Indoor Exposure and Adverse Birth Outcomes Related to Fetal Growth, Miscarriage and Prematurity—A Systematic Review

Abstract
:1. Introduction
2. Methods
2.1. Literature Search Strategy

{kind=link}
| IAP § and Pregnancy Outcome |
|---|
| Exposure |
| 1. * Air Pollution, Indoor/ |
| 2. * Particulate Matter/ |
| 3. * Nicotine/ |
| 4. * Carbon Monoxide/ |
| 5. * Nitrogen Dioxide/ |
| 6. * Sulfur Dioxide/ |
| 7. * Polycyclic Hydrocarbons, Aromatic/ |
| 8. * Radon/ |
| 9. * Solvents/ |
| 10. * Asbestos/ |
| 11. * Ozone/ |
| 12. * Pesticides/ |
| 13. * Volatile Organic Compounds/ |
| 14. * Formaldehyde/ |
| 15. * Benzene/ |
| 16. * Toluene/ |
| 17. * Styrene/ |
| 18. * Dibutyl Phthalate/or phthalate.mp. |
| 19. * Polyvinyl Chloride/ |
| 20. * Noise/or * Noise, Occupational/ |
| 21. * Electromagnetic Fields/ |
| 22. * Magnetic Fields/ |
| 23. 1 or 2 or 3 or 4 or 5 or 6 or 7 or 8 or 9 or 10 or 11 or 12 or 13 or 14 or 15 or 16 or 17 or 18 or 19 or 20 or 21 or 22 |
| Outcome |
| 24. * Pregnancy Outcome |
| 25. * Pre-Eclampsia/or * Pregnancy Outcome/or * Fetal Death/or * Premature Birth/or * Pregnancy Complications/or * Abortion, Spontaneous/ |
| 26. * Birth Weight |
| 27. low birth weight.mp. or * Infant, Low Birth Weight/ |
| 28. Fetal Growth Retardation/or Gestational Age/or intrauterine growth.mp. or “Embryonic and Fetal Development”/ |
| 29. * Congenital Abnormalities/ |
| 30. * Hypertension, Pregnancy-Induced/ |
| 31. * Infant Mortality/or * Perinatal Mortality/or *Fetal Death |
| 32. * Infant, Premature/or preterm.mp. |
| 33. 24 OR 25 OR 26 OR 27 OR 28 OR 29 OR 30 OR 31 OR 32 |
| Combined terms |
| 34. 23 AND 33 |
2.2. Selection Criteria
- papers published in peer-reviewed journal
- papers published in English language
- human epidemiological studies of any study design
- studies conducted in developed countries (definition was based on the list of Developing Countries provided by the International Statistical Institute)
2.3. Literature Screening and Data Extraction
2.4. Study Evaluation and Critical Appraisal of the Evidence
3. Results
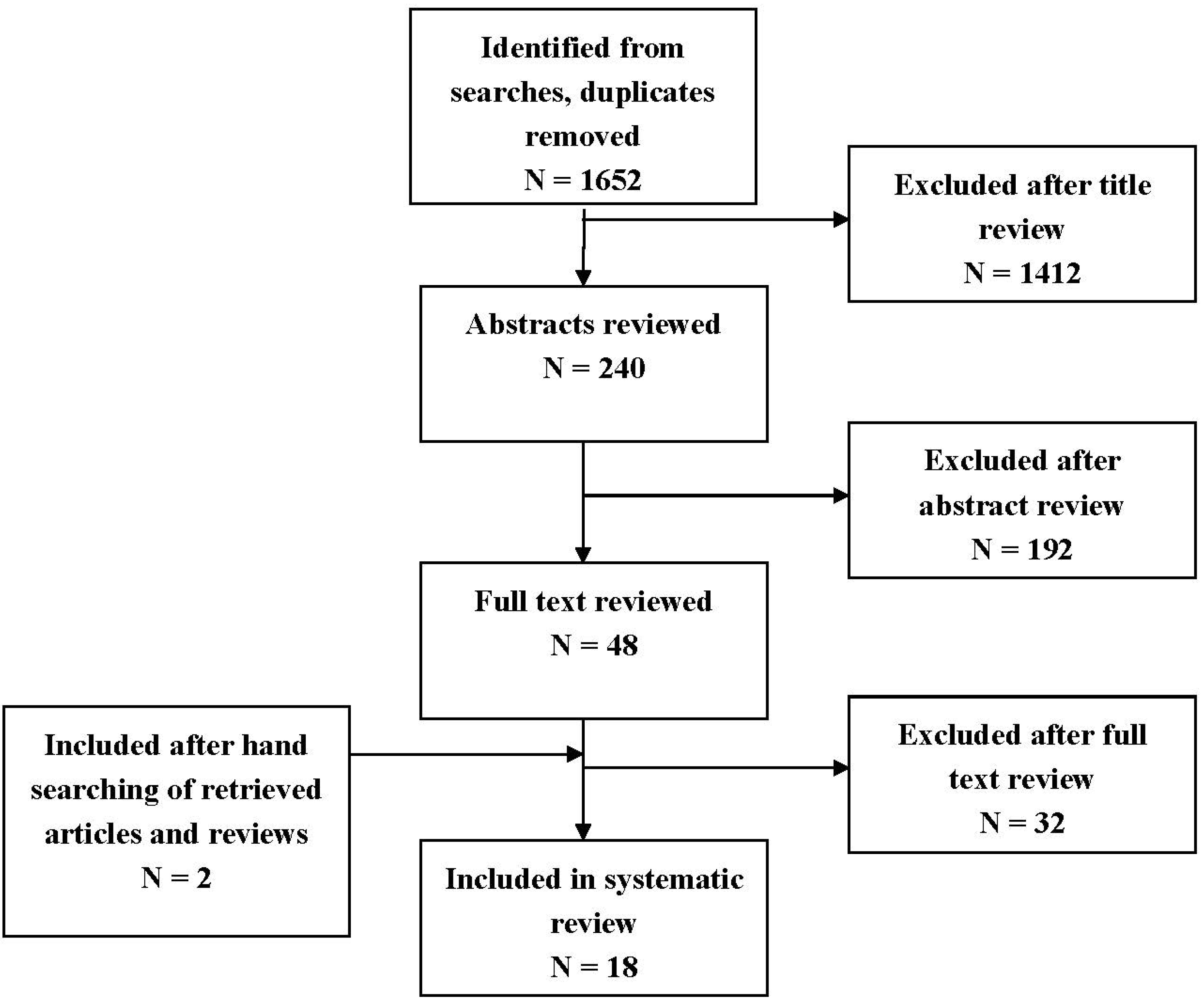
3.1. Bibliographic Search

3.2. Overview of the Included Studies
3.3. Effects of Quantified Exposure to Indoor Pollutants on Birth Outcomes
3.4. Effects of Quantified All-day Exposure to Pollutants on Birth Outcomes
| Reference | Study Characteristics | Exposure Assessment | Pollutants Studied (Units) | Outcome Assessment |
|---|---|---|---|---|
| [27] | USA 1987–1988: telephone interviews 1990: measurements of the electromagnetic fields Retrospective study design Women employed as directory—assistance operators and general telephone operators at two companies Sample population: 730 | Occupational exposure status based on measurements conducted at some (8 of the 50) workstations. Measurements taken at operator’s abdomen. | MF (μT) | Self reported cross-checked with state records |
| [25] | Finland, 1975–1985 Case- control study Women employed as bank clerks and clerical workers in three companies Sample population: 585 | Occupational exposure status based on laboratory measurements of the fields of 17 models of VDT. Measurements taken at 50 cm in front of the screen and at the site approximated for the fetus (25 cm down) at the same distance. | EMF (μT) | Self reported cross-checked with nationwide data records |
| [24] | Kuopio, Finland, 1988–1989 A nested case-control study 89 cases and 102 controls that had participated to the Work and Fertility study during the period 1984–1986 Sample population: 191 | Magnetic field was measure in the residences where the women lived when participating in the Work and Fertility study. The magnetic field strength was measured at the front door of each residence in the living room, in the kitchen, and in the parents’ bedroom. The measurement in the bedroom was taken at the center of the bed whereas the measurements in the other rooms were taken near the center of the room, 1m above the floor. Measurements were also taken in other parts of the room to check that the field in the chosen measuring point represents the average level of the room. | MF (A/m) | Hospital records |
| [26] | Colorado, USA, 1976–1983 Case-control study 78 childhood cancer cases and 78 controls selected through birth certificates Sample population: 156 | Electric and magnetic field measurements were sought at the time of the interviews at those residences. Measurements were taken near the front door, in the child’s bedroom, and in the parents’ bedroom. Any room reported in the questionnaire to have been occupied by the child an average of one or more hours per day was measured. In each selected room, measurements were taken as near as possible to the center of the room while avoiding close proximity to appliances or large metal objects. | EMF (mT) | Hospital records |
| [28] | Connecticut, USA, 1988–1991 Prospective study Women receiving their prenatal care at 11 private obstetrical practices and two health maintenance organizations Sample population: 2,967 | Residential exposure status. EMF exposure using: personal monitors—women were asked to wear an average magnetic field exposure meter for the following 7 days leaving it at the bedside at night. Home measurement- An electric and magnetic digital exposure meter was placed in the center of a room for a 24-h period. | EMF (mG) | Hospital records and direct examination of the newborns |
| [17] | Taiwan, 1991 Prospective study Women in the first trimester of their pregnancy from obstetric clinics at 25 maternity hospitals Sample population: 200 | Residential exposure status. Personal 24-h noise exposure was measured on work days at work and home. | Noise (dBALeq24) | Hospital records |
| [36] | California, USA, 1990–1991 Prospective sub-study Nested Case-Control Study Subjects recruited from a cohort of 3403 pregnant women who participated in a large prospective reproductive health study Sample population: 155 cases, 509 controls | Residential and occupational exposure status. EMF exposure using: Personal monitors—women were asked to use a meter for a 24-h period and record on an activity card the time when they entered a new environment. Women were leaving meters at the bedside at night. Home measurement- Spot measurements with the same meter were taken outside the front door and inside the home in the center of the kitchen, living room, and participant’s bedroom | EMF (mG) | Prospective reproductive health study records |
| [37] | San Francisco, USA, 1996–1998 Prospective cohort study All women with a positive pregnancy test at less 10 weeks of gestation and residing in the San Francisco area were contacted for participation in the study. Sample population: 969 | All participants were also asked to wear a magnetic field measuring meter for 24 h and to keep a diary of their activities. Spot measurements were taken in the subject’s bed room, the kitchen and the most frequent occupied room that was neither a bedroom nor a kitchen. Measurements were made at the abdominal level in the center of each room as well as the location at the subject typically occupied. In addition, measurements were taken at the front entrance of the residence and at approximately 15-foot intervals proceeding clockwise around the residence. | MF (mG) | Health databases |
| Reference | Study Characteristics | Exposure Assessment | Pollutants Studied (Units) | Outcome Assessment |
|---|---|---|---|---|
| [38] | New York, USA NYC prospective study Non-smoking women aged 18–35, who registered at the obstetrics and gynecology clinics of two hospitals by the 20th week of pregnancy Sample population: 263 | During the 3rd trimester of pregnancy women were asked to wear a small backpack containing a personal monitor during the day time hours for 2 consecutive days and to place the monitor near the bed at night. | 8 carcinogenic PAHs (ng/m3): benz[a]anthracene, chrysene, benzo[b]fluroanthene, benzo[k]fluroanthene, B[a]P, indeno[1,2,3-cd]pyrene, disbenz[a,h]anthracene and benzo[g,h,i]perylene | Hospital records |
| [32] | Krakow, Poland, 2001–2003 Krakow prospective study The cohort consisted of 362 pregnant women who gave birth between 34 and 43 weeks of gestation Sample population: 362 | Women were asked personal air monitoring over 48 h during the 2nd trimester of pregnancy | PM2.5 (ng/m3) | Hospital records |
| [33] | Krakow, Poland, 2001–2004 Krakow prospective study The cohort consisted of 493 pregnant women who gave birth between 37 and 43 weeks of gestation Sample population: 493 | Women were asked personal air monitoring over 48 h during the 2nd trimester of pregnancy | PM2.5 (ng/m3) | Hospital records |
| [34] | Krakow, Poland, 2001–2004 Krakow prospective study The cohort consisted of 481 pregnant women who gave birth between 37 and 43 weeks of gestation Sample population: 481 | Women were asked personal air monitoring over 48 h during the 2nd trimester of pregnancy In the monitoring period women have spent on average 3 h outdoors and 2 h in the public transportation and those who used the public transportation had insignificantly higher level of PM2.5 exposures. | PM2.5 (ng/m3) | Hospital records |
| [35] | Krakow, Poland, 2001–2004 Krakow prospective study The cohort consisted of 431 pregnant women who gave birth between 37 and 43 weeks of gestation Sample population: 431 | Women were asked personal air monitoring over 48 h during the 2nd trimester of pregnancy | PM2.5 (ng/m3) | Hospital records |
| [29] | Krakow, Poland 2000–2003 New York, USA 2004 Data from two prospective cohort studies (Krakow and NYC) that enrolled non-smoking, healthy, and non-occupationally exposed women and their newborns. Sample population: 720 | Women were asked to wear a small backpack containing a personal monitor during the day time hours for 2 consecutive days and to place the monitor near the bed at night. | Levels of pyrene and 8 carcinogenic PAHs (ng/m3): benz[a]anthracene, chrysene, benzo[b]fluroanthene, benzo[k]fluroanthene, B[a]P, indeno[1,2,3-cd]pyrene, disbenz[a,h]anthracene and benzo[g,h,i]perylene | Hospital records |
| [30] | New York, USA, 2004 NYC prospective study Women non-smoking, healthy, and non-occupationally exposed women and their newborns. Sample population: 616 | During the 3rd trimester of pregnancy women were asked to wear a small backpack containing a personal monitor during the day time hours for 2 consecutive days and to place the monitor near the bed at night. | Levels of pyrene and 8 carcinogenic PAHs (ng/m3): benz[a]anthracene, chrysene, benzo[b]fluroanthene, benzo[k]fluroanthene, B[a]P, indeno[1,2,3-cd]pyrene, disbenz[a,h]anthracene and benzo[g,h,i]perylene | Hospital records |
| [31] | Krakow, Poland, 2000–2003 Krakow prospective study Causacian pregnant women of ethnic Polish background aged 18–34 during the 8th to 13th weeks of gestation were included in the study. Sample population: 344 | Women were simultaneously monitored for their personal (n = 344), home indoor (n = 76) and outdoor (n = 70) levels of PAHs and PM2.5 during the 2nd trimester of pregnancy. The subset of women that were personal monitored were asked to wear a small backpack containing a personal monitor during the day time hours for 2 consecutive days and personal monitoring was repeatedly taken once during each trimester. | Levels of pyrene and 8 carcinogenic PAHs (ng/m3): benz[a]anthracene, chrysene, benzo[b]fluroanthene, benzo[k]fluroanthene, B[a]P, indeno[1,2,3-cd]pyrene, disbenz[a,h]anthracene and benzo[g,h,i]perylene | Hospital records |
| [39] | France, 2005–2006 EDEN prospective cohort study Women at <20 gestational weeks were recruited from two maternity hospitals between 2003–2006. Sample population: 271 | Women were asked to carry a diffusive air sampler for 7 consecutive days and to keep it close to their bed when they slept. | Benzene (ng/m3) | Hospital records, measurements at birth, ultrasound examinations |
| [40] | New York, US 2000–2006 NYC prospective study Women 18–35 years of age who self identified as either African American or Dominican and who had resided in northern Manhattan or the South Bronx for ≥1 year before pregnancy. Sample population: 331 | Women were asked to wear a small backpack containing a personal monitor during the day time hours for 2 consecutive days and to place the monitor near the bed at night. | Di(2-ethylhexyl)Phthalate (ng/m3) | Hospital records |
| References | Time of Exposure | Outcome | Main Results OR (95% CI) | Covariates | CASPgrade |
|---|---|---|---|---|---|
| [27] | 1st trimester | SAB (n = 136) | non users vs. 0.07 μT vs. 0.08 μT | None adjustment | 4/9 |
| OR 1.00 vs. 0.92 95% CI (0.58–1.47) vs. 0.98 95% CI (0.58–1.64) | |||||
| [25] | 1st trimester | SAB (n = 91) | <0.4 μT vs. 0.4–0.9 μT vs. >0.9 μT | Use of video display terminals, hours of use per week, quantity of work, frequency of technical breakdowns in automatic data processing devices, exposure to organic solvents, number of previous births, previous spontaneous abortions, use of an intrauterine device | 5/9 |
| OR 1.0 vs. 1.9 95% CI (0.9–3.9) vs. 3.4 95% CI (1.4–8.6) | |||||
| [24] | Not specific trimester exposure | Pregnancy loss (n = 89) | Magnetic field exposure (A/m) | Smoking | 6/9 |
| Front door value < 0.2 vs. ≥ 0.2 | |||||
| OR 1.11 95% CI (0.6 to 2.3) | |||||
| Average < 0.2 vs. ≥ 0.2 | |||||
| OR 5.44 95% CI (1.1 to 28) | |||||
| [26] | Not specific trimester exposure | Measured magnetic fields- Spot measurements | None | 5/9 | |
| ≥2 mT vs. <2 mT | |||||
| Miscarriage OR 0.8 95% CI (0.3 to 2.3) | |||||
| Low birth weight OR 0.3 95% CI (0.0 to 2.4) | |||||
| Preterm delivery OR 0.7 95% CI (0.1 to 4.0) | |||||
| [28] | At conception, at ≤16 weeks, or 3rd trimester | LBW IUGR LBW IUGR | 24-h home EMDEX monitor (mG) | Maternal religion, race, height, weight, gravity, age, work in pregnancy, third trimester smoking, caffeine consumption | 8/10 |
| <1.0 vs. 1.0–1.9 vs. ≥2.0 | |||||
| Referent vs. 0.94 (0.24–3.61) vs. not estimable | |||||
| Referent vs. 0.79 (0.32–1.92) vs. 0.62 (0.16–2.31) | |||||
| 7-day personal AMEX monitor (mG) | |||||
| <1.0 vs. 1.0–1.9 vs. ≥2.0 | |||||
| Referent vs. 0.65 (0.15–2.88) vs. 1.35 (0.30–6.11) | |||||
| Referent vs. 0.40 (0.14–1.15) vs. 1.16 (0.43–3.11) | |||||
| [17] | 1st, 2nd, 3rd trimester | Birth weight (grams) | No risk reported | None adjustment | 4/9 |
| [36] | 30th week of pregnancy | SAB (n = 155) | Measured fields 24 h | Maternal age, gestation at interview, coffee consumption around conception, income, race, and each of the other personal 24-h exposures (excluding total 24-h) | 6/9 |
| ≥2 mG vs. <2 mG | |||||
| Home: OR 0.8 95% CI (0.2–3.5) | |||||
| Work: OR 0.7 95% CI (0.3–1.5) | |||||
| Total: 24-h OR 1.0 95% CI (0.5–2.1) | |||||
| Front door spot: OR 1.2 95% CI (0.6–2.5) | |||||
| Inside spots: OR 1.1 95% CI (0.5–2.2) | |||||
| Time-weighted average | |||||
| <0.72 vs. 0.72–0.93 vs. 0.93–1.28 vs. >1.28 | |||||
| OR 1.0 vs. OR 1.7 95% CI (0.9–3.3) vs. OR 1.7 95% CI (0.9–3.3) vs. OR 1.7 95% CI (0.9–3.2) | |||||
| Maximum value (mG) | |||||
| <14.31 vs. 14.31–23.42 vs. 23.42–35.05 vs. >35.05 | |||||
| OR 1.0 vs. OR 1.4 95% CI (0.7–2.8) vs. OR 1.9 95% CI (1.0–3.5) vs. OR 2.3 95% CI (1.2–4.4) | |||||
| [37] | 1st trimester | SAB (n = 159) | Measured fields 24 h | Previous miscarriage, education, maternal age, gravidity, race, smoking since last menstrual period | 6/9 |
| <16 mG vs. ≥16 mG | |||||
| RR 1.8 95% CI (1.2–2.7) | |||||
| Total sum of exposure over 16 mG in tertiles | |||||
| 160–1,079 vs. 1,080–4,759 vs. ≥ 4,760 mG | |||||
| RR 1.7 95% CI (1.1–2.8) vs. RR 1.8 95% CI (1.1–2.9) vs. RR 2.0 95% CI (1.2–3.17) |
| References | Time of Exposure | Outcome | Main Results OR (95%CI) | Covariates | CASPgrade | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| [38] | 3rd trimester | Birth weight (grams), length (cm), head circumference (cm) | All | BMI, parity, cotinine, sex of baby, gestational age | 6/10 | |||||
| Birth weight: Beta-coefficient −0.05, p-value = 0.08 | ||||||||||
| Birth length: Beta-coefficient −0.02, p-value = 0.08 | ||||||||||
| Birth head circumference: Beta-coefficient −0.01, p-value = 0.12 | ||||||||||
| African-American | ||||||||||
| Birth weight: Beta-coefficient −0.10, p-value = 0.02 | ||||||||||
| Birth length: Beta-coefficient −0.02, p-value = 0.24 | ||||||||||
| Birth head circumference: Beta-coefficient −0.02, p-value = 0.06 | ||||||||||
| Dominican | ||||||||||
| Birth weight: Beta-coefficient −0.009, p-value = 0.81 | ||||||||||
| Birth length: Beta-coefficient −0.02, p-value = 0.11 | ||||||||||
| Birth head circumference: Beta-coefficient 0.003, p-value = 0.80 | ||||||||||
| [32] | 2nd trimester | Birth weight (grams), length (cm), head circumference (cm) | LogPM2.5 | Number of pregnancies, height, and prepregnancy weight of mother, sex of newborn, gestational age | 7/10 | |||||
| Birth weight: Beta-coefficient −200.821 95% CI (−385.968 to −15.674) | ||||||||||
| Birth length: Beta-coefficient −1.439 95% CI (−2.583 to −0.294) | ||||||||||
| Birth head circumference: Beta-coefficient −0.729 95% CI (−1.347 to −0.112) | ||||||||||
| [33] | 2nd trimester | Birth weight (grams), length (cm), head circumference (cm) | PM2.5 | Maternal education, parity, maternal height, pre- pregnancy weight, weight gain over pregnancy, gestational age, gender of child, season of birth | 7/10 | |||||
| 27.0–46.19 μg/m3 vs. ≥46.2 μg/m3 | ||||||||||
| Birth weight: Beta-coefficient −16.51 95% CI (−94.64 to 61.61) vs. −109.956 95% CI (196.649 to −23.263) | ||||||||||
| Birth length: Beta-coefficient −0.288 95% CI (−0.790 to 0.214) vs. −0.810 95% CI (−1.367 to −0.253) | ||||||||||
| [34] | 2nd trimester | Birth weight (grams), length (cm), head circumference (cm) | LogPM2.5 | Maternal education, gestational age, parity, maternal height, prepregnancy weight, sex of infant, prenatal environmental tobacco smoke, season of birth | 7/10 | |||||
| Birth weight: Beta-coefficient −155.9 95% CI (−307.2 to −4.7) | ||||||||||
| Birth length: Beta-coefficient −1.24 95% CI (−2.19 to −0.28) | ||||||||||
| Birth head circumference: Beta- coefficient −0.53 95% CI (−1.04 to −0.02) | ||||||||||
| [35] | 2nd trimester | Systolic blood pressure (mmHg)Diastolic blood pressure (mmHg) | LogPM2.5 | Maternal age, education, parity, gestational weight gain, prepregnancy BMI, environmental tobacco smoke, blood lead level | 7/10 | |||||
| Systolic blood pressure: Beta-coefficient −6.126 95% CI (0.610 to 11.642) | ||||||||||
| Diastolic blood pressure: Beta-coefficient 4.083 95% CI (−0.019 to 8.185) | ||||||||||
| [35] | 2nd trimester | Systolic blood pressure (mmHg)Diastolic blood pressure (mmHg) | NYC African-American | |||||||
| (ln) Birth weight: Beta-coefficient −0.055, p-value = 0.004 | ||||||||||
| (ln) Birth length: Beta-coefficient −0.011, p-value = 0.112 | ||||||||||
| (ln) Birth head circumference: Beta-coefficient −0.010, p-value = 0.125 | ||||||||||
| NYC Dominican | ||||||||||
| (ln) Birth weight: Beta-coefficient 0.018, p-value = 0.094 | ||||||||||
| (ln) Birth length: Beta-coefficient 0.003, p-value = 0.712 | ||||||||||
| (ln) Birth head circumference: Beta-coefficient 0.004, p-value = 0.168 | ||||||||||
| [29] | Krakow: 8th to 24th week of pregnancyNYC: 3rd trimester | Gestational age (weeks), birth weight (g), length (cm) and head circumference (cm) | (ln)Σ8c-PAHs | Not specified | 7/10 | |||||
| Krakow Caucasian | ||||||||||
| (ln) Birth weight: Beta-coefficient −0.02, p-value = 0.007 | ||||||||||
| (ln) Birth length: Beta-coefficient −0.009, p-value = 0.003 | ||||||||||
| (ln) Birth head circumference: Beta-coefficient −0.006, p-value = 0.010 | ||||||||||
| NYC African-American | ||||||||||
| (ln) Birth weight: Beta-coefficient −0.055, p-value = 0.004 | ||||||||||
| (ln) Birth length: Beta-coefficient −0.011, p-value = 0.112 | ||||||||||
| (ln) Birth head circumference: Beta-coefficient −0.010, p-value = 0.125 | ||||||||||
| NYC Dominican | ||||||||||
| (ln) Birth weight: Beta-coefficient 0.018, p-value = 0.094 | ||||||||||
| (ln) Birth length: Beta-coefficient 0.003, p-value = 0.712 | ||||||||||
| (ln) Birth head circumference: Beta-coefficient 0.004, p-value = 0.168 | ||||||||||
| [30] | 3rd trimester | Gestational age (weeks), preterm delivery (n = 20), small for gestational age (n = 53) | (ln)Σ8c-PAHs | * Maternal pre-pregnancy BMI, months of gestational ETS exposure, parity, winter delivery ** BMI, gestational weight gain, months of gestational ETS exposure, parity | 7/10 | |||||
| African- American | ||||||||||
| Gestational age *: Beta- coefficient −0.354 95% CI (−0.714 to 0.006) | ||||||||||
| Preterm delivery *: OR 4.676, 95% CI (1.839 to 11.886) | ||||||||||
| Small for gestational age **: OR 1.94, 95% CI (1.09– 3.47) | ||||||||||
| Dominican | ||||||||||
| Gestational age *: Beta-coefficient −0.006 95% CI (−0.190 to 0.178) | ||||||||||
| Preterm delivery *: OR 0.523, 95% CI (0.182 to 1.504) | ||||||||||
| Small for gestational age **: OR 0.82, 95% CI (0.44–1.51) | ||||||||||
| [31] | 2nd trimester | Birth weight (g) Birth length (cm) Birth head circumference (cm) | Natural log- PAH exposure correlated with the reduction from the mean outcome | Gestational age, gender, parity, maternal pre- pregnancy BMI, and c-section delivery included only for the head circumference | 7/10 | |||||
| Birth weight: Beta-coefficient −67 95% CI (−110 to −23) | ||||||||||
| Birth length: Beta-coefficient −0.48 95% CI (−0.76 to −0.20) | ||||||||||
| Birth head circumference −0.20 95% CI (−0.34 to −0.05) | ||||||||||
| Fetal growth ratio: −1.85 95% CI (−3.09 to −0.60) | ||||||||||
| Ponderal index: 0.01 95% CI (−0.01 to 0.04) | ||||||||||
| Cephalisation index: 1 95% CI (−2 to 4) | ||||||||||
| [39] | 27th week of pregnancy | Birth weight (g), head circumference (mm) and ultrasound examinations of head circumference (mm) and biparietal diameter (mm) between the 29th and 36th gestational weeks and before the 15th gestational week | Benzene exposure (μg/m3) | Gestational age at the examination, sex, maternal passive smoking, urinary cotinine levels, prepregnancy weightm height, parity, maternal occupational exposure to paints or pesticides, month of conception, maternal education, center | 8/10 | |||||
| <1.4 vs. 1.4–2.59 vs. ≥2.6 | ||||||||||
| Birth weight: Beta-coefficient 95%CI | ||||||||||
| 0 vs. −74 (−197 to 50) vs. −90 (−215 to 36) vs. −68 (−135 to −1) | ||||||||||
| Head circumference at birth: Beta-coefficient 95%CI | ||||||||||
| 0 vs. −0.9 (−4.5 to 2.7) vs. −3.7 (−7.3 to 0.0) vs. −1.9 (−3.8 to 0.0) | ||||||||||
| Head circumference the 2nd trimester ultrasound scan: Beta-coefficient 95%CI | ||||||||||
| 0 vs. −1.3 (−4.2 to 1.6) vs. −2.5 (−5.4 to 0.5) vs. −1.5 (−3.1 to 0.0) | ||||||||||
| Biparietal diameter the 2nd trimester ultrasound scan: Beta-coefficient 95%CI | ||||||||||
| 0 vs. −0.5 (−1.5 to 0.5) vs. −1.0 (−2.0 to 0.0) vs. −0.6 (−1.1 to −0.1) | ||||||||||
| [39] | 27th week of pregnancy | Birth weight (g), head circumference (mm) and ultrasound examinations of head circumference (mm) and biparietal diameter (mm) between the 29th and 36th gestational weeks and before the 15th gestational week | Head circumference at the 3rd trimester ultrasound scan: Beta-coefficient 95%CI | |||||||
| 0 vs. −1.6 (−5.4 to 2.3) vs. −4.8 (−8.8 to −0.8) vs. −1.9 (−4.0 to 0.3) | ||||||||||
| Biparietal diameter at the 3rd trimester ultrasound scan: Beta-coefficient 95%CI | ||||||||||
| 0 vs. −0.2 (−1.5 to 1.0) vs. −1.3 (−2.6 to −0.1) vs. −0.6 (−1.2 to 0.1) | ||||||||||
| ln(benzene) | ||||||||||
| Birth weight: Beta-coefficient 95% CI −68 (−135 to −1) | ||||||||||
| Head circumference at birth: Beta-coefficient 95% CI −1.9 (−3.8 to 0.0) | ||||||||||
| [40] | 3rd trimester | Length of gestation (weeks) | Log DEHP exposure (per unit increase) | Maternal ethnicity, maternal age, maternal prepregnancy weight and height, active smoking during pregnancy, prenatal asthma, diabetes, hypertension, planned caesarean section, premature rupture membrane | 7/10 | |||||
| Gestational age: Beta-coefficient −0.15 95% CI (−0.39 to 0.09) | ||||||||||
4. Discussion
5. Conclusions
Author Contributions
Conflicts of Interest
References
- Stillerman, K.P.; Mattison, D.R.; Giudice, L.C.; Woodruff, T.J. Environmental exposures and adverse pregnancy outcomes: A review of the science. Reprod. Sci. 2008, 15, 631–650. [Google Scholar] [CrossRef]
- Kallen, K. Maternal smoking and urinary organ malformations. Int. J. Epidemiol. 1997, 26, 571–574. [Google Scholar] [CrossRef]
- Kallen, K. Maternal smoking during pregnancy and limb reduction malformations in Sweden. Amer. J. Public Health 1997, 87, 29–32. [Google Scholar] [CrossRef]
- Wyszynski, D.F.; Duffy, D.L.; Beaty, T.H. Maternal cigarette smoking and oral clefts: A meta-analysis. Cleft Palate-Craniofac. J. 1997, 34, 206–210. [Google Scholar] [CrossRef]
- Perera, F.P.; Rauh, V.; Whyatt, R.M.; Tsai, W.Y.; Bernert, J.T.; Tu, Y.H.; Andrews, H.; Ramirez, J.; Qu, L.; Tang, D. Molecular evidence of an interaction between prenatal environmental exposures and birth outcomes in a multiethnic population. Environ. Health Perspect. 2004, 112, 626–630. [Google Scholar] [CrossRef]
- Bobak, M. Outdoor air pollution, low birth weight, and prematurity. Environ. Health Perspect. 2000, 108, 173–176. [Google Scholar] [CrossRef]
- Dejmek, J.; Solansky, I.; Benes, I.; Lenicek, J.; Sram, R.J. The impact of polycyclic aromatic hydrocarbons and the particles on pregnancy outcome. Environ. Health Perspect. 2000, 108, 1159–1164. [Google Scholar] [CrossRef]
- Vardavas, C.I.; Chatzi, L.; Patelarou, E.; Plana, E.; Sarri, K.; Kafatos, A.; Koutis, A.D.; Kogevinas, M. Smoking and smoking cessation during early pregnancy and its effect on adverse pregnancy outcomes and fetal growth. Eur. J. Pediatr. 2010, 169, 741–748. [Google Scholar] [CrossRef]
- Stieb, D.M.; Chen, L.; Eshoul, M.; Judek, S. Ambient air pollution, birth weight and preterm birth: A systematic review and meta-analysis. Environ. Res. 2012, 117, 100–111. [Google Scholar] [CrossRef]
- Pedersen, M.; Giorgis-Allemand, L.; Bernard, C.; Aguilera, I.; Andersen, A.M.; Ballester, F.; Beelen, R.M.; Chatzi, L.; Cirach, M.; Danileviciute, A.; et al. Ambient air pollution and low birthweight: A European cohort study (ESCAPE). Lancet Respir. Med. 2013, 1, 695–704. [Google Scholar] [CrossRef]
- Misra, P.; Srivastava, R.; Krishnan, A.; Sreenivaas, V.; Pandac, C.S. Indoor air pollution-related acute lower respiratory infections and low birthweight: A systematic review. J. Trop. Pediat. 2012, 58, 457–466. [Google Scholar] [CrossRef]
- Pope, D.P.; Mishra, V.; Thompson, L.; Siddiqui, R. Risk of low birth weight and stillbirth associated with indoor air pollution from solid fuel use in developing countries. Epidemiol. Rev. 2010, 32, 70–81. [Google Scholar] [CrossRef]
- Feychting, M.; Forssen, U.; Floderus, B. Occupational and residential magnetic field exposure and leukemia and central nervous system tumors. Epidemiology 1997, 8, 384–389. [Google Scholar] [CrossRef]
- Linet, M.S.; Hatch, E.E.; Kleinerman, R.A.; Robison, L.L.; Kaune, W.T.; Friedman, D.R.; Haines, C.M.; Muirhead, C.R.; Boice, J.D.; Robison, L.L. Residential exposure to magnetic fields and acute lymphoblas? Tic leukemia in children. N. Engl. J. Med. 1997, 337, 1–7. [Google Scholar] [CrossRef]
- McBride, M.L.; Gallagher, R.P.; Theriault, G.; Armstrong, B.G.; Tamaro, S.; Spinelli, J.J.; Deadman, J.E.; Fincham, S.; Robson, D.; Choi, W. Power-frequencye lectric and magnetic fields and risk of childhood leukemia in Canada. Amer. J. Epidemiol. 1999, 149, 831–842. [Google Scholar] [CrossRef]
- Savitz, D.A.; Wachtel, H.; Barnes, F.A.; John, E.M.; Tvrdir, J.G. Case-control study of childhood cancer and exposure to 60-Hz magnetic fields. Amer. Epidemiol. 1988, 128, 21–38. [Google Scholar]
- Wu, T.N.; Chen, L.J.; Lai, J.S.; Ko, G.N.; Shen, C.Y.; Chang, P.Y. Prospective study of noise exposure during pregnancy on birth weight. Amer. J. Epidemiol. 1996, 143, 792–796. [Google Scholar] [CrossRef]
- Stroup, D.F.; Berlin, J.A.; Morton, S.C.; Olkin, I.; Williamson, G.D.; Rennie, D.; Moher, D.; Becker, B.J.; Sipe, T.; Thacke, R.S.B. Meta-analysis of observational studies in epidemiology: A proposal for reporting Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. JAMA 2000, 283, 2008–2012. [Google Scholar] [CrossRef]
- Katsoyiannis, A.; Bogdal, C. Interactions between indoor and outdoor air pollution-trends and scientific challenges. Environ. Pollut. 2012, 169, 150–151. [Google Scholar] [CrossRef]
- Dadvand, P.; de Nazelle, A.; Triguero-Mas, M.; Schembari, A.; Cirach, M.; Amoly, E.; Figueras, F.; Basagaña, X.; Ostro, B.; Nieuwenhuijsen, M. Surrounding greenness and exposure to air pollution during pregnancy: An analysis of personal monitoring data. Environ. Health Perspect. 2012, 120, 1286–1290. [Google Scholar] [CrossRef]
- Nethery, E.; Brauer, M.; Janssen, P. Time activity patterns of pregnant women and changes during the course of pregnancy. J. Expo. Sci. Environ. Epidemiol. 2009, 19, 317–324. [Google Scholar] [CrossRef]
- Critical Appraisal Skills Programme: 12 Questions to Help you Make Sense of Cohort Study. Available online: http://media.wix.com/ugd/dded87_36c5c76519f7bf14731ed1985e8e9798.pdf (accessed on 26 May 2014).
- Critical Appraisal Skills Programme: 12 Questions to Help You Make Sense of Case Control Study. Available online: http://media.wix.com/ugd/dded87_19dd1d558a9977c0e0b30cedf86a9da7.pdf (accessed on 26 May 2014).
- Juutilainen, J.; Matilainen, P.; Saarikoski, S.; Laara, E.; Suonio, S. Early pregnancy loss and exposure to 50-Hz magnetic fields. Bioelectromagnetics 1993, 14, 229–236. [Google Scholar] [CrossRef]
- Lindbohm, M.L.; Hietanen, M.; Kyyronen, P.; Sallmen, M.; von Nandelstadh, P.; Taskinen, H.; Pekkarinen, M.; Ylikoski, M.; Hemminki, K. Magnetic fields of video display terminals and spontaneous abortion. Amer. J. Epidemiol. 1992, 136, 1041–1051. [Google Scholar]
- Savitz, D.A.; Ananth, C.V. Residential magnetic fields, wire codes, and pregnancy outcome. Bioelectromagnetics 1994, 15, 271–273. [Google Scholar] [CrossRef]
- Schnorr, T.M.; Grajewski, B.A.; Hornung, R.W. Video display terminals and the risk of spontaneous abortion. N. Engl. J. Med. 1991, 324, 727–373. [Google Scholar] [CrossRef]
- Bracken, M.B.; Belanger, K.; Hellenbrand, K. Exposure to electromagnetic fields during pregnancy with emphasis on electrically heated beds: Association with birthweight and intrauterine growth retardation. Epidemiology 1995, 6, 263–270. [Google Scholar] [CrossRef]
- Choi, H.; Jedrychowski, W.; Spengler, J.; Camann, D.E. International studies of prenatal exposure to polycyclic aromatic hydrocarbons and fetal growth. Environ. Health Perspect. 2006, 114, 1744–1750. [Google Scholar]
- Choi, H.; Rauh, V.; Garfinkel, R.; Tu, Y.; Perera, F.P. Prenatal exposure to airborne polycyclic aromatic hydrocarbons and risk of intrauterine growth restriction. Environ. Health Perspect. 2008, 116, 658–665. [Google Scholar] [CrossRef]
- Choi, H.; Wang, L.; Lin, X.; Spengler, J.D.; Perera, F.P. Fetal window of vulnerability to airborne polycyclic aromatic hydrocarbons on proportional intrauterine growth restriction. PLoS One 2012, 7. [Google Scholar] [CrossRef]
- Jedrychowski, W.; Bendkowska, I.; Flak, E.; Penar, A.; Jacek, R.; Kaim, I.; Spengler, J.D.; Camann, D.; Perera, F.P. Estimated risk for altered fetal growth resulting from exposure to fine particles during pregnancy: An epidemiologic prospective cohort study in Poland. Environ. Health Perspect. 2004, 112, 1398–1402. [Google Scholar] [CrossRef]
- Jedrychowski, W.; Masters, E.; Choi, H.; Sochacka, E.; Flak, E.; Mroz, E.; Pac, A.; Jacek, R.; Kaim, I.; Skolicki, Z.; et al. Pre-pregnancy dietary vitamin A intake may alleviate the adverse birth outcomes associated with prenatal pollutant exposure: Epidemiologic cohort study in Poland. Int. J. Occup. Environ. Health 2007, 13, 175–180. [Google Scholar] [CrossRef]
- Jedrychowski, W.; Perera, F.; Mrozek-Budzyn, D.; Mroz, E.; Flak, E.; Spengler, J.D.; Edwards, S.; Jacek, R.; Kaim, I.; Skolicki, Z. Gender differences in fetal growth of newborns exposed prenatally to airborne fine particulate matter. Environ. Res. 2009, 109, 447–456. [Google Scholar] [CrossRef]
- Jedrychowski, W.A.; Perera, F.P.; Maugeri, U.; Spengler, J.; Mroz, E.; Flak, E.; Stigter, L.; Majewska, R.; Kaim, I.; Sowa, A.; et al. Prohypertensive effect of gestational personal exposure to fine particulate matter. Prospective cohort study in non-smoking and non-obese pregnant women. Cardiovasc. Toxicol. 2012, 12, 216–225. [Google Scholar] [CrossRef]
- Lee, G.M.; Neutra, R.R.; Hristova, L.; Yost, M.; Hiatt, R.A. A nested case-control study of residential and personal magnetic field measures and miscarriages. Epidemiology 2002, 13, 21–31. [Google Scholar] [CrossRef]
- Li, D.K.; Odouli, R.; Wi, S.; Janevic, T.; Golditch, I.; Bracken, T.D.; Senior, R.; Rankin, R.; Iriye, R. A population-based prospective cohort study of personal exposure to magnetic fields during pregnancy and the risk of miscarriage. Epidemiology 2002, 13, 9–20. [Google Scholar] [CrossRef]
- Perera, F.P.; Rauh, V.; Tsai, W.Y.; Kinney, P.; Camann, D.; Barr, D.; Bernert, T.; Garfinkel, R.; Tu, Y.H.; Diaz, D.; et al. Effects of transplacental exposure to environmental pollutants on birth outcomes in a multiethnic population. Environ. Health Perspect. 2003, 111, 201–205. [Google Scholar]
- Slama, R.; Thiebaugeorges, O.; Goua, V.; Aussel, L.; Sacco, P.; Bohet, A.; Forhan, A.; Ducot, B.; Annesi-Maesano, I.; Heinrich, J.; et al. Maternal personal exposure to airborne benzene and intrauterine growth. Environ. Health Perspect. 2009, 117, 1313–1321. [Google Scholar] [CrossRef]
- Whyatt, R.M.; Adibi, J.J.; Calafat, A.M.; Camann, D.E.; Rauh, V.; Bhat, H.K.; Perera, F.P.; Andrews, H.; Just, A.C.; Hoepner, L.; et al. Prenatal di(2-ethylhexyl)phthalate exposure and length of gestation among an inner-city cohort. Pediatrics 2009, 124, 1213–1220. [Google Scholar] [CrossRef]
- Kannan, S.; Misra, D.P.; Dvonch, J.T.; Krishnakumar, A. Exposures to airborne particulate matter and adverse perinatal outcomes: A biologically plausible mechanisticframework for exploring potential effect modification by nutrition. Environ. Health Perspect. 2006, 114, 1636–1642. [Google Scholar]
- Van den Hooven, E.H.; Pierik, F.H.; de Kluizenaar, Y.; Willemsen, S.P.; Hofman, A.; van Ratingen, S.W.; Zandveld, P.Y.; Mackenbach, J.P.; Steegers, E.A.; Miedema, H.M.; et al. Air pollution exposure during pregnancy, ultrasound measures of fetal growth, and adverse birth outcomes: A prospective cohort study. Environ. Health Perspect. 2012, 120, 150–156. [Google Scholar]
- Bostrom, C.E.; Gerde, P.; Hanberg, A.; Jernstrom, B.; Johansson, C.; Kyrklund, T.; Rannug, A.; Törnqvist, M.; Victorin, K.; Westerholm, R. Cancer risk assessment, indicators, and guidelines for polycyclic aromatic hydrocarbons in the ambient air. Environ. Health Perspect. 2002, 110, S451–S488. [Google Scholar] [CrossRef]
- Duarte-Salles, T.; Mendez, M.A.; Pessoa, V.; Guxens, M.; Aguilera, I.; Kogevinas, M.; Sunyer, J. Smoking during pregnancy is associated with higher dietary intake of polycyclic aromatic hydrocarbons and poordiet quality. Public Health Nutr. 2010, 13, 2034–2043. [Google Scholar] [CrossRef]
- Bocskay, K.A.; Tang, D.; Orjuela, M.A.; Liu, X.; Warburton, D.P.; Perera, F.P. Chromosomal aberrations in cord blood are associated with prenatal exposure to carcinogenic polycyclic aromatic hydrocarbons. Cancer Epidemiol. Biomark. Prev. 2005, 14, 506–511. [Google Scholar] [CrossRef]
- Ilgen, E.; Levsen, K.; Angerer, J.; Schneider, P.; Heinrich, J.; Wichmann, H.E. Aromatic hydrocarbons in the atmospheric environment. Part III: Personal monitoring. Atmos. Environ. 2001, 35, 1265–1279. [Google Scholar] [CrossRef]
- Bruinen de Bruin, Y.; Koistinen, K.; Kephalopoulos, S.; Geiss, O.; Tirendi, S.; Kotzias, D. Characterisation of urban inhalation exposures to benzene, formaldehyde and acetaldehyde in the European Union: Comparison of measured and modelled exposure data. Environ. Sci. Pollut. Res. Int. 2008, 15, 417–430. [Google Scholar] [CrossRef]
- Ilgen, E.; Levsen, K.; Angerer, J.; Schneide, R.P.; Heinrich, J.; Wichmann, H.E. Aromatic hydrocarbons in the atmospheric environment. Part II: Univariate and multivariate analysis and case studies of indoor concentrations. Atmos. Environ. 2001, 35, 1253–1264. [Google Scholar] [CrossRef]
- Zuurbier, M.; Hoek, G.; Oldenwening, M.; Lenters, V.; Meliefste, K.; van den Hazel, P.; Brunekreef, B. Commuters’ exposure to particulate matter air pollution is affected by mode of transport, fuel type, and route. Environ. Health Perspect. 2010, 118, 783–789. [Google Scholar] [CrossRef]
- Zuurbier, M.; Hoek, G.; Oldenwening, M.; Meliefste, K.; van den Hazel, P.; Brunekreef, B. Respiratory effects of commuters’ exposure to air pollution in traffic. Epidemiology 2011, 22, 219–227. [Google Scholar] [CrossRef]
- Morawska, L.; Afshari, A.; Bae, G.N.; Buonanno, G.; Chao, C.Y.; Hanninen, O.; Hofmann, W.; Isaxon, C.; Jayarante, E.R.; Pasane, P.; et al. Indoor aerosols: From personal exposure to risk assessment. Indoor Air 2013, 23, 462–487. [Google Scholar] [CrossRef] [Green Version]
- Kelly, F.J.; Fuller, G.W.; Walton, H.A.; Fussell, J.C. Monitoring air pollution: Use of early warning systems for public health. Respirology 2012, 17, 7–19. [Google Scholar] [CrossRef]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Patelarou, E.; Kelly, F.J. Indoor Exposure and Adverse Birth Outcomes Related to Fetal Growth, Miscarriage and Prematurity—A Systematic Review. Int. J. Environ. Res. Public Health 2014, 11, 5904-5933. https://doi.org/10.3390/ijerph110605904
Patelarou E, Kelly FJ. Indoor Exposure and Adverse Birth Outcomes Related to Fetal Growth, Miscarriage and Prematurity—A Systematic Review. International Journal of Environmental Research and Public Health. 2014; 11(6):5904-5933. https://doi.org/10.3390/ijerph110605904
Chicago/Turabian StylePatelarou, Evridiki, and Frank J. Kelly. 2014. "Indoor Exposure and Adverse Birth Outcomes Related to Fetal Growth, Miscarriage and Prematurity—A Systematic Review" International Journal of Environmental Research and Public Health 11, no. 6: 5904-5933. https://doi.org/10.3390/ijerph110605904