Radiation-Driven Migration: The Case of Minamisoma City, Fukushima, Japan, after the Fukushima Nuclear Accident

Abstract
:1. Introduction
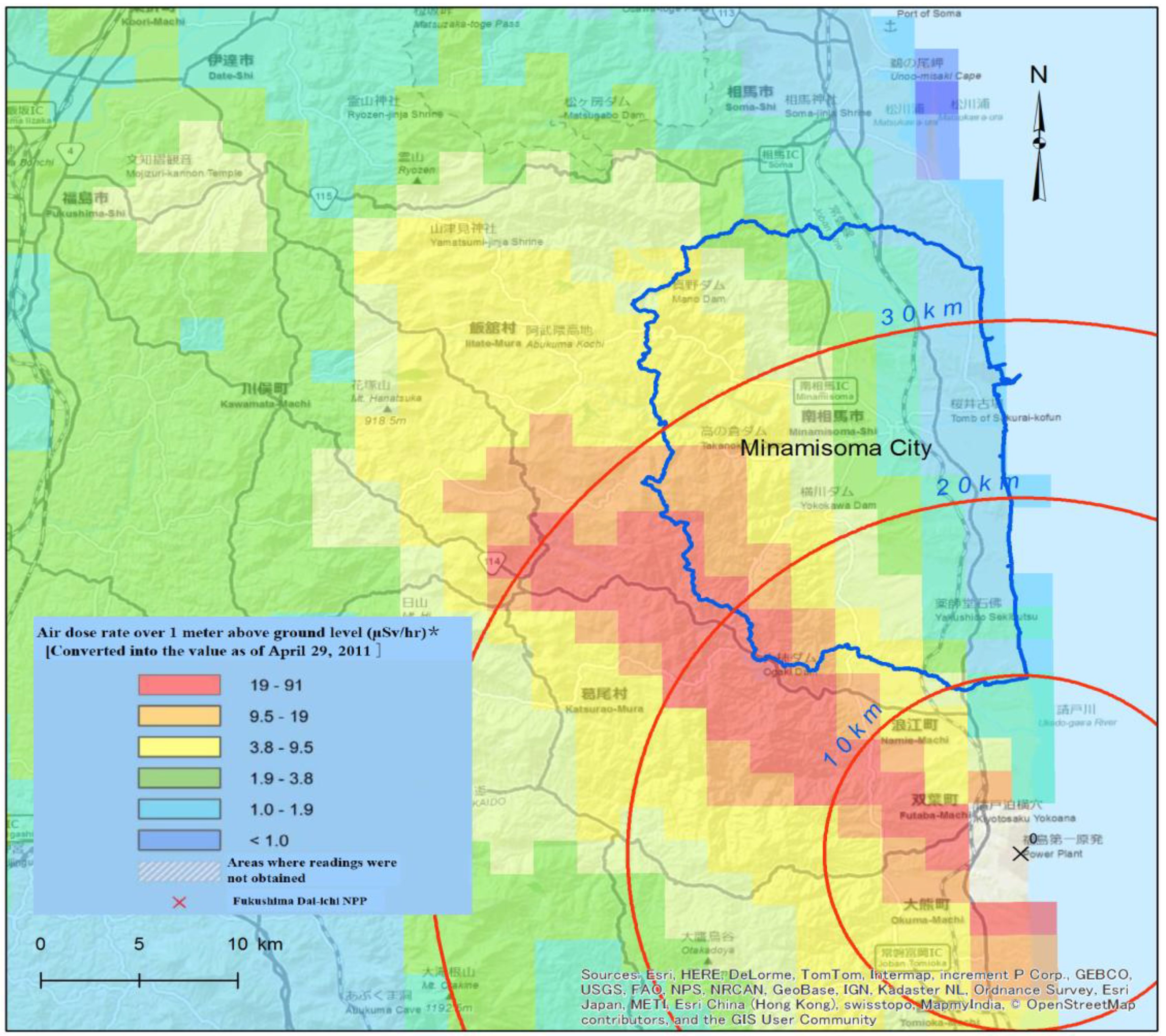
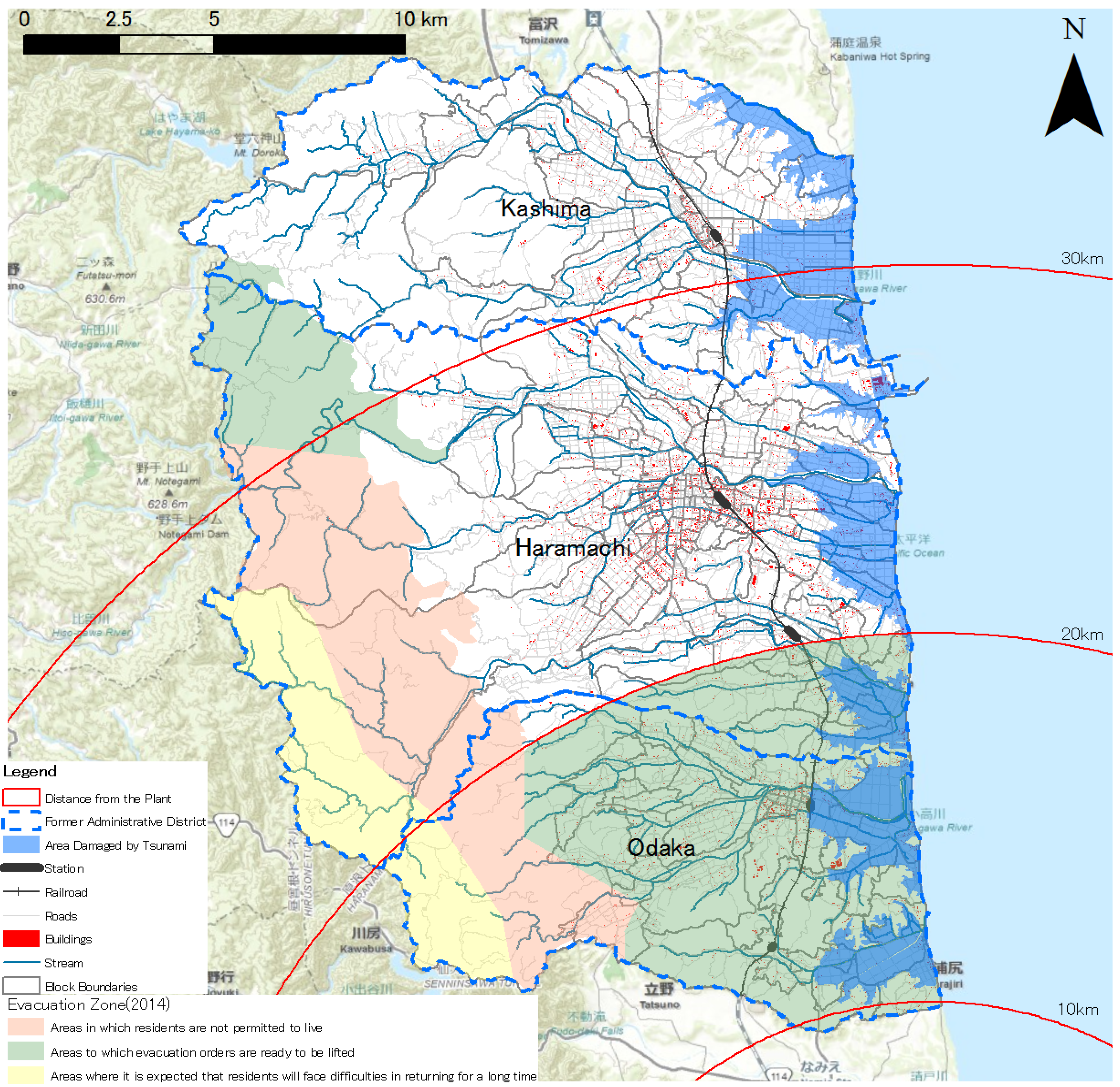
2. The Study Area: Evacuation Plan and Restoration Efforts


{kind=link}
{kind=link}
{kind=link}
{kind=link}
3. The Post-Disaster Population Situation and Its Effects
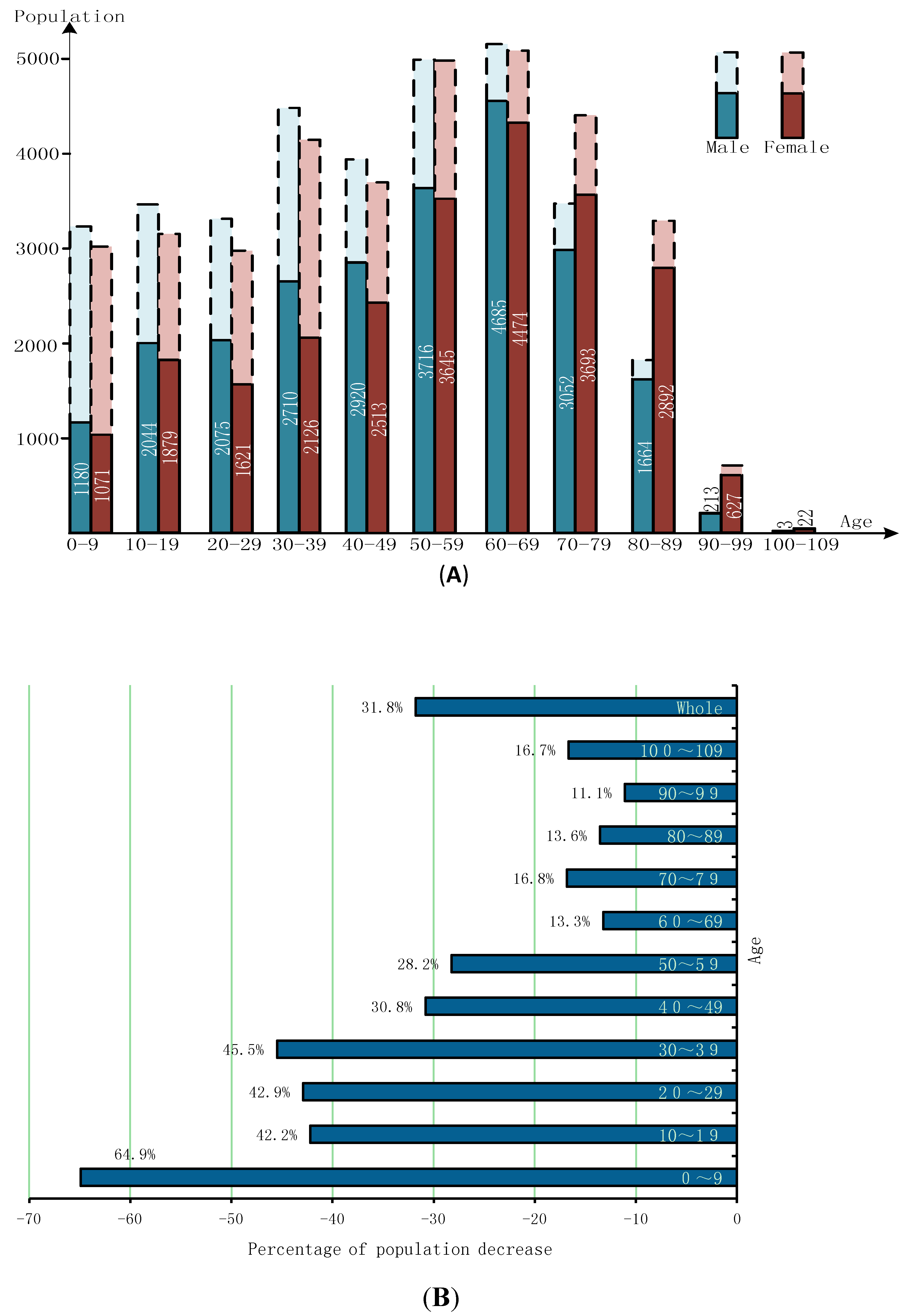
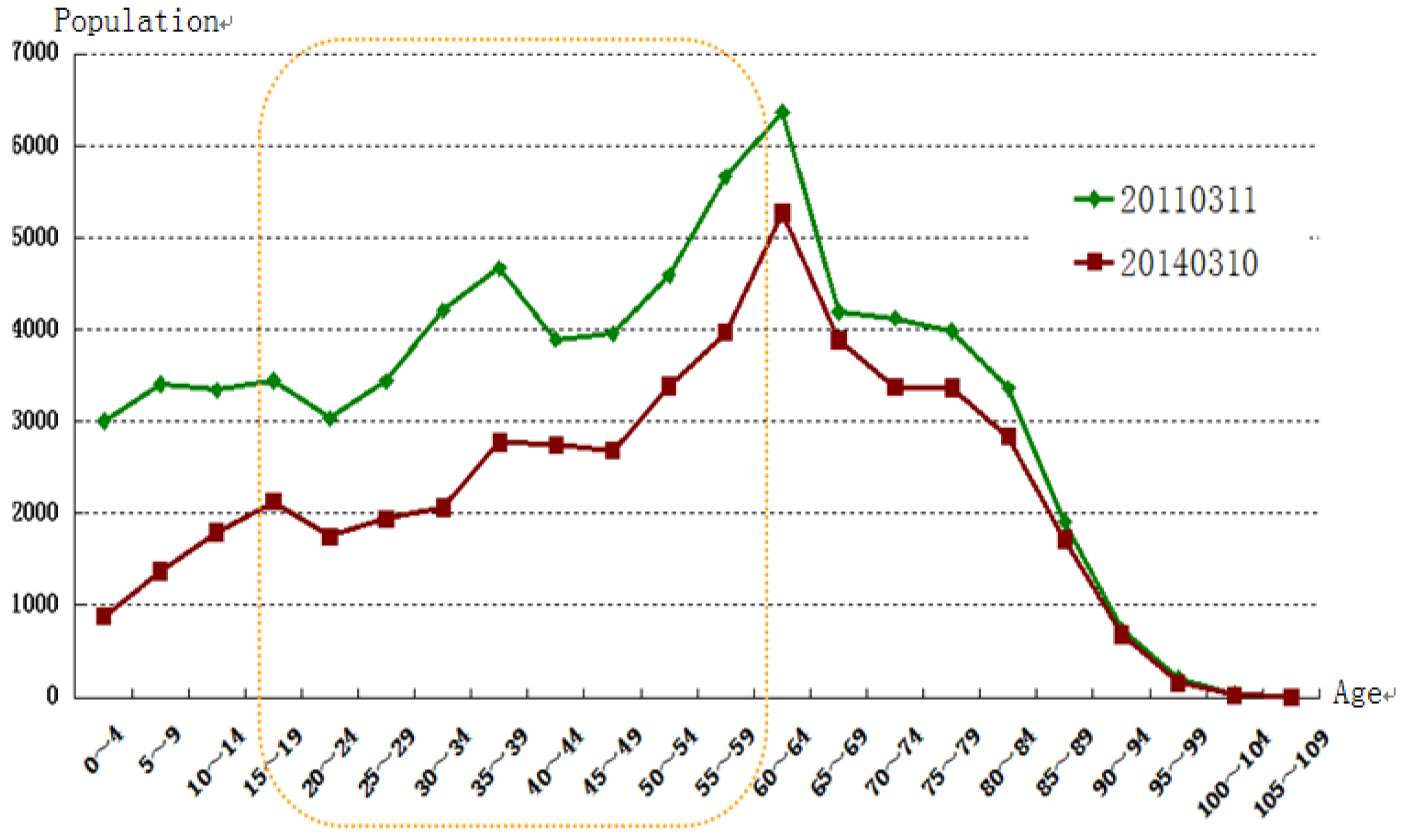
3.1. Post-Disaster Population Data for Minamisoma


3.2. The Effects of Evacuation and Demographic Change
4. Reasons for Emigration
4.1. Relevant Health Influence
4.2. Psychological Resilience
4.3. Economic Fluctuation
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Baba, M. Fukushima Accident: What Happened? Radiat. Meas. 2013, 55, 17–21. [Google Scholar] [CrossRef]
- Steinhauser, G.; Brandl, A.; Johnson, T.E. Comparison of the chernobyl and Fukushima nuclear accidents: A review of the environmental impacts. Sci. Total Environ. 2014, 470–471, 800–817. [Google Scholar]
- Suzuki, I.; Kaneko, Y. Managing Fukushima NPS accidents: In particular focus on government crisis communication. In Japan’s Disaster Governance; Springer: New York, NY, USA, 2013; pp. 49–79. [Google Scholar]
- Final Report of The International Mission on Remediation of Large Contaminated Areas Off-Site the Fukushima Daiichi NPP; International Atomic Energy Agency: Vienna, Austria, 2011. Available online: http://reliefweb.int/report/japan/final-report-international-mission-remediation-large-contaminated-areas-site-fukushima (accessed on 5 May 2014).
- Ishikawa, K.; Kanazawa, Y.; Morimoto, S.; Takahashi, T. Depopulation with rapid aging in Minamisoma city after the Fukushima daiichi nuclear power plant accident. J. Am. Vet. Med. Assoc. 2014, 244, 1243–1245. [Google Scholar] [CrossRef] [PubMed]
- The Current Situation in Minamisoma City after the Nuclear Disaster; (In Japanese)Ministry of Education, Culture, Sports and Technology: Minami-Soma, Japan, 2013. Available online: http://www.mext.go.jp/b_menu/shingi/chousa/kaihatu/016/shiryo/__icsFiles/afieldfile/2013/06/24/1336650_1_1.pdf (accessed on 22 April 2014).
- Main report Chapter 4. Overview of Damage from the Nuclear Power Plant Accident; The National Diet of Japan Fukushima Nuclear Accident Independent Investigation Commission: Fukushima City, Japan, 2012. Available online: http://warp.da.ndl.go.jp/info:ndljp/pid/3856371/naiic.go.jp/en/index.html (accessed on 22 April 2014).
- Health Risk Assessment from the Nuclear Accident after the 2011 Great East Japan Earthquake and Tsunami Based on Preliminary Dose Estimation; World Health Organization: Geneva, Switzerland, 2013. Available online: http://warp.da.ndl.go.jp/info:ndljp/pid/3856371/naiic.go.jp/en/index.html (accessed on 22 April 2014).
- Yamashita, S.; Suzuki, S. Risk of thyroid cancer after the Fukushima nuclear power plant accident. Respir. Investig. 2013, 51, 128–133. [Google Scholar] [CrossRef] [PubMed]
- International Atomic Energy Agency. Fukushima Nuclear Accident Update Log. Available online: http://www.iaea.org/newscenter/news/2011/fukushima200511.html (accessed on 3 April 2014).
- Nuclear Regulation Authority. Results of Airborne Monitoring by the Ministry of Education, Culture, Sports, Science and Technology and the U.S. Department of Energy. Available online: http://radioactivity.nsr.go.jp/en/contents/4000/3180/24/1304797_0506.pdf (accessed on 3 August 2014).
- Minamisoma Statistical Yearbook; (In Japanese)Minamisoma Government: Minami-Soma, Japan, 2013. Available online: http://www.city.minamisoma.lg.jp/index.cfm/8,4226,44,html (accessed on 6 March 2014).
- Minamisoma Government. The Geography of Minamisoma. (In Japanese)Available online: http://www.city.minamisoma.lg.jp/index.cfm/8,1620,c,html/1620/04_3shou.pdf (accessed on 3 April 2014).
- Prime Minister of Japan and His Cabinet. The Map of Evacuation Zone. (In Japanese)Available online: http://www.kantei.go.jp/saigai/pdf/20140401gainenzu.pdf (accessed on 3 August 2014).
- Thielen, H. The Fukushima daiichi nuclear accident—An overview. Health Phys. 2012, 103, 169–174. [Google Scholar] [CrossRef] [PubMed]
- Onishi, N.; Fackler, M. In nuclear crisis, crippling mistrust. New York Times 2011, 12, 1–7. [Google Scholar]
- International Atomic Energy Agency. Report of Japanese Government to the IAEA Ministerial Conference on Nuclear Safety—The Accident at TEPCO’s Fukushima Nuclear Power Stations. Available online: http://www.iaea.org/newscenter/focus/fukushima/japan-report/ (accessed on 7 June 2011).
- Hamada, N.; Ogino, H. Food safety regulations: What we learned from the Fukushima nuclear accident. J. Environ. Radioact. 2012, 111, 83–99. [Google Scholar] [CrossRef] [PubMed]
- Sugimoto, A.; Gilmour, S.; Tsubokura, M.; Nomura, S.; Kami, M.; Oikawa, T.; Kanazawa, Y.; Shibuya, K. Assessment of the risk of medium-term internal contamination in Minamisoma city, Fukushima, Japan, after the Fukushima Dai-Chi nuclear accident. Environ. Health Perspect. 2014, 122, 587–593. [Google Scholar] [PubMed]
- The Government of Japan, Ministry of Health Labor and Welfare. Response to the Great East Japan Earthquake By the Ministry of Health, Labor and Welfare. Available online: http://www.mhlw.go.jp/english/topics/2011eq/index.html (accessed on 23 April 2014).
- Merz, S.; Steinhauser, G.; Hamada, N. Anthropogenic radionuclides in Japanese food: Environmental and legal implications. Environ. Sci. Technol. 2013, 47, 1248–1256. [Google Scholar] [PubMed]
- Minamisoma Government. Decontamination Plan in Minamisoma (The Third Version). (In Japanese)Available online: http://www.city.minamisoma.lg.jp/index.cfm/10,16764,60,368,html (accessed on 29 March 2014).
- Ministry of Environment. Progress on Off-Site Cleanup Efforts in Japan. Available online: https://josen.env.go.jp/en/pdf/progressseet_progress_on_cleanup_efforts.pdf?140425 (accessed on 29 March 2014).
- Minamisoma Government. The Current Situation of Recovery in Minamisoma City. (In Japanese)Available online: http://www.city.minamisoma.lg.jp/index.cfm/10,5572,58,html (accessed on 3 April 2014).
- International Atomic Energy Agency. IAEA Fukushima Daiichi Status Report. Available online: http://www.iaea.org/newscenter/focus/fukushima/statusreports/fukushima28_09_12.html (accessed on 3 April 2014).
- Matanle, P. Ageing and Depopulation in Japan Understanding the Consequences for East and Southeast Asia By and Southeast Asia in the 21st Century. Available online: http://papers.ssrn.com/sol3/papers.cfm?abstract_id=2406498 (accessed on 10 March 2014).
- Barusch, A.S. Disaster, vulnerability, and older adults: Toward a social work response. J. Gerontol. Soc. Work 2011, 54, 347–350. [Google Scholar] [CrossRef] [PubMed]
- Phifer, J.; Kaniasty, K.; Norris, F. The impact of natural disaster on the health of older adults: A multiwave prospective study. J. health Soc. Behav. 1988, 29, 65–78. [Google Scholar] [CrossRef] [PubMed]
- Brown, L.A.; Shumway-Cook, A.; Woollacott, M.H. Attentional demands and postural recovery: The effects of aging. J. Gerontol. Series A, Biol. Sci. Med. Sci. 1999, 54, M165–M171. [Google Scholar]
- Adams, V.; Kaufman, S.R.; van Hattum, T.; Moody, S. Aging disaster: Mortality, vulnerability, and long-term recovery among Katrina survivors. Med. Anthropol. 2011, 30, 247–270. [Google Scholar] [CrossRef] [PubMed]
- Yasumura, S.; Goto, A.; Yamazaki, S.; Reich, M.R. Excess mortality among relocated institutionalized elderly after the Fukushima nuclear disaster. Public Health 2013, 127, 186–188. [Google Scholar] [CrossRef] [PubMed]
- Koeda, S.; Narita, H.; Tsushima, H. A literature review of health problems among nuclear power disaster evacuees: Common conditions, treatment, and rehabilitation. Radiat. Emerg. Med. 2012, 1, 88–92. [Google Scholar]
- Ishikawa, K. Long-Term evacuation after the nuclear accident in Fukushima: Different daily living under low-dose radioactive suffering. (In Japanese)Nihon Ronen Igakkai zasshi. 2013, 50, 84–87. [Google Scholar] [CrossRef] [PubMed]
- Higuchi, Y.; Inui, T.; Hosoi, T.; Takabe, I.; Kawakami, A. The impact of the great east Japan earthquake on the labor market: Need to resolve the employment mismatch in the disaster-stricken areas. Jpn. Labor Rev. 2012, 9, 4–21. [Google Scholar]
- Cardis, E.; Hatch, M. The Chernobyl accident—An epidemiological perspective. Clin. Oncol. 2011, 23, 251–260. [Google Scholar] [CrossRef]
- Tokonami, S.; Hosoda, M.; Akiba, S.; Sorimachi, A.; Kashiwakura, I.; Balonov, M. Thyroid doses for evacuees from the Fukushima nuclear accident. Sci. Rep. 2012, 2. [Google Scholar] [CrossRef]
- United Nations Scientific Committee on the Effects of Atomic Radiation. Effects of Ionizing Radiation: Report to the General Assembly, with Scientific Annexes; United Nations Publications: Herndon, VA, USA, 2008; Volume I. [Google Scholar]
- United Nations Scientific Committee on the Effects of Atomic Radiation. Sources, Effects and Risks of Ionizing Radiation UNSCEAR 2013 Report: Report to the General Assembly, with Scientific Annexes A: Levels and effects of Radiation Exposure Due to the Nuclear Accident after the 2011 Great East-Japan Earthquake and Tsunami; United Nations Publications: Herndon, VA, USA, 2014; Volume I. [Google Scholar]
- United Nations Scientific Committee on the Effects of Atomic Radiation. Sources, Effects and Risks of Ionizing Radiation UNSCEAR 2013 Report: 39 Scientific Annexes B: Effects of Radiation Exposure of Children; United Nations Publications: Herndon, VA, USA, 2014; Volume II. [Google Scholar]
- Steinhauser, G.; Merz, S.; Hainz, D.; Sterba, J.H. Artificial radioactivity in environmental media (air, rainwater, soil, vegetation) in Austria after the Fukushima nuclear accident. Environ. Sci. Pollut. Res. 2013, 20, 2527–2534. [Google Scholar] [CrossRef]
- Minamisoma Government. Individual Internal Radiation Dose Test Results. (In Japanese)Available online: http://www.city.minamisoma.lg.jp/index.cfm/10,0,61,367,html (accessed on 3 April 2014).
- Steinhauser, G.; Schauer, V.; Shozugawa, K. Concentration of strontium-90 at selected hot spots in Japan. PloS ONE 2013, 8. [Google Scholar] [CrossRef]
- Povinec, P.; Hirose, K.; Aoyama, M. Radiostrontium in the western North Pacific: Characteristics, behavior, and the Fukushima impact. Environ. Sci. Technol. 2012, 47, 2520–2526. [Google Scholar]
- Zheng, J.; Tagami, K.; Watanabe, Y.; Uchida, S.; Aono, T.; Ishii, N.; Yoshida, S.; Kubota, Y.; Fuma, S.; Ihara, S. Isotopic evidence of plutonium release into the environment from the Fukushima DNPP accident. Sci. Rep. 2012, 2. [Google Scholar] [CrossRef]
- Schneider, S.; Walther, C.; Bister, S. Plutonium release from Fukushima daiichi fosters the need for more detailed investigations. Sci. Rep. 2013, 3. [Google Scholar] [CrossRef]
- Zheng, J.; Tagami, K.; Uchida, S. Release of plutonium isotopes into the environment from the Fukushima daiichi nuclear power plant accident: What is known and what needs to be known. Environ. Sci. Technol. 2013, 47, 9584–9595. [Google Scholar] [CrossRef] [PubMed]
- Normile, D. Insistence on gathering real data confirms low radiation exposures. Science 2013, 340, 678–679. [Google Scholar]
- Hayano, R.S.; Tsubokura, M.; Miyazaki, M.; Satou, H.; Sato, K.; Masaki, S.; Sakuma, Y. Internal Radiocesium Contamination of Adults and Children in Fukushima 7 to 20 Months after the Fukushima NPP Accident as Measured by Extensive Whole-Body-Counter Surveys. Proc. Jpn. Acad. Ser. B, Phys. Boil. Sci. 2013, 89, 157–163. [Google Scholar]
- Kinley, D.; International Atomic Energy Agency. Chernobyl’s Legacy: Health, Environmental and Socio-Economic Impacts and Recommendations to the Governments of Belarus, the Russian Federation and Ukraine; Second revised version; IAEA: Vienna, Austria, 2006. [Google Scholar]
- Stephan, V. Chernobyl: Poverty and stress pose ‘bigger threat’ than radiation. Nature 2005, 437. [Google Scholar] [CrossRef]
- Adams, R.E.; Guey, L.T.; Gluzman, S.F.; Bromet, E.J. Psychological well-being and risk perceptions of mothers in Kyiv, Ukraine, 19 years after the Chornobyl disaster. Int. J. Soc. Psychiatry 2011, 57, 637–645. [Google Scholar] [CrossRef] [PubMed]
- Tateno, S.; Yokoyama, H.M. Article public anxiety, trust, and the role of Mediators in communicating risk of exposure to low dose radiation after the Fukushima daiichi nuclear plant explosion. J. Sci. Commun. 2013, 12, 1–22. [Google Scholar]
- Harada, K.H.; Fujii, Y.; Adachi, A.; Tsukidate, A.; Asai, F.; Koizumi, A. Dietary intake of radiocesium in adult residents in Fukushima prefecture and neighboring regions after the Fukushima nuclear power plant accident: 24-H food-duplicate survey in December 2011. Environ. Sci. Technol. 2013, 47, 2520–2526. [Google Scholar] [CrossRef] [PubMed]
- Hamada, N.; Ogino, H.; Fujimichi, Y. Safety regulations of food and water implemented in the first year following the Fukushima nuclear accident. J. Radiat. Res. 2012, 53, 641–671. [Google Scholar] [CrossRef] [PubMed]
- Environmental Counselors Union. The Current Situation of Recovery in Minamisoma. (In Japanese)Available online: http://webcache.googleusercontent.com/search?q=cache:0jXvOqWizIYJ:fec.jyoukamachi.com/report/2013/2013_report_1.pdf+&cd=1&hl=zh-CN&ct=clnk&gl=jp (accessed on 3 April 2014).
- Ministry of Agriculture Forestry and Fisheries, Japan. The Trend of Self-Sufficiency Rate and National Consciousness. (In Japanese)Available online: http://www.maff.go.jp/j/wpaper/w_maff/h22/pdf/z_1_1_2.pdf (accessed on 3 August 2014).
- Pröhl, G.; Ehlken, S.; Fiedler, I.; Kirchner, G.; Klemt, E.; Zibold, G. Ecological half-lives of 90Sr and 137Cs in terrestrial and aquatic ecosystems. J. Environ. Radioact. 2006, 91, 41–72. [Google Scholar]
- Yasutaka, T.; Naito, W.; Nakanishi, J. Cost and effectiveness of decontamination strategies in radiation contaminated areas in Fukushima in regard to external radiation dose. PloS ONE 2013, 8. [Google Scholar] [CrossRef]
- The International Commission on Radiological Protection. The 2007 Recommendations of the International Commission on Radiological Protection; Elsevier: Oxford, UK, 2007. [Google Scholar]
- Sugimoto, A.; Krull, S.; Nomura, S.; Morita, T.; Tsubokura, M. The voice of the most vulnerable: Lessons from the nuclear crisis in Fukushima, Japan. Bull. World Health Organ. 2012, 90, 629–630. [Google Scholar] [CrossRef] [PubMed]
- Von Hippel, F.N. The radiological and psychological consequences of the Fukushima daiichi accident. Bull. At. Sci. 2011, 67, 27–36. [Google Scholar]
- Norris, F.H.; Friedman, M.J.; Watson, P.J.; Byrne, C.M.; Diaz, E.; Kaniasty, K. 60,000 disaster victims speak: Part I. An empirical review of the empirical literature, 1981–2001. Psychiatry 2002, 65, 207–239. [Google Scholar]
- Chandra, A.; Acosta, J.D. Disaster recovery also involves human recovery. JAMA : J. Am. Med. Assoc. 2010, 304, 1608–1609. [Google Scholar]
- Powell, S.; Plouffe, L.; Gorr, P. When ageing and disasters collide: Lessons from 16 international case studies. Radiat. Prot. Dosim. 2009, 134, 202–206. [Google Scholar] [CrossRef]
- JA Kyosai Research Institute. The Suicide Caused by Earthquake: Direct Death and Indirect Death. (In Japanese)Available online: http://www.jkri.or.jp/PDF/2011/Rep117hamada.pdf (accessed on 3 April 2014).
- Brumfiel, G. Fukushima: Fallout of fear. Nature 2013, 493, 290–293. [Google Scholar]
- Slovic, P. Perception of risk from radiation. Radiat. Prot. Dosim. 1996, 68, 165–180. [Google Scholar] [CrossRef]
- NHK. Thyroid Cancer: Found in 18 Fukushima Children. Available online: http://www.youtube.com/watch?v=23dOVb76uzc (accessed on 29 August 2013).
- Leflar, R.; Hirata, A. Human flotsam, legal fallout: Japan’s tsunami and nuclear meltdown. J. Environ. Law Litig. 2012, 27, 107–124. [Google Scholar]
- Steinhauser, G. Fukushimas forgotten radionuclides: A review of the understudied radioactive emissions. Environ. Sci. Technol. 2014, 48, 4649–4663. [Google Scholar] [CrossRef] [PubMed]
- Landry, C.E.; Bin, O.; Hindsley, P.; Whitehead, J.C.; Wilson, K. Going home: Evacuation-Migration decisions of hurricane Katrina survivors. South. Econ. J. 2007, 74, 326–343. [Google Scholar]
- Chamlee-Wright, E.; Storr, V.H. “There’s no place like new Orleans”: Sense of place and community recovery in the ninth ward after hurricane Katrina. J. Urban. Aff. 2009, 31, 615–634. [Google Scholar]
- Falk, W.W.; Hunt, M.O.; Hunt, L.L. Hurricane Katrina and new Orleanians’ sense of place: Return and reconstitution or “Gone with the Wind”? Du Bois Rev.: Soc. Sci. Res. Race 2006, 3, 115–128. [Google Scholar]
- Graves, P.E. Migration and climate. J. Reg. Sci. 1980, 20, 227–237. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walker, R.; Ellis, M.; Barff, R. Linked migration systems: Immigration and internal labor flows in the United States. Econ. Geogr. 1992, 68, 234–248. [Google Scholar] [CrossRef] [PubMed]
- Greenwood, M.J. Human migration: Theory, models, and empirical studies. J. Reg. Sci. 1985, 25, 521–544. [Google Scholar] [CrossRef] [PubMed]
- Vigdor, J. The economic aftermath of hurricane Katrina. J. Econ. Perspect. 2008, 22, 135–154. [Google Scholar] [CrossRef]
- Nakanishi, T.M.; Keitaro, T. Agricultural Implications of the Fukushima Nuclear Accident; Springer: Tokyo, Japan, 2013. [Google Scholar]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Zhang, H.; Yan, W.; Oba, A.; Zhang, W. Radiation-Driven Migration: The Case of Minamisoma City, Fukushima, Japan, after the Fukushima Nuclear Accident. Int. J. Environ. Res. Public Health 2014, 11, 9286-9305. https://doi.org/10.3390/ijerph110909286
Zhang H, Yan W, Oba A, Zhang W. Radiation-Driven Migration: The Case of Minamisoma City, Fukushima, Japan, after the Fukushima Nuclear Accident. International Journal of Environmental Research and Public Health. 2014; 11(9):9286-9305. https://doi.org/10.3390/ijerph110909286
Chicago/Turabian StyleZhang, Hui, Wanglin Yan, Akihiro Oba, and Wei Zhang. 2014. "Radiation-Driven Migration: The Case of Minamisoma City, Fukushima, Japan, after the Fukushima Nuclear Accident" International Journal of Environmental Research and Public Health 11, no. 9: 9286-9305. https://doi.org/10.3390/ijerph110909286
APA StyleZhang, H., Yan, W., Oba, A., & Zhang, W. (2014). Radiation-Driven Migration: The Case of Minamisoma City, Fukushima, Japan, after the Fukushima Nuclear Accident. International Journal of Environmental Research and Public Health, 11(9), 9286-9305. https://doi.org/10.3390/ijerph110909286