Diagnosing Cervical Dysplasia Using Visual Inspection of the Cervix with Acetic Acid in a Woman in Rural Haiti

{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction

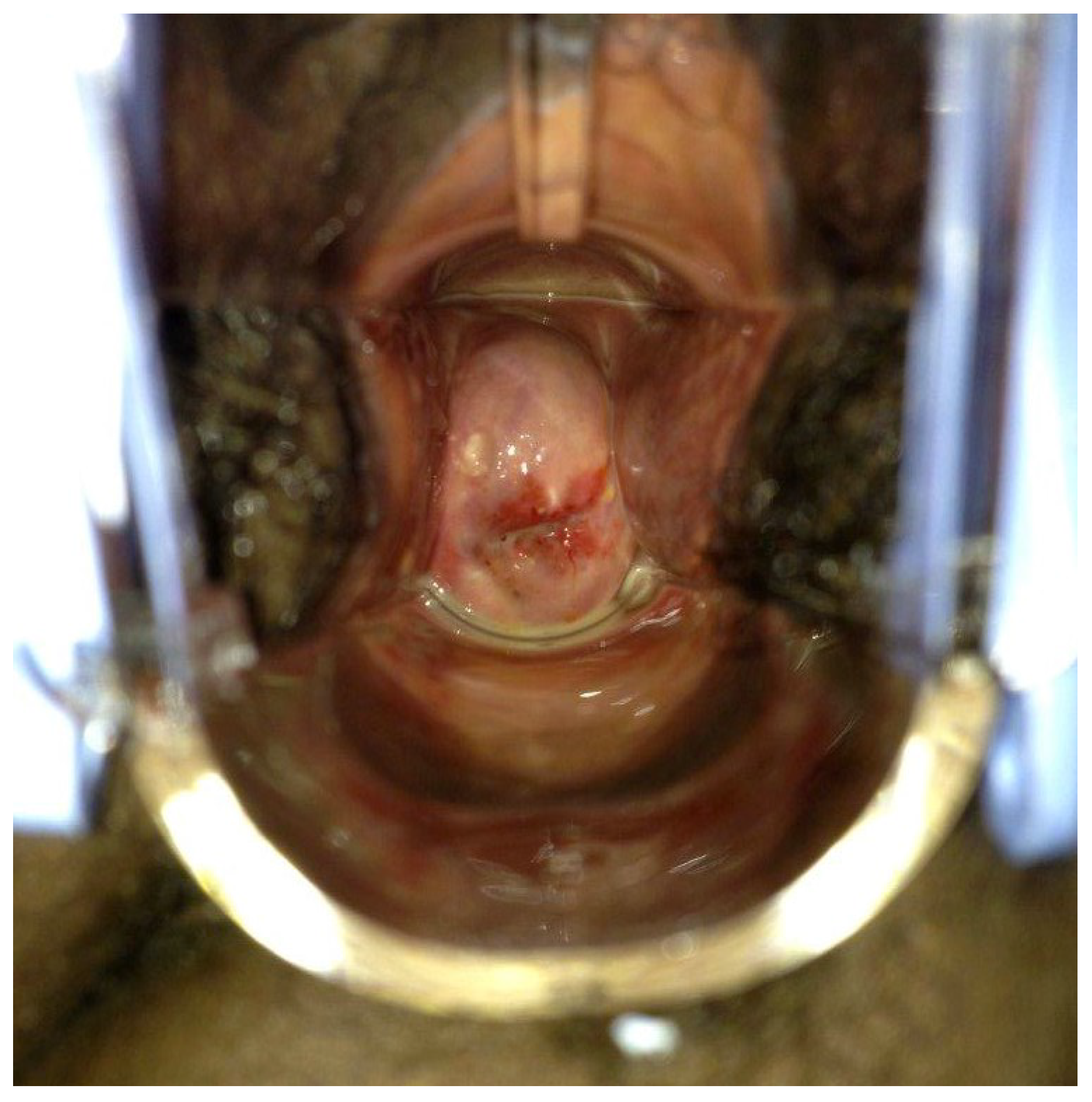
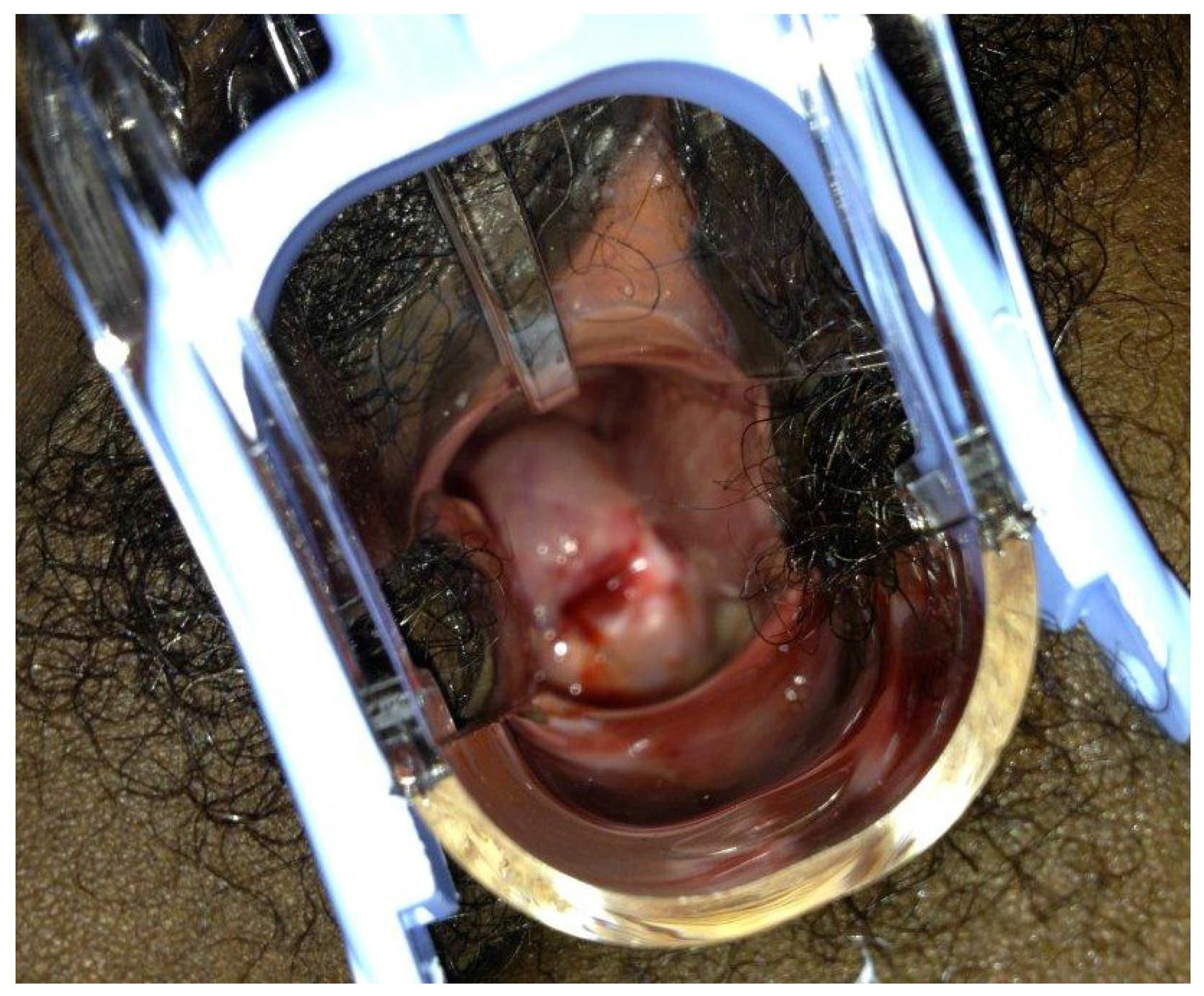
2. Case Presentation


3. Discussion
4. Conclusions
Acknowledgments
Author Contributions
Conflicts of interest
References
- Ferlay, J.; Shin, H.-R.; Bray, F.; Forman, D.; Mathers, C.; Parkin, D.M. Estimates of worldwide burden of cancer in 2008: Globocan 2008. Int. J. Cancer 2010, 127, 2893–2917. [Google Scholar] [CrossRef] [PubMed]
- Arrossi, S.; Sankaranarayanan, R.; Parkin, D.M. Incidence and mortality of cervical cancer in latin america. Incid. Mortal. Cáncer Cerv. Am. Lat. 2003, 45, S306–S314. [Google Scholar]
- Phillips, A.A.; Jacobson, J.S.; Magai, C.; Consedine, N.; Horowicz-Mehler, N.C.; Neugut, A.I. Cancer incidence and mortality in the caribbean. Cancer Investig. 2007, 25, 476–483. [Google Scholar] [CrossRef]
- Kumar, R.V.; Bhasker, S. Potential opportunities to reduce cervical cancer by addressing risk factors other than HPV. J. Gynecol. Oncol. 2013, 24, 295–297. [Google Scholar] [CrossRef] [PubMed]
- Asiaf, A.; Ahmad, S.T.; Mohammad, S.O.; Zargar, M.A. Review of the current knowledge on the epidemiology, pathogenesis, and prevention of human papillomavirus infection. Eur. J. Cancer Prev. 2014, 23, 206–224. [Google Scholar] [CrossRef]
- Denny, L.; Kuhn, L.; Risi, L.; Richart, R.M.; Pollack, A.; Lorincz, A.; Kostecki, F.; Wright, T.C., Jr. Two-stage cervical cancer screening: An alternative for resource-poor settings. Am. J. Obstet. Gynecol. 2000, 183, 383–388. [Google Scholar] [CrossRef] [PubMed]
- Van le, L.; Broekhuizen, F.F.; Janzer-Steele, R.; Behar, M.; Samter, T. Acetic acid visualization of the cervix to detect cervical dysplasia. Obstet. Gynecol. 1993, 81, 293–295. [Google Scholar]
- Denny, L.; Kuhn, L.; de Souza, M.; Pollack, A.E.; Dupree, W.; Wright, T.C., Jr. Screen-and-treat approaches for cervical cancer prevention in low-resource settings: A randomized controlled trial. JAMA 2005, 294, 2173–2181. [Google Scholar] [CrossRef] [PubMed]
- Ngelangel, C.A.; Limson, G.M.; Cordero, C.P.; Abelardo, A.D.; Avila, J.M.; Festin, M.R. Acetic-acid guided visual inspection vs. Cytology-based screening for cervical cancer in the philippines. Int. J. Gynaecol. Obstet 2003, 83, 141–150. [Google Scholar] [CrossRef]
- University of zimbabwe/jhpiego cervical cancer project. Visual inspection with acetic acid for cervical-cancer screening: Test qualities in a primary-care setting. Lancet 1999, 353, 869–873. [Google Scholar]
- Sankaranarayanan, R.; Basu, P.; Wesley, R.S.; Mahe, C.; Keita, N.; Mbalawa, C.C.; Sharma, R.; Dolo, A.; Shastri, S.S.; Nacoulma, M.; et al. Accuracy of visual screening for cervical neoplasia: Results from an iarc multicentre study in india and africa. Int. J. Cancer. 2004, 110, 907–913. [Google Scholar] [CrossRef] [PubMed]
- Tayyeb, R.; Khawaja, N.P.; Malik, N. Comparison of visual inspection of cervix and pap smear for cervical cancer screening. J. Coll. Phys. Surg. Pak. 2003, 13, 201–203. [Google Scholar]
- Sangwa-Lugoma, G.; Mahmud, S.; Nasr, S.H.; Liaras, J.; Kayembe, P.K.; Tozin, R.R.; Drouin, P.; Lorincz, A.; Ferenczy, A.; Franco, E.L. Visual inspection as a cervical cancer screening method in a primary health care setting in Africa. Int. J. Cancer 2006, 119, 1389–1395. [Google Scholar] [CrossRef] [PubMed]
- Praditsitthikorn, N.; Teerawattananon, Y.; Tantivess, S.; Limwattananon, S.; Riewpaiboon, A.; Chichareon, S.; Ieumwananonthachai, N.; Tangcharoensathien, V. Economic evaluation of policy options for prevention and control of cervical cancer in Thailand. PharmacoEconomics 2011, 29, 781–806. [Google Scholar] [CrossRef] [PubMed]
- Zhao, F.H.; Jeronimo, J.; Qiao, Y.L.; Schweizer, J.; Chen, W.; Valdez, M.; Lu, P.; Zhang, X.; Kang, L.N.; Bansil, P.; et al. An evaluation of novel, lower-cost molecular screening tests for human papillomavirus in rural China. Cancer Prev. Res. (Phila. Pa.) 2013, 6, 938–948. [Google Scholar] [CrossRef]
- Lorenzi, A.T.; Fregnani, J.H.; Possati-Resende, J.C.; Neto, C.S.; Villa, L.L.; Longatto-Filho, A. Self-collection for high-risk HPV detection in brazilian women using the care HPV test. Gynecol. Oncol. 2013, 131, 131–134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trope, L.A.; Chumworathayi, B.; Blumenthal, P.D. Feasibility of community-based carehpv for cervical cancer prevention in rural Thailand. J. Lower Genit. Tract Dis. 2013, 17, 315–319. [Google Scholar] [CrossRef]
- Elfstrom, K.M.; Herweijer, E.; Sundstrom, K.; Arnheim-Dahlstrom, L. Current cervical cancer prevention strategies including cervical screening and prophylactic human papillomavirus vaccination: A review. Curr. Opin. Oncol. 2014, 26, 120–129. [Google Scholar] [CrossRef] [PubMed]
- Davis-Dao, C.A.; Cremer, M.; Felix, J.; Cortessis, V.K. Effect of cervicitis on visual inspection with acetic acid. J. Lower Genit. Tract Dis. 2008, 12, 282–286. [Google Scholar]
- Shastri, S.S.; Mittra, I.; Mishra, G.; Gupta, S.; Dikshit, R.; Badwe, R.A. Effect of VIA screening by primary health workers: Randomized controlled study in Mumbai, India. J. Natl. Cancer Inst. 2014, 106. [Google Scholar] [CrossRef] [PubMed]
- Mathers, L.J.; Wigton, T.R.; Leonhardt, J.G. Screening for cervical neoplasia in an unselected rural guatemalan population using direct visual inspection after acetic acid application: A pilot study. J. Lower Genit. Tract Dis. 2005, 9, 232–235. [Google Scholar] [CrossRef]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Roger, E.; Nwosu, O. Diagnosing Cervical Dysplasia Using Visual Inspection of the Cervix with Acetic Acid in a Woman in Rural Haiti. Int. J. Environ. Res. Public Health 2014, 11, 12304-12311. https://doi.org/10.3390/ijerph111212304
Roger E, Nwosu O. Diagnosing Cervical Dysplasia Using Visual Inspection of the Cervix with Acetic Acid in a Woman in Rural Haiti. International Journal of Environmental Research and Public Health. 2014; 11(12):12304-12311. https://doi.org/10.3390/ijerph111212304
Chicago/Turabian StyleRoger, Elizabeth, and Oguchi Nwosu. 2014. "Diagnosing Cervical Dysplasia Using Visual Inspection of the Cervix with Acetic Acid in a Woman in Rural Haiti" International Journal of Environmental Research and Public Health 11, no. 12: 12304-12311. https://doi.org/10.3390/ijerph111212304