Towards a Conceptual Model of Diabetes Self-Management among Chinese Immigrants in the United States

{kind=link}
Abstract
:1. Introduction
2. Background
3. Experimental Section
3.1. Data Sources
3.2. Search Outcomes
4. Results
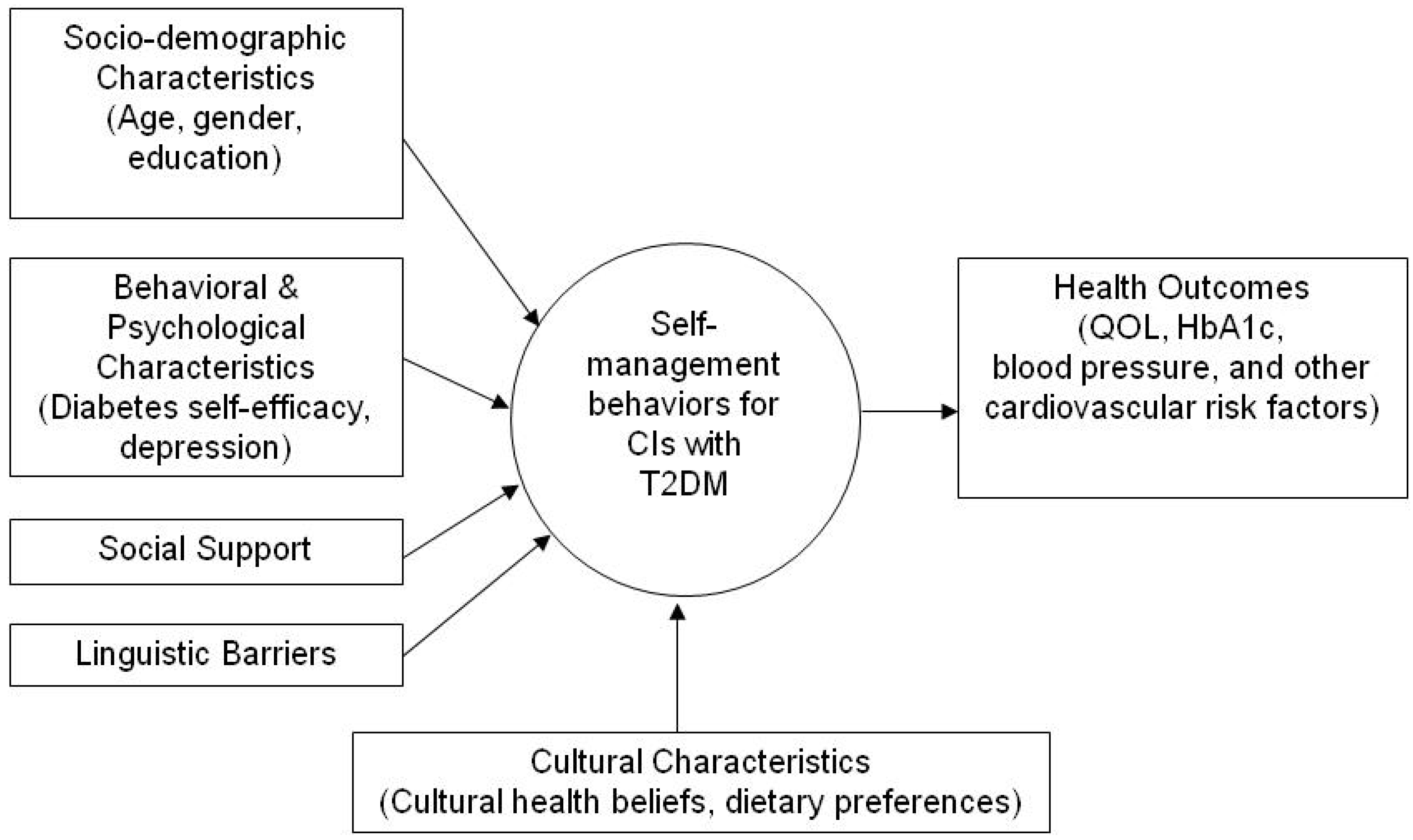
4.1. The Conceptual Model

4.1.1. T2DM Self-Management
4.1.2. Socio-Demographic Characteristics
Age
Gender
Education
4.1.3. Behavioral and Psychological Characteristics
Diabetes Self-Efficacy
Depression
4.1.4. Social Support
4.1.5. Linguistic Barriers
4.1.6. Cultural Characteristics
Cultural Health Beliefs
Dietary Preferences
4.1.7. Health Outcomes
QOL
HbA1c
Blood Pressure and Other Cardiovascular Risk Factors
5. Discussion
6. Conclusion
Acknowledgements
Author Contributions
Conflicts of Interest
References
- World Health Organization. Diabetes 2013. Available online: http://www.who.int/mediacentre/factsheets/fs312/ en/index.html (accessed on 8 April 2013).
- Rajpathak, S.N.; Wylie-Rosett, J. High prevalence of diabetes and impaired fasting glucose among Chinese immigrants in New York City. J. Immigr. Minor. Health 2011, 13, 181–183. [Google Scholar] [CrossRef]
- Oza-Frank, R.; Stephenson, R.; Narayan, K.M. Diabetes prevalence by length of residence among US immigrants. J. Immigr. Minor. Health 2011, 13, 1–8. [Google Scholar] [CrossRef]
- Glasgow, R.E.; Anderson, R.M. In diabetes care, moving from compliance to adherence is not enough. Something entirely different is needed. Diabetes Care 1999, 22, 2090–2092. [Google Scholar] [CrossRef]
- Grey, M.; Knafl, K.; McCorkle, R. A framework for the study of self- and family management of chronic conditions. Nurs. Outlook 2006, 54, 278–286. [Google Scholar] [CrossRef]
- Wang, Y.; Chuang, L.; Bateman, W.B. Focus group study assessing self-management skills of Chinese Americans with type 2 diabetes mellitus. J. Immigr. Minor. Health 2012, 14, 869–874. [Google Scholar] [CrossRef]
- Washington, G.; Wang-Letzkus, M.F. Self-care practices, health beliefs, and attitudes of older diabetic Chinese Americans. J. Health Hum. Serv. Adm. 2009, 32, 305–323. [Google Scholar]
- United States Census Bureau. The Asian Population: 2010. Available online: http://www.census.gov/prod/cen2010/briefs/c2010br-11.pdf (accessed on 12 May 2014).
- Jacob, M.; Cho, L. Asian Americans and cardiometabolic risk why and how to study them. J. Am. Coll. Cardiol. 2010, 55, 974–975. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. National Diabetes Fact Sheet 2007: General Information; US Department of Health and Human Services, Centers for Disease Control and Prevention: Atlanta, GA, USA, 2007.
- King, G.L.; McNeely, M.J.; Thorpe, L.E.; Mau, M.I.M.; Ko, J.; Liu, L.L.; Sun, A.; Hsu, W.C.; Chow, E.A. Understanding and addressing unique needs of diabetes in Asian Americans, Native Hawaiians, and Pacific Islanders. Diabetes Care 2012, 35, 1181–1188. [Google Scholar] [CrossRef]
- Lee, J.W.; Brancati, F.L.; Yeh, H.C. Trends in the prevalence of type 2 diabetes in Asians versus whites: Results from the United States National Health Interview Survey, 1997–2008. Diabetes Care 2011, 34, 353–357. [Google Scholar] [CrossRef]
- McNeely, M.J.; Boyko, E.J. Type 2 diabetes prevalence in Asian Americans: Results of a national health survey. Diabetes Care 2004, 27, 66–69. [Google Scholar] [CrossRef]
- US Department of Health and Human Service. The Diabetic Epidemic among Hispanics/Latinos. 2011a. Available online: http://ndep.nih.gov/media/FS_HispLatino_Eng.pdf. (accessed on 7 April 2013). [Google Scholar]
- US Department of Health and Human Service. The diabetic epidemic among African Americans. 2011b. Available online: http://www.ndep.nih.gov/media/FS_AfricanAm.pdf?redirect=true. (accessed on 7 April 2013). [Google Scholar]
- Tseng, J.; Halperin, L.; Ritholz, M.D.; Hsu, W.C. Perceptions and management of psychosocial factors affecting type 2 diabetes mellitus in Chinese Americans. J. Diabetes Complications 2013, 27, 383–390. [Google Scholar] [CrossRef]
- Ramachandran, A.; Ma, R.C.; Snehalatha, C. Diabetes in Asia. Lancet 2010, 375, 408–418. [Google Scholar] [CrossRef]
- Xu, Y.; Pan, W.; Liu, H. Self-management practices of Chinese Americans with type 2 diabetes. Nurs. Health Sci. 2010, 12, 228–234. [Google Scholar] [CrossRef]
- Chun, K.M.; Chesla, C.A. Cultural issues in disease management for Chinese Americans with type 2 diabetes. Psychol. Health 2004, 19, 767–785. [Google Scholar] [CrossRef]
- Walker, L.O.; Avant, K.C. Strategies for Theory Construction in Nursing, 4th ed.; Pearson Prentice Hall: New Jersey, NJ, USA, 2005. [Google Scholar]
- Liu, T. A concept analysis of self-efficacy among Chinese elderly with diabetes mellitus. Nurs. Forum. 2012, 47, 226–235. [Google Scholar] [CrossRef]
- Chesla, C.A.; Chun, K.M. Accommodating type 2 diabetes in the Chinese American family. Qual. Health Res. 2005, 15, 240–255. [Google Scholar] [CrossRef]
- Haas, L.; Maryniuk, M.; Beck, J.; Cox, C.E.; Duker, P.; Edwards, L.; Fisher, E.B.; Hanson, L.; Kent, D; Kolb, L.; et al. National standards for diabetes self-management education and support. Diabetes Care 2013, 36, S100–S108. [Google Scholar] [CrossRef]
- Norris, S.L.; Lau, J.; Smith, S.J.; Schmid, C.H.; Engelgau, M.M. Self-management education for adults with type 2 diabetes: A meta-analysis of the effect on glycemic control. Diabetes Care 2002, 25, 1159–1171. [Google Scholar]
- Xu, Y.; Pan, W.; Liu, H. The role of acculturation in diabetes self-management among Chinese Americans with type 2 diabetes. Diabetes Res. Clin. Pract. 2011, 93, 363–370. [Google Scholar] [CrossRef]
- Bandura, A. Self-efficacy: Toward a unifying theory of behavioral change. Psychol. Rev. 1977, 84, 191–215. [Google Scholar] [CrossRef]
- Hurley, A.C.; Shea, C.A. Self-efficacy: Strategy for enhancing diabetes self-care. Diabetes Educ. 1992, 18, 146–150. [Google Scholar] [CrossRef]
- Wu, S.F.; Courtney, M.; Edwards, H.; McDowell, J.; Shortridge-Baggett, L.M.; Chang, P.J. Self-efficacy, outcome expectations and self-care behaviour in people with type 2 diabetes in Taiwan. J. Clin. Nurs. 2007, 16, 250–257. [Google Scholar] [CrossRef]
- Sarkar, U.; Fisher, L.; Schillinger, D. Is self-efficacy associated with diabetes self-management across race/ethnicity and health literacy? Diabetes Care 2006, 29, 823–829. [Google Scholar] [CrossRef]
- Bandura, A. Social Foundations of Thought and Action: A Social Cognitive Theory; Prentice-Hall Inc.: New Jersey, NJ, USA, 1986. [Google Scholar]
- Mishali, M.; Omer, H.; Heymann, A.D. The importance of measuring self-efficacy in patients with diabetes. Fam. Pract. 2011, 28, 82–87. [Google Scholar] [CrossRef]
- Ali, S.; Stone, M.A.; Peters, J.L.; Davies, M.J.; Khunti, K. The prevalence of co-morbid depression in adults with type 2 diabetes: A systematic review and meta-analysis. Diabet. Med. 2006, 23, 1165–1173. [Google Scholar] [CrossRef]
- Ciechanowski, P.S.; Katon, W.J.; Russo, J.E. Depression and diabetes: Impact of depressive symptoms on adherence, function, and costs. Arch. Intern. Med. 2000, 160, 3278–3285. [Google Scholar] [CrossRef]
- Gonzalez, J.S.; Safren, S.A.; Delahanty, L.M.; Cagliero, E.; Wexler, D.J.; Meigs, J.B.; Grant, R.W. Symptoms of depression prospectively predict poorer self-care in patients with type 2 diabetes. Diabet. Med. 2008, 25, 1102–1107. [Google Scholar] [CrossRef]
- Lin, E.H.; Katon, W.; Von Korff, M.; Rutter, C.; Simon, G.E.; Oliver, M.; Ciechanowski, P.; Ludman, E.J.; Bush, T.; Young, B. Relationship of depression and diabetes self-care, medication adherence, and preventive care. Diabetes Care 2004, 27, 2154–2160. [Google Scholar] [CrossRef]
- Chen, Y.H.; Caine, R.M.; Wang, M.F. Depression in Chinese immigrants. Overcoming the cultural stronghold on symptom report. Adv. Nurse Pract. 2009, 17, 35–38. [Google Scholar]
- Chung, I. Changes in the sociocultural reality of Chinese immigrants: Challenges and opportunities in help-seeking behaviour. Int. J. Soc. Psychiatr. 2010, 56, 436–447. [Google Scholar] [CrossRef]
- Bakan, G.; Akyol, A.D. Theory-guided interventions for adaptation to heart failure. J. Adv. Nurs. 2008, 61, 596–608. [Google Scholar] [CrossRef]
- Gallant, M.P. The influence of social support on chronic illness self-management: A review and directions for research. Health Educ. Behav. 2003, 30, 170–195. [Google Scholar] [CrossRef]
- Van Dam, H.A.; van der Horst, F.G.; Knoops, L.; Ryckman, R.M.; Crebolder, H.F.; van den Borne, B.H. Social support in diabetes: A systematic review of controlled intervention studies. Patient Educ. Couns. 2005, 59, 1–12. [Google Scholar] [CrossRef]
- Kwan, C.M.; Mullan, J.T.; Chun, K.M.; Kwong, Y.; Hsu, L.; Chesla, C.A. Social relationships and health among Chinese Americans: Does age make a difference? Clin. Gerontol. 2014, 37, 191–210. [Google Scholar] [CrossRef]
- Chun, K.M.; Chesla, C.A.; Kwan, C.M. “So We Adapt Step by Step”: Acculturation experiences affecting diabetes management and perceived health for Chinese American immigrants. Soc. Sci. Med. 2011, 72, 256–264. [Google Scholar] [CrossRef]
- Fisher, L.; Chesla, C.A.; Chun, K.M.; Skaff, M.M.; Mullan, J.T.; Kanter, R.A.; Gardiner, P.S. Patient-appraised couple emotion management and disease management among Chinese American patients with type 2 diabetes. J. Fam. Psychol. 2004, 18, 302–310. [Google Scholar] [CrossRef]
- Fisher, L. Family, ethnicity, and chronic disease: An ongoing story with a new twist. Fam. Syst. Health 2005, 23, 293–306. [Google Scholar] [CrossRef]
- Rosland, A.M.; Kieffer, E.; Israel, B.; Cofield, M.; Palmisano, G.; Sinco, B.; Spencer, M.; Heisler, M. When is social support important? The association of family support and professional support with specific diabetes self-management behaviors. J. Gen. Intern. Med. 2008, 23, 1992–1999. [Google Scholar] [CrossRef]
- Shaw, B.A.; Gallant, M.P.; Riley-Jacome, M.; Spokane, L.S. Assessing sources of support for diabetes self-care in urban and rural underserved communities. J. Community Health 2006, 31, 393–412. [Google Scholar] [CrossRef]
- Hsu, W.C.; Cheung, S.; Ong, E.; Wong, K.; Lin, S.; Leon, K.; Weinger, K.; King, G.L. Identification of linguistic barriers to diabetes knowledge and glycemic control in Chinese Americans with diabetes. Diabetes Care 2006, 29, 415–416. [Google Scholar] [CrossRef]
- Fisher, L.; Skaff, M.M.; Chesla, C.A.; Chun, K.M.; Mullan, J.T.; Kanter, R.A.; Gardiner, P.S. Disease management advice provided to African-American and Chinese-American patients with type 2 diabetes. Diabetes Care 2004, 27, 2249–2250. [Google Scholar]
- Ngo-Metzger, Q.; Massagli, M.P.; Clarridge, B.R.; Manocchia, M.; Davis, R.B.; Lezzoni, L.I.; Phillips, R.S. Linguistic and cultural barriers to care. J. Gen. Intern. Med. 2003, 18, 44–52. [Google Scholar] [CrossRef]
- Holmstrom, I.M.; Rosenqvist, U. Misunderstandings about illness and treatment among patients with type 2 diabetes. J. Adv. Nurs. 2005, 49, 146–154. [Google Scholar] [CrossRef]
- Andrews, M.M.; Boyle, J.S. Transcultural Concepts in Nursing Care, 5th ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2008. [Google Scholar]
- Ma, G. The Culture of Health: Asian Communities in the United States; Bergin & Garvey: CT, USA, 1999. [Google Scholar]
- Chesla, C.A.; Chun, K.M.; Kwan, C.M. Cultural and family challenges to managing type 2 diabetes in immigrant Chinese Americans. Diabetes Care 2009, 32, 1812–1816. [Google Scholar] [CrossRef]
- Kong, H.; Hsieh, E. The social meanings of traditional Chinese medicine: elderly Chinese immigrants’ health practice in the United States. J. Immigr. Minor. Health 2012, 14, 841–849. [Google Scholar] [CrossRef]
- Ho, E.Y.; Tran, H.; Chesla, C.A. Assessing the Cultural in Culturally Sensitive Printed Patient-education Materials for Chinese Americans with Type 2 Diabetes. Available online: http://www.tandfonline.com/doi/abs/10.1080/10410236.2013.835216#.U6FFeChZSqI (accessed on 21 January 2014).
- Ho, E.Y.; Chesla, C.A.; Chun, K.M. Health communication with Chinese Americans about type 2 diabetes. Diabetes Educ. 2012, 38, 67–76. [Google Scholar]
- Polonsky, W.H. Understanding and assessing diabetes-specific quality of life. Diabetes Spectrum. 2000, 13, 36–41. [Google Scholar]
- Cochran, J.; Conn, V.S. Meta-analysis of quality of life outcomes following diabetes self-management training. Diabetes Educ. 2008, 34, 815–823. [Google Scholar] [CrossRef]
- Huang, M.C.; Hung, C.H. Quality of life and its predictors for middle-aged and elderly patients with type 2 diabetes mellitus. J. Nurs. Res. 2007, 15, 193–201. [Google Scholar] [CrossRef]
- Skelly, A.H.; Carlson, J.; Leeman, J.; Soward, A.; Burns, D. Controlled trial of nursing interventions to improve health outcomes of older African American women with type 2 diabetes. Nurs. Res. 2009, 58, 410–418. [Google Scholar] [CrossRef]
- Wang, C.Y.; Chan, S.M. Culturally tailored diabetes education program for Chinese Americans: A pilot study. Nurs. Res. 2005, 54, 347–353. [Google Scholar] [CrossRef]
- Chesla, C.A.; Chun, K.M.; Kwan, C.M.; Mullan, J.T.; Kwong, Y.; Hsu, L.; Huang, P.; Strycker, L.A.; Shum, T.; To, D.; et al. Testing the efficacy of culturally adapted coping skills training for Chinese American immigrants with type 2 diabetes using community-based participatory research. Res. Nurs. Health 2013, 36, 359–372. [Google Scholar] [CrossRef]
- American Diabetes Assocociation. Standards of medical care in diabetes-2013. Diabetes Care 2013, 36, S11–S66. [Google Scholar] [CrossRef]
- Nathan, D.M.; Buse, J.B.; Davidson, M.B.; Ferrannini, E.; Holman, R.R.; Sherwin, R.; Zinman, B. Medical management of hyperglycemia in type 2 diabetes: A consensus algorithm for the initiation and adjustment of therapy a consensus statement of the American Diabetes Association and the European Association for the Study of Diabetes. Diabetes Care 2009, 32, 193–203. [Google Scholar] [CrossRef]
- Hartz, A.; Kent, S.; James, P.; Xu, Y.H.; Kelly, M.; Daly, J. Factors that influence improvement for patients with poorly controlled type 2 diabetes. Diabetes Res. Clin. Pr. 2006, 74, 227–232. [Google Scholar] [CrossRef]
- Heisler, M.; Smith, D.M.; Hayward, R.A.; Krein, S.L.; Kerr, E.A. How well do patients’ assessments of their diabetes self-management correlate with actual glycemic control and receipt of recommended diabetes services? Diabetes Care 2003, 26, 738–743. [Google Scholar] [CrossRef]
- Sousa, V.D.; Zauszniewski, J.A.; Musil, C.M.; Price Lea, P.J.; Davis, D.A. Relationships among self-care agency, self-efficacy, self-care, and glycemic control. Res. Theory Nurs. Pract. 2005, 19, 217–230. [Google Scholar] [CrossRef]
- Jones, H.; Edwards, L.; Vallis, T.M.; Ruggiero, L.; Rossi, S.R.; Rossi, J.S.; Greene, G.; Prochaska, J.O.; Zinman, B. Changes in diabetes self-care behaviors make a difference in glycemic control—The Diabetes Stages of Change (DiSC) study. Diabetes Care 2003, 26, 732–737. [Google Scholar] [CrossRef]
- Sun, A.C.; Tsoh, J.Y.; Saw, A.; Chan, J.L.; Cheng, J.W. Effectiveness of a culturally tailored diabetes self-management program for Chinese Americans. Diabetes Educ. 2012, 38, 685–694. [Google Scholar] [CrossRef]
- Palaniappan, L.P.; Araneta, M.R.; Assimes, T.L.; Barrett-Connor, E.L.; Carnethon, M.R.; Criqui, M.H.; Fung, G.L.; Narayan, K.M.V.; Patel, H.; Taylor-Piliae, R.E.; et al. Call to action: Cardiovascular disease in Asian Americans A science advisory from the American Heart Association. Circulation 2010, 122, 1242–1252. [Google Scholar] [CrossRef]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Zeng, B.; Sun, W.; Gary, R.A.; Li, C.; Liu, T. Towards a Conceptual Model of Diabetes Self-Management among Chinese Immigrants in the United States. Int. J. Environ. Res. Public Health 2014, 11, 6727-6742. https://doi.org/10.3390/ijerph110706727
Zeng B, Sun W, Gary RA, Li C, Liu T. Towards a Conceptual Model of Diabetes Self-Management among Chinese Immigrants in the United States. International Journal of Environmental Research and Public Health. 2014; 11(7):6727-6742. https://doi.org/10.3390/ijerph110706727
Chicago/Turabian StyleZeng, Bin, Wenjie Sun, Rebecca A. Gary, Changwei Li, and Tingting Liu. 2014. "Towards a Conceptual Model of Diabetes Self-Management among Chinese Immigrants in the United States" International Journal of Environmental Research and Public Health 11, no. 7: 6727-6742. https://doi.org/10.3390/ijerph110706727