Correlates of Unsupervised Bathing of Infants: A Cross-Sectional Study


Abstract
:1. Introduction
2. Experimental Section
2.1. Participants and Setting
2.2. Design
2.3. Parental Supervision
2.4. Potential Correlates
2.5. Statistical Analyses
3. Results and Discussion
3.1. Participants

{kind=link}
| Total group | Children left unsupervised | Children never left unsupervised | p value | |
|---|---|---|---|---|
| Infant is bathed in bathtub | n = 1,410 | n = 87 | n = 1,319 | |
| Child characteristics | n (%) | n (%) | n (%) | |
| Mean age in months (SD) | 7.2 (1.1) | 7.5 (1.2) | 7.2 (1.1) | 0.01 ** |
| Range in months | 4–12 | 4–12 | 4–12 | |
| Gender | ||||
| Girl | 681 (48.3) | 47 (54.0) | 633 (48.0) | 0.28 * |
| Child can crawl | ||||
| Yes | 484 (34.4) | 34 (39.1) | 450 (34.2) | 0.35 * |
| Family characteristics | n (%) | n (%) | n (%) | |
| Mother is respondent | 1,315 (93.3) | 83 (95.4) | 1,229 (93.2) | 0.71 * |
| Family situation | ||||
| One-parent family | 39 (2.8) | 3 (3.5) | 36 (2.7) | 0.67 * |
| Number of children in family | ||||
| One child | 682 (48.4) | 34 (39.1) | 645 (48.9) | 0.08 * |
| Two or more children | 728 (51.6) | 53 (60.9) | 674 (51.1) | |
| Mother | ||||
| Employment | ||||
| Paid job fulltime | 90 (6.6) | 7 (8.5) | 83 (6.5) | 0.63 * |
| Paid job part time | 1,024 (75.1) | 63 (76.8) | 959 (75.1) | |
| No paid job | 249 (18.3) | 12 (14.6) | 235 (18.4) | |
| Educational level | ||||
| Low | 234 (16.6) | 11 (12.6) | 222 (16.9) | 0.51 * |
| Intermediate | 623 (44.2) | 38 (43.7) | 583 (44.3) | |
| High | 551 (39.1) | 38 (43.7) | 512 (38.9) | |
| Ethnicity | ||||
| Western | 1,292 (91.6) | 79 (90.8) | 1,211 (91.8) | 0.55 * |
| Non Western | 118 (8.4) | 8 (9.2) | 108 (8.2) | |
| Father | ||||
| Employment | ||||
| Paid job fulltime | 1,149 (85.7) | 70 (87.5) | 1,076 (85.6) | 0.81 * |
| Paid job part time | 138 (10.3) | 6 (7.5) | 131 (10.4) | |
| No paid job | 54 (4.0) | 4 (5.0) | 50 (4.0) | |
| Educational level | ||||
| Low | 319 (22.9) | 23 (27.1) | 295 (22.6) | 0.62 * |
| Intermediate | 569 (40.8) | 32 (37.6) | 536 (41.1) | |
| High | 506 (36.3) | 30 (35.3) | 474 (36.3) | |
| Ethnicity | ||||
| Western | 1,284 (91.8) | 81 (95.3) | 1,200 (91.6) | 0.30 * |
| Non-Western | 115 (8.2) | 4 (4.7) | 110 (8.4) | |
| PMT constructs | Mean (SD) | Mean (SD) | Mean (SD) | |
| Self-efficacy (−2, +2) | 1.49 (1.0) | 0.57 (1.0) | 1.56 (0.9) | <0.0001 ** |
| Response efficacy (−2, +2) | 1.74 (0.5) | 1.16 (0.7) | 1.77 (0.5) | <0.0001 ** |
| Vulnerability (−2, +2) | −1.42 (0.9) | −1.21 (0.8) | −1.43 (0.9) | 0.02 ** |
| Severity (−2, +2) | 1.39 (0.9) | 0.92 (1.0) | 1.42 (0.9) | <0.0001 ** |
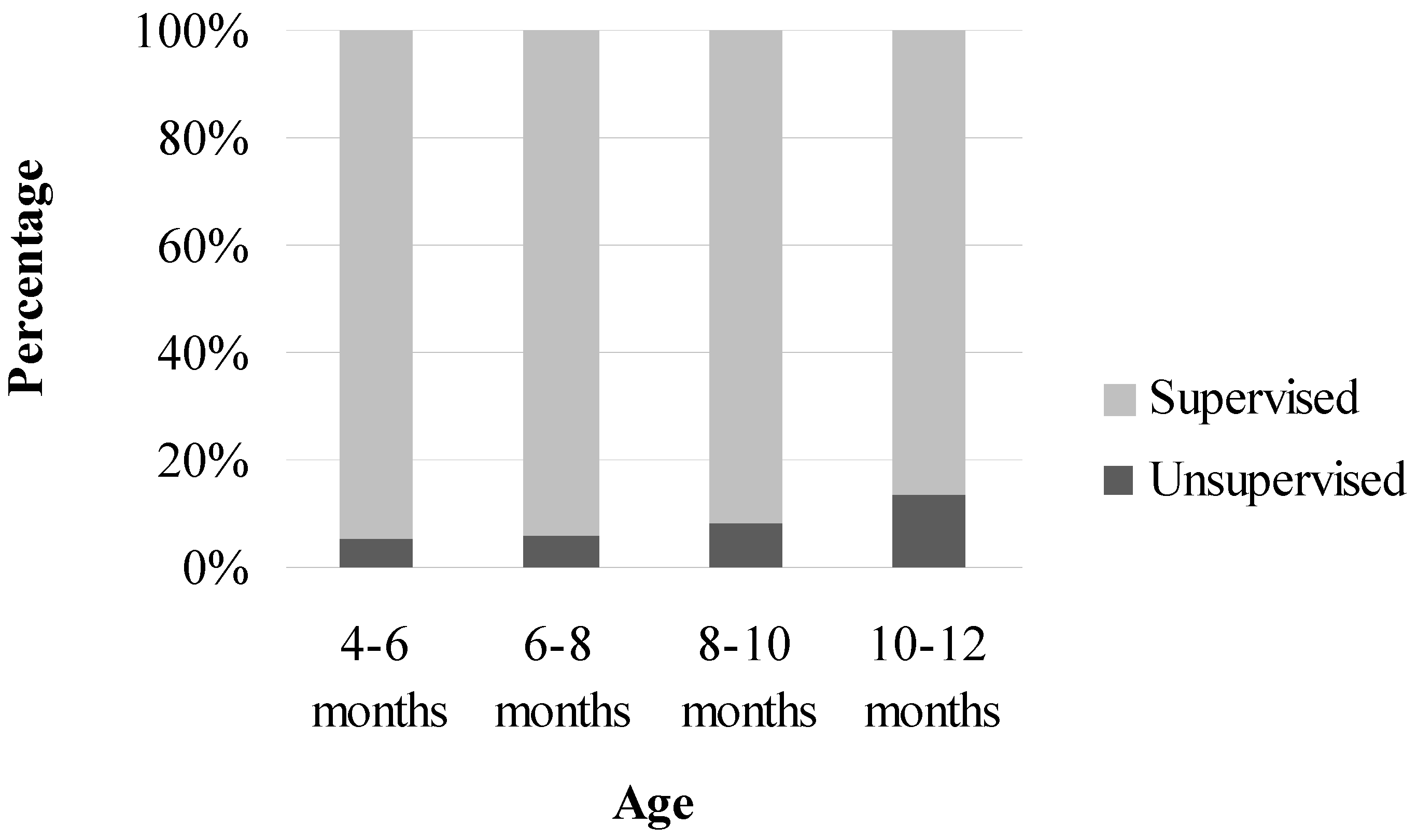
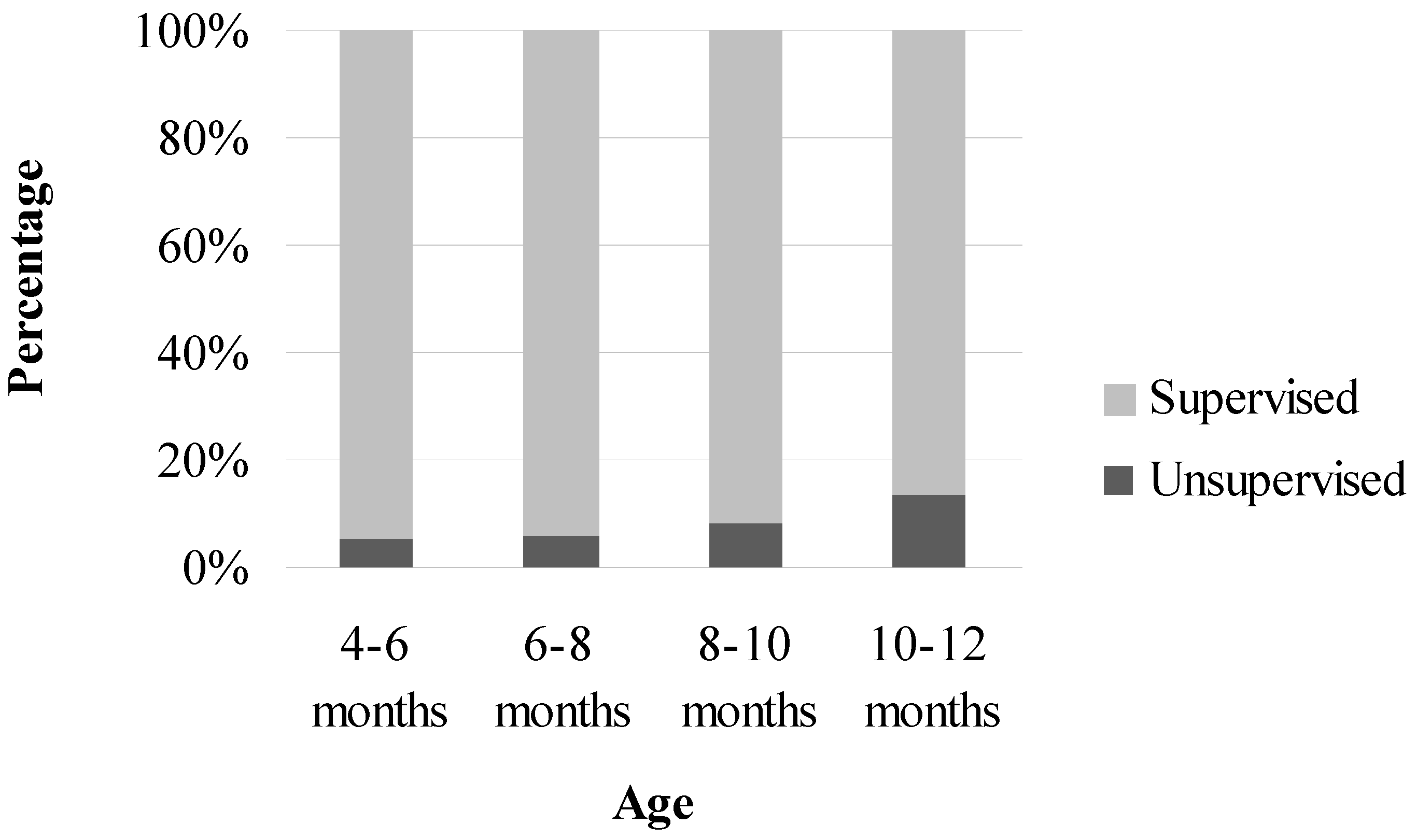
3.2. Correlates of Leaving the Infant Unsupervised in the Bathtub
| Infant left unsupervised in the bathtub | ||||||
|---|---|---|---|---|---|---|
| Model 1 OR (95%CI) | p value | Model 2 OR (95%CI) | p value | Model 3 OR (95%CI) | p value | |
| Demographic variables | ||||||
| Infants | ||||||
| Age in months | 1.29 (1.06–1.57) | 0.01 | 1.29 (1.06–1.57) | 0.01 | 1.24 (1.00–1.54) | 0.05 |
| Girl | 1.27 (0.82–1.97) | 0.28 | - | - | - | - |
| Infant can crawl | 0.81 (0.52–1.26) | 0.35 | - | - | - | - |
| Family | ||||||
| One-parent family | 1.30 (0.39–4.30) | 0.67 | - | - | - | - |
| First-time parent | 0.67 (0.43–1.05) | 0.08 | - | - | 0.59 (0.36–0.97) | 0.04 |
| Mother | ||||||
| Employment | ||||||
| Paid job fulltime | 1.00 | - | - | - | - | - |
| Paid job part time | 0.78 (0.35–1.76) | 0.55 | - | - | - | - |
| No paid job | 0.61 (0.23–1.59) | 0.31 | - | - | - | - |
| Educational level | ||||||
| Low | 1.00 | - | - | - | - | - |
| Intermediate | 1.32 (0.66–2.62) | 0.44 | - | - | - | - |
| High | 1.50 (0.75–2.98) | 0.25 | - | - | - | - |
| Non-Western migrant | 1.14 (0.54–2.41) | 0.74 | - | - | - | - |
| Father | ||||||
| Employment | ||||||
| Paid job fulltime | 1.00 | - | - | - | - | - |
| Paid job part time | 0.70 (0.30–1.65) | 0.42 | - | - | - | - |
| No paid job | 1.23 (0.43–3.50) | 0.70 | - | - | - | - |
| Educational level | ||||||
| Low | 1.00 | - | - | - | - | - |
| Intermediate | 0.77 (0.44–1.33) | 0.35 | - | - | - | - |
| High | 0.81 (0.46–1.42) | 0.47 | - | - | - | - |
| Non-Western migrant | 0.54 (0.19–1.50) | 0.24 | - | - | 0.18 (0.05–0.63) | 0.01 |
| PMT constructs a | ||||||
| Self-efficacy (−2, +2) | 0.53 (0.45–0.62) | <0.001 | - | - | 0.57 (0.47–0.69) | <0.001 |
| Response efficacy (−2, +2) | 0.26 (0.19–0.35) | <0.001 | - | - | 0.34 (0.24–0.48) | <0.001 |
| Vulnerability (−2, +2) | 1.30 (1.05–1.61) | 0.02 | - | - | - | - |
| Severity (−2, +2) | 0.63 (0.52–0.76) | <0.001 | - | - | 0.74 (0.58–0.93) | 0.01 |
3.3. Discussion
4. Conclusions
Acknowledgments
Conflict of Interest
References
- Peden, M.; Oyegbite, K.; Ozanne-Smith, J.; Hyder, A.A.; Branche, C.; Fazlur Rahman, A.K.M.; Rivara, F.; Bartolomeos, K. World Report on Child Injury Prevention; WHO: Geneva, Switzerland, 2008. [Google Scholar]
- van Beeck, E.F.; Branche, C.M.; Szpilman, D.; Modell, J.H.; Bierens, J.J. A new definition of drowning: Towards documentation and prevention of a global public health problem. Bull. World Health Organ. 2005, 83, 853–856. [Google Scholar]
- Lee, L.K.; Thompson, K.M. Parental survey of beliefs and practices about bathing and water safety and their children: Guidance for drowning prevention. Accid Anal. Prev. 2007, 39, 58–62. [Google Scholar] [CrossRef]
- Quan, L.; Cummings, P. Characteristics of drowning by different age groups. Inj. Prev. 2003, 9, 163–168. [Google Scholar] [CrossRef]
- Byard, R.W.; Lipsett, J. Drowning deaths in toddlers and preambulatory children in South Australia. Am. J. Forensic. Med. Pathol. 1999, 20, 328–332. [Google Scholar] [CrossRef]
- Sibert, J.; John, N.; Jenkins, D.; Mann, M.; Sumner, V.; Kemp, A.; Cornall, P. Drowning of babies in bath seats: Do they provide false reassurance? Child Care Health Dev. 2005, 31, 255–259. [Google Scholar] [CrossRef]
- Porter, T.R.; Crane, L.A.; Dickinson, L.M.; Gannon, J.; Drisko, J.; DiGuiseppi, C. Parent opinions about the appropriate ages at which adult supervision is unnecessary for bathing, street crossing, and bicycling. Arch. Pediatr. Adolesc. Med. 2007, 161, 656–662. [Google Scholar] [CrossRef]
- Shannon, A.; Brashaw, B.; Lewis, J.; Feldman, W. Nonfatal childhood injuries: A survey at the Children’s Hospital of Eastern Ontario. Can. Med. Assn. J. 1992, 146, 361–365. [Google Scholar]
- Sinclair, K.A.; Morrongiello, B.A.; Dowd, M.D. Parenting behaviors and attitudes about supervision among parents of acutely poisoned children. Ambul. Pediatr. 2008, 8, 135–138. [Google Scholar] [CrossRef]
- Somers, G.R.; Chiasson, D.A.; Smith, C.R. Pediatric drowning: A 20-year review of autopsied cases: III. Bathtub drownings. Am. J. Forensic. Med. Pathol. 2006, 27, 113–116. [Google Scholar] [CrossRef]
- Petrass, L.A.; Blitvich, J.D.; Finch, C.F. Lack of caregiver supervision: A contributing factor in Australian unintentional child drowning deaths, 2000–2009. Med. J. Aust. 2011, 194, 228–231. [Google Scholar]
- Simon, H.K.; Tamura, T.; Colton, K. Reported level of supervision of young children while in the bathtub. Ambul. Pediatr. 2003, 3, 106–108. [Google Scholar] [CrossRef]
- Turner, J. Prevention of drowning in infants and children. Dimens. Crit. Care Nurs. 2004, 23, 191–193. [Google Scholar] [CrossRef]
- Rogers, R. Protection Motivation Theorie; Plenum Press: New York, NY, USA, 1997. [Google Scholar]
- van Beelen, M.E.; Beirens, T.M.; Struijk, M.K.; den Hertog, P.; Oenema, A.; van Beeck, E.F.; Raat, H. “BeSAFE”, effect-evaluation of internet-based, tailored safety information combined with personal counselling on parents’ child safety behaviours: Study design of a randomized controlled trial. BMC Public Health 2010, 10, 466. [Google Scholar] [CrossRef]
- Beirens, T.M.J.; Brug, J.; van Beeck, E.F.; Dekker, R.; den Hertog, P.; Raat, H. Assessing psychosocial correlates of parental safety behaviour using Protection Motivation Theory: Stair gate presence and use among parents of toddlers. Health Educ. Res. 2008, 23, 723–731. [Google Scholar]
- Beirens, T.M.J.; Brug, J.; van Beeck, E.F.; Dekker, R.; Juttmann, R.E.; Raat, H. Presence and use of stair gates in homes with toddlers (11–18 months old). Accid. Anal. Prevent. 2007, 39, 964–968. [Google Scholar] [CrossRef]
- Beirens, T.M.J.; van Beeck, E.F.; Dekker, R.; Brug, J.; Raat, H. Unsafe storage of poisons in homes with toddlers. Accid. Anal. Prevent. 2006, 38, 772–776. [Google Scholar] [CrossRef]
- Statistics Netherlands. Available online: http://statline.cbs.nl/StatWeb/publication/?VW=T&DM=SLNL&PA=71102ned&D1=a&D2=0&D3=(l-11)-l&HD=080901-1401 (accessed on 16 May 2012).
- Committee on Injury, Violence, and Poison Prevention. Prevention of drowning. Pediatrics 2010, 126, e253–e262. [CrossRef]
- Byard, R.; de Koning, C.; Blackbourne, B.; Nadeau, J.; Krous, H.F. Shared bathing and drowning in infants and young children. J. Paediatr. Child Health 2001, 37, 542–544. [Google Scholar] [CrossRef]
- Byard, R.W.; Donald, T. Infant bath seats, drowning and near-drowning. J. Paediatr. Child Health 2004, 40, 305–307. [Google Scholar] [CrossRef]
© 2013 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Van Beelen, M.E.J.; Van Beeck, E.F.; Den Hertog, P.; Beirens, T.M.J.; Raat, H. Correlates of Unsupervised Bathing of Infants: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2013, 10, 856-866. https://doi.org/10.3390/ijerph10030856
Van Beelen MEJ, Van Beeck EF, Den Hertog P, Beirens TMJ, Raat H. Correlates of Unsupervised Bathing of Infants: A Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2013; 10(3):856-866. https://doi.org/10.3390/ijerph10030856
Chicago/Turabian StyleVan Beelen, Mirjam E. J., Eduard F. Van Beeck, Paul Den Hertog, Tinneke M. J. Beirens, and Hein Raat. 2013. "Correlates of Unsupervised Bathing of Infants: A Cross-Sectional Study" International Journal of Environmental Research and Public Health 10, no. 3: 856-866. https://doi.org/10.3390/ijerph10030856
APA StyleVan Beelen, M. E. J., Van Beeck, E. F., Den Hertog, P., Beirens, T. M. J., & Raat, H. (2013). Correlates of Unsupervised Bathing of Infants: A Cross-Sectional Study. International Journal of Environmental Research and Public Health, 10(3), 856-866. https://doi.org/10.3390/ijerph10030856