Volcanic Ash and Daily Mortality in Sweden after the Icelandic Volcano Eruption of May 2011

Abstract
:1. Introduction
2. Material and Methods
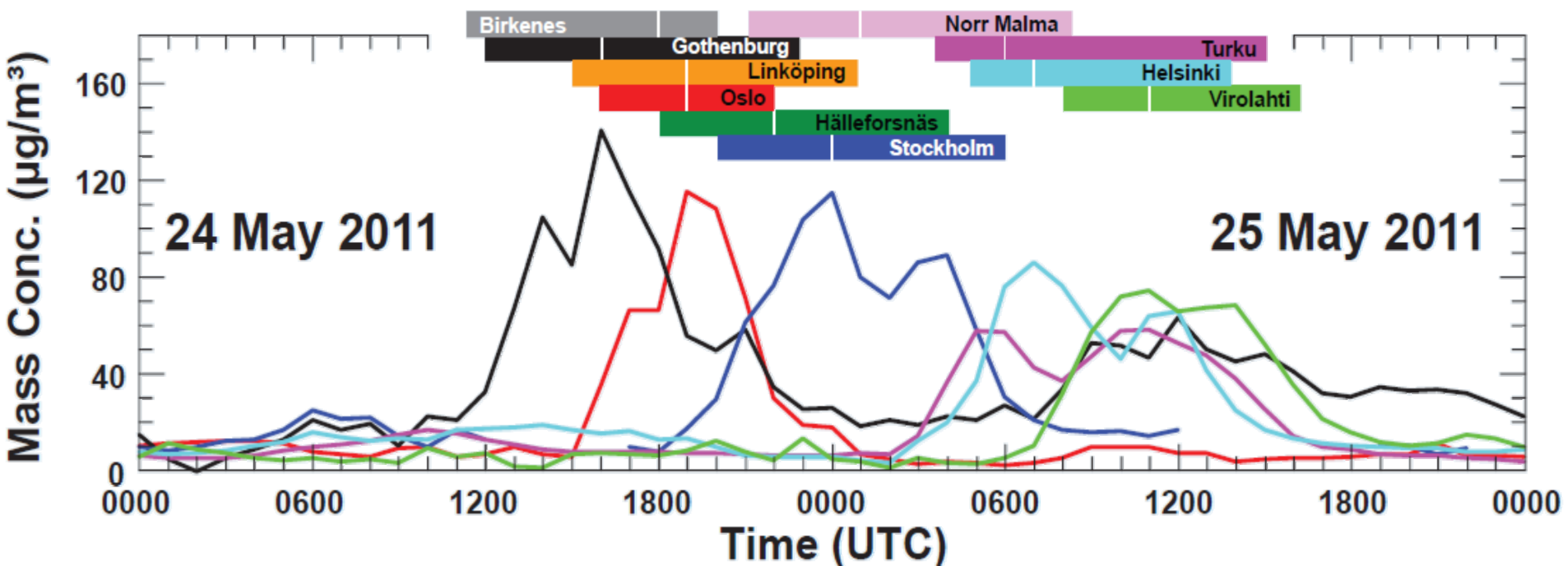
2.1. Particle Concentration Measurements
2.2. Exposure Assessment

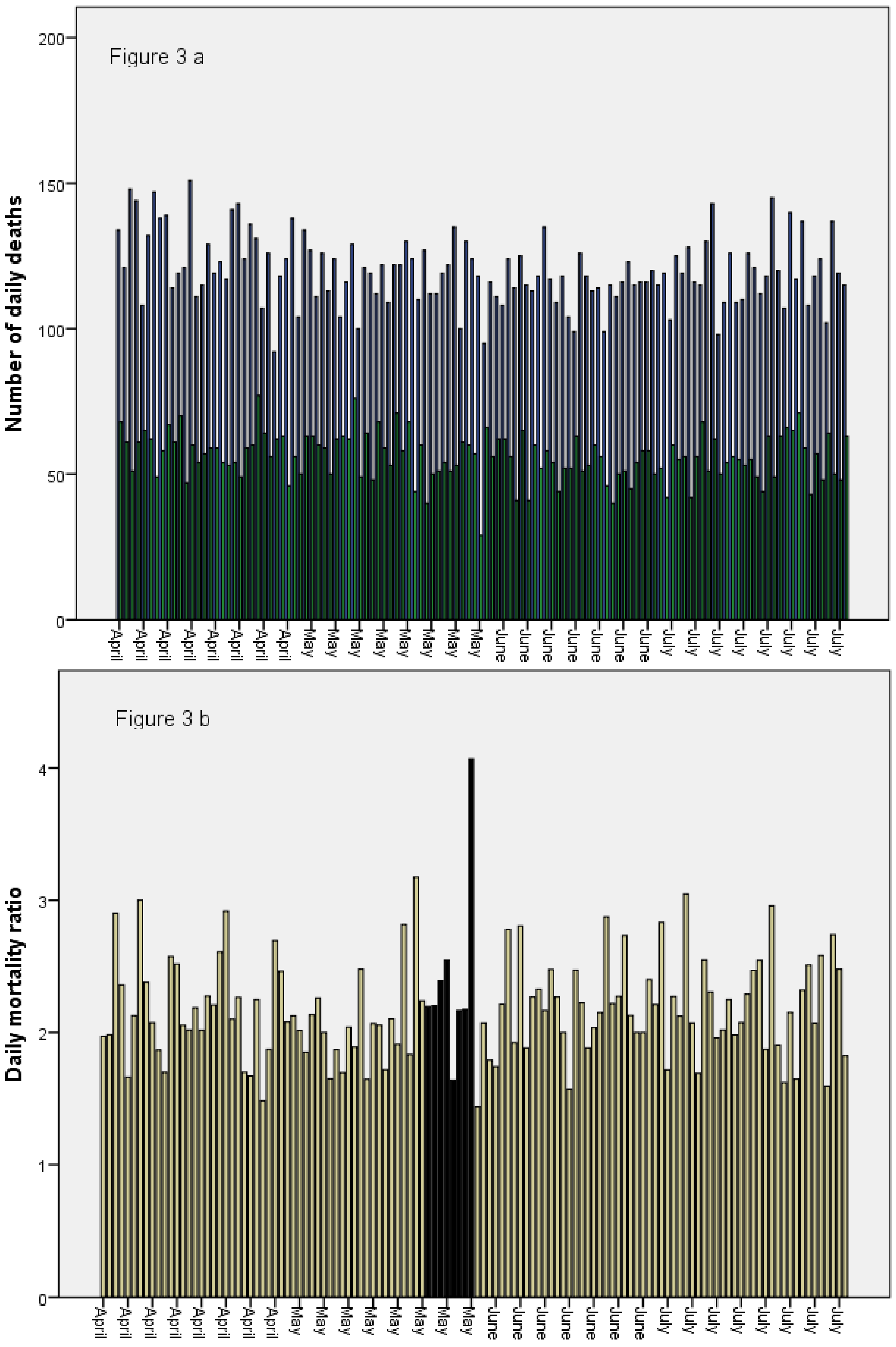
2.3. Mortality Data and Assessment of Impact on Mortality

3. Results

{kind=link}
{kind=link}
{kind=link}
| Outcome | Area | Mean/Median | Exposure Period (24–31 May) | Control Period (1 April–23 May, 1–31 June) |
|---|---|---|---|---|
| Number of daily deaths | Ash area | Mean | 120 | 120 |
| Median | 121 | 119 | ||
| No ash area | Mean | 52 | 56 | |
| Median | 54 | 56 | ||
| Mortality ratios 1 | Mean | 2.42 | 2.17 | |
| Median | 2.20 | 2.13 |

4. Discussion
5. Conclusions
Conflicts of Interest
References
- Tesche, M.; Glantz, P.; Johansson, C.; Norman, M.G.; Hiebsch, A.; Seifert, P.; Ansmann, A.; Engelmann, R.; Althausen, D. Volcanic ash over Scandinavia originating from the Grímsvötn eruptions in May 2011. J. Geophys. Res. 2012, 117. [Google Scholar] [CrossRef]
- Kerminen, V.-M.; Niemi, J.V.; Timonen, H.; Aurela, M.; Frey, A.; Carbone, S.; Saarikoski, S.; Teinilä, K.; Hakkarainen, J.; Tamminen, J.; et al. Characterization of a volcanic ash episode in southern Finland caused by the Grimsvötn eruption in Iceland in May 2011. Atmos. Chem. Phys. 2011, 11, 24933–24968. [Google Scholar] [CrossRef]
- Carlsen, H.K.; Zoëga, H.; Valdimarsdóttir, U.; Gíslason, T.; Hrafnkelsson, B. Hydrogen sulfide and particle matter levels associated with increased dispensing of anti-asthma drugs in Iceland’s capital. Environ. Res. 2012, 113, 33–39. [Google Scholar] [CrossRef]
- Meister, K.; Johansson, C.; Forsberg, B. Estimated short-term effects of coarse particles on daily mortality in Stockholm, Sweden. Environ. Health Perspect. 2011, 120, 431–436. [Google Scholar] [CrossRef]
- Oudin, A.; Strömberg, U.; Jakobsson, K.; Stroh, E.; Björk, J. Estimations of short-term effects of air pollution on stroke hospital admissions in Southern Sweden. Neuroepidemiology 2009, 34, 131–142. [Google Scholar]
- Pope, C.A., 3rd; Muhlestein, J.B.; May, H.T.; Renlund, D.G.; Anderson, J.L.; Horne, B.D. Ischemic heart disease events triggered by short-term exposure to fine particulate air pollution. Circulation 2006, 114, 2443–2448. [Google Scholar]
- Dominici, F.; Peng, R.D.; Bell, M.L. Fine particulate air Pollution and hospital admission for cardiovascular and respiratory diseases. JAMA 2006, 295, 1127–1135. [Google Scholar] [CrossRef]
- Witham, C.S.; Oppenheimer, C. Mortality in England during the 1783–4 Laki Craters eruption. Bull. Volcanol. 2004, 67, 15–26. [Google Scholar]
- Smithsonian, Global Volcanism Program: Worldwide Holocene Volcano and Eruption Information. 2012. Available online: http://www.volcano.si.edu/volcano.cfm?vn=372030 (accessed on 6 December 2013).
- Thordarson, T.; Larsen, G. Volcanism in Iceland in historical time: Volcano types, eruption styles and eruptive history. J. Geodynamics 2007, 43, 118–152. [Google Scholar] [CrossRef]
- Schmidt, A.; Ostro, B.; Carslaw, K.S.; Wilson, M.; Thordarson, T.; Mann, G.W.; Simmons, A.J. Excess mortality in Europe following a future Laki-style Icelandic eruption. Proc. Nat. Acad. Sci. USA 2011, 108, 15710–15715. [Google Scholar] [CrossRef]
- Small, C.; Naumann, T. The global distribution of human population and recent volcanism. Environ. Hazards 2001, 3, 93–109. [Google Scholar]
- Hansell, A.L.; Horwell, C.J.; Oppenheimer, C. The health hazards of volcanoes and geothermal areas. Occup. Environ. Med. 2006, 63, 149–156. [Google Scholar] [CrossRef]
- Horwell, C.; Baxter, P. The respiratory health hazards of volcanic ash: A review for volcanic risk mitigation. Bull. Volcanol. 2006, 69, 1–24. [Google Scholar] [CrossRef]
- Ferm, M.; Peterson, K.; Svanberg, P.-A.; Lövblad, G. Cost-efficient Measurements of PM10 Using Simple Sampling Equipment. EMEP/CCC-Report; Hanssen, Norway, 2000. Available online: http://www.nilu.no/projects/CCC/reports/cccr9-2000.pdf#page=107 (accessed on 6 December 2013).
- Newnham, R.M.; Dirks, K.N.; Samaranayake, D. An investigation into long-distance health impacts of the 1996 eruption of Mt. Ruapehu. Atmos. Environ. 2010, 44, 1568–1578. [Google Scholar] [CrossRef]
- Zeger, S.L.; Thomas, D.; Dominici, F.; Samet, J.M.; Schwartz, J.; Dockery, D.; Cohen, A. Exposure measurement error in time-series studies of air pollution: Concepts and consequences. Environ. Health Perspect. 2000, 108, 419–426. [Google Scholar] [CrossRef]
- Norman, M.; Johansson, C. Studies of some measures to reduce road dust emissions from paved roads in Scandinavia. Atmos. Environ. 2006, 40, 6154–6164. [Google Scholar] [CrossRef]
- Kupiainen, K.J.; Pirjola, L. Vehicle non-exhaust emissions from the tyre-road interface—Effect of stud properties, traction sanding and resuspension. Atmos. Environ. 2011, 45, 4141–4146. [Google Scholar] [CrossRef]
- Omstedt, G.; Bringfelt, B.; Johansson, C. A model for vehicle-induced non-tailpipe emissions of particles along Swedish roads. Atmos. Environ. 2005, 39, 6088–6097. [Google Scholar]
- Ketzel, M.; Omstedt, G.; Johansson, C.; Düring, I.; Pohjola, M.; Oettl, D.; Gidhagen, L.; Wåhlin, P.; Lohmeyer, A.; Haakana, M.; et al. Estimation and validation of PM2.5/PM10 exhaust and non-exhaust emission factors for practical street pollution modelling. Atmos. Environ. 2007, 41, 9370–9385. [Google Scholar] [CrossRef]
- Stevenson, J.A.; Loughlin, S.C.; Font, A.; Fuller, G.W.; MacLeod, A.; Oliver, I.W.; Jackson, B.; Horwell, C.J.; Thordarson, T.; Dawson, I. UK monitoring and deposition of tephra from the May 2011 eruption of Grimsvotn, Iceland. J. Appl. Volcanol. 2013, 2. [Google Scholar] [CrossRef] [Green Version]
© 2013 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Oudin, A.; Carlsen, H.K.; Forsberg, B.; Johansson, C. Volcanic Ash and Daily Mortality in Sweden after the Icelandic Volcano Eruption of May 2011. Int. J. Environ. Res. Public Health 2013, 10, 6909-6919. https://doi.org/10.3390/ijerph10126909
Oudin A, Carlsen HK, Forsberg B, Johansson C. Volcanic Ash and Daily Mortality in Sweden after the Icelandic Volcano Eruption of May 2011. International Journal of Environmental Research and Public Health. 2013; 10(12):6909-6919. https://doi.org/10.3390/ijerph10126909
Chicago/Turabian StyleOudin, Anna, Hanne K. Carlsen, Bertil Forsberg, and Christer Johansson. 2013. "Volcanic Ash and Daily Mortality in Sweden after the Icelandic Volcano Eruption of May 2011" International Journal of Environmental Research and Public Health 10, no. 12: 6909-6919. https://doi.org/10.3390/ijerph10126909