4.1. Data Collection
The results of this study rely on availability of smoking data. Among miners, particularly in the S sub-cohort, smoking data collection started in the mid-1990s, when about one-fourth of the cohort members were still alive. The investigation on smoking habits started firstly among cases and it was mostly based on medical files and information from relatives. The controls were randomly selected for each case with smoking data and data on controls were obtained in person if selected miners were alive and from relatives if selected controls deceased. This depended on the availability of addresses, which was more complicated for subjects who died long time ago. Therefore, earlier cases had less controls with smoking data than later cases. In the N and L sub-cohorts, smoking data were routinely collected during periodic medical checks in the 1970s and 1980s, when miners were asked to fill a simple questionnaire on number of cigarettes smoked per day and the year of cessation. These data were available for about 80% subjects. The controls selected in the N and L studies were asked again on their current smoking habits. Numbers of ex-smokers in the present study were generally low as the smoking status was considered at the index year, which was often before they stopped smoking.
4.2. Strengths and Limitations
The main strength of the present study is relatively low uncertainty of exposure estimates resulting from extensive measurements since nearly the beginning of the occupational study. The three occupational sub-studies are naturally different, namely as for the level of exposures and exposure duration. Exposure estimates in the N study are more precise then in the S study. This differences, however, is not reflected in the risk coefficients. The ERR/WLM coefficients in the multiplicative risk model—0.012 (S), 0.016 (N), and 0.012 (L) do not substantially differ (p = 0.97).
Limitations are in exposure data in the residential study. For obvious reasons, measurements of exposure in each year of relevant previous exposure period are not possible. Measurements in the present study were based on one-year measurements of radon, which are more reliable than short term measurements conducted for several months in most residential studies [
16]. The effect from radon in residential studies is influenced by these uncertainties. The correction for uncertainty in the present study is planned in future, when the study of repeated measurements in residential study will be completed.
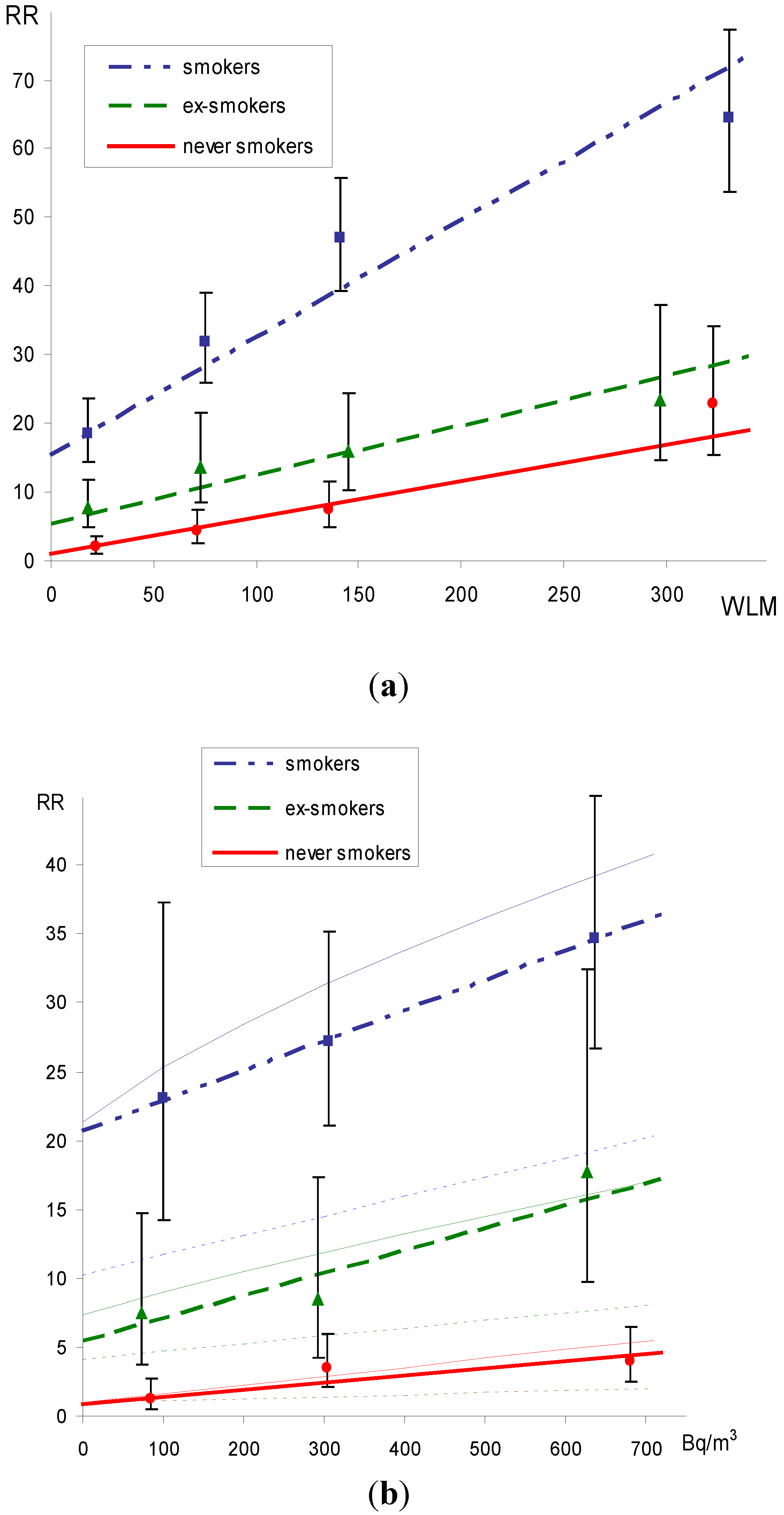
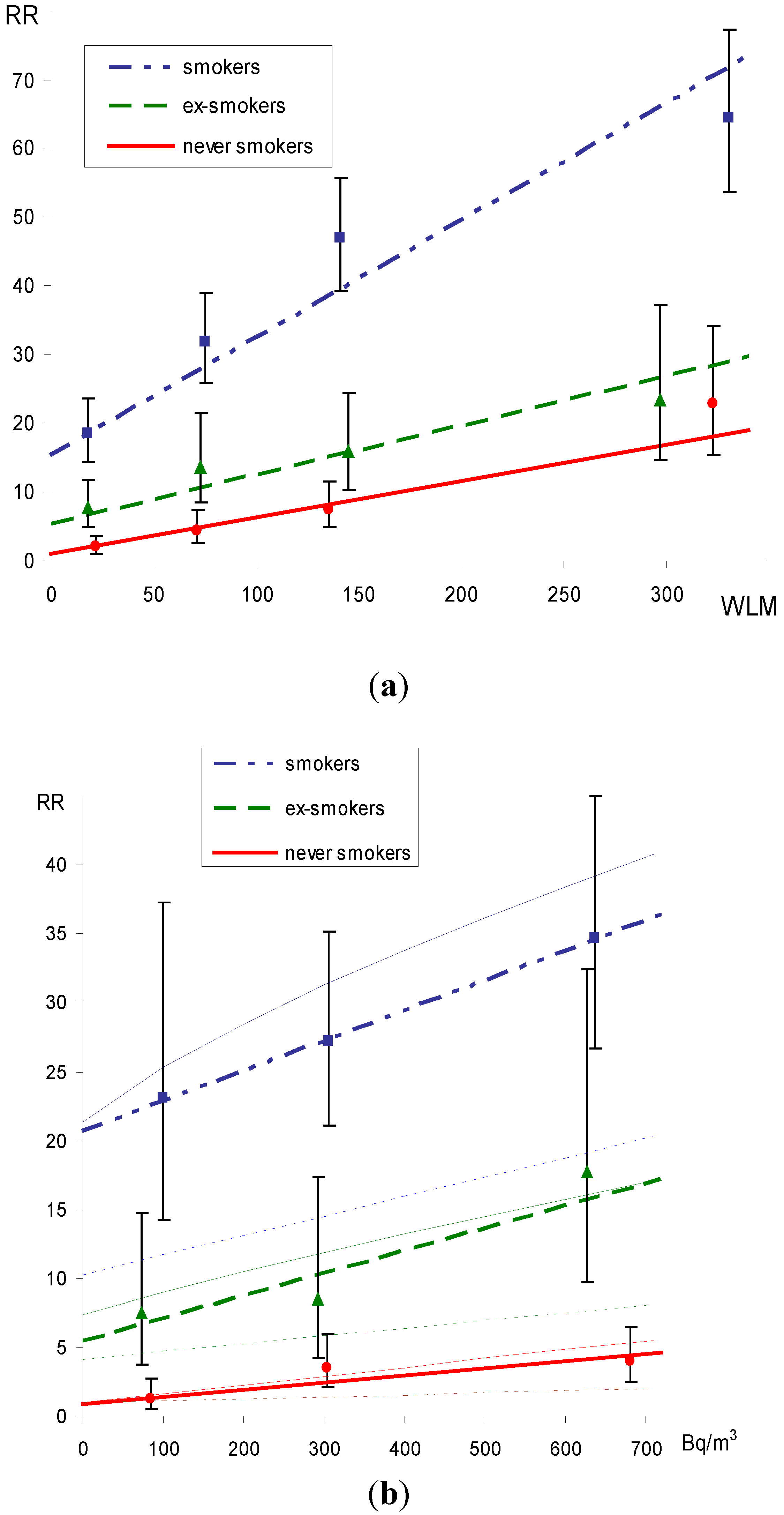
Limitations of the studies are in smoking data. In the occupational study, these data are based on personal interview or medical files, 60% and 63% among cases and controls, respectively. In the residential study of Mid-Bohemia Pluton, smoking data reported in person were 46% and 51% among cases and controls, whereas in the Bulovka study all smoking data were obtained in person. Smoking data not available in person or from medical files were obtained from relatives (mostly spouse, sometimes children). Generally, data obtained from relatives may not be quite exact as for the amount of cigarettes and years of quitting, but it is believed that the three smoking categories used in the models analyses are reliable. The estimated relative risks from smoking (at zero exposure) in the geometric mixture model (1, 6.0 18.8 and 1, 7.3, 21.4 for never-, ex-, and other smokers in the present occupational and residential studies) correspond to usual figures reported by other epidemiological studies (1, 7.5, 23.9) as summarized by Simonato
et al. [
17]. The evaluation of uncertainties in smoking data is planned in future, together with the uncertainties of exposure data.
Another limitation of the present study is a lack of smoking data among subjects who died long time ago as availability of relatives and their addresses was limited. For instance, for 102 cases who died before 1960, there was only 27 with smoking information. However, for later periods the coverage was at least 80%. The crude estimate of ERR/WLM in the entire cohort study was 0.010 (90%CI: 0.007–0.013) which is close to the value 0.013 (90%CI: 0.007–0.019), when smoking was ignored (
Table 4). In the residential study, smoking data were available for 98% cases.
The evidence of an effect from residential radon is generally more difficult because of lower exposure and uncertainties in exposure estimates. The results of the present studies are in line with other residential studies. The excess relative risk per unit exposure (100 Bq/m
3) in the present study, when smoking was adjusted for 0.14 is between the values 0.09 and 0.16 estimated in the European pooled study [
16].
4.3. Comparison of Risk Coefficients in Relative Risk Models
The increased relative risk from radon exposure among non-smokers was consistently observed in the present study in all models. Seemingly surprising observations of higher excess relative risks per unit exposure in non-smokers do not mean that the absolute risks are higher because the baseline lung cancer risks are by about one order of magnitude higher.
The relative risk coefficients (both ERR/WLM and ERR/Bq·m−3) when smoking is ignored is not substantially different from the one when smoking is adjusted for. The adjusted ERR/WLM in the occupational study is 0.014 and this risk coefficient is similar to that among smokers (0.010) as most cases are smokers. Similar results are seen in the present residential study. The ERR/Bq·m−3 was 0.14 among ever smokers and in the entire study when smoking was adjusted for.
The confounding effect of smoking in residential studies reported by Darby
et al [
16] generally reflects the association between radon exposure and smoking,
i.e., higher prevalence of smokers in low exposure groups, most likely because of the socio-economic status and type of housing. In the present Czech study, this association is relatively weak. In the occupational studies, the confounding effect by smoking was not observed in the present study, similarly as in other studies of uranium miners [
18].
The model of relative risk with time since exposure specific ERR/WLM model (2) substantially improved the fit (p < 0.001) and deepened differences in smoking categories. In comparison to model (1), where the ratio of ERR/ WLM in never smokers and smokers was 5, this ratio of ERR/WLM corresponding to exposure window 5–19 was 9 [
10], while the ERR/WLM from more distant exposures was substantially lower.
4.4. Comparison to Other Studies
The interaction between exposure to radon and smoking in six studies of miners were investigated by Lubin
et al. and reported in BEIR VI [
1]. Results for separate studies were consistent with a model intermediate between additive and multiplicative (mixing parameter between 0 and 0.7). Because of small numbers of cases particularly among non-smokers (64 cases), the additive and multiplicative models were not significantly different. Better fits were reported for the additive model in the China and Newfoundland studies, whereas better fits were observed for the multiplicative model in the Colorado, New Mexico and Sweden studies [
1]. The joint analysis of all six studies resulted in a three times higher estimate of ERR/WLM (0.0103, 95%CI 0.002–0.057) among never smokers than among smokers (0.0034, 95%CI 0.0008–0.0170) [
1]. In comparison to more different estimates in the present study, the uncertainty of estimates in the BEIR VI report is much higher despite large numbers of lung cancers (1,442 cases) observed in the joint study. Results by Placek
et al. [
6] based on follow-up up to 1990 of the
N and
L Czech cohorts found four times higher risk coefficients among non-smokers.
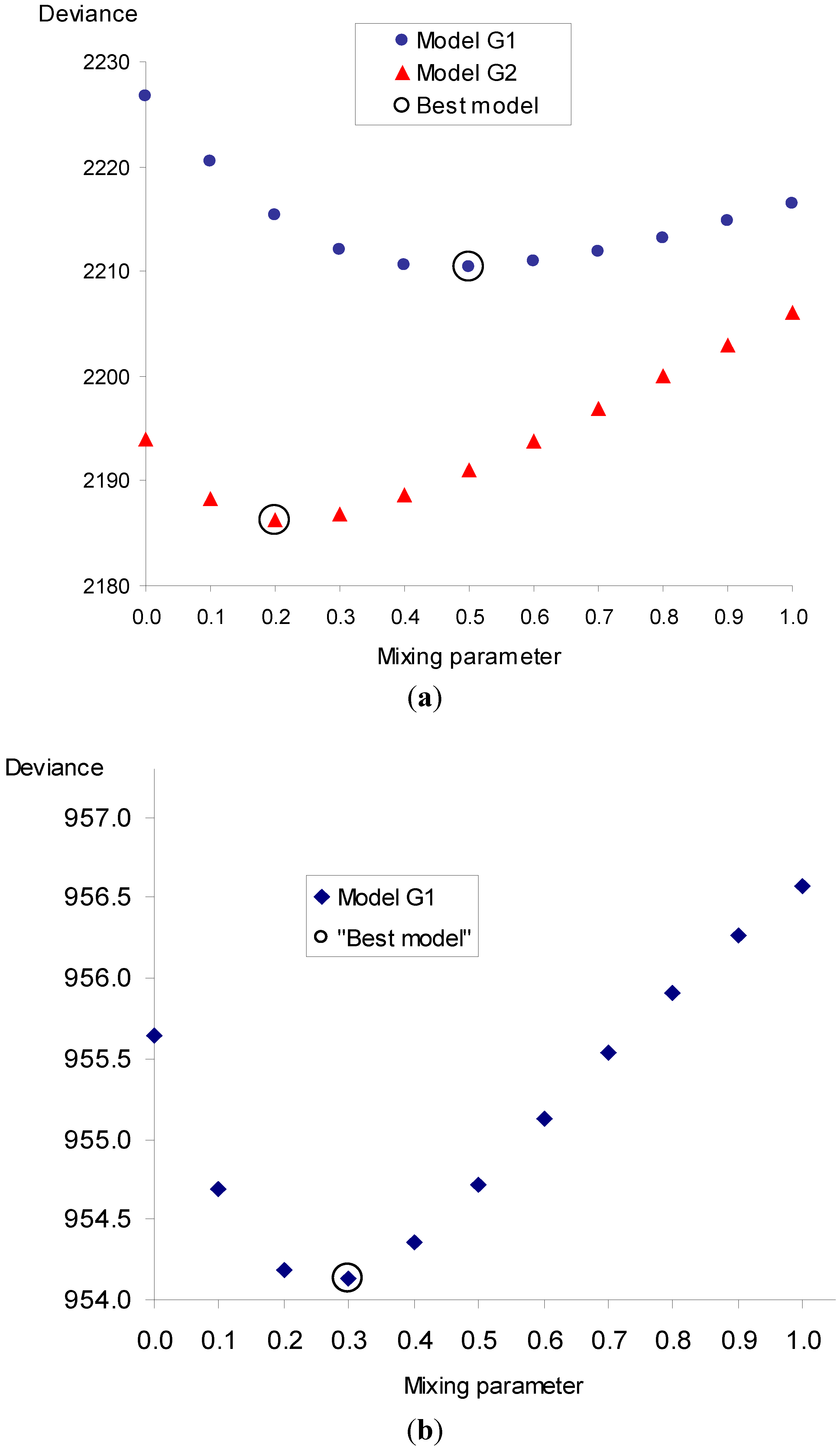
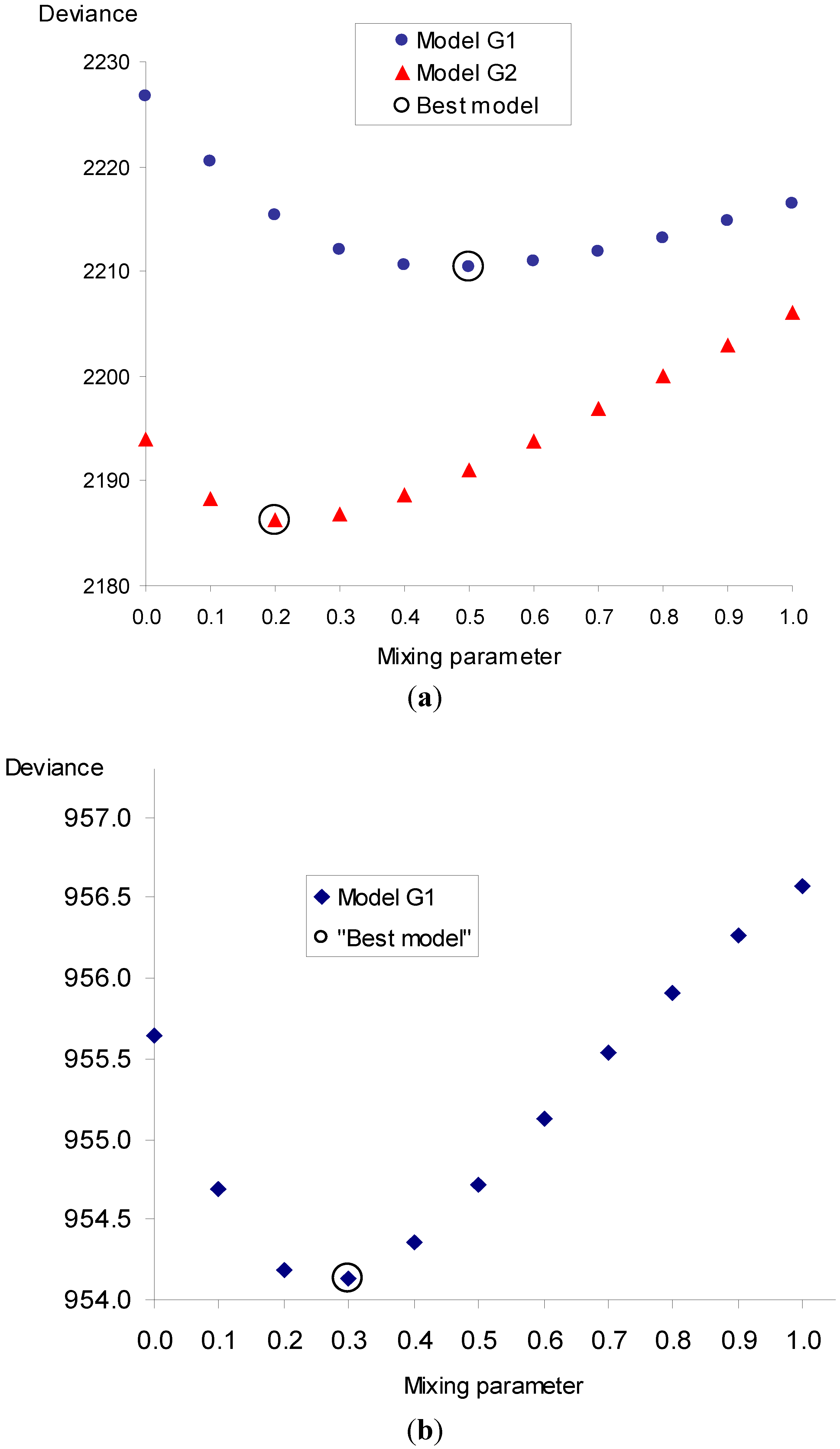
In the present occupational study, the best estimate of mixing parameter (θ = 0.5, see
Figure 2, model G1) was between the additive and multiplicative model in relation to cumulated exposure. Virtually the same findings (θ = 0.5) were reported by Leuraud in a large joint study of uranium miners (1,046 cases, 2,492 controls) in relation to cumulated exposure [
18]. The mixing parameter in the present study, however, was substantially shifted (θ = 0.2) when time since exposure modifying factor was used. This approach could not been used in the residential study as the statistical power for two exposure windows is limited by smaller numbers of cases and substantially lower exposures in comparison to the occupational study. In the residential study, the best mixing parameter (θ = 0.3) is, however, close to the parameter estimated from the occupational study.
So far, in residential studies, the geometric mixture approach has not been used. The different estimates in non-smokers and smokers in the present residential study are in line with observations in other residential studies, where the relative risk per unit exposure is 2–3 times higher. For instance, in the joint European residential study [
16] 2.2 times, in the joint North American residential study [
19] 1.8 times, and in the joint China study [
19] 2.6 times. These differences, however, were not statistically significant because of relatively low exposures and high uncertainties of exposures. The issue of additive and multiplicative effect of radon and smoking was recently investigated by Barros-Dios
et al. [
20]. They found an additive interaction when individuals were classified as exposed (>50 Bq·m
−3) or non-exposed to residential radon and smokers in never- or ever-smokers. These results are supported by the present residential study. In comparison to never-smokers, the relative risk (OR) in smokers is 27.5 for exposures <200 Bq·m
−3, whereas for exposure >200 Bq·m
−3 the relative risk is only 8.0 .
Generally, the assessment of interactions between risk factors requires studies of higher statistical power than the evaluation of single risk factors. The strength of the study generally depends on the number of cases and on the levels of exposure. In studies of lung cancer risk from radon and smoking, the substantial issue is the level of radon exposure and its reliability.
In the BEIR VI report [
1], potential reasons for interactions of smoking and radon exposure are given. Some of them include the impact of smoking on exposure, others exposure–dose relation and others dose-response relation in smokers and non-smokers as was reported by Baias
et al. [
21]. Although the study does not provide evidence relevant to each of the reasons, the probable explanations include differences in lung morphometry of target cells, thickness of the mucous layer and mucociliary clearance between smokers and non-smokers.









{kind=link}
{kind=link}
{kind=link}
{kind=link}