Climate Change and Cerebrospinal Meningitis in the Ghanaian Meningitis Belt

{kind=link}
{kind=link}
Abstract
:1. Introduction
1.1. Overview of Cerebrospinal Meningitis

1.2. Cerebrospinal Meningitis in Ghana
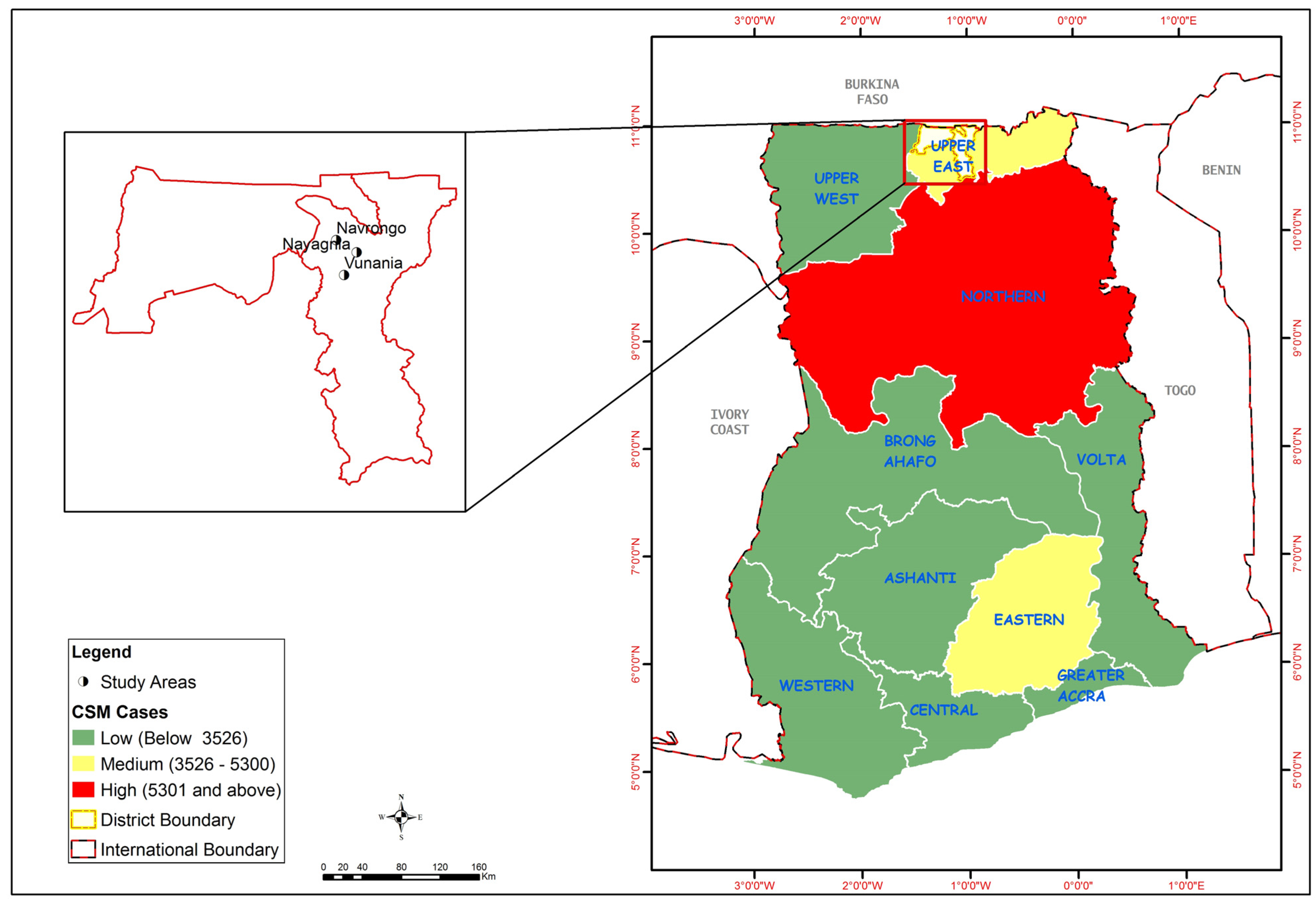
1.3. Study Area
2. Methodology
2.1. Data
2.2. Method of Analysis
3. Results and Discussion
3.1. Public Perceptions of Climate Change and CSM Prevalence
The weather is now not stable and I cannot predict when the seasons will start and end. Some years ago, the rains would start in early May as the latest and end in October, then the harmattan season will start in October and end around February, and the dry season continues from March to late May. But now I cannot tell. This is seriously affecting us. Because we rely on the rains for farming and the dry season to sell our farm produce. Besides, the temperature during the dry season is increasing every year.
The rain does not fall at the correct time these days. It will fall at a time when you don’t expect it to fall. These days it also falls very much when we don’t expect it. I think, the rainfall pattern has changed. At one time you experience very heavy rainfall over a very long time which leads to floods, and at other times it only drizzles over a couple of days, causing droughts and dusty conditions. These are the challenges we are facing in this community and we cannot do anything about it.
Climate change is real in Navrongo. Over the course of the 25 years that I have worked at this station, I have observed a progressive rise in temperature and decrease in mean annual rainfall. Climate change is therefore happening all around us due to rising temperatures; declining rainfall totals and increased variability; high incidence of weather extremes and disasters.
Most communities here are prone to CSM because of their location near the Sahelian region, which is CSM-endemic. CSM mostly assumes endemic proportions when the Ghana Health Service fails to vaccinate people before the start of the dry season. In that case, the heat and congestion in most compounds serve as a conducive atmosphere for the disease to thrive given that the people possess very little capacity to prevent the occurrence of the disease.
Well, everybody here can associate CSM with temperature and rainfall, but some of us still believe that the disease is a curse from our forefathers on people who fail to honour them or those who disobey the gods. I remember a young boy once insulted the gods when he was brought before them to apologise for an offense he had committed. He refused to apologise and before we knew it he was afflicted by the disease and he died. Some of us still believe that the disease is from our ancestors. Once we stop offending them, they will also stop infecting our children and generations yet to come with the disease.
For us we have observed that in recent years the heat becomes so severe, and that is when we experience a lot of CSM cases. It happened some few years back when the meteorological officer told us that temperatures for the first time went up to 48 °C. A number of people in this community were attacked by the disease.
Unlike malaria which occurs at any time of the year, CSM is the only disease which attacks us during the dry season, and in years when the heat becomes very severe. One thing we still do not understand is that the disease also affects us the poor people and our children.
3.2. Adaptation Strategies
3.2.1. Reactive Adaptation: Annual Mass CSM Immunization, Moderation of Socio-cultural Activities that Result in Mass Gathering and Movement Restrictions on Carriers
We thank the government for the annual vaccination which is done in the dry season against CSM. This is helping us and saving the lives of our children, brothers, sisters and community members who used to die when there is an outbreak. Now we are not afraid of the disease like in the past.
The vaccinations have been very helpful in fighting the disease in this community, especially when they do it before the beginning of the dry season. They are however not able to solve the problem completely when they delay in the vaccination before the outbreak occurs. I say this because my son died of the disease whilst on admission at the hospital in Navrongo some ten years ago.
The leaders of this community always meet and place bans on the performance of funerals and other communal social-cultural activities when they detect that there is an outbreak of CSM. Through this action, they are always able to control huge gatherings and therefore further spread of the disease. An example is the year 2001 when the leaders temporary placed a ban on the performance of funerals in the community because of a CSM outbreak. Though people could not perform their funerals, this helped a great deal to prevent the spread of the disease.We as community leaders always have a responsibility to protect our people. As a result, we have set up community bye-laws that temporarily place a restriction on the movement of people suspected of having CSM. In this way, we have managed to reduce the spread of CSM for the last ten years, since the last epidemic was experienced.
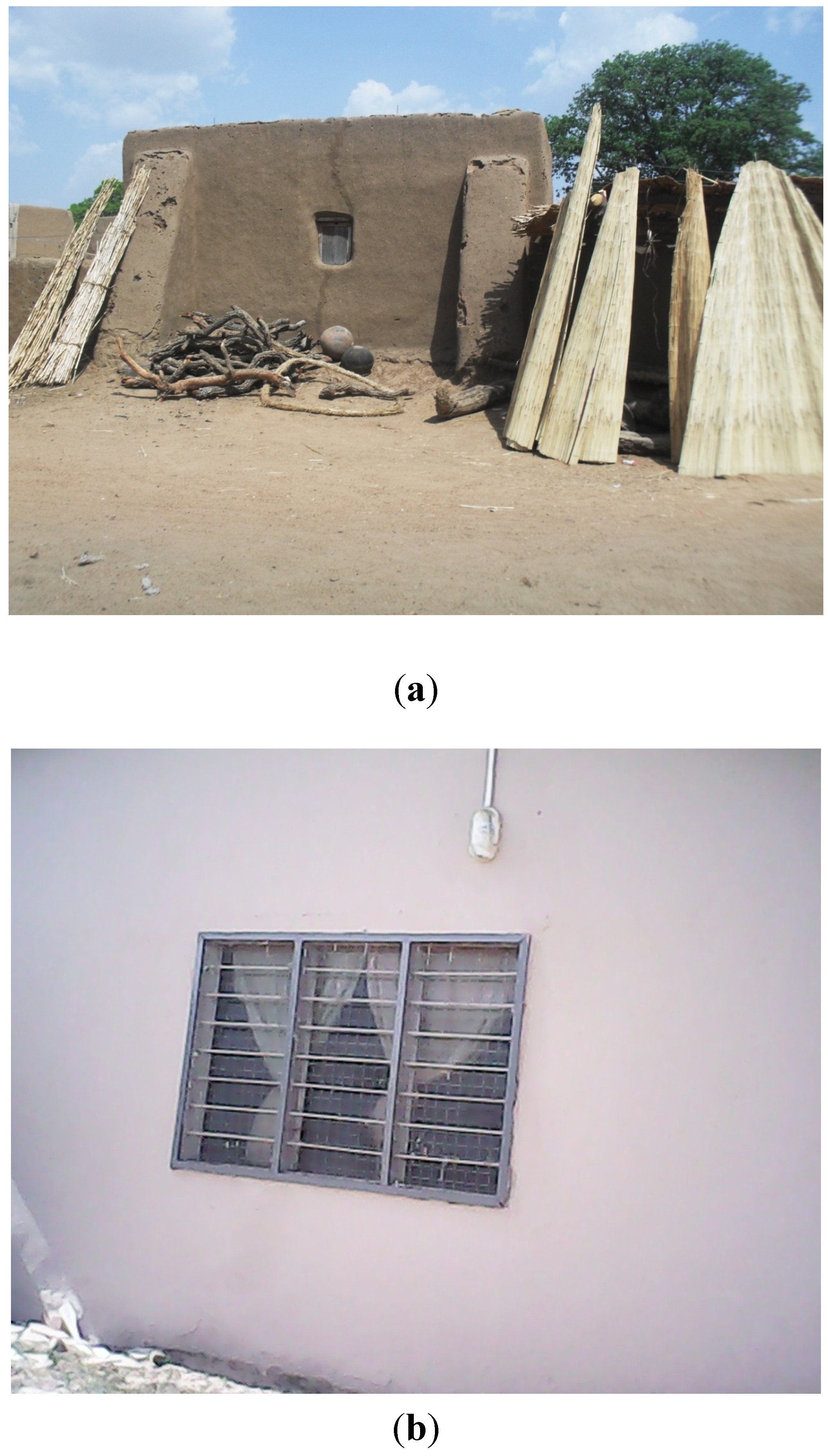
3.2.2. Autonomous Adaptation: Modifications in Dwelling Types, Use of Fuel Efficient and Improved Cooking Methods, Sleeping in Open Air

We respect our culture and traditions, including the types of houses we live in. However, the traditional local houses expose us to a lot of heat and diseases like CSM. Based on the recommendation of our community leaders in our community action plans, we decided to modify our houses into cement block houses and zinc or aluminium roofs gradually. Though relatively expensive, we have not regretted because the new houses are more airy and spacious than the previous ones.
3.2.3. Planned Adaptation: Afforestation and Preservation of Sacred Groves in Communities
We now grow trees along the boundaries of our communities, and within our houses. We have taken to various afforestation projects to improve upon the natural environment. We have planted teak along the Bolgatanga-Navrongo road just before the Notre Dame Minor Seminary/Secondary School at Nayagnia. We have also planted canopy-top trees that offer various degrees of shades in our backyards. It is these trees that we take cover under during the daytime when temperatures rise so high in the dry season.We have put in place initiatives that help preserve our community sacred groves as an intervention for improving the environment and bringing temperatures down. We revere these sacred groves so we prevent people from going there to cut down the trees.
4. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Intergovernmental Panel on Climate Change. Impacts; Adaptation and Vulnerability. Part A: Global and Sectoral Aspects. In Contribution of Working Group II to the 5th Assessment Report of the Intergovernmental Panel on Climate Change; Field, C.B.; Barros, V.R.; Dokken, D.K.; Mach, K.J.; Mastrandrea, M.D.; Bilir, T.E.; Chatterjee, M.; Ebi, K.L.; Estrada, Y.O.; Genova, R.C. (Eds.) Cambridge University Press: Cambridge, UK, 2014.
- Rosenzweig, C.; Karoly, D.; Vicarelli, M.; Neofotis, P.; Wu, Q.G.; Casasa, G.; Menzel, A.; Root, T.L.; Estrella, N.; Seguin, B.; et al. Attributing physical and biological impacts to anthropogenic climate change. Nature 2008, 453, 353–357. [Google Scholar] [CrossRef]
- Chaves, L.F.; Koenraadt, C.J.M. Climate change and highland malaria: Fresh air for a hot debate. Quart. Rev. Biol. 2010, 85, 27–55. [Google Scholar] [CrossRef]
- Haines, A.; McMichael, A.J.; Smith, K.R.; Roberts, I.; Woodcock, J.; Markandya, A.; Armstrong, B.G.; Campbell-Lendrum, D.; Dangour, A.D.; Davies, M.; et al. Public health benefits of strategies to reduce greenhouse-gas emissions: Overview and implications for policy makers. Lancet 2009, 374, 2104–2114. [Google Scholar] [CrossRef]
- Confalonieri, U.; Menne, B.; Akhtar, R.; Ebi, K.L.; Hauengue, M.; Kovats, R.S.; Revich, B.; Woodward, A. Human Health. In Climate Change 2007: Impacts; Adaptation and Vulnerability. Contribution of Working Group II to the 4th Assessment Report of the Intergovernmental Panel on Climate Change; Parry, M.L., Canziani, O.F., Palutikof, J.P., van der Linden, P.J., Hanson, C.E., Eds.; Cambridge University Press: Cambridge, UK, 2007; pp. 391–431. [Google Scholar]
- Broutin, H.; Philippon, S.; Constantin de Magny, G.; Courel, F.; Sultan, B.; Guegan, J.F. Comparative study of meningitis dynamics across nine African countries: A global perspective. Int. J. Health Geogr. 2007, 6. [Google Scholar] [CrossRef]
- Cuevas, L.E.; Jeanne, I.; Molesworth, A.; Bell, M.; Savory, E.C.; Connor, S.J.; Thomson, M.C. Risk mapping and early warning systems for the control of meningitis in Africa. Vaccine 2007, 25, 12–17. [Google Scholar] [CrossRef]
- Abdussalam, A.F.; Monaghan, A.J.; Dukic, V.M.; Hayden, M.H.; Hopson, T.M.; Leckebusch, G.C.; Thornes, J. Climate influences on the interannual variability of meningitis incidence in northwest Nigeria. Weather Clim. Soc. 2014, 6, 62–76. [Google Scholar]
- Molesworth, A.M.; Thomson, M.C.; Connor, S.J.; Creswell, M.P.; Morse, A.P. Where is the meningitis belt? Defining an area at risk of epidemic meningitis in Africa. Trans. Roy. Soc. Trop. Med. Hyg. 2002, 96, 242–249. [Google Scholar] [CrossRef]
- Thomson, M.C.; Molesworth, A.M.; Djingarey, M.H.; Yameogo, K.R.; Belanger, F.; Cuevas, L.E. Potential of environmental models to predict meningitis epidemics in Africa. Trop. Med. Int. Health 2006, 11, 781–788. [Google Scholar] [CrossRef]
- Yaka, P.; Sultan, B.; Broutin, H.; Janicot, S.; Philippon, S.; Fourquet, N. Relationship between climate and year to year variability in meningitis outbreaks: A case study in Burkina Faso and Niger. Int. J. Health Geogr. 2008, 7. [Google Scholar] [CrossRef]
- Obiakor, M.O. Weather variables and climatic influence on the epidemiology of cerebrospinal or meningococcal meningitis. Asian J. Med. Pharm. Res. 2011, 3, 1–10. [Google Scholar]
- Palmgren, H. Meningococcal disease and climate. Glob. Health Action 2009, 2. [Google Scholar] [CrossRef]
- Savory, E.C.; Cuevas, L.E.; Yassin, M.A.; Hart, C.A.; Molesworth, A.M.; Thomson, M.C. Evaluation of the meningitis epidemics risk model in Africa. Epidemiol. Infect. 2006, 134, 1047–1051. [Google Scholar] [CrossRef]
- Block, C.; Roitman, M.; Bogokowsky, B.; Meizlin, S.; Slater, P.E. Forty years of meningococcal disease in Israel: 1951–1990. Clin. Infect. Dis. 1993, 17, 126–132. [Google Scholar] [CrossRef]
- Collier, C.G. Weather conditions prior to major outbreaks of meningococcal meningitis in the United Kingdom. Int. J. Biometeorol. 1992, 36, 18–29. [Google Scholar]
- Fisman, D.N. Seasonality of infectious diseases. Annu. Rev. Public Health 2007, 28, 127–143. [Google Scholar] [CrossRef]
- Jensen, E.S.; Lundbye-Christensen, S.; Pedersen, L.; Sørensen, H.T.; Schønheyder, H.C. Seasonal variation in meningococcal disease in Denmark: Relation to age and meningococcal phenotype. Scand. J. Infect. Dis. 2003, 35, 226–229. [Google Scholar]
- Kinlin, L.M.; Spain, C.V.; Ng, V.; Johnson, C.C.; White, A.N.; Fisman, D.N. Environmental exposures and invasive meningococcal disease: An evaluation of effects on varying time scales. Amer. J. Epidemiol. 2009, 169, 588–595. [Google Scholar]
- Lindsay, A.P.; Hope, V.; Marshall, R.J.; Salinger, J. Meningococcal disease and meteorological conditions in Auckland, New Zealand. Aust. N. Z. J. Public Health 2002, 26, 212–218. [Google Scholar] [CrossRef]
- Michele, M.M.; Alberto, M.; Liana, S.; Francesco, D. Do environmental factors influence the occurrence of acute meningitis in industrialized countries? An epidemic of varying aetiology in northern Italy. Eur. J. Epidemiol. 2006, 21, 465–468. [Google Scholar] [CrossRef]
- Millon, C. When and Where are We at Risk? The Geographical Distribution of Meningococcal Meningitis in England and Wales. Bachelor Thesis, School of Geography, University of Oxford, Oxford, UK, 1983. [Google Scholar]
- De Chabalier, F.; Djingarey, M.H.; Hassane, A.; Chippanx, J.P.C. Meningitis seasonal pattern in Africa and detection of epidemics: A retrospective study in Niger; 1990–1998. Trans. Roy. Soc. Trop. Med. Hyg. 2000, 94, 664–668. [Google Scholar] [CrossRef]
- Greenwood, B.M.; Bradley, A.K.; Wall, R.A. Meningococcal disease and season in sub-Saharan Africa. Lancet 1985, 2, 829–830. [Google Scholar] [CrossRef]
- Lapeyssonnie, L. La méningite cérébro-spinale en Afrique. Bull. World Health Organ. 1963, 2, 3–14. (in French). [Google Scholar]
- Salih, M.A.; Danielsson, D.; Bäckman, A.; Caugant, D.A.; Achtman, M.; Olcén, P. Characterization of epidemic and non-epidemic Neisseria meningitidis serogroup A strains from Sudan and Sweden. J. Clin. Microbiol. 1990, 28, 1711–1719. [Google Scholar]
- Cheesbrough, J.S.; Morse, A.P.; Green, S.D.R. Meningococcal meningitis and carriage in western Zaire. A hypoendemic zone related to climate? Epidemiol. Infect. 1995, 114, 75–92. [Google Scholar] [CrossRef]
- Greenwood, B.M.; Greenwood, A.M.; Bradley, A.K.; Williams, K.; Hassan-King, M.; Shenton, F.C. Factors influencing susceptibility to meningococcal disease during an epidemic in the Gambia, west Africa. J. Infect. 1987, 14, 167–184. [Google Scholar] [CrossRef]
- Mueller, J.E.; Yaro, S.; Madec, Y.; Somda, P.K.; Idohou, R.S.; Lafourcade, B.M.; Drabo, A.; Tarnagda, Z.; Sangare, L.; Traore, Y.; et al. Association of respiratory tract infection symptoms and air humidity with meningococcal carriage in Burkina Faso. Trop. Med. Int. Health 2008, 13, 1543–1552. [Google Scholar] [CrossRef]
- Jackou-Boulama, M.; Michel, R.; Ollivier, L.; Meynard, J.B.; Nicolas, P.; Boutin, J.P. Correlation between rainfall and meningococcal meningitis in Niger. Med. Trop. 2005, 65, 329–333. [Google Scholar]
- Besancenot, J.P.; Boko, M.; Oke, P.C. Weather conditions and cerebrospinal meningitis in Benin (Gulf of Guinea, west Africa). Eur. J. Epidemiol. 1997, 13, 807–815. [Google Scholar] [CrossRef]
- Molineaux, L. Climate and Meningococcal Disease. Ph.D. Thesis, University of Berkeley, Berkeley, CA, USA, 1969. [Google Scholar]
- Moore, P.S. Meningococcal meningitis in sub-Saharan Africa: A model for the epidemic process. Clin. Infect. Dis. 1992, 14, 515–525. [Google Scholar] [CrossRef]
- Sultan, B.; Labadi, K.; Gue’gan, J.F.; Janicot, S. Climate drives the meningitis epidemics onset in west Africa. PLoS Med. 2005, 2. [Google Scholar] [CrossRef]
- Heitz, C.; Spaeter, S.; Auzet, A.V.; Glatron, S. Local stakeholders’ perception of muddy flood risk and implications for management approaches: A case study in Alsace (France). Land Use Policy 2009, 26, 443–451. [Google Scholar] [CrossRef]
- Ho, M.C.; Shaw, D.; Lin, S.Y.; Chiu, Y.C. How do disaster characteristics influence risk perception? Risk Anal. 2008, 28, 635–643. [Google Scholar] [CrossRef]
- Hunter, L.M.; Strife, S.; Twine, W. Environmental perceptions of rural South African residents: The complex nature of environmental concern. Soc. Nat. Resour. 2010, 24, 525–541. [Google Scholar]
- Leiserowitz, A. Climate change risk perception and policy preferences: The role of affect, imagery and values. Climatic Change 2006, 77, 45–72. [Google Scholar]
- Guidelines on the Control of Epidemic Meningococcal Disease, 2nd ed.; WHO: Geneva, Switzerland, 1998.
- WHO. Meningococcal Meningitis. Fact Sheet. 2003. Available online: http://www.who.int/mediacentre/factsheets>/2003/fs141/en/indexhtml (accessed on 11 March 2013).
- Greenwood, B. 100 years of epidemic meningitis in west Africa—Has anything changed? Trop. Med. Int. Health 2006, 11, 773–780. [Google Scholar] [CrossRef]
- Ministry of Health. Recorded Cerebrospinal Meningitis Cases in Ghana, 1985–2008; Centre for Health Information Management Systems: Accra, Ghana, 2010.
- Grimwood, K.; Anderson, P.; Anderson, V.; Tan, L.; Nolan, T. Twelve year outcomes following bacterial meningitis: Further evidence for persisting effects. Arch. Dis. Child. 2000, 83, 111–116. [Google Scholar] [CrossRef]
- Mar, I.D.; Denis, F.; Cadoz, M. Epidemiologic features of pneumococcal meningitis in Africa. Clinical and serotypical aspects. Pathol. Biol. 1979, 27, 543–548. [Google Scholar]
- Kumanda, V. Changing Pattern of Incidence of Meningococcal Meningitis as Seen in Ahmadu Bello University, Teaching Hospital, Zaria (1979–1982); Department of Community Medicine, Ahmadu Bello University: Zaria, Nigeria, 1983. [Google Scholar]
- Akande, T.M.; Olu, O. Perception and attitude to outbreak of Meningitis. Niger. J. Med. 1998, 7, 154–156. [Google Scholar]
- Elias, J.; Harmsen, D.; Claus, H.; Hellenbrand, W.; Frosch, M.; Vogel, V. Spatiotemporal analysis of invasive meningococcal disease, Germany. Emerg. Infect. Dis. 2006, 12, 1689–2695. [Google Scholar]
- Hastenrath, S. Climate Dynamics of the Tropics; Kluwer Academic: Dordrecht, the Netherlands, 1995. [Google Scholar]
- Van Deuren, M.; Brandtzaeg, P.; van der Meer, J.W.M. Update on meningococcal disease with emphasis on pathogenesis and clinical management. Clin. Microbiol. Rev. 2000, 13, 144–166. [Google Scholar] [CrossRef]
- WHO. Pneumococcal vaccines. Wkly. Epidemiol. Rec. 1999, 74, 177–183. [Google Scholar]
- WHO. Detecting meningococcal meningitis epidemics in highly-endemic African countries. Wkly. Epidemiol. Rec. 2000, 75, 305–312. [Google Scholar]
- WHO. Enhanced surveillance of epidemic meningococcal meningitis in Africa. Wkly. Epidemiol. Rec. 2005, 80, 313–320. [Google Scholar]
- Forgor, A.A. Meningococcal and Pneumococcal Meningitis in Northern Ghana; Faculty of Philosophy and Natural Science, University of Basel: Basel, Switzerland, 2007. [Google Scholar]
- Waddy, B.B. African epidemic cerebrospinal meningitis. J. Trop. Med. Hyg. 1957, 60, 179–189. [Google Scholar]
- Horn, A.E. Report on an investigation of cerebrospinal fever in the northern territories of the Gold Coast. J. Trop. Med. Hyg. 1908, 11, 358–364. [Google Scholar]
- Belcher, D.W.; Sherriff, A.C.; Nimo, K.P.; Chew, G.L.; Richardson, W.D.; Voros, A.; Feldman, H.A.; Richardson, W.D.; Feldman, H.A. Meningococcal meningitis in northern Ghana: Epidemiology and control measures. Amer. J. Trop. Med. Hyg. 1977, 26, 748–755. [Google Scholar]
- Haddock, D.R. Forty-seven cases of pyogenic meningitis in adults in Korle Bu Hospital, Accra. Ghana Med. J. 1971, 10, 3–8. [Google Scholar]
- Greene, J.D.; Waddy, B.B. A cycle of Cerebro-spinal Meningitis in the Gold Coast. Trans. Roy. Soc. Trop. Med. Hyg. 1954, 48, 64–72. [Google Scholar] [CrossRef]
- Browne, M.P. Report on the First 7000 Cases of Cerebrospinal Meningitis in the Western Northern Territories—1st January to 21st March 1945; PRAAD: Accra, Ghana.
- Enos, K. Cerebrospinal Meningitis in Northern Ghana: The Experience of the War Memorial Hospital, Navrongo; Ministry of Health: Accra, Ghana, 1997. [Google Scholar]
- Mackie, E.J.; Shears, P.; Frimpong, E.; Mustafa-Kutana, S.N. A study of bacterial meningitis in Kumasi, Ghana. Ann. Trop. Paediatr. 1992, 12, 143–148. [Google Scholar]
- Woods, C.W.; Armstrong, G.; Sackey, S.O.; Tetteh, C.; Bugri, S.; Perkins, B.A.; Rosenstein, N.E. Emergency vaccination against epidemic meningitis in Ghana: Implications for the control of meningococcal disease in west Africa. Lancet 2000, 355, 30–33. [Google Scholar] [CrossRef]
- Hodgson, A.; Smith, T.; Gagneux, S.; Adjuik, M.; Pluschke, G.; Mensah, N.K.; Binka, F.; Genton, B. Risk factors for meningococcal meningitis in northern Ghana. Trans. Roy. Soc. Trop. Med. Hyg. 2001, 95, 477–480. [Google Scholar]
- Hodgson, A.; Smith, T.; Gagneux, S.; Akumah, I.; Adjuik, M.; Pluschke, G.; Binka, F.; Genton, B. Survival and sequelae of meningococcal meningitis in Ghana. Int. J. Epidemiol. 2001, 30, 1440–1446. [Google Scholar] [CrossRef]
- Hodgson, A.; Smith, T.; Gagneux, S.; Enos, K.E.; Adjuik, M.; Pluschke, G.; Binka, F.; Genton, B. Meningococcal Meningitis in Northern Ghana: Epidemiological Features of the 1997 Outbreak in the Kassena-Nankana District. In Meningococcal Meningitis in Northern Ghana: Epidemiological and Clinical Features, Risk Factors, Survival and Sequelae; University of Basel: Basel, Switzerland, 2002; pp. 19–39. [Google Scholar]
- Forgor, A.A.; Leimkugel, J.; Hodgson, A.; Bugri, A.; Dangy, J.P.; Gagneux, S.; Smith, T.; Pluschke, G. Emergence of W135 meningococcal meningitis in Ghana. Trop. Med. Int. Health 2005, 10, 1229–1234. [Google Scholar] [CrossRef]
- Gagneux, S.P.; Hodgson, A.; Ehrhard, I.; Morelli, G.; Genton, B.; Smith, T.; Tanner, M.; Binka, F.; Achtman, M.; Pluschke, G. Microheterogeneity of serogroup A (subgroup III) Neisseria meningitidis during an outbreak in northern Ghana. Trop. Med. Int. Health 2000, 5, 280–287. [Google Scholar] [CrossRef]
- Gagneux, S.P.; Hodgson, A.; Smith, T.A.; Wirth, T.; Ehrhard, I.; Morelli, G.; Genton, B.; Binka, F.N.; Achtman, M.; Pluschke, G. Prospective study of a serogroup X Neisseria meningitidis outbreak in northern Ghana. J. Infect. Dis. 2002, 185, 618–626. [Google Scholar] [CrossRef]
- Leimkugel, J.; Forgor, A.A.; Gagneux, S.; Pfluger, V.; Flierl, C.; Awine, E.; Naegeli, M.; Dangy, J.P.; Smith, T.; Hodgson, A.; Pluschke, G. An outbreak of serotype 1 Streptococcus pneumoniae meningitis in northern Ghana with features that are characteristic of Neisseria meningitidis meningitis epidemics. J. Infect. Dis. 2005, 192, 192–199. [Google Scholar] [CrossRef]
- Leimkugel, J.; Hodgson, A.; Forgor, A.A.; Pflüger, V.; Dangy, J.P.; Smith, T.; Achtman, M.; Gagneux, S.; Pluschke, G. Clonal waves of Neisseria colonisation and disease in the African meningitis belt: Eight-year longitudinal study in northern Ghana. PLoS Med. 2007, 4. [Google Scholar] [CrossRef]
- Taha, M.K.; Achtman, M.; Alonso, J.M.; Greenwood, B.; Ramsay, M.; Fox, A.; Gray, S.; Kaczmarski, E. Serogroup W135 meningococcal disease in Hajj pilgrims. Lancet 2000, 356. [Google Scholar] [CrossRef]
- Commey, J.O.; Rodrigues, O.P.; Akita, F.A.; Newman, M. Bacterial meningitis in children in southern Ghana. East Afr. Med. J. 1994, 71, 113–117. [Google Scholar]
- Owusu, M.; Nguah, S.B.; Boaitey, Y.A.; Badu-Boateng, E.; Abubakr, A.R.; Lartey, R.A.; Adu-Sarkodie, Y. Aetiological agents of cerebrospinal meningitis: A retrospective study from a teaching hospital in Ghana. Ann. Clin. Microbiol. Antimicrob. 2012, 11. [Google Scholar] [CrossRef]
- Hayden, M.H.; Dalaba, M.; Awine, T.; Akweongo, P.; Nyaaba, G.; Anaseba, D.; Pelzman, J.; Hodgson, A.; Pandya, R. Knowledge, attitudes, and practices related to Meningitis in northern Ghana. Amer. J. Trop. Med. Hyg. 2013, 89, 265–270. [Google Scholar] [CrossRef]
- Akweongo, P.; Dalaba, M.A.; Hayden, M.H.; Awine, T.; Nyaaba, G.N.; Anaseba, D.; Hodgson, A.; Forgor, A.A.; Pandya, R. The economic burden of Meningitis to households in Kassena-Nankana district of northern Ghana. PLoS One 2013, 8. [Google Scholar] [CrossRef]
- Dukic, V.; Hayden, M.; Forgor, A.A.; Hopson, T.; Akweongo, P.; Hodgson, A.; Monaghan, A.; Wiedinmyer, C.; Yoksas, T.; Thomson, M.C.; et al. The role of weather in Meningitis outbreaks in Navrongo, Ghana: A generalized additive modeling approach. J. Agric. Biol. Environ. Stat. 2012, 17, 442–460. [Google Scholar] [CrossRef]
- Ghana Statistical Service. 2010 Population and Housing Census. Summary Report of Final Results; Sakoa Press: Accra, Ghana, 2012. [Google Scholar]
- Tschakert, P.; Sagoe, R.; Ofori-Darko, G.; Codjoe, S.N. Floods in the Sahel: An analysis of anomalies, memory and anticipatory learning. Climatic Change 2010, 103, 471–502. [Google Scholar] [CrossRef]
- Intergovernmental Panel on Climate Change. Climate Change: Impacts, Adaptation and Vulnerability. In Contribution of Working Group II to the 4th Assessment Report of the Intergovernmental Panel on Climate Change; Parry, M.L., Canziani, O.F., Palutikof, J.P., van der Linden, P.J., Handson, C.E., Eds.; Cambridge University Press: Cambridge, UK, 2007. [Google Scholar]
- Smit, B.; Burton, I.; Klein, R.J.T.; Wandel, J. An anatomy of adaptation to climate change and vairability. Climatic Change 1999, 45, 223–251. [Google Scholar]
- Frankhauser, S.; Smith, J.B.; Tol, R.S.J. Weathering climate change: Some simple rules to guide adaptation decisions. Ecol. Econ. 1999, 30, 67–78. [Google Scholar] [CrossRef]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Codjoe, S.N.A.; Nabie, V.A. Climate Change and Cerebrospinal Meningitis in the Ghanaian Meningitis Belt. Int. J. Environ. Res. Public Health 2014, 11, 6923-6939. https://doi.org/10.3390/ijerph110706923
Codjoe SNA, Nabie VA. Climate Change and Cerebrospinal Meningitis in the Ghanaian Meningitis Belt. International Journal of Environmental Research and Public Health. 2014; 11(7):6923-6939. https://doi.org/10.3390/ijerph110706923
Chicago/Turabian StyleCodjoe, Samuel Nii Ardey, and Vivian Adams Nabie. 2014. "Climate Change and Cerebrospinal Meningitis in the Ghanaian Meningitis Belt" International Journal of Environmental Research and Public Health 11, no. 7: 6923-6939. https://doi.org/10.3390/ijerph110706923
APA StyleCodjoe, S. N. A., & Nabie, V. A. (2014). Climate Change and Cerebrospinal Meningitis in the Ghanaian Meningitis Belt. International Journal of Environmental Research and Public Health, 11(7), 6923-6939. https://doi.org/10.3390/ijerph110706923