Rights (UNCESCR). General Comment No. 15: The Right to Water (Arts. 11 and 12 of the Covenant). United Nations: New York, NY, USA, 2003. Available online: http://www.unhchr.ch/tbs/doc.nsf/0/a5458d1d1bbd713fc1256cc400389e94 (accessed on 16 June 2013).
- WHO/UNICEF. The History of the JMP. Available online: http://www.wssinfo.org/about-the-jmp/history/ (accessed on 15 February 2013).
- WHO/UNICEF. Joint Monitoring Programme for Water Supply and Sanitation. The Drinking-Water and Sanitation Ladders; WHO/UNICEF JMPWSS: Geneva, Switzerland, 2010. Available online: http://www.wssinfo.org/definitions-methods/watsan-ladder (accessed on 16 June 2013).
- Renwick, M.; Joshi, D.; Huang, M.; Kong, S.; Petova, S.; Bennett, G.; Bingham, R.; Fonseca, C.; Moriarty, P.; Smits, S.; et al. Multiple-Use Water Services for the Poor: Assessing the State of Knowledge; Winrock International: Arlington, VA, USA, 2007. Available online: http://www.winrock.org/sites/default/files/publications/attachments/Gates%20Final%20Report%20MUS%20no%20annex%20horizontal.pdf (accessed on 2 September 2013).
- Van Koppen, B.; Moriarty, P.; Boelee, E.; Hagmann, J. Multiple Use Water Services to enhance the Millennium Development Goals, Report 98; International Water Management Institute: Battaramulla, Sri Lanka, 2006. [Google Scholar]
- Smits, S.; Moriarty, P.; Penning de Vries, F.; Mikhail, M.; Boelee, E. Climbing the Water Ladder—Multiple-Use Water Services for Poverty Reduction; International Water and Sanitation Centre (IRC): The Hague, The Netherlands, 2009. [Google Scholar]
- van Koppen, B.; Burr, P.; Fonseca, C. Applying the Life-Cycle Costs approach to Water: Costs and Service Levels in Andhra Pradesh (India), Burkina Faso, Ghana and Mozambique; International Water and Sanitation Centre (IRC): The Hague, The Netherlands, 2012. [Google Scholar]
- Adank, M.; Kumasi, T.; Abbey, E.; Dickinson, N.; Dzansi, P.; Alengdem, J.; Chimbar, T.; Effah-Appiah, E. The Status of Rural Water Services in Ghana. A Synthesis of Findings from 3 Districts; International Water and Sanitation Centre (IRC): The Hague, The Netherlands, 2013. [Google Scholar]
- Skinner, J. WhereEvery Drop Counts: Tacking Rural Africa’s Water Crisis; International Institute for Environment and Development (IIED): London, UK, 2009. [Google Scholar]
- Taylor, B. Addressing the Sustainability Crisis: Lessons from Research on Managing Rural Water Projects; WaterAid: Clearwater, Tanzania, 2009. [Google Scholar]
- Moriarty, P.; Nyarko, K.B.; Dwumfour-Asare, B.; Appiah-Effah, E.; Obuobisa-Darko, A. Life-Cycle Costs in Ghana: Background and Methodology; International Water and Sanitation Centre: The Hague, The Netherlands, 2011. [Google Scholar]
- Moriarty, P.; Nyarko, K.B.; Dwumfour-Asare, B.; Appiah-Effah, E.; Obuobisa-Darko, A. Access to Water Services in Rural Areas and Small Towns in Ghana; International Water and Sanitation Centre: The Hague, The Netherlands, 2011. [Google Scholar]
- Montgomery, M.A.; Elimelech, M. Water and sanitation in developing countries: Including health in the equation. Environ. Sci. Technol. 2007, 41, 17–24. [Google Scholar] [CrossRef]
- Sorenson, S.B.; Morissink, C.; Abril Campos, P. Safe access to safe water in low income countries: Water fetching in current times. Soc. Sci. Med. 2011, 72, 1522–1526. [Google Scholar] [CrossRef]
- Hughes, C.; Le, T.P.; Bartram, J. Water and sanitation in schools: A systematic review of the health and hygiene outcomes. Int. J. Environ. Res. Public Health 2012, 9, 2772–2787. [Google Scholar] [CrossRef]
- Geere, J.; Hunter, P.; Jagals, P. Domestic water carrying and its implications for health: A review of mixed methods pilot study in Limpopo Province, South Africa. Environ. Health 2010, 9, 52–63. [Google Scholar] [CrossRef]
- Levy, K.; Nelson, K.; Hubbard, A.; Eisenberg, J. Following the water: A controlled study of drinking water storage in northern coastal Ecuador. Environ. Health Perspect. 2008, 116, 1533–1540. [Google Scholar] [CrossRef]
- Wright, J.; Grundy, S.; Conroy, R. Household drinking water in developing countries: A systematic review of microbiological contamination between source and point-of-use. Trop. Med. Int. Health 2004, 9, 106–117. [Google Scholar] [CrossRef]
- Trevett, A.F.; Carter, R.C.; Tyrrel, S.F. The importance of domestic water quality management in the context of fecal-oral disease transmission. J. Water Health 2005, 3, 259–270. [Google Scholar]
- Clasen, T.F.; Bastable, A. Fecal contamination of drinking water during collection and household storage: The need to extend protection to the point of use. J. Water Health 2003, 1, 109–115. [Google Scholar]
- Pickering, A.; Davis, J. Freshwater availability affects child health in sub-Saharan Africa. Environ. Sci. Technol. 2012, 46, 2391–2397. [Google Scholar] [CrossRef]
- Hutton, G. Global Costs and Benefits of Drinking-Water Supply and Sanitation Interventions to Reach the MDG Target and Universal Coverage; World Health Organization: Geneva, Switzerland, 2012. [Google Scholar]
- Hutton, G.; Haller, L.; Bartram, J. Global cost-benefit analysis of water supply and sanitation interventions. J. Water Health 2007, 5, 481–502. [Google Scholar] [CrossRef]
- Pattanvak, S.; Yang, J.; Whittington, D.; Kumar, K. Coping with unreliable public water supplies: Averting expenditures by households in Kathmandu, Nepal. Water Resour. Res. 2005, 41, 1–11. [Google Scholar]
- Subbaraman, R.; Shitole, S.; Shitole, T.; Sawant, K.; O’Brien, J.; Bloom, D.E.; Patil-Deshmukh, A. The social ecology of water in a Mumbai slum: Failures in water quality, quantity, and reliability. BMC Public Health 2013, 13. [Google Scholar] [CrossRef]
- Hunter, P.R.; Zmirou-Navier, D.; Hartemann, P. Estimating the impact on health of poor reliability of drinking water interventions in developing countries. Sci. Total Environ. 2009, 407, 2621–2624. [Google Scholar] [CrossRef]
- Risebro, H.L.; Doria, M.F.; Andersson, Y.; Medema, G.; Osborn, K.; Schlosser, O.; Hunter, P.R. Fault tree analysis of the causes of waterborne outbreaks. J. Water Health 2007, 5, 1–18. [Google Scholar] [CrossRef]
- Nygard, K.; Wahl, E.; Krogh, T.; Tveit, O.A.; Bohleng, E.; Tverdal, A. Breaks and maintenance work in the water distribution systems and gastrointestinal illness: A cohort study. Int. J. Epidemiol. 2007, 36, 873–880. [Google Scholar] [CrossRef]
- World Health Organization. Guidelines for Drinking-water Quality, 2nd ed.; WHO: Geneva, Switzerland, 1997; Volume 3. [Google Scholar]
- Pruss, A.; Kay, D.; Fewtrell, L.; Bartram, J. Estimating the burden of disease from water, sanitation, and hygiene at a global level. Environ. Health Perspect. 2002, 110, 537–542. [Google Scholar] [CrossRef]
- Esrey, S.A.; Potash, J.B.; Roberts, L.; Shiff, C. Effects of improved water supply and sanitation on ascariasis, diarrhoea, dracunculiasis, hookworm infection, schistosomiasis, and trachoma. Bull. World Health Organ. 1991, 69, 609–621. [Google Scholar]
- Fewtrell, L.; Kaufman, R.; Kay, D.; Enanoria, W.; Haller, L.; Colford, J. Water, sanitation, and hygiene intervention to reduce diarrhea in less developed countries: A systematic review and meta-analysis. Lancet Infect. Dis. 2005, 5, 42–52. [Google Scholar] [CrossRef]
- Clasen, T.; Schmidt, W.P.; Rabie, T.; Roberts, I.; Cairncross, S. Interventions to improve water quality for preventing diarrhea: Systematic review and meta-analysis. BMJ 2007, 335, 782–792. [Google Scholar] [CrossRef]
- Nokes, C.; Grantham-McGregor, S.M.; Sawyer, A.W.; Cooper, E.S.; Bundy, D.A. Parasitic helminth infection and cognitive function in school children. Proc. Biol. Sci. 1992, 247, 77–81. [Google Scholar] [CrossRef]
- Sakti, H.; Nokes, C.; Hertanto, W.S.; Hendratno, S.; Hall, A. Evidence for an association between hookworm infection and cognitive function in Indonesian school children. Trop. Med. Int. Health 1999, 4, 322–334. [Google Scholar] [CrossRef]
- Cutler, D.; Miller, G. The role of public health improvements in health advances: The twentieth-Century United States. Demography 2005, 42, 1–22. [Google Scholar] [CrossRef]
- World Health Organization. Guidelines for Drinking-Water Quality, 3rd ed.; WHO: Geneva, Switzerland, 2004; Volume 1. [Google Scholar]
- WHO/UNICEF. Rapid Assessment of Drinking Water Quality: A Handbook for Implementation; World Health Organization & United Nations Children’s Fund: Geneva, Switzerland, 2011. [Google Scholar]
- Teschke, K.; Bellack, N.; Shen, H.; Atwater, J.; Chu, R.; Koehoorn, M.; MacNab, Y.C.; Schreier, H.; Isaac-Renton, J.L. Water and sewage systems, socio-demographics, and duration of residence associated with endemic intestinal infectious diseases: A cohort study. BMC Public Health 2010, 10, 767. [Google Scholar] [CrossRef]
- Gunnarsdottir, M.; Gardarsson, S.; Elliot, M.; Sigmudsdottir, G.; Bartram, J. Benefits of water safety plans: Microbiology, compliance, and public health. Environ. Sci. Technol. 2012, 4614, 7782–7789. [Google Scholar]
- Luby, S.P.; Gupta, S.K.; Sheikh, M.A.; Johnston, R.B.; Ram, P.K.; Islam, M.S. Tubewell water quality and predictors of contamination in three flood-prone areas in Bangladesh. J. Appl. Microbiol. 2008, 105, 1002–1008. [Google Scholar] [CrossRef]
- Howard, G.; Pedley, S.; Barrett, M.; Nalubega, M.; Johal, K. Risk factors contributing to microbiological contamination of shallow groundwater in Kampala, Uganda. Water Res. 2003, 37, 3421–34219. [Google Scholar] [CrossRef]
- Bradley, D. Health Aspects of Water Supplies in Tropical Countries. In Water Wastes and Health in Hot Climates; Feachem, R., McGarry, M., Mara, D., Eds.; John Wile and Sons: Chichester, UK, 1977. [Google Scholar]
- Whittington, D. What have we learned from 20 years of stated preference research in less-developed countries? Annu. Rev. Resour. Econ. 2010, 2, 209–236. [Google Scholar] [CrossRef]
- Roaf, V.; Khalfan, A.; Langford, M. Monitoring Implementation of the Right to Water: A Framework for Developing Indicators; Heinrich Böll Foundation: Berlin, Germany, 2005. Available online: http://www.boell.de/internationalepolitik/internationale-politik-2143.html (accessed on 16 June 2013).
- UNICEF; WHO. Drinking Water Equity, Safety and Sustainability: Thematic Report on Drinking Water; WHO: Geneva, Switzerland, 2011. [Google Scholar]
- Snehalatha, M.; Busenna, P.; Ratna Reddy, V.; Anitha, V. Rural Drinking Water Service Levels: A Study of Andhra Pradesh, South India; Center for Economic and Social Studies: Andhra Pradesh, India, 2011. [Google Scholar]
- WHO. UN-Water Global Annual Assessment of Sanitation and Drinking-Water (GLAAS)2010: Targeting Resources for Better Results; WHO: Geneva, Switzerland, 2010. [Google Scholar]
- Cullis, J.; van Koppen, B. Research Report 113: Applying the Gini Coefficient to Measure Inequality of Water Use in the Olifants River Water Management Area, South Africa; International Water Management Institute: Colombo, Sri Lanka, 2007. [Google Scholar]
- Wang, X.-J.; Zhang, J.-Y.; Shahid, S.; El Madi, A.; He, R.-M.; Wang, X.-G.; Ali, M. Gini coefficients to assess equity in domestic water supply in the Yellow River. Mitig. Adapt. Strategy Glob. Chang. 2012, 17, 65–75. [Google Scholar] [CrossRef]
- Kirigia, G.G.; Kirigia, J.M. Inequalities in selected health-related millennium development goals indicators in all WHO member states. Afr. J. Health Sci. 2007, 14, 171–186. [Google Scholar]
- Luh, J.; Braum, R.; Bartram, J. Equity in water and sanitation: Developing an index to measure progressive realization of the human right. Int. J. Hyg. Environ. Health 2013. [Google Scholar] [CrossRef]
- Lockwood, H.; Smits, S. Supporting Rural Water Supply: Moving towards a Service Delivery Approach; Practical Action: London, UK, 2011. [Google Scholar]
- Hutton, G. Monitoring “Affordability”of Water and Sanitation Services after 2015: Review of Global Indicator Options; United Nations Office of the High Commissioner for Human Rights: Geneva, Switzerland, 2012. [Google Scholar]
- Fonseca, C.; Franceys, R.; Batchelor, C.; McIntyre, P.; Klutse, A.; Komives, K.; Moriarty, P.; Naafs, A.; Nyarko, K.; Pezo, C.; et al. Life-Cycle Costs Approach: Costing Sustainable Services; IRC International Water and Sanitation Centre: The Hague, The Netherlands, 2011. [Google Scholar]
- Ntengw, F. The impact of consumer awareness of water sector issues on willingness to pay and cost recovery in Zambia. Phys. Chem. Earth 2004, 29, 1301–1308. [Google Scholar] [CrossRef]
- Ginneken, M.; Netterstron, U.; Bennett, A. More, Better, or Different Spending? Trends in Public Expenditure on Water and Sanitation in Sub-Saharan Africa; The World Bank: Washington, DC, USA, 2012. [Google Scholar]
- Sullivan, C. Calculating a water poverty index. World Dev. 2002, 30, 1195–1210. [Google Scholar] [CrossRef]
- Simon, S. A framework for sustainable water management: Integrating ecological constraints in policy tools in the UK. Environ. Pract. 1999, 1, 19–30. [Google Scholar]
- Sullivan, C.A. The Development and Testing of a Water Poverty Index; Progress report to DFID; Centre for Ecology and Hydrology: Wallingford, UK, 2001. [Google Scholar]
- Giné, R.; Pérez-Fogut, A. Improved method to calculate the Water Poverty Index at local scale. ASCE J. Environ. Eng. 2010, 136, 1287–1298. [Google Scholar] [CrossRef]
© 2013 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Kayser, G.L.; Moriarty, P.; Fonseca, C.; Bartram, J. Domestic Water Service Delivery Indicators and Frameworks for Monitoring, Evaluation, Policy and Planning: A Review. Int. J. Environ. Res. Public Health 2013, 10, 4812-4835. https://doi.org/10.3390/ijerph10104812
Kayser GL, Moriarty P, Fonseca C, Bartram J. Domestic Water Service Delivery Indicators and Frameworks for Monitoring, Evaluation, Policy and Planning: A Review. International Journal of Environmental Research and Public Health. 2013; 10(10):4812-4835. https://doi.org/10.3390/ijerph10104812
Chicago/Turabian StyleKayser, Georgia L., Patrick Moriarty, Catarina Fonseca, and Jamie Bartram. 2013. "Domestic Water Service Delivery Indicators and Frameworks for Monitoring, Evaluation, Policy and Planning: A Review" International Journal of Environmental Research and Public Health 10, no. 10: 4812-4835. https://doi.org/10.3390/ijerph10104812
APA StyleKayser, G. L., Moriarty, P., Fonseca, C., & Bartram, J. (2013). Domestic Water Service Delivery Indicators and Frameworks for Monitoring, Evaluation, Policy and Planning: A Review. International Journal of Environmental Research and Public Health, 10(10), 4812-4835. https://doi.org/10.3390/ijerph10104812