
Repetitive Daily Point of Choice Prompts and Occupational Sit-Stand Transfers, Concentration and Neuromuscular Performance in Office Workers: An RCT

Abstract
:1. Introduction
2. Methods
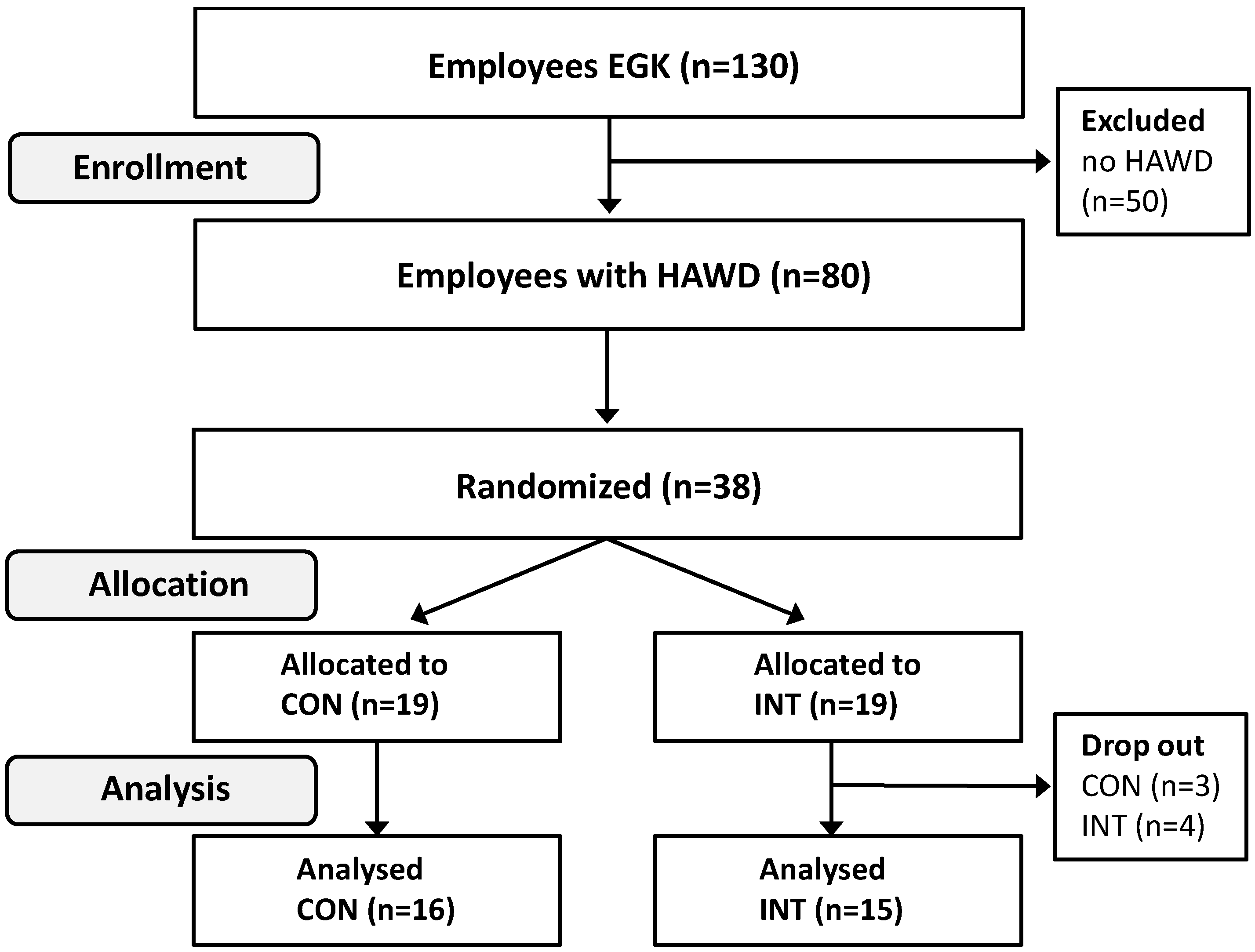
2.1. Study Design and Participants

{kind=link}
{kind=link}
| Demographical data | INT (n = 15) | CON (n = 16) | ||||||
|---|---|---|---|---|---|---|---|---|
| gender (m/f) | 4/11 | 4/12 | ||||||
| Pre | Post | Pre | Post | |||||
| age (years) | 45 (12) | 40 (10) | ||||||
| height (cm) | 167.4 (9.0) | 168.7 (10) | ||||||
| weight (kg) | 65.8 | (12.9) | 65.4 | (12.7) | 70.4 | (15.7) | 69.9 | (14.0) |
| BMI (kg/m²) | 23.7 | (3.7) | 23.7 | (3.7) | 24.7 | (5.0) | 24.6 | (4.3) |
| body fat (%) | 28.2 | (7.3) | 27.4 | (7.2) | 28.3 | (8.3) | 29.0 | (7.9) |
| physical activity (h/week) | 6.2 | (5.0) | 7.0 | (4.7) | 6.2 | (4.0) | 7.1 | (7.6) |
| working time (h/week) | 39 | (8) | 39 | (9) | 36 | (9) | 36 | (9) |

2.2. Outcome Measures
2.2.1. Standing and Sitting Time Assessment
2.2.2. Concentration
2.2.3. Neuromuscular Outcomes
2.3. Point of Choice Prompt Intervention
2.4. Statistical Analysis
3. Results
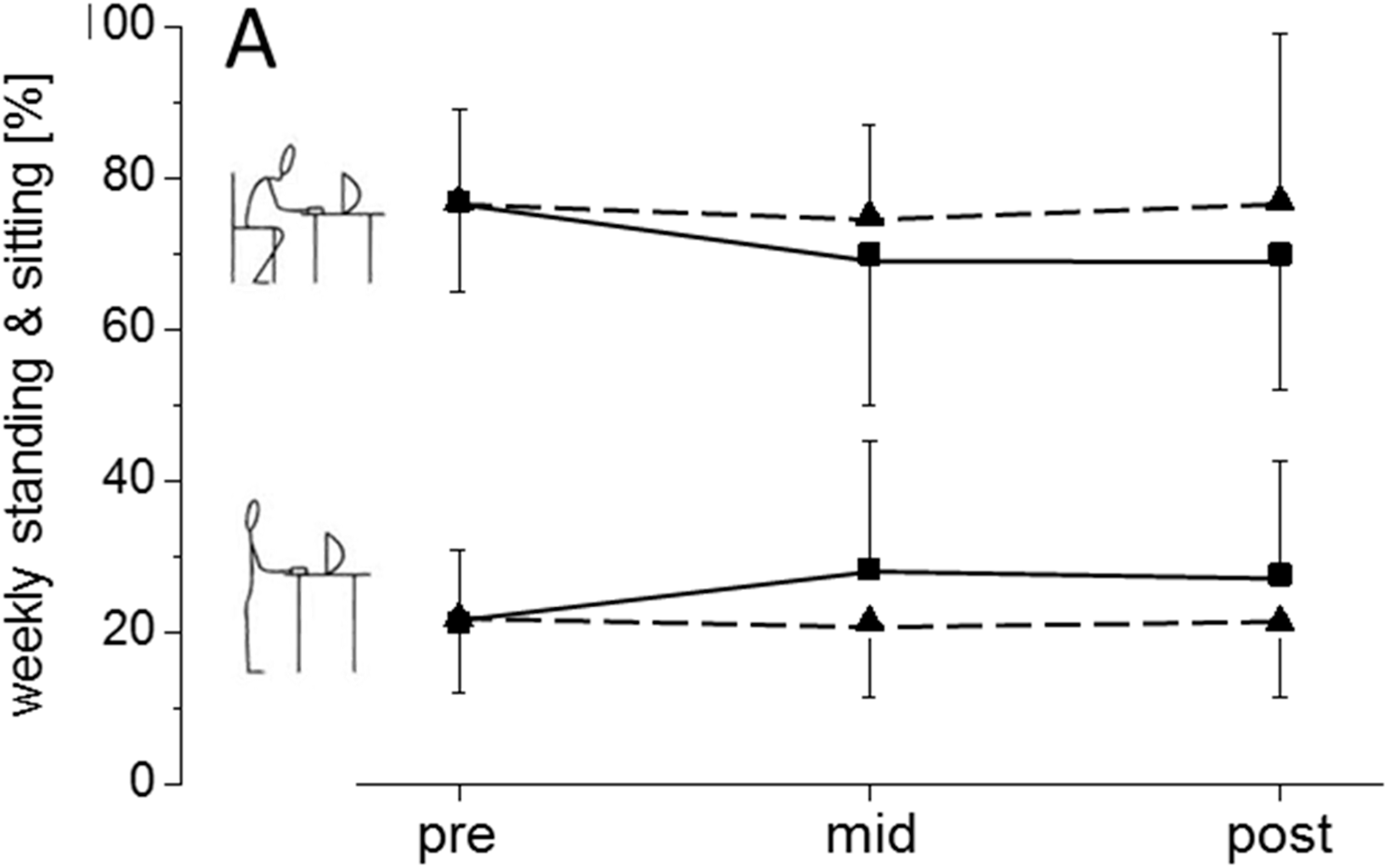
3.1. Sitting and Standing Time Proportions

| Performance Data | INT | CON | rANOVA | |||||
|---|---|---|---|---|---|---|---|---|
| Pre | Post | Pre | Post | Time-Effect | ηp2 | Group × Time Interaction | ηp2 | |
| Standing time (hours per week) | 7.2 (4.8) | 9.7 (6.6) | 6.2 (3.0) | 6.0 (3.0) | p = 0.18 | 0.06 | p = 0.09 | 0.09 |
| Sitting time (hours per week) | 29.4 (6.5) | 27.8 (10.7) | 27.7 (9.5) | 27.5 (9.2) | p = 0.55 | 0.01 | p = 0.63 | 0.008 |
| CONP | 157 (52) | 181 (52) | 154 (36) | 179 (37) | p < 0.001 | 0.73 | p = 0.80 | 0.002 |
| %ERR | 6.0 (5.1) | 4.1 (3.4) | 9.8 (8.4) | 6.0 (6.1) | p = 0.004 | 0.25 | p = 0.52 | 0.01 |
| DLEC | 143 (27) | 134 (17) | 150 (34) | 143 (25) | p = 0.09 | 0.09 | p = 0.95 | <0.001 |
| SLEO | 439 (129) | 400 (126) | 447 (158) | 403 (143) | p = 0.009 | 0.21 | p = 0.87 | <0.001 |
| SLEO + COG | 514 (166) | 449 (146) | 492 (161) | 473 (132) | p = 0.03 | 0.15 | p = 0.23 | 0.05 |
| SLEO + COG and +MOT | 472 (175) | 466 (154) | 512 (163) | 481 (158) | p = 0.20 | 0.06 | p = 0.38 | 0.02 |
| repetitions | 37 (16) | 34 (18) | 35 (14) | 34 (13) | p = 0.44 | 0.02 | p = 0.76 | 0.003 |
| perceived exertion | 7 (2) | 7 (2) | 7 (2) | 7 (2) | p = 0.92 | <0.001 | p = 0.70 | 0.005 |
3.2. Concentration
3.3. Strength-Endurance and Balance Outcome
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Van Uffelen, J.G.; Wong, J.; Chau, J.Y.; van der Ploeg, H.P.; Riphagen, I.; Gilson, N.D.; Burton, N.W.; Healy, G.N.; Thorp, A.A.; Clark, B.K.; et al. Occupational sitting and health risks: A systematic review. Amer. J. Prev. Med. 2010, 39, 379–388. [Google Scholar] [CrossRef] [Green Version]
- Pate, R.R.; O’Neill, J.R.; Lobelo, F. The evolving definition of “sedentary”. Exerc. Sport. Sci. Rev. 2008, 36, 173–178. [Google Scholar] [CrossRef] [PubMed]
- Chau, J.Y.; Grunseit, A.C.; Chey, T.; Stamatakis, E.; Brown, W.J.; Matthews, C.E.; Bauman, A.E.; van der Ploeg, H.P. Daily sitting time and all-cause mortality: A meta-analysis. PLoS One 2013, 8. [Google Scholar] [CrossRef] [PubMed]
- Fenety, A.; Walker, J.M. Short-term effects of workstation exercises on musculoskeletal discomfort and postural changes in seated video display unit workers. Phys. Ther. 2002, 82, 578–589. [Google Scholar] [PubMed]
- Owen, N.; Healy, G.N.; Matthews, C.E.; Dunstan, D.W. Too much sitting: The population health science of sedentary behavior. Exerc. Sport. Sci. Rev. 2010, 38, 105–113. [Google Scholar] [CrossRef] [PubMed]
- Owen, N.; Bauman, A.; Brown, W. Too much sitting: A novel and important predictor of chronic disease risk? Brit. J. Sport. Med. 2009, 43, 81–83. [Google Scholar] [CrossRef]
- Evans, R.E.; Fawole, H.O.; Sheriff, S.A.; Dall, P.M.; Grant, P.M.; Ryan, C.G. Point-of-choice prompts to reduce sitting time at work: A randomized trial. Amer. J. Prev. Med. 2012, 43, 293–297. [Google Scholar] [CrossRef]
- Gilson, N.D.; Puig-Ribera, A.; McKenna, J.; Brown, W.J.; Burton, N.W.; Cooke, C.B. Do walking strategies to increase physical activity reduce reported sitting in workplaces: A randomized control trial. Int. J. Behav. Nutr. Phys. Act. 2009, 6, 293–297. [Google Scholar]
- Parry, S.; Straker, L. The contribution of office work to sedentary behaviour associated risk. BMC Public Health 2013, 13. [Google Scholar] [CrossRef]
- Ryan, C.G.; Dall, P.M.; Granat, M.H.; Grant, P.M. Sitting patterns at work: Objective measurement of adherence to current recommendations. Ergonomics 2011, 54, 531–538. [Google Scholar] [CrossRef] [Green Version]
- Chau, J.Y.; Daley, M.; Dunn, S.; Srinivasan, A.; Do, A.; Bauman, A.E.; van der Ploeg, H.P. The effectiveness of sit-stand workstations for changing office workers inverted question mark sitting time: Results from the stand at work randomized controlled trial pilot. Int. J. Behav. Nutr. Phys. Act. 2014, 11. [Google Scholar] [CrossRef] [PubMed]
- Pronk, N.P.; Katz, A.S.; Lowry, M.; Payfer, J.R. Reducing occupational sitting time and improving worker health: The take-a-stand project, 2011. Prev. Chronic Dis. 2012, 9. [Google Scholar] [CrossRef]
- Gilson, N.D.; Suppini, A.; Ryde, G.C.; Brown, H.E.; Brown, W.J. Does the use of standing “hot” desks change sedentary work time in an open plan office? Prev. Med. 2012, 54, 65–67. [Google Scholar] [CrossRef] [PubMed]
- Healy, G.N.; Eakin, E.G.; Lamontagne, A.D.; Owen, N.; Winkler, E.A.; Wiesner, G.; Gunning, L.; Neuhaus, M.; Lawler, S.; Fjeldsoe, B.S.; et al. Reducing sitting time in office workers: Short-term efficacy of a multicomponent intervention. Prev. Med. 2013, 57, 43–48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alkhajah, T.A.; Reeves, M.M.; Eakin, E.G.; Winkler, E.A.; Owen, N.; Healy, G.N. Sit-stand workstations: A pilot intervention to reduce office sitting time. Amer. J. Prev. Med. 2012, 43, 298–303. [Google Scholar] [CrossRef] [Green Version]
- Neuhaus, M.; Healy, G.N.; Dunstan, D.W.; Owen, N.; Eakin, E.G. Workplace sitting and height-adjustable workstations: A randomized controlled trial. Amer. J. Prev. Med. 2014, 46, 30–40. [Google Scholar] [CrossRef]
- Nocon, M.; Muller-Riemenschneider, F.; Nitzschke, K.; Willich, S.N. Review article: Increasing physical activity with point-of-choice prompts—A systematic review. Scand. J. Public Health 2010, 38, 633–638. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, S.J.; Cooley, P.D.; Mainsbridge, C. An e-health intervention designed to increase workday energy expenditure by reducing prolonged occupational sitting habits. Work 2014, 49, 289–295. [Google Scholar] [PubMed]
- Swartz, A.M.; Rote, A.E.; Welch, W.A.; Maeda, H.; Hart, T.L.; Cho, Y.I.; Strath, S.J. Prompts to disrupt sitting time and increase physical activity at work, 2011–2012. Prev. Chronic Dis. 2014, 11. [Google Scholar] [CrossRef] [PubMed]
- Miles-Chan, J.L.; Sarafian, D.; Montani, J.P.; Schutz, Y.; Dulloo, A. Heterogeneity in the energy cost of posture maintenance during standing relative to sitting: Phenotyping according to magnitude and time-course. PLoS One 2013, 8. [Google Scholar] [CrossRef] [PubMed]
- Saffer, M.; Kiemel, T.; Jeka, J. Coherence analysis of muscle activity during quiet stance. Exp. Brain Res. 2008, 185, 215–226. [Google Scholar] [CrossRef] [PubMed]
- Granacher, U.; Wick, C.; Rueck, N.; Esposito, C.; Roth, R.; Zahner, L. Promoting balance and strength in the middle-aged workforce. Int. J. Sport. Med. 2011, 32, 35–44. [Google Scholar] [CrossRef]
- Pelclova, J.; Gaba, A.; Tlucakova, L.; Pospiech, D. Association between physical activity (PA) guidelines and body composition variables in middle-aged and older women. Arch. Gerontol. Geriatr. 2012, 55, 14–20. [Google Scholar] [CrossRef]
- Frey, I.; Berg, A.; Grathwohl, D.; Keul, J. Freiburg questionnaire of physical activity—Development, evaluation and application. Soz. Pravent. 1999, 44, 55–64. [Google Scholar] [CrossRef]
- Pocock, S.J.; Simon, R. Sequential treatment assignment with balancing for prognostic factors in the controlled clinical trial. Biometrics 1975, 31, 103–115. [Google Scholar] [CrossRef] [PubMed]
- Lagersted-Olsen, J.; Korshoj, M.; Skotte, J.; Carneiro, I.G.; Sogaard, K.; Holtermann, A. Comparison of objectively measured and self-reported time spent sitting. Int. J. Sport. Med. 2014, 35, 534–540. [Google Scholar]
- Steeves, J.A.; Bowles, H.R.; McClain, J.J.; Dodd, K.W.; Brychta, R.J.; Wang, J.; Chen, K.Y. Ability of thigh-worn actigraph and activpal monitors to classify posture and motion. Med. Sci. Sport. Exercise 2014. [Google Scholar] [CrossRef]
- Skotte, J.; Korshøj, M.; Kristiansen, J.; Hanisch, C.; Holtermann, A. Detection of physical activity types using triaxial accelerometers. J. Phys. Act. Health 2012. [Google Scholar] [CrossRef]
- Choi, L.; Liu, Z.; Matthews, C.E.; Buchowski, M.S. Validation of accelerometer wear and nonwear time classification algorithm. Med. Sci.Sport. Exercise 2011, 43, 357–364. [Google Scholar] [CrossRef]
- Brickenkamp, R.; Schmidt-Atzert, L.; Liepmann, D. Test D2—Revision; Hogrefe: Göttingen, Germany, 2010. [Google Scholar]
- Donath, L.; Roth, R.; Zahner, L.; Faude, O. Testing single and double limb standing balance performance: Comparison of COP path length evaluation between two devices. Gait Posture 2012, 36, 439–443. [Google Scholar] [CrossRef] [PubMed]
- Coren, S. The lateral preference inventory for measurement of handedness, footedness, eyedness, and earedness: Norms for young adults. Bull. Psych. Soc. 1993, 31, 1–3. [Google Scholar] [CrossRef]
- Lunsford, B.R.; Perry, J. The standing heel-rise test for ankle plantar flexion: Criterion for normal. Phys. Ther. 1995, 75, 694–698. [Google Scholar] [PubMed]
- Neely, G.; Ljunggren, G.; Sylven, C.; Borg, G. Comparison between the visual analogue scale (VAS) and the category ratio scale (CR-10) for the evaluation of leg exertion. Int. J. Sport. Med. 1992, 13, 133–136. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for The Behavior Sciences, 2nd ed.; Lawrence Erlbaum Associates: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Levine, J.A.; Schleusner, S.J.; Jensen, M.D. Energy expenditure of nonexercise activity. Amer. J. Clin. Nutr. 2000, 72, 1451–1454. [Google Scholar] [PubMed]
- Webb, O.J.; Eves, F.F. Promoting stair climbing: Effects of message specificity and validation. Health Educ. Res. 2007, 22, 49–57. [Google Scholar] [PubMed]
- Eckhardt, M.R.; Kerr, J.; Taylor, W.C. Point-of-decision signs and stair use in a university worksite setting: General vs. specific messages. Amer. J. Health Promotion 2014. [Google Scholar] [CrossRef]
- Wressle, E.; Samuelsson, K. High job demands and lack of time: A future challenge in occupational therapy. Scand. J. Occup. Ther. 2014, 21, 421–428. [Google Scholar] [CrossRef]
- Gallagher, K.M.; Campbell, T.; Callaghan, J.P. The influence of a seated break on prolonged standing induced low back pain development. Ergonomics 2014, 57, 555–562. [Google Scholar] [CrossRef] [PubMed]
- Fry, J.P.; Neff, R.A. Periodic prompts and reminders in health promotion and health behavior interventions: Systematic review. J. Med. Internet. Res. 2009, 11. [Google Scholar] [CrossRef] [PubMed]
- Kreuter, M.W.; Wray, R.J. Tailored and targeted health communication: Strategies for enhancing information relevance. Amer. J. Health Behav. 2003, 27, S227–S232. [Google Scholar] [CrossRef]
- Cooley, D.; Pedersen, S. A pilot study of increasing nonpurposeful movement breaks at work as a means of reducing prolonged sitting. J. Environ. Public Health 2013. [Google Scholar] [CrossRef]
- Parry, S.; Straker, L.; Gilson, N.D.; Smith, A.J. Participatory workplace interventions can reduce sedentary time for office workers—A randomised controlled trial. PLoS One 2013, 8. [Google Scholar] [CrossRef] [PubMed]
- Dutta, N.; Koepp, G.A.; Stovitz, S.D.; Levine, J.A.; Pereira, M.A. Using sit-stand workstations to decrease sedentary time in office workers: A randomized crossover trial. Int. J. Environ. Res. Public Health 2014, 11, 6653–6665. [Google Scholar] [PubMed]
- Grunseit, A.C.; Chau, J.Y.; van der Ploeg, H.P.; Bauman, A. “Thinking on your feet”: A qualitative evaluation of sit-stand desks in an Australian workplace. BMC Public Health 2013, 13. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.K.; Etnier, J.L.; Barella, L.A. Exploring the relationship between exercise-induced arousal and cognition using fractionated response time. Res. Quart. Exercise Sport. 2009, 80, 78–86. [Google Scholar] [CrossRef]
- Thorp, A.A.; Kingwell, B.A.; Owen, N.; Dunstan, D.W. Breaking up workplace sitting time with intermittent standing bouts improves fatigue and musculoskeletal discomfort in overweight/obese office workers. Occup. Environ. Medicine 2014, 71, 765–771. [Google Scholar]
- Thorp, A.A.; Kingwell, B.A.; Sethi, P.; Hammond, L.; Owen, N.; Dunstan, D.W. Alternating bouts of sitting and standing attenuate postprandial glucose responses. Med. Sci. Sport. Exercise 2014, 46, 2053–2061. [Google Scholar] [CrossRef]
- Muehlbauer, T.; Roth, R.; Bopp, M.; Granacher, U. An exercise sequence for progression in balance training. J. Strength Cond. Res. 2012, 26, 568–574. [Google Scholar] [CrossRef] [PubMed]
- Gruber, M.; Gollhofer, A. Impact of sensorimotor training on the rate of force development and neural activation. Eur. J. Appl. Physiol. 2004, 92, 98–105. [Google Scholar] [CrossRef] [PubMed]
- Faude, O.; Donath, L.; Bopp, M.; Hofmann, S.; Erlacher, D.; Zahner, L. Neuromuscular training in construction workers: A longitudinal controlled pilot study. Int. Arch. Occup. Environ. Health 2014. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Donath, L.; Faude, O.; Schefer, Y.; Roth, R.; Zahner, L. Repetitive Daily Point of Choice Prompts and Occupational Sit-Stand Transfers, Concentration and Neuromuscular Performance in Office Workers: An RCT. Int. J. Environ. Res. Public Health 2015, 12, 4340-4353. https://doi.org/10.3390/ijerph120404340
Donath L, Faude O, Schefer Y, Roth R, Zahner L. Repetitive Daily Point of Choice Prompts and Occupational Sit-Stand Transfers, Concentration and Neuromuscular Performance in Office Workers: An RCT. International Journal of Environmental Research and Public Health. 2015; 12(4):4340-4353. https://doi.org/10.3390/ijerph120404340
Chicago/Turabian StyleDonath, Lars, Oliver Faude, Yannick Schefer, Ralf Roth, and Lukas Zahner. 2015. "Repetitive Daily Point of Choice Prompts and Occupational Sit-Stand Transfers, Concentration and Neuromuscular Performance in Office Workers: An RCT" International Journal of Environmental Research and Public Health 12, no. 4: 4340-4353. https://doi.org/10.3390/ijerph120404340
APA StyleDonath, L., Faude, O., Schefer, Y., Roth, R., & Zahner, L. (2015). Repetitive Daily Point of Choice Prompts and Occupational Sit-Stand Transfers, Concentration and Neuromuscular Performance in Office Workers: An RCT. International Journal of Environmental Research and Public Health, 12(4), 4340-4353. https://doi.org/10.3390/ijerph120404340