Communication by Mothers with Breast Cancer or Melanoma with Their Children

 ,
,
Abstract
:1. Introduction
2. Methods
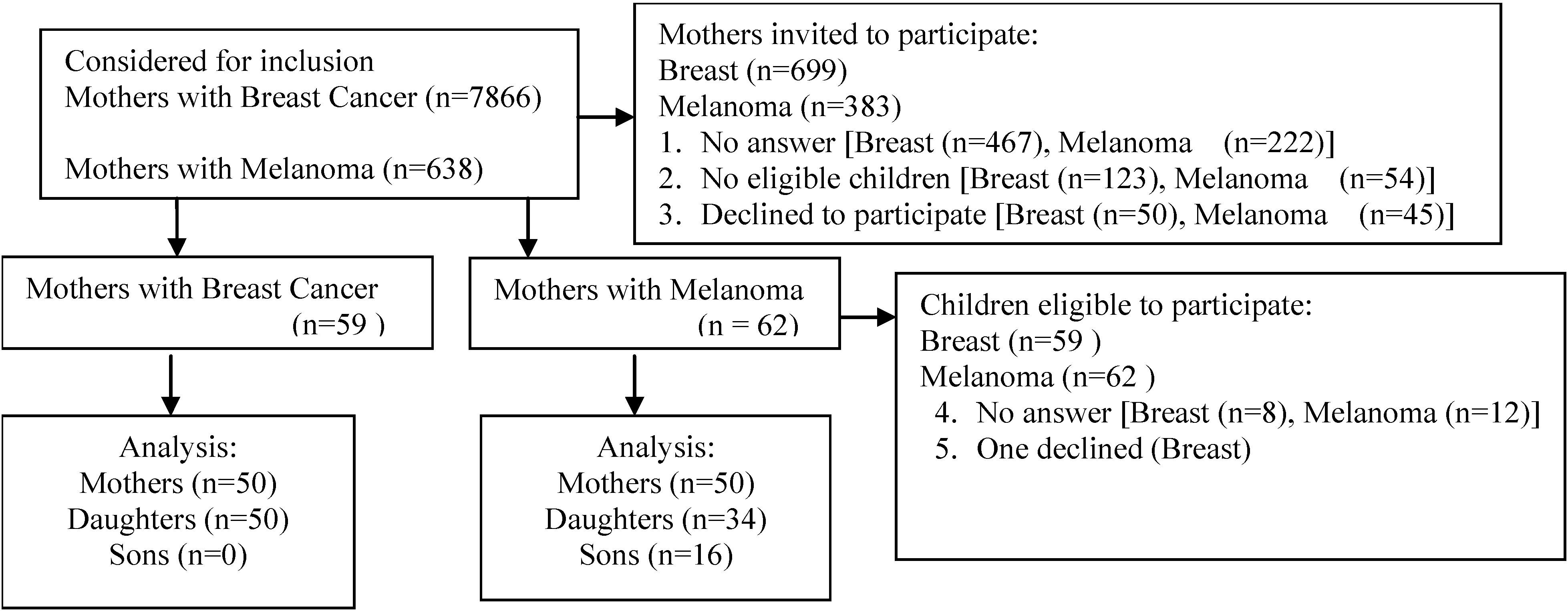
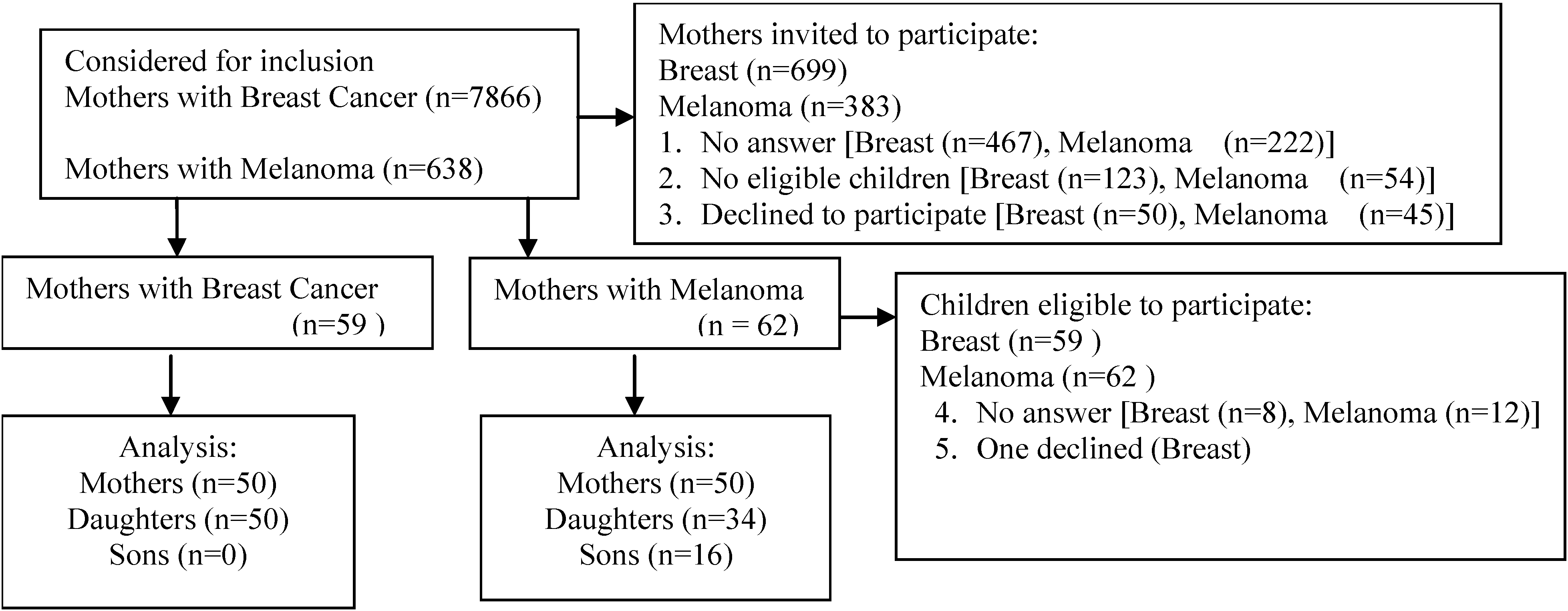
2.1. Recruitment of Participants
2.2. Data Collection and Measures
2.3. Data Analysis Methods

{kind=link}
| Variables | Breast Cancer | Melanoma | |||
|---|---|---|---|---|---|
| Mothers n = 50 # (%) | Children n = 50 # (%) | Mothers n = 50 # (%) | Children n = 50 # (%) | ||
| Marital status | |||||
| - Single | 0 (0) | 21 (42) | 2 (4) | 24 (48) | |
| - Married | 36 (72) | 25 (50) | 37 (74) | 25 (50) | |
| - Divorced | 10 (20) | 1 (2) | 4 (8) | 1 (2) | |
| - Separated | 1 (2) | 2 (4) | 0 (0) | 0 (0) | |
| - Widowed | 3 (6) | 1 (2) | 7 (14) | 0 (0) | |
| Education | |||||
| - Did not attend high school | 0 (0) | 0 (0) | 1 (2) | 0 (0) | |
| - Some high school | 1 (2) | 0 (0) | 1 (2) | 0 (0) | |
| - High school graduate | 7 (14) | 10 (20) | 5 (10) | 6 (12) | |
| - Some post-high school education | 15 (30) | 4 (8) | 8 (16) | 3 (6) | |
| - College graduate | 16 (32) | 25 (50) | 15 (30) | 24 (48) | |
| - Graduate degree | 11 (22) | 11 (22) | 20 (40) | 17 (34) | |
| Income | |||||
| - <$10,000 | 1 (2) | 4 (8) | 4 (8) | 3 (6) | |
| - $10,000–19,999 | 0 (0) | 3 (6) | 0 (0) | 1 (2) | |
| - $20,000–34,999 | 4 (8) | 1 (2) | 0 (0) | 4 (8) | |
| - $35,000–50,999 | 4 (8) | 6 (12) | 7 (14) | 5 (10) | |
| - $51,000–100,000 | 10 (20) | 16 (32) | 11 (22) | 13 (26) | |
| - >$100,000 | 12 (24) | 13 (26) | 18 (36) | 16 (32) | |
| - Not specified | 19 (38) | 7 (14) | 10 (20) | 8 (16) | |
| Occupational status | |||||
| - Student | 0 (0) | 7 (14) | 0 (0) | 5 (10) | |
| - Work part-time | 4 (8) | 10 (20) | 8 (16) | 4 (8) | |
| - Work full-time | 7 (14) | 27 (54) | 15 (30) | 34 (68) | |
| - Unemployed | 3 (6) | 2 (4) | 2 (4) | 5 (10) | |
| - Retired | 24 (48) | 0 (0) | 21 (42) | 0 (0) | |
| - Disabled | 0 (0) | 2 (4) | 0 (0) | 0 (0) | |
| - Homemaker | 12 (24) | 2 (4) | 4 (8) | 2 (4) | |
| Racial/ethnic background | |||||
| - White (non-Hispanic) | 41 (82) | 41 (82) | 48 (96) | 46 (92) | |
| - Black/African American | 6 (12) | 8 (16) | 2 (4) | 2 (4) | |
| - Multiracial | 3 (6) | 1 (2) | 0 (0) | 2 (4) | |
| - Hispanic/Latino | 3 (6) | 4 (8) | 2 (4) | 2 (4) | |
| Have health insurance | 50 (100) | 50 (100) | 49 (98) | 47 (94) | |
| Variables for Mother | Breast Cancer Pairs n = 50 # (%) | Melanoma Pairs n =50 # (%) | p value |
|---|---|---|---|
| Believes child can develop same type of cancer | 37 (74) | 43 (86) | 0.21 |
| Told child at increased risk | 45 (90) | 45 (90) | 0.99 |
| - told daughters | 45 (90) | 45 (90) | 0.99 |
| - told sons | 7 (14) | 45 (90) | <0.0001 |
| Did not tell child at increased risk | |||
| - did not tell daughters | 5 (10) | 4 (8) | 0.99 |
| - did not tell sons | 38 (76) | 7 (14) | <0.0001 |
| Reason told child * | |||
| - knowledge of child’s risk based on: | |||
| ○ family history | 17 (34) | 5 (10) | <0.0001 |
| ○ similar physically ( body type, skin type) | 6 (12) | 40 (80) | <0.0001 |
| ○ doctor recommendation | 15 (30) | 0 (0) | <0.0001 |
| - open communication | 7 (14) | 15 (30) | 0.09 |
| - child’s behavior (hormones, deliberate tanning) | 8 (16) | 28 (56) | <0.0001 |
| Reason did not tell child | |||
| - avoid causing anxiety | 1 (2) | 1 (2) | 0.99 |
| - child too busy to talk | 3 (6) | 3 (6) | 0.99 |
| - did not get a good opportunity to talk | 5 (10) | 3 (6) | 0.72 |
| Advice given | |||
| - primary prevention | |||
| ○ sun protection | 0 (0) | 30 (6) | <0.0001 |
| ○ genetic testing | 31 (62) | 5 (10) | <0.0001 |
| ○ general health and wellness (smoking, diet, exercise) | 16 (32) | 13 (26) | 0.66 |
| - secondary prevention | |||
| ○ BSE, SSE ** | 12 (24) | 4 (8) | 0.05 |
| ○ doctor examination | 13 (26) | 8 (16) | 0.33 |
| ○ mammogram | 19 (38) | 0 (0) | <0.0001 |
| Period of discussion # | |||
| - at diagnosis | 49 (98) | 50 (1) | 0.77 |
| - before treatment | 3 (6) | 3 (6) | 0.99 |
| - during treatment | 6 (12) | 7 (14) | 0.99 |
| - after treatment | 18 (36) | 15 (30) | 0.73 |
| Frequency of discussion with children ^ | |||
| - once | 14 (28) | 15 (30) | 0.99 |
| - 2–10 times | 43 (86) | 39 (78) | 0.74 |
| - over 10 times | 24 (48) | 19 (38) | 0.54 |
| - not in the last year | 14 (28) | 13 (26) | 0.99 |
| Mother believes child took advice | 42 (84) | 39 (78) | 0.82 |
| Variables for Child | Breast Cancer Pairn = 50 # (%) | Melanoma Pair n = 50 # (%) | p value |
|---|---|---|---|
| Child believes could get same type of cancer as Mother | 42 (84) | 42 (84) | 0.99 |
| Child feels open communication | 33 (66) | 39 (78) | |
| Child remembers advice | 44 (88) | 41 (82) | 0.58 |
| - primary prevention | |||
| ○ sun protection (sunscreen, stay out of sun, no tanning beds) | 0 (0) | 25 (50) | <0.0001 |
| ○ genetic testing | 6 (12) | 1 (2) | 0.11 |
| ○ general health and wellness (smoking, diet, exercise) | 10 (20) | 5 (10) | 0.26 |
| - secondary prevention | |||
| ○ BSE or SSE ** | 8 (16) | 1 (2) | 0.03 |
| ○ doctor examination | 13 (26) | 17 (34) | 0.51 |
| ○ mammogram | 31(62) | 0 (0) | <0.0001 |
| Child acted on advice by early detection * | |||
| - BSE or SSE | 33 (66) | 15 (30) | 0.0005 |
| - doctor examination | 21 (42) | 24 (48) | 0.69 |
| - mammogram | 29 (58) | 0 (0) | <0.0001 |
| Child intends to act on advice by early detection | 2 (4) | 11 (22) | 0.01 |
3. Results
3.1. Participants
3.2. Mother’s Communication about Cancer Risk
3.3. Children’s Perceptions of Risk and Actions Taken
4. Discussion
5. Conclusions
Appendix
A. Mother Interview
- (1)
- How old are you? ___________ years old
- 35–44
- 45–54
- 55–64
- 65–75
- (2)
- How many adult living children do you have? ________
- (3)
- How many boys? ______
- (4)
- How many girls? ______
- (5)
- In general, how would you describe your family’s attitudes about discussing health matters?
- do not share health matters
- share some information that is not too personal
- share just about everything
- discuss everything
- (6)
- Do you believe that is it possible that your children could develop the same type of cancer that you had?
- Yes
- No
- Don’t know
- (7)
- Have you told any of your children that they are now at greater risk of developing the same type of cancer that you had?
- Yes
- No
- (8)
- Did your child advise you about getting tested?
- Yes
- No
- (9)
- Please give me some reasons why you chose not to tell your children that they may develop the same type of cancer that you had.
- Did not want to upset them
- Children are too busy to talk to
- Family does not discuss health matters
- Doctor should tell them
- Did not get the opportunity
- Child knows because child is in the healthcare field
- (9)
- If you told your adult children about the possibility of developing cancer, how many adult children did you tell?
- (10)
- ____ Daughters (write in a number)
- (11)
- _____ Sons (write in a number)
- (12)
- How did you choose which children to tell about the possibility of developing cancer?
- daughter/son lives near me
- Children are too busy to talk to
- have a good relationship with the child
- daughter/son has children—desire to prevent grandchild from getting cancer e.g., stay out of sun, eat healthy, get genetic testing done
- Told all children because of family history
- Told all children because doctor recommended it
- Told all children so that they take care of themselves
- Just because
- Gender preference-girl
- Gender preference-boy
- Potential genetic risk
- (13)
- Do your children engage in behaviors that you think make them more likely to develop cancer?
- No, no such behaviors
- Daughter/son has an unhealthy diet
- Daughter/son doesn’t exercise
- Daughter/son goes to tanning salons
- Daughter/son has been exposed to radiation
- Daughter/son takes hormones (hormone replacement therapy, oral contraceptives, etc…)
- Lot of sun exposure at any point in their lives
- Stressful life
- Smoker
- (14)
- What advice did you give them about the cancer?
- Go see doctor (detection)
- Stay out of the sun/cover up (prevention)
- Wear sunscreen (prevention)
- Be aware of your skin/health (prevention)
- Get tested/screened (i.e., mammograms) (detection)
- Self-exams (detection)
- Don’t go to tanning salons (prevention)
- General health and wellness (i.e., no smoking, eat healthy, exercise, no hormones, positive attitude) (prevention)
- Possible genetic risk (detection)
- Consider mastectomy (detection)
- (15)
- Did you suggest skin or breast self-examination to your child/children?
- Yes
- No
- (16)
- Did you suggest going to see their doctor?
- Yes
- No
- (17)
- Did you suggest finding out more information? (i.e., on the web, library, print, books, magazines)
- Yes
- No
- (18)
- Did you suggest the possibility of getting genetic testing?
- Yes
- No
- (19)
- When during your care for cancer did you discuss early detection practices with your child?
- At time of diagnosis
- Before treatment
- During treatment
- After treatment
- (20)
- Do you think your child took your advice?
- Yes
- No
- (21)
- Did you talk to your child about what prevention steps they might take? (e.g., making doctor appointments, examining skin or breasts on a regular basis)
- Yes
- No
- (22)
- Over the past year, about how many times have you discussed your children’s risk for cancer with them?
- Once
- 2–10 times
- Over ten times (nagged)
- Not discussed in the past year
- (23)
- What is your marital status?
- Married
- Never married
- Divorced
- Separated
- Widowed
- (24)
- What is the highest level of education you have received?
- Did not attend high school
- Some high school
- High school graduate
- Some post-high school education
- College graduate
- Graduate degree
- (25)
- What is your current occupational status?
- Student
- Work part-time
- Work full-time
- Unemployed
- Retired
- Disabled
- Homemaker
- (26)
- Which of the following categories best describes your annual household income? Stop me when I get to the one that best fits.
- Less than $10,000
- $10,000 to $19,999
- $20,000 to $34,999
- $35,000 to $50,999
- $51,000 to $100,000
- Over $100,000
- Prefer not to answer
- (27)
- Which of the following describes your racial background?
- Caucasian/White
- Black or African American
- Asian
- Native Hawaiian or other Pacific Islander (please specify: ___________________)
- American Indian or Alaska Native
- Multiracial
- Other (please specify: ____________________________________)
- (28)
- Do you consider yourself to be Hispanic or Latino?
- Yes
- No
- (29)
- Do you have health insurance?
- Yes
- No
B. Adult Child Interview
- (1)
- How old are you? ________ years old
- 18–24
- 25–29
- 30
- 31–39
- 40
- 41–50
- (2)
- Participant is:
- Daughter
- Son
- (3)
- In general, how would you describe your family’s attitudes about discussing health matters?
- do not share health matters
- share some information that is not too personal
- share just about everything (=pretty open)
- discuss everything
- (4)
- Do you remember your Mother telling you that you could develop the same type of cancer that she had?
- a.
- Yes
- b.
- No
- b.
- If no—go to question 10 and continue from there
- (5)
- What advice did your Mother give you about the cancer?
- Go see doctor (detection)
- Stay out of the sun (prevention)
- Wear sunscreen (prevention)
- Be aware of your skin and health (prevention)
- Get tested (i.e., mammograms) (detection)
- Don’t go to tanning salons (prevention)
- Possible genetic risk (detection)
- Self-exams (detection)
- General health and wellness (prevention)
- Consider mastectomy (detection)
- (6)
- Did your Mother suggest that you perform skin or breast self-examination?
- Yes
- No
- (7)
- Did your Mother suggest going to see your doctor to learn about the type of cancer that she had?
- Yes
- No
- (8)
- Did you talk to a family member that is a healthcare professional to learn more about the type of cancer she had?
- Yes
- No
- (9)
- Did your Mother suggest finding out more information? (i.e., on the web, library, print, books, magazines)
- Yes
- No
- (10)
- Did your Mother suggest the possibility of getting genetic testing?
- Yes
- No
- (11)
- Do you believe that is it possible that you could develop the same type of cancer that your Mother had?
- Yes
- No
- Don’t know
- (12)
- Have you taken steps to check for cancer early?
- a.
- Yes
- b.
- No
- c.
- Not yet, but intend to
- c.
- (If no, go to question 18)
- (13)
- What steps have you taken?
- Breast self-examination
- Skin self-examination
- Doctor visit
- Mammogram
- Genetic testing
- (14)
- Have you continued with the cancer checks?
- Yes
- No
- Intend to
- (15)
- What is your marital status?
- Married
- Never married
- Divorced
- Separated
- Widowed
- (16)
- What is the highest level of education you have received?
- Did not attend high school
- Some high school
- High school graduate
- Some post-high school education
- College graduate
- Graduate degree
- (17)
- What is your current occupational status?
- Student
- Work part-time
- Work full-time
- Unemployed
- Retired
- Disabled
- Homemaker
- (18)
- Which of the following categories best describes your annual household income? Stop me when I get to the one that best fits.
- Less than $10,000
- $10,000 to $19,999
- $20,000 to $34,999
- $35,000 to $50,999
- $51,000 to $100,000
- Over $100,000
- Prefer not to answer
- (19)
- Which of the following describes your racial background? Stop me when I get to the one that best fits.
- Caucasian/White
- Black or African American
- Asian
- Native Hawaiian or other Pacific Islander (please specify: __________________)
- American Indian or Alaska Native
- Multiracial
- Other (please specify: ____________________________________)
- (20)
- Do you consider yourself to be Hispanic or Latino?
- Yes
- No
- (21)
- Do you have health insurance?
- Yes
- No
Acknowledgments
Conflict of Interest
References
- Brady, M.S.; Oliveria, S.A.; Christos, P.J.; Berwick, M.; Coit, D.G.; Katz, J.; Halpern, A.C. Patterns of detection in patients with cutaneous melanoma. Implications for secondary prevention. Cancer 2000, 89, 342–347. [Google Scholar] [CrossRef]
- Manson, J.E.; Rexrode, K.M.; Gardland, F.C.; Garland, C.F.; Weinstock, M.A. The case for a comprehensive national campaign to prevent melanoma and associated mortality. Epidemiology 2000, 11, 728–734. [Google Scholar] [CrossRef]
- Breast Cancer Survival Rates by Stage. Available online: http://www.cancer.org/cancer/breastcancer/detailedguide/breast-cancer-survival-by-stage (accessed on 12 December 2012).
- Clinical Breast Exam. Available online: http://ww5.komen.org/BreastCancer/ClinicalBreastExam.html (accessed on 9 October 2012).
- Puntervoll, H.E.; Yang, X.R.; Vetti, H.H.; Bachmann, I.M.; Avril, M.F.; Benfodda, M.; Catricalà, C.; Dalle, S.; Duval-Modeste, A.B.; Ghiorzo, P.; et al. Melanoma prone families with CDK4 germline mutation: Phenotypic profile and associations with MC1R variants. J. Am. Acad. Dermatol. 2011, 65, 281–288. [Google Scholar] [CrossRef]
- Mellon, S.; Berry-Bobovski, L.; Gold, R.; Levin, N.; Tainsky, M. Communication and decision-making about seeking inherited cancer risk information: Findings from female survivor-relative focus groups. Psychooncology 2006, 15, 193–208. [Google Scholar] [CrossRef]
- Stafford, L. Communication competencies and sociocultural priorities of middle childhood. In Handbook of Family Communication; Vangelista, A., Ed.; Lawrence Erlbaum Associates: Mahwah, NJ, USA, 2004; pp. 311–332. [Google Scholar]
- Olson, D. Circumplex model of marital and family systems. J. Family Ther. 2000, 22, 144–167. [Google Scholar]
- Loescher, L.J.; Crist, J.D.; Siaki, L.A. Perceived intrafamily melanoma risk communication. Cancer Nurs. 2009, 32, 203–210. [Google Scholar] [CrossRef]
- Richards, M.P.M. Families, kinship and genetics. In The Troubled Helix: Social and Psychological Implications of the New Genetics; Marteau, T.M., Richards, M.P.M., Eds.; Cambridge University Press: Cambridge, UK, 1996; pp. 249–273. [Google Scholar]
- Hay, J.; Ostroff, J.; Martin, A.; Serle, N.; Soma, S.; Mujumdar, U.; Berwick, M. Skin cancer risk discussions in melanoma-affected families. J. Cancer Educ. 2005, 20, 240–246. [Google Scholar] [CrossRef]
- Hay, J.; DiBonaventura, M.; Baser, R.; Press, N.; Shoveller, J.; Bowen, D. Personal attributions for melanoma risk in melanoma-affected patients and family members. J. Behav. Med. 2011, 34, 53–63. [Google Scholar] [CrossRef]
- Lawson, C.; Duhamel, K.; Brown, K.; Jandorf, L. An examination of the psychosocial factors influencing colorectal cancer patients’ communication of colorectal cancer patient risk with their siblings. Cancer Epidemiol. Biomarkers Prev. 2009, 18, 2907–2912. [Google Scholar] [CrossRef]
- Knoppers, B.M. Genetic information and the family: Are we our brother’s keeper? Trends Biotechnol. 2002, 20, 85–86. [Google Scholar] [CrossRef]
- Walter, F.M.; Emery, J. “Coming down the line”—Patients’ understanding of their family history of common chronic disease. Ann. Fam. Med. 2005, 3, 405–414. [Google Scholar] [CrossRef]
- Wolff, J.L. Family matters in health care delivery. JAMA 2012, 308, 1529–1530. [Google Scholar] [CrossRef]
- Dreyfuss, H.J.; Marvin, M.L.; Dohany, L.; Milliron, K.; Merajver, S.; Stoffel, E. Comparing Male and Female BRCA1/2 Mutation Carriers Communication of Their BRCA1/2 Test Results to Family Members. In Proceedings of the Annual Education Conference, National Society of Genetic Counselors, Boston, MA, USA, October 2012.
- Palchykov, V.; Kaski, K.; Kertesz, J.; Barabasi, A.L.; Dunbar, R.I.M. Sex differences in intimate relationships. Sci. Rep. 2012, 2, 370–375. [Google Scholar]
- Neuberger, L.; Silk, K.J.; Yun, D.; Bowman, N.D.; Anderson, J. Concern as motivation for protection: Identifying mothers’ concerns about their daughters’ breast cancer risk. J. Health Commun. 2011, 16, 1055–1071. [Google Scholar] [CrossRef]
- Gaff, C.L.; Collins, V.; Symes, T.; Halliday, J. Facilitating family communication about predictive genetic testing: Probands’ perceptions. J. Genet. Couns. 2005, 14, 133–140. [Google Scholar] [CrossRef]
- Reimer, R.R.; Clark, W.H., Jr.; Greene, M.H. Precursor lesions in familial melanoma. A new genetic preneoplastic syndrome. JAMA 1978, 239, 744–746. [Google Scholar] [CrossRef]
- National Priorities Partnership. Priorities for the National Quality Strategy. Available online: http://www.qualityforum.org/Setting_Priorities?NPP?national_Priorities_Partnership.aspx (accessed on 19 November 2012).
© 2013 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Gaber, R.; Desai, S.; Smith, M.; Eilers, S.; Blatt, H.; Guevara, Y.; Robinson, J.K. Communication by Mothers with Breast Cancer or Melanoma with Their Children. Int. J. Environ. Res. Public Health 2013, 10, 3483-3501. https://doi.org/10.3390/ijerph10083483
Gaber R, Desai S, Smith M, Eilers S, Blatt H, Guevara Y, Robinson JK. Communication by Mothers with Breast Cancer or Melanoma with Their Children. International Journal of Environmental Research and Public Health. 2013; 10(8):3483-3501. https://doi.org/10.3390/ijerph10083483
Chicago/Turabian StyleGaber, Rikki, Sapna Desai, Maureen Smith, Steve Eilers, Hanz Blatt, Yanina Guevara, and June K. Robinson. 2013. "Communication by Mothers with Breast Cancer or Melanoma with Their Children" International Journal of Environmental Research and Public Health 10, no. 8: 3483-3501. https://doi.org/10.3390/ijerph10083483