Autonomous Motivation Is Not Enough: The Role of Compensatory Health Beliefs for the Readiness to Change Stair and Elevator Use

Abstract
:1. Introduction
1.1. Associations between Motivation, Behavior Change, and CHBs
1.1.1. Motivation and Behavior Change
1.1.2. Motivation and CHBs
1.2. Physical (In)activity
1.3. Aims of the Study
2. Method
2.1. Procedure and Participants
2.2. Measures
2.2.1. CHBs Scale
2.2.2. Autonomous and Controlled Motivation
2.2.3. Readiness to Change Behavior
2.2.4. Self-Reported Stair and Elevator Use
2.3. Data Analysis
3. Results
3.1. Descriptives

{kind=link}
| Scale | M | SD | Range |
|---|---|---|---|
| CHBs | 4.03 | 0.99 | 1.00 to 6.00 |
| Relative Autonomy Index.(RAI) | |||
| Stair use | 4.37 | 3.43 | –6.00 to 11.67 |
| Elevator use | 2.32 | 3.21 | –4.67 to 10.83 |
| Readiness to change behavior | 3.38 | 0.99 | 1.00 to 6.00 |
| Self-reported behavior (last 7 days) | |||
| Stair use | 3.08 | 4.55 | 0.00 to 20.00 |
| Elevator use | 5.73 | 6.34 | 0.00 to 40.00 |
| Scale | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 |
|---|---|---|---|---|---|---|---|---|---|
| 1. CHBs | 1.00 | ||||||||
| 2. RAI stair use | 0.35 ** | 1.00 | |||||||
| 3. RAI elevator use | –0.13 | –0.13 | 1.00 | ||||||
| 4. RCB | 0.52 ** | 0.11 | 0.08 | 1.00 | |||||
| 5. SR stair use | 0.05 | –0.12 | 0.14 | –0.23 | 1.00 | ||||
| 6. SR elevator use | –0.08 | –0.07 | –0.19 | –0.22 | 0.29 ** | 1.00 | |||
| 7. Floor level | –0.15 | –0.14 | 0.08 | 0.02 | –0.13 | 0.29 * | 1.00 | ||
| 8. Gender | –0.33 * | –0.12 | –0.11 | –0.23 * | 0.04 | 0.07 | 0.12 | 1.00 | |
| 9. Age | 0.05 | 0.19 | 0.14 | 0.06 | 0.09 | 0.16 | 0.15 | 0.39 ** | 1.00 |
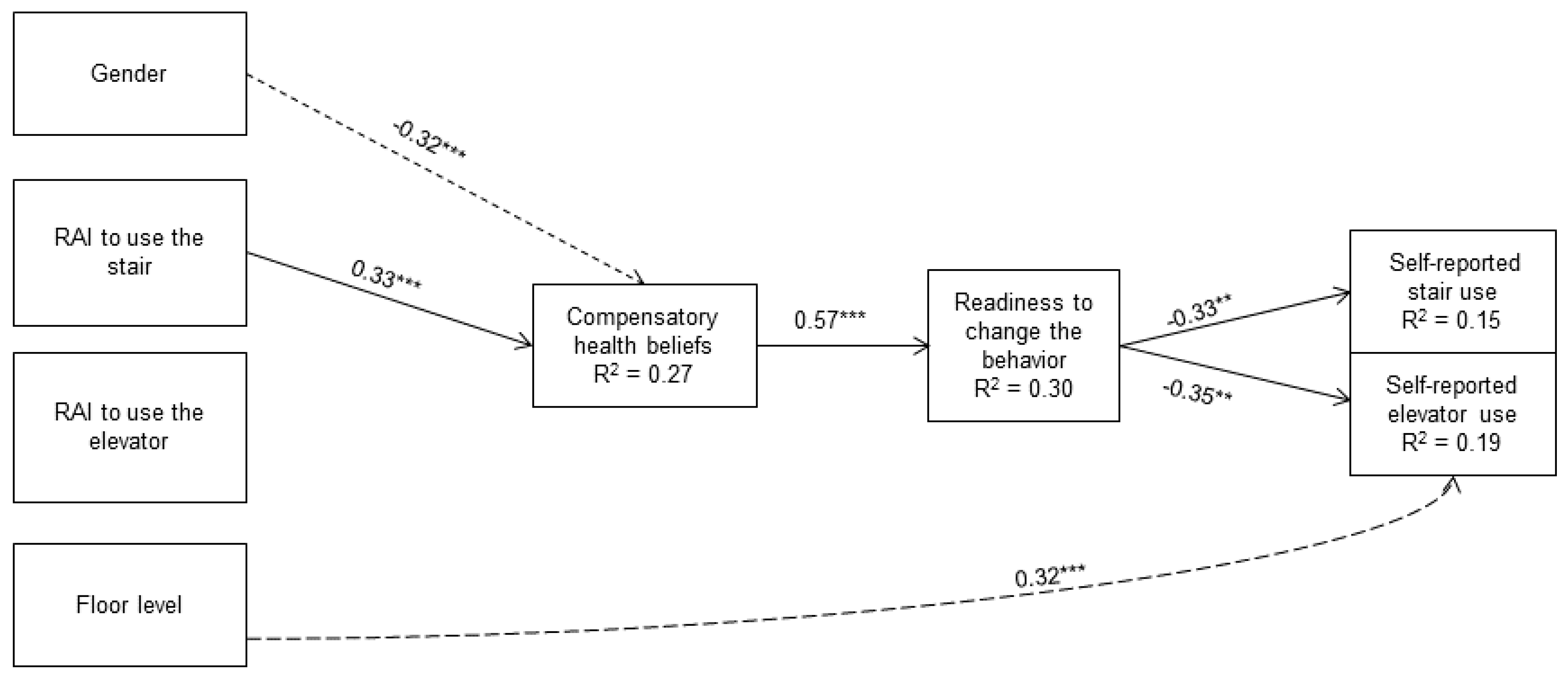
3.2. Hypothesized Model

Hypothesized Mediation Analysis
4. Discussion
4.1. Discussion of Results Concerning CHBs
4.2. Discussion of Results for Motivation
4.3. Discussion of Results for the Control Variables
4.4. Limitations
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References and Notes
- Festinger, L.A. A Theory of Cognitive Dissonance; Stanford University Press: Stanford, CA, USA, 1957. [Google Scholar]
- Rabiau, M.; Knäuper, B.; Miquelon, P. The external quest for optimal balance between maximizing pleasure and minimizing harm: The Compensatory Health Beliefs model. Brit. J. Health Psych. 2006, 11, 139–153. [Google Scholar] [CrossRef]
- Muraven, M.; Baumeister, R.F. Self-regulation and depletion of limited resources: Does self-control resemble a muscle? Psychol. Bull. 2000, 126, 247–259. [Google Scholar] [CrossRef] [PubMed]
- Higgins, E.T. Beyond pleasure and pain. Am. Psychol. 1997, 52, 1280–1300. [Google Scholar] [CrossRef] [PubMed]
- Knäuper, B.; Rabiau, M.; Cohen, O.; Patriciu, N. Compensatory health beliefs scale development and psychometric properties. Psychol. Health 2004, 19, 607–624. [Google Scholar] [CrossRef]
- Ajzen, I. Perceived behavioral control, self-efficacy, locus of control, and the theory of planned behavior. J. Appl. Soc. Psych. 2002, 32, 665–683. [Google Scholar] [CrossRef]
- Prochaska, J.O.; DiClemente, C.C. Stages and processes of self-change of smoking: Toward an integrative model of change. J. Consult. Clin. Psychol. 1983, 51, 390–395. [Google Scholar] [CrossRef] [PubMed]
- Belding, M.A.; Iguchi, M.Y.; Lamb, R.J. Stages of change in methadone maintenance: Assessing the convergent validity of two measures. Psychol. Addict. Behav. 1996, 10, 157–166. [Google Scholar] [CrossRef]
- Radtke, T.; Scholz, U.; Keller, R.; Hornung, R. Smoking is ok as long as I eat healthily: Compensatory Health Beliefs and their role for intentions and smoking within the Health Action Process Approach. Psychol. Health 2012, 27, 91–107. [Google Scholar] [CrossRef] [PubMed]
- Radtke, T.; Scholz, U.; Keller, R.; Knäuper, B.; Hornung, R. Smoking-specific compensatory health beliefs and the readiness to stop smoking in adolescents. Br. J. Health Psychol. 2011, 16, 610–625. [Google Scholar] [CrossRef] [PubMed]
- Berli, C.; Loretini, P.; Radtke, T.; Hornung, R.; Scholz, U. Predicting physical activity in adolescents: The role of compensatory health beliefs within the health action process approach. Psychol. Health 2014, 29, 458–474. [Google Scholar] [CrossRef] [PubMed]
- Miquelon, P.; Knäuper, B.; Vallerand, R.J. Motivation and goal attainment. The role of compensatory beliefs. Appetite 2012, 58, 608–615. [Google Scholar] [CrossRef] [PubMed]
- Kronick, I.; Auerbach, R.P.; Stich, C.; Knäuper, B. Compensatory beliefs and intentions contribute to the prediction of caloric intake in dieters. Appetite 2011, 57, 435–438. [Google Scholar] [CrossRef] [PubMed]
- Rabiau, M.; Knäuper, B.; Nguyen, T.-K.; Sufrategui, M.; Polychronakos, C. Compensatory beliefs about glucose testing are associated with low adherence to treatment and poor metabolic control in adolescents with type 1 diabetes. Health Educ. Res. 2009, 24, 890–896. [Google Scholar] [CrossRef] [PubMed]
- De Ridder, D. Themed issue: Plans, norms, motivation, and cheating a little—The curious case of healthy eating. Psychol. Health 2012, 27, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Deci, E.L.; Ryan, R.M. Handbook of Self-Determination Research; The University of Rochester Press: Rochester, NY, USA, 2004. [Google Scholar]
- Pelletier, L.G.; Sarrazin, P. Measurement issues in self-determination and sport. In Intrinsic Motivation and Self-Determination in Exercise and Sport; Hagger, M.S., Chatzisarantis, N.L.D., Eds.; Human Kinetics: Champaign, IL, USA, 2007; pp. 143–152. [Google Scholar]
- Williams, G.C.; Ryan, R.M.; Deci, E.L. Self-Determination in Health-Care Questionnaire Packet. The University of Rochester Press: Rochester, NY, USA, 2000; pp. 1–21. [Google Scholar]
- DeCharms, R. Personal Causation; Academic: New York, NY, USA, 1968. [Google Scholar]
- Ng, J.Y.Y.; Ntoumanis, N.; Thøgersen-Ntoumani, C.; Deci, E.L.; Ryan, R.M.; Duda, J.L.; Williams, G.C. Self-determination theory applied to health contexts: A meta-analysis. Perspect. Psychol. Sci. 2012, 7, 325–340. [Google Scholar] [CrossRef]
- Ryan, R.M.; Patrick, H.; Deci, E.L.; Williams, G.C. Facilitating health behavior change and its maintenance: Interventions based on self-determination theory. Eur. Health Psychol. 2008, 10, 2–5. [Google Scholar]
- Hagger, M.S.; Chatzisarantis, N.L.D.; Biddle, S.J.H. The influence of autonomous and controlling motives on physical activity intentions within the theory of planned behavior. Br. J. Health Psychol. 2002, 7, 283–297. [Google Scholar] [CrossRef] [PubMed]
- Sheeran, P.; Norman, P.; Orbell, S. Evidence that intentions based on attitudes better predict behavior than intentions based on subjective norms. Eur. J. Soc. Psychol. 1999, 29, 403–406. [Google Scholar] [CrossRef]
- Edmunds, J.K.; Ntoumanis, N.; Duda, J.L. A test of self-determination theory in the exercise domain. J. Appl. Soc. Psychol. 2006, 36, 2240–2265. [Google Scholar] [CrossRef]
- Wilson, P.M.; Rodgers, W.M. The relationship between perceived autonomy support, exercise regulations and behavioral intentions in women. Psychol. Sport Exerc. 2004, 5, 229–242. [Google Scholar] [CrossRef]
- Sheldon, K.M.; Elliot, A.J. Not all personal goals are “personal”. Comparing autonomous and controlling goals on effort and attainment. Pers. Soc. Psychol. Bull. 1998, 24, 546–557. [Google Scholar] [CrossRef]
- Andersen, R.E.; Franckowiak, S.C.; Snyder, J.; Bartlett, S.J.; Fontaine, K.R. Physical activity promotion by the encouraged use of stairs. Ann. Intern. Med. 1998, 129, 363–369. [Google Scholar] [CrossRef] [PubMed]
- Boreham, C.A.G.; Wallace, W.F.M.; Nevill, A. Training effects of accumulated daily stair-climbing exercise in previously sedentary young women. Preventive Med. 2000, 30, 277–281. [Google Scholar] [CrossRef]
- Benn, S.J.; McCartney, N.; McKelvie, R.S. Circulatory responses to weight lifting, walking, and stair climbing in older males. J. Am. Geriatr. Soc. 1996, 44, 121–125. [Google Scholar] [PubMed]
- Soler, R.E.; Leeks, K.D.; Buchanan, L.R.; Brownson, R.C.; Heath, G.W.; Hopkins, D.H.; Task Force on Community Preventive Services. Point-of-decision prompts to increase stair use. A systematic review update. Am. J. Prev. Med. 2010, 38, 292–300. [Google Scholar] [CrossRef]
- Bundesamt für Sport (BASPO). Gesundheitswirksame Bewegung (Health Effective Physical Activity); BASPO: Magglingen, Switzerland, 2009. [Google Scholar]
- Hardman, A.E.; Stensel, D.J. Physical Activity and Health: The Evidence Explained; Routledge: London, UK, 2003. [Google Scholar]
- World Health Organization. Global Recommendations on Physical Activity for Health. WHO: Geneva, Switzerland, 2010. [Google Scholar]
- Müller-Riemenschneider, F.; Nocon, M.; Reinhold, T.; Willich, S.N. Promotion of physical activity using point-of-decision prompts in Berlin underground stations. Int. J. Environ. Res. Public Health 2010, 7, 3063–3070. [Google Scholar] [CrossRef] [PubMed]
- Kwak, L.; Kremers, S.P.J.; van Baak, M.A.; Brug, J. Formation of implementation intentions promotes stair use. Am. J. Prev. Med. 2007, 32, 254–255. [Google Scholar] [CrossRef] [PubMed]
- World Medical Organization. Declaration of Helsinki (1964). BMJ 1964, 7070, 1448–1449. [Google Scholar]
- Results of a confirmatory factor analysis showed that all four items represent compensatory health beliefs regarding physical activity. The tested model indicating a good model fit (χ2(8, N = 135) = 171.18; p < 0.01; CFI = 1.00, TLI = 1.03, RMSEA < 0.01, SRMR = 0.02).
- Seelig, H.; Fuchs, R. Messung der sport-und bewegungsbezogenen Selbstkonkordanz (Measurement of exercise related self-concordance). Zeitschrift. für Sportpsychologie. 2006, 13, 121–139. [Google Scholar] [CrossRef]
- Hannöver, W.; Thyrian, J.R.; Rumpf, H.-J.; Meyer, C.; Hapke, U.; John, U. Der Fragebogen zur Änderungsbereitschaft bei Rauchern (FÄR) (Questionnaire of the readiness to change smoking behavior). In Elektronisches Handbuch zu Erhebungsinstrumenten im Suchtbereich (EHES)(Electronic manual on survey measures in the area of addiction), 3rd ed.; Glöckner-Rist, A., Rist, F., Küfner, H., Eds.; Zentrum für Umfragen, Methoden und Analysen: Mannheim, Germany, 2001. [Google Scholar]
- Muthén, L.K.; Muthén, B.O. Mplus User’s Guide, 6th ed.; Muthén & Muthén: Los Angeles, CA, USA, 2011. [Google Scholar]
- Testing Structural Equation Models; Bollen, K.; Long, J. (Eds.) Sage: Thousand Oaks, CA, USA, 1993.
- Preacher, K.J.; Hayes, A.F. Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behav. Res. Methods 2008, 40, 879–891. [Google Scholar] [CrossRef] [PubMed]
- Radtke, T.; Kaklamanou, D.; Scholz, U.; Hornung, R.; Armitage, C.J. Are diet-specific compensatory health beliefs predictive of dieting intentions and behavior? Appetite 2014, 76, 36–43. [Google Scholar] [CrossRef] [PubMed]
- Engbers, L.H.; van Poppel, M.N.M.; Paw, M.C.A.; van Mechelen, W. The effects of a controlled worksite environmental intervention on determinants of dietary behavior and self-reported fruit, vegetable and fat intake. BMC Public Health 2006, 6, 253–254. [Google Scholar] [CrossRef] [PubMed]
- Epstein, L.H.; Gordy, C.C.; Raynor, H.A.; Beddome, M.; Kilanowski, C.K.; Paluch, R. Increasing fruit and vegetable intake and decreasing fat and sugar intake in families at risk for childhood obesity. Obes. Res. 2001, 9, 171–178. [Google Scholar] [CrossRef] [PubMed]
- Epstein, L.H.; Paluch, R.A.; Beecher, M.D.; Roemmich, J.N. Increasing healthy eating vs. reducing high energy-dense foods to treat pediatric obesity. Obesity 2008, 16, 318–326. [Google Scholar] [CrossRef] [PubMed]
- Salmon, J.; Jorna, M.; Humel, C.; Arundell, L.; Chahine, N.; Tienstra, M.; Crawford, D. A translational research intervention to reduce screen behaviors and promote physical activity among children: Switch-2-Activit. Health Promot. Int. 2011, 26, 311–321. [Google Scholar] [CrossRef] [PubMed]
- Courtenay, W.H. Constructions of masculinity and their influence on men’s well-being: A theory of gender and health. Soc. Sci. Med. 2000, 50, 1385–1401. [Google Scholar] [CrossRef] [PubMed]
- George, D.; Mallery, P. SPSS for Windows Step by Step: A Simple Guide and Reference. 11.0 Update, 4th ed.; Allyn & Bacon: Boston, MA, USA, 2003. [Google Scholar]
- Wallace, L.S.; Buckworth, J. Application of the transtheoretical model to exercise behavior among nontraditional college students. Am. J. Health Educ. 2001, 32, 39–47. [Google Scholar] [CrossRef]
- Kline, R.B. Principles and Practice of Structural Equation Modeling; Guilford Press: New York, NY, USA, 2005. [Google Scholar]
- Adriaanse, M.A.; De Ridder, D.T.D.; de Wit, J.B.F. Finding the critical cue: Implementation intentions to change one’s diet work best when tailored to personally relevant reasons for unhealthy eating. Pers. Soc. Psychol. Bull. 2009, 35, 60–71. [Google Scholar] [CrossRef]
- Pantalon, M.V.; Sledge, W.H.; Bauer, S.F.; Brodsky, B.; Giannandrea, S.; Kay, J.; Lazar, S.G.; Mellman, L.A.; Offenkrantz, W.C.; Oldham, J.; et al. Important medical decisions: Using brief motivational interviewing to enhance patients’ autonomous decision-making. J. Psychiatr. Pract. 2013, 19, 98–108. [Google Scholar] [CrossRef] [PubMed]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Radtke, T.; Rackow, P. Autonomous Motivation Is Not Enough: The Role of Compensatory Health Beliefs for the Readiness to Change Stair and Elevator Use. Int. J. Environ. Res. Public Health 2014, 11, 12412-12428. https://doi.org/10.3390/ijerph111212412
Radtke T, Rackow P. Autonomous Motivation Is Not Enough: The Role of Compensatory Health Beliefs for the Readiness to Change Stair and Elevator Use. International Journal of Environmental Research and Public Health. 2014; 11(12):12412-12428. https://doi.org/10.3390/ijerph111212412
Chicago/Turabian StyleRadtke, Theda, and Pamela Rackow. 2014. "Autonomous Motivation Is Not Enough: The Role of Compensatory Health Beliefs for the Readiness to Change Stair and Elevator Use" International Journal of Environmental Research and Public Health 11, no. 12: 12412-12428. https://doi.org/10.3390/ijerph111212412
APA StyleRadtke, T., & Rackow, P. (2014). Autonomous Motivation Is Not Enough: The Role of Compensatory Health Beliefs for the Readiness to Change Stair and Elevator Use. International Journal of Environmental Research and Public Health, 11(12), 12412-12428. https://doi.org/10.3390/ijerph111212412