An Intuitive Approach to Understanding the Attributable Fraction of Disease Due to a Risk Factor: The Case of Smoking


Abstract
:1. Introduction
1.1. Attributable Fraction
1.2. Original Formula for the Attributable Fraction

- p = the underlying prevalence of the risk factor in the population (for example, the prevalence of smoking in the population), and
- RR (Relative Risk): Risk of contracting a disease in an exposed population (e.g., smokers) divided by the risk of contracting the disease in an unexposed population (e.g., nonsmokers)
2. Materials and Method
3. Results
3.1. Proposed Formula for the Attributable Fraction

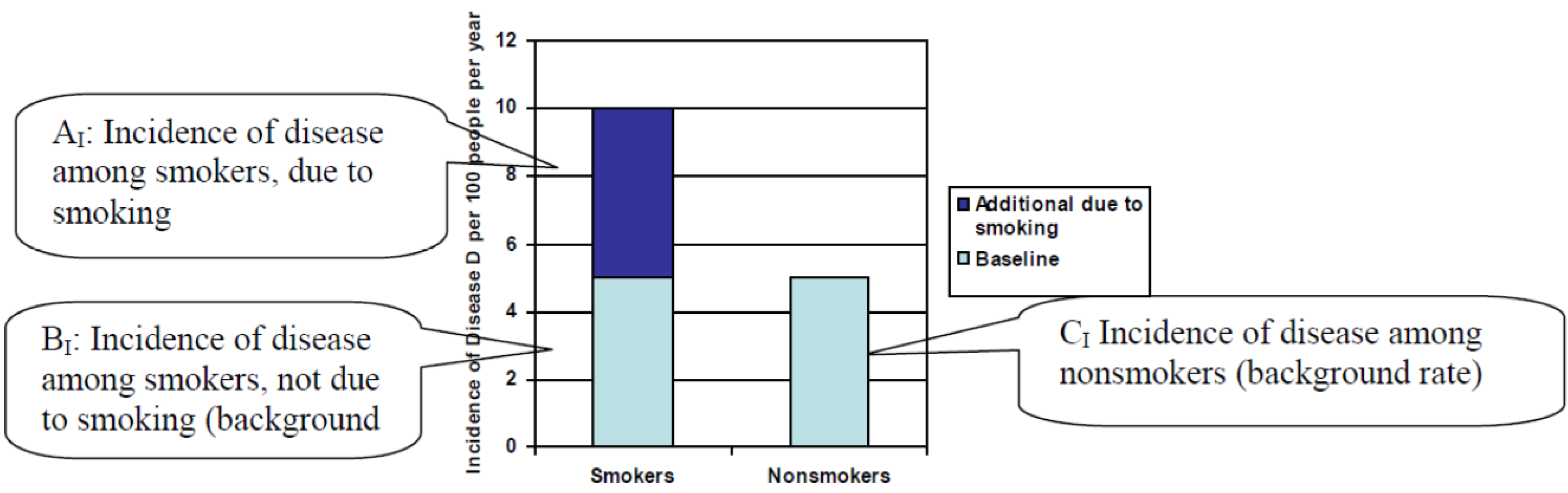
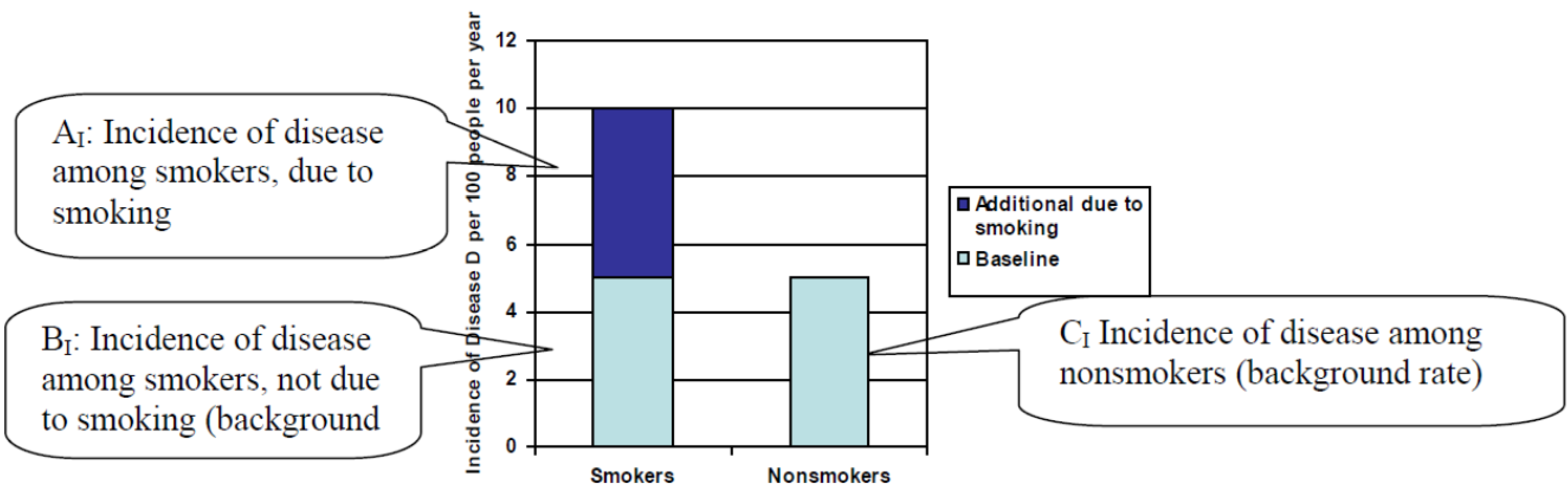
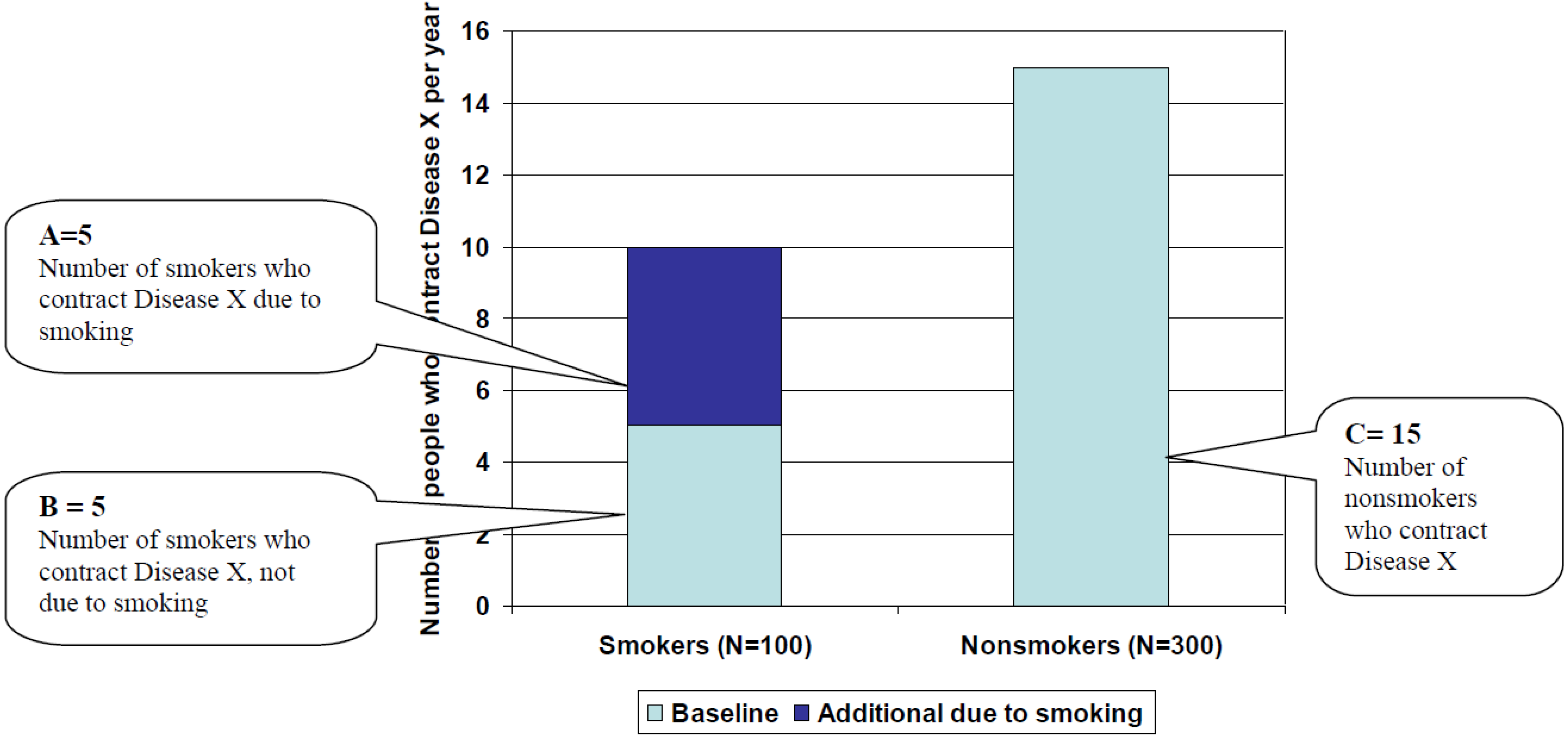
- A = Number of smokers in the population who contract a particular disease, Disease X, due to their smoking habit
- B = Number of smokers in the population who contract a particular disease, Disease X, but not due to their smoking habit
- C = Number of nonsmokers in the population who contract Disease X.
3.2. Graphical Illustration of Proposed Formula
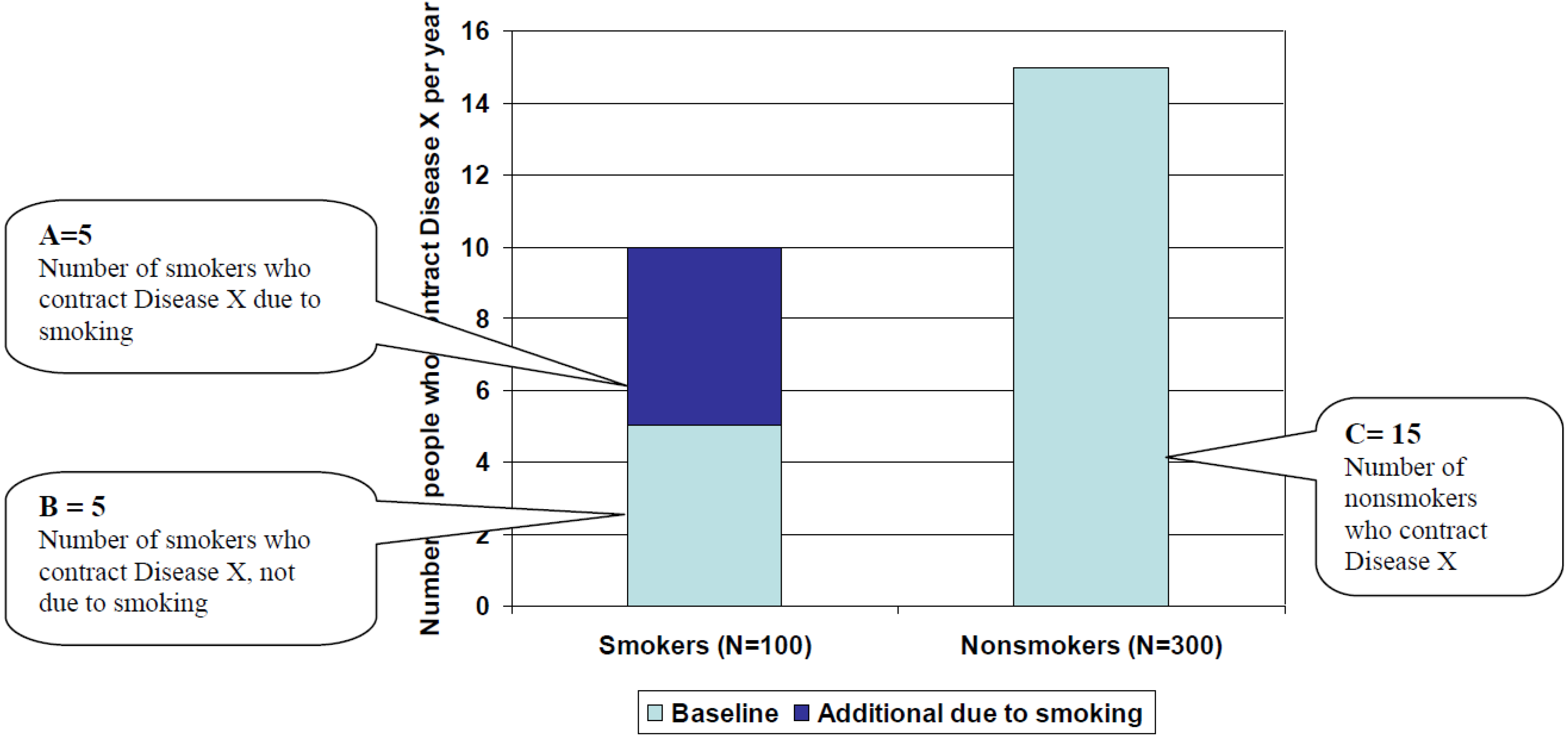 . As pictured in Figure 2, AF = 5/25 = 20%.
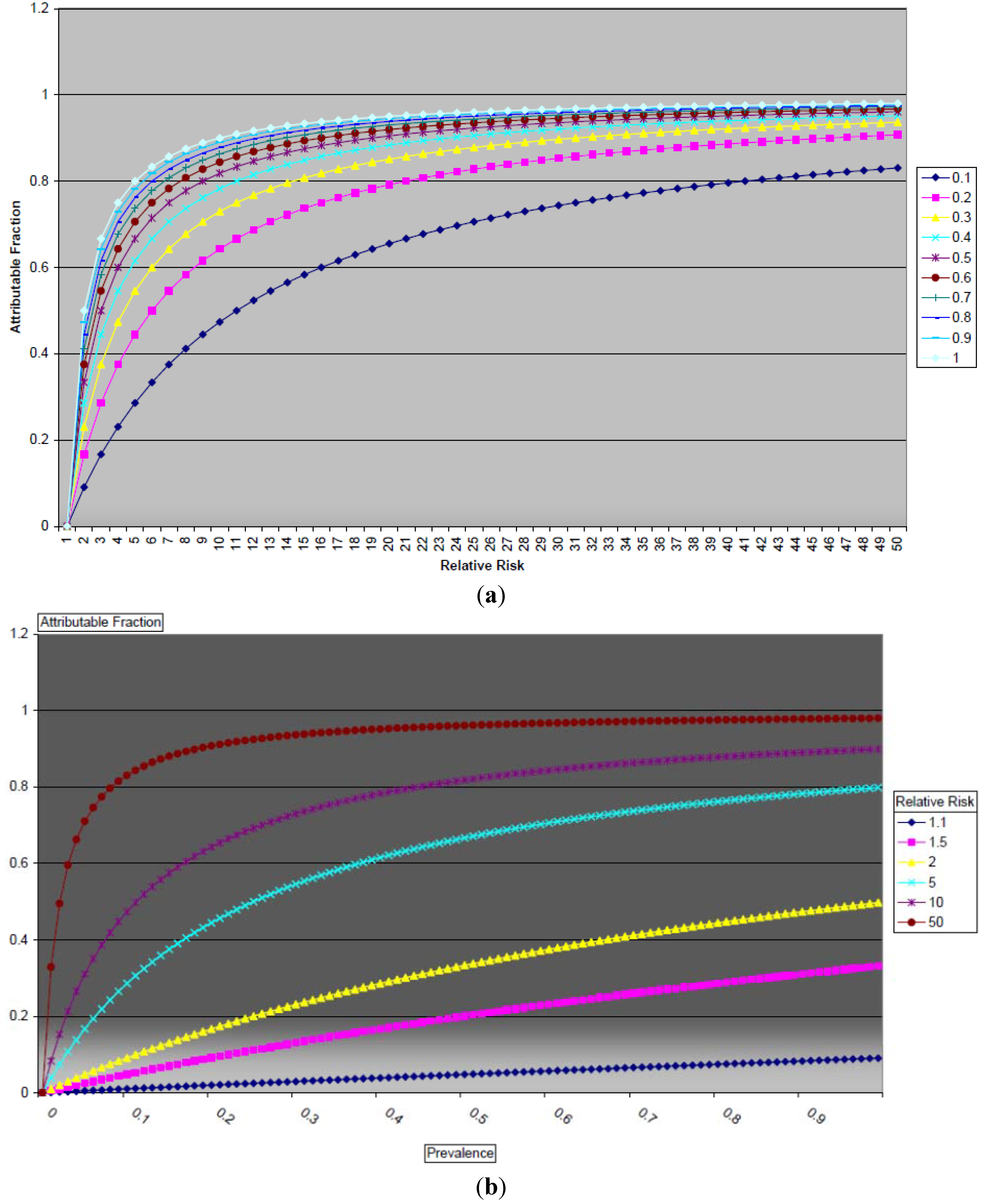
. As pictured in Figure 2, AF = 5/25 = 20%.3.3. Relationship between the Attributable Fraction, the Relative Risk, and the Proportion of Smokers in the Population
3.4. Illustrative Examples

{kind=link}
{kind=link}
{kind=link}
| Disease | Incidence among nonsmokers per 1,000 men/year | Incidence among smokers (15–24 cigarettes per day) per 1,000 men/year | Assumed Relative Risk of mortality among smokers (15–24 cigarettes per day) | Male Smoking Prevalence | A | B | C | Hypothetical Attributable Fraction |
|---|---|---|---|---|---|---|---|---|
| Lung cancer | 0.17 | 2.33 | 13.7 | 9.9% 1 | 214 | 17 | 153 | 55.7% |
| 0.17 | 2.33 | 13.7 | 19.0% 2 | 410 | 32 | 138 | 70.7% | |
| 0.17 | 2.33 | 13.7 | 44.3% 3 | 957 | 75 | 95 | 84.9% | |
| 0.17 | 2.33 | 13.7 | 63.6% 4 | 1,374 | 108 | 62 | 89.0% | |
| Heart disease | 6.19 | 10.07 | 1..6 | 9.9% 1 | 384 | 613 | 5,577 | 5.8% |
| 6.19 | 10.07 | 1.6 | 19.0% 2 | 737 | 1,176 | 5,014 | 10.6% | |
| 6.19 | 10.07 | 1.6 | 44.3% 3 | 1,719 | 2,742 | 3,448 | 21.7% | |
| 6.19 | 10.07 | 1.6 | 63.6% 4 | 2,468 | 3,937 | 2,253 | 28.5% |
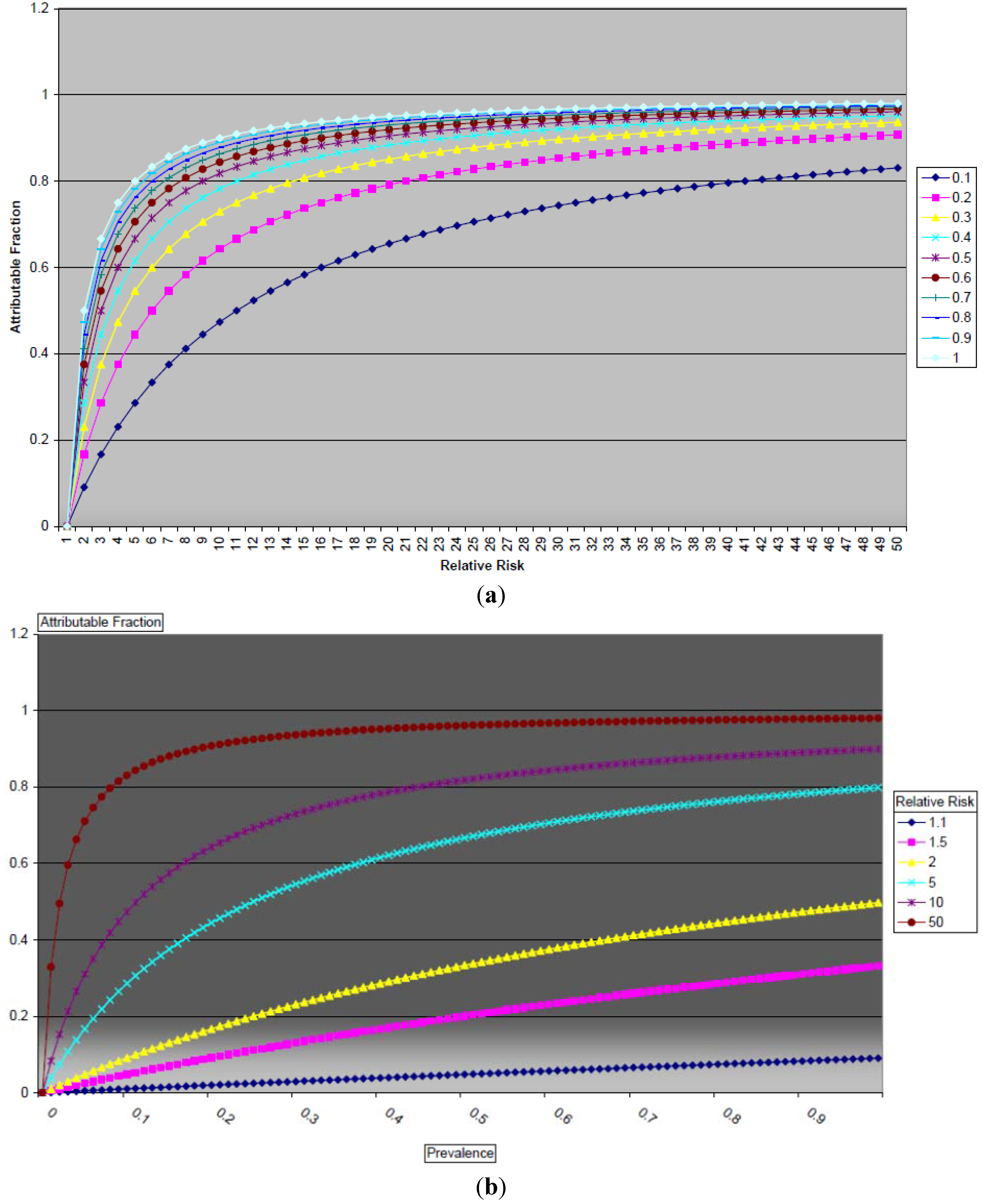
3.5. Mathematical Relationships between the Attributable Fraction, the Relative Risk, and the Prevalence of Smoking
4. Discussion
5. Conclusions
List of abbreviations
| AF | Attributable Fraction |
| CDC | US Centers for Disease Control |
| SAMMEC | Smoking attributable mortality, morbidity, and economic costs |
| p | Underlying prevalence of a risk factor in a population |
| RR | Relative Risk: Risk of contracting a disease in an exposed population divided by the risk of contracting the disease in an unexposed population |
| A | Number of smokers who contract a particular disease—“Disease X”—due to their smoking habit |
| B | Number of smokers who contract a disease, unrelated to their smoking habit |
| C | Number of nonsmokers who contract a given disease (unrelated to smoking) |
Acknowledgments
Conflict of Interest
References
- How Tobacco Smoke Causes Disease: The Biology and Behavioral Basis for Smoking-Attributable Disease: A Report of the Surgeon General; US Department of Health & Human Services: Washington, DC, USA, 2010.
- WHO Report on the Global Tobacco Epidemic, 2008; WHO: Geneva, Switzerland, 2008.
- Yach, D.; Bialous, S. Junking science to promote tobacco. Am. J. Public Health 2001, 91, 1745–1748. [Google Scholar]
- The Health Consequences of Smoking: A Report of the Surgeon General; US Department of Health & Human Services: Washington, DC, USA, 2004.
- Doll, R.; Peto, R.; Boreham, J.; Sutherland, I. Mortality in relation to smoking: 50 years’ observations on male British doctors. BMJ 2004, 328. [Google Scholar] [CrossRef]
- Stellman, S.; Garfinkel, L. Smoking habits and tar levels in a new American Cancer Society prospective study of 1.2 million men and women. J. Natl. Cancer Inst. 1986, 76, 1057–1063. [Google Scholar]
- Rockhill, B.; Newman, B.; Weinberg, C. Use and misuse of population attributable fractions. Am. J. Public Health 1998, 88, 15–19. [Google Scholar] [CrossRef]
- Levin, M. The occurrence of lung cancer in man. Acta Unio Int. Contra Cancrum. 1953, 9, 531–541. [Google Scholar]
- Gordis, L. Epidemiology, 4th ed.; Saunders Elsevier: Philadelphia, PA, USA, 2009. [Google Scholar]
- Northridge, M. Public health methods—Attributable risk as a link between causality and public health action. Am. J. Public Health 1995, 85, 1202–1204. [Google Scholar] [CrossRef]
- Shafey, O.; Eriksen, M.; Ross, H.; Mackay, J. The Tobacco Atlas, 3rd ed.; American Cancer Society: Atlanta, GA, USA, 2009. [Google Scholar]
- Tversky, A.; Kahneman, D. Judgment under uncertainty: Heuristics and biases. Science 1974, 185, 1124–1131. [Google Scholar]
- MacMahon, B.; Pugh, T. Epidemiology: Principles and Methods; Little: Boston, MA, USA, 1970. [Google Scholar]
- Bruzzi, P.; Green, S.B.; Byar, D.P.; Brinton, L.A.; Schairer, C. Estimating the population attributable risk for multiple risk factors using case-control data. Am. J. Epidemiol. 1985, 122, 904–914. [Google Scholar]
- McNulty, J.; Hopkins, D.; Grant-Worley, J.; Baron, R.; Fleming, D. A comparison of alternative systems for measuring smoking-attributable deaths in Oregon, USA. Tob. Cont. 1994, 3, 115–119. [Google Scholar] [CrossRef]
- Peto, R.; Lopez, A.D.; Boreham, J.; Thun, M.; Heath, C., Jr. Mortality from tobacco in developed countries: Indirect estimation from national vital statistics. Lancet 1992, 339, 1268–1278. [Google Scholar] [CrossRef]
- Benichou, J. A review of adjusted estimators of attributable risk. Stat. Methods Med. Res. 2001, 10, 195–216. [Google Scholar] [CrossRef]
- Steenland, K.; Armstrong, B. An overview of methods for calculating the burden of disease due to specific risk factors. Epidemiology 2006, 17, 512–519. [Google Scholar] [CrossRef]
- Miettinen, O. Proportion of disease caused or prevented by a given exposure, trait or intervention. Am. J. Epidemiol. 1974, 99, 325–332. [Google Scholar]
- Greenland, S. Bias in methods for deriving standardized morbidity ratio and attributable fraction estimates. Stat. Med. 1984, 3, 131–141. [Google Scholar] [CrossRef]
- Murray, C.J.; Lopez, A. Evidence-based health policy—Lessons from the global burden of disease study. Science 1996, 274, 740–743. [Google Scholar] [CrossRef]
- Lopez, A. The evolution of the Global Burden of Disease framework for disease, injury and risk factor quantification: Developing the evidence base for national, regional and global public health act. Glob. Health 2005, 1, 5. [Google Scholar] [CrossRef] [Green Version]
- Lim, S.S.; Vos, T.; Flaxman, A.D.; Danaei, G.; Shibuya, K.; Adair-Rohani, H.; Amann, M.; Anderson, H.R.; Andrews, K.G.; Aryee, M.; et al. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2224–2260. [Google Scholar]
- Murray, C.J.; Salomon, J.A.; Mathers, C. A critical examination of summary measures of population health. Bull. WHO 2000, 78, 981–994. [Google Scholar]
Appendix I: Proof

Appendix II: Worked Example
© 2013 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Rosen, L. An Intuitive Approach to Understanding the Attributable Fraction of Disease Due to a Risk Factor: The Case of Smoking. Int. J. Environ. Res. Public Health 2013, 10, 2932-2943. https://doi.org/10.3390/ijerph10072932
Rosen L. An Intuitive Approach to Understanding the Attributable Fraction of Disease Due to a Risk Factor: The Case of Smoking. International Journal of Environmental Research and Public Health. 2013; 10(7):2932-2943. https://doi.org/10.3390/ijerph10072932
Chicago/Turabian StyleRosen, Laura. 2013. "An Intuitive Approach to Understanding the Attributable Fraction of Disease Due to a Risk Factor: The Case of Smoking" International Journal of Environmental Research and Public Health 10, no. 7: 2932-2943. https://doi.org/10.3390/ijerph10072932