
Smoking Cessation among Low-Socioeconomic Status and Disadvantaged Population Groups: A Systematic Review of Research Output

 ,
,
Abstract
:1. Introduction
- (i)
- Total published research output (reviews, non-data based publications, data-based publications (descriptive, measurement and intervention research)) would have significantly increased;
- (ii)
- The proportion of the total published output that is intervention research would have significantly increased; and
- (iii)
- The methodological quality of the published intervention research would have significantly increased: (a) the proportion of intervention studies using Cochrane Effective Practice Organisation of Care (EPOC)-accepted evaluation designs: randomised controlled trial (RCT), controlled clinical trial (CCT), controlled before and after (CBA) study, or interrupted time series (ITS) would have significantly increased; and (b) the proportion of intervention studies using biochemical verification of self-reported smoking abstinence would have significantly increased.
2. Method
2.1. Data Sources
Search Strategy, Selection of Studies and Coding


2.2. Study Selection
2.3. Data Extraction
2.3.1. Publication Volume and Types
2.3.2. Evaluation Designs and Biochemical Verification
2.4. Statistical Analyses
3. Results
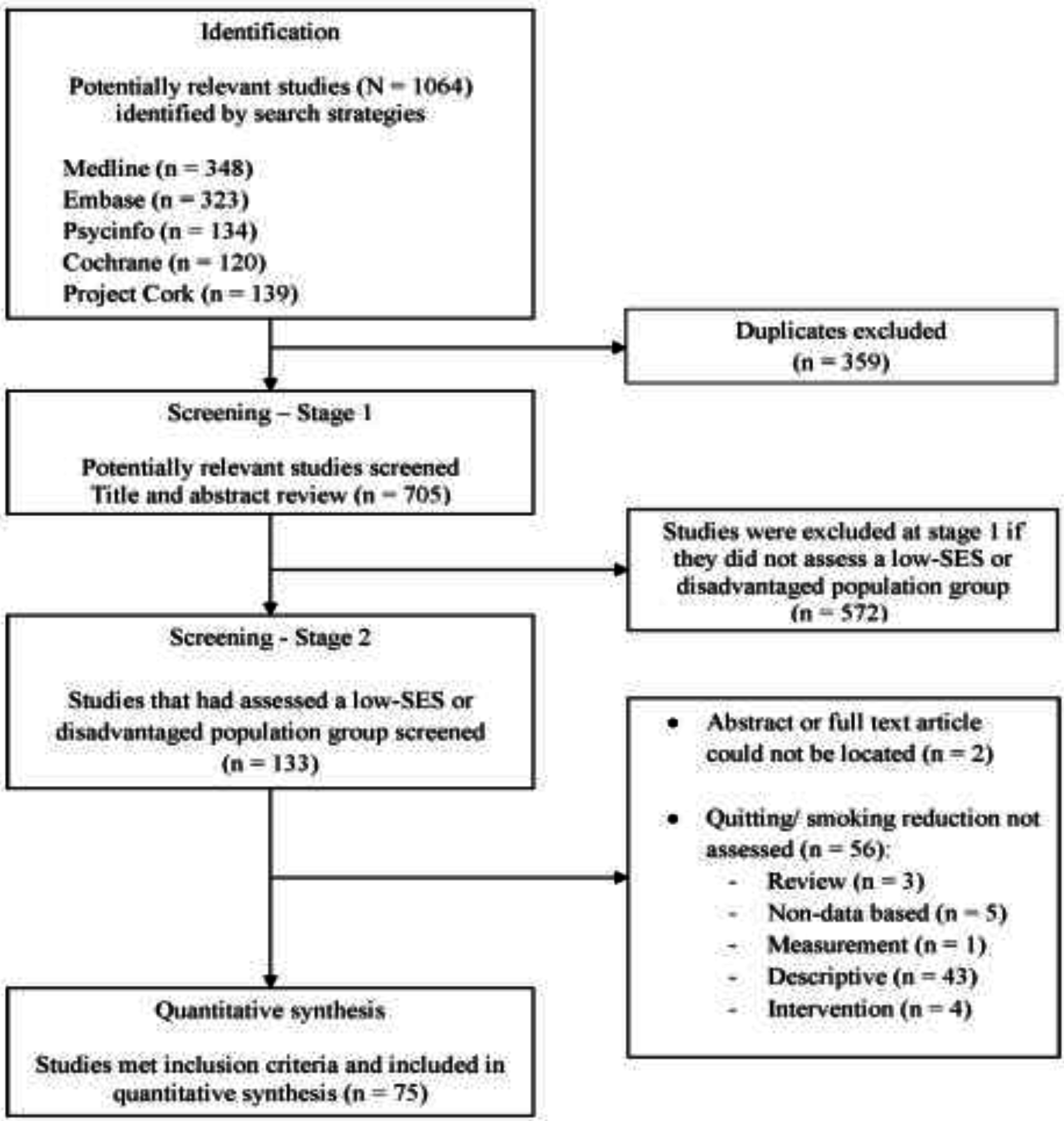
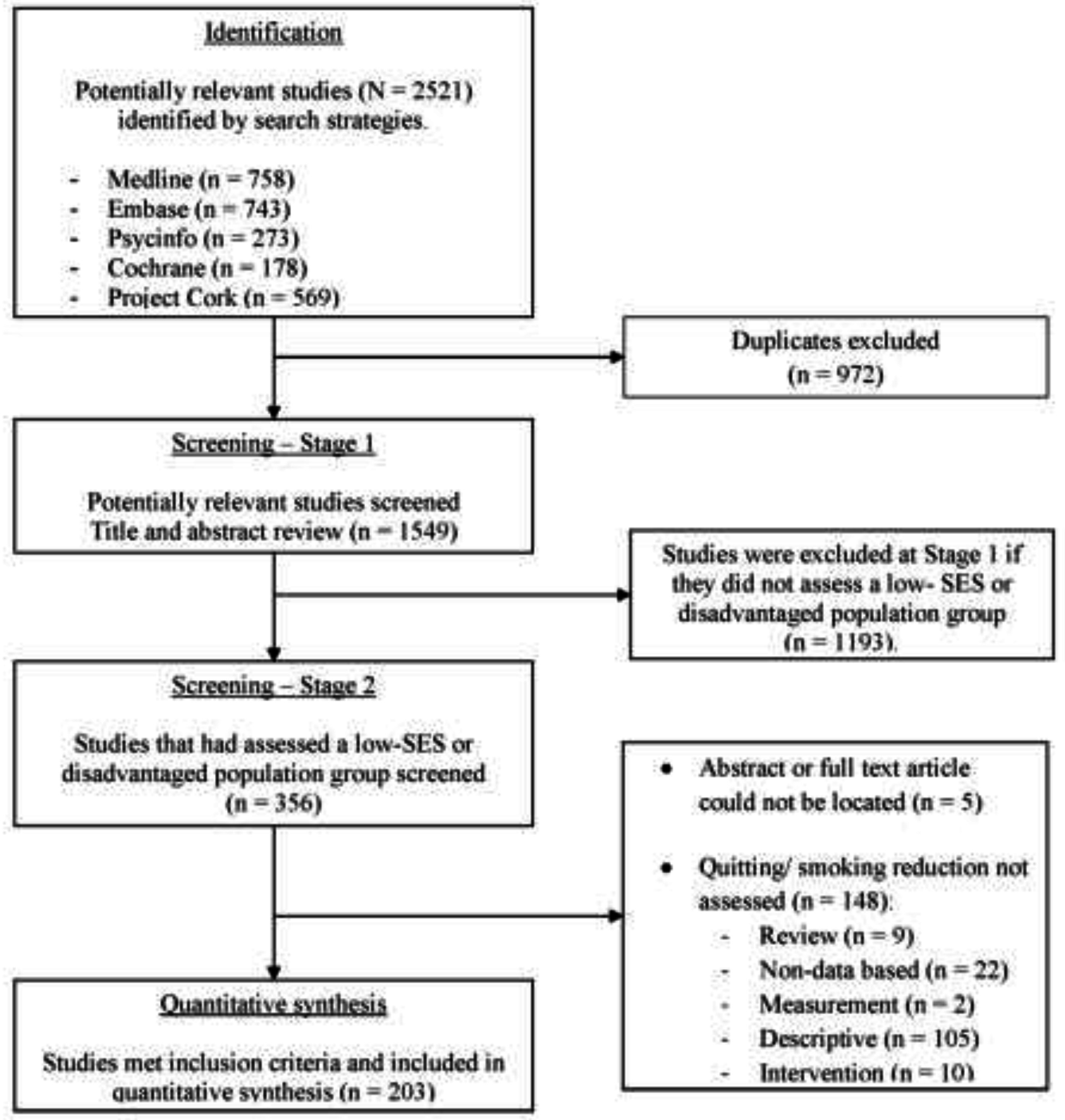
3.1. Data Synthesis
Identification of Studies
3.2. Volume of Research

{kind=link}
{kind=link}
| Country | TP1 | TP2 | ||
|---|---|---|---|---|
| Descriptive a | Intervention | Descriptive | Intervention | |
| Australia/New Zealand | 1 (25%) | 3 (75%) | 4 (31%) | 9 (69%) |
| United States/Canada | 6 (19%) | 26 (81%) | 31 (36%) | 54 (64%) |
| United Kingdom | 2 (40%) | 3 (60%) | 0 (0%) | 1 (100%) |
| Other | 1 (50%) | 1 (50%) | 2 (15%) | 11 (85%) |
| Total | 10 | 33 | 37 | 75 |
3.3. Specific Low-SES and Disadvantaged Populations by Country
| Country | TP1 | TP2 | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Low-SES/ Homeless | Mental Illness | Prisoners | At-risk Youth | Indigenous | Total | Low-SES/ Homeless | Mental Illness | Prisoners | At-risk Youth | Indigenous | Total | |
| Australia/ New Zealand | 0 (0%) | 5 (45%) | 2 (18%) | 0 (0%) | 4 (36%) | 11 | 5 (15%) | 12 (35%) | 4 (12%) | 0 (0%) | 13 (38%) | 34 |
| United States/ Canada | 11 (21%) | 29 (56%) | 1 (2%) | 7 (13%) | 4 (8%) | 52 | 33 (24%) | 76 (55%) | 7 (5%) | 7 (5%) | 16 (12%) | 139 |
| United Kingdom | 8 (89%) | 0 (0%) | 1 (11%) | 0 (0%) | 0 (0%) | 9 | 2 (29%) | 4 (57%) | 1 (14%) | 0 (0%) | 0 (0%) | 7 |
| Other | 0 (0%) | 3 (100%) | 0 (0%) | 0 (0%) | 0 (0%) | 3 | 5 (22%) | 18 (78%) | 0 (0%) | 0 (0%) | 0 (0%) | 23 |
| Total | 19 (25%) | 37 (49%) | 4 (5%) | 7 (9%) | 8 (11%) | 75 | 45 (22%) | 110 (54%) | 12 (6%) | 7 (3%) | 29 (14%) | 203 |
3.4. Proportion of Intervention Studies
| Country | TP1 | TP2 | ||||||
|---|---|---|---|---|---|---|---|---|
| EPOC | Non-EPOC | Total | EPOC | Non-EPOC | Total | |||
| RCT | CCT | RCT | CCT | |||||
| Australia/New Zealand | 1 (33%) | 0 (0%) | 2 (67%) | 3 | 2 (22%) | 0 (0%) | 7 (78%) | 9 |
| United States/Canada | 17 (65%) | 0 (0%) | 9 (35%) | 26 | 34 (63%) | 1 (2%) | 19 (35%) | 54 |
| United Kingdom | 2 (67%) | 0 (0%) | 1 (33%) | 3 | 0 (0%) | 0 (0%) | 1 (100%) | 1 |
| Other | 1 (100%) | 0 (0%) | 0 (0%) | 1 | 7 (64%) | 0 (0%) | 4 (36%) | 11 |
| Total | 21 (64%) | 0 (0%) | 12 (36%) | 33 | 43 (57%) | 1 (1%) | 31 (41%) | 75 |
3.5. Methodological Quality of Intervention Studies
3.5.1. Evaluation Designs
| Country | TP1 | TP2 | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Low-SES/ Homeless | Mental Illness | Prisoners | At-risk Youth | Indigenous | Total | Low-SES/ Homeless | Mental Illness | Prisoners | At-risk Youth | Indigenous | Total | |
| Australia/ New Zealand | 0 (0%) | 1 (100%) | 0 (0%) | 0 (0%) | 0 (0%) | 1 | 0 (0%) | 1 (50%) | 0 (0%) | 0 (0%) | 1 (50%) | 2 |
| United States/ Canada | 4 (24%) | 9 (53%) | 0 (0%) | 3 (18%) | 1 (6%) | 17 | 9 (26%) | 19 (54%) | 4 (11%) | 2 (6%) | 1 (3%) | 35 |
| United Kingdom | 2 (100%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | 2 | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 |
| Other | 0 (0%) | 1 (100%) | 0 (0%) | 0 (0%) | 0 (0%) | 1 | 1 (14%) | 6 (86%) | 0 (0%) | 0 (0%) | 0 (0%) | 7 |
| Total | 6 (29%) | 11 (52%) | 0 (0%) | 3 (14%) | 1 (5%) | 21 | 10 (23%) | 26 (59%) | 4 (9%) | 2 (5%) | 2 (5%) | 44 |
3.5.2. Use of Biochemical Verification
4. Discussion
4.1. Summary of Findings
4.2. Increasing Output of Methodologically Rigorous Intervention Research
Using Accepted EPOC Evaluation Designs
4.3. Increasing the Use of Biochemical Verification of Self-Reported Abstinence
4.4. Study Limitations
5. Conclusions
Acknowledgments
Author Contributions
Appendix
Search Terms for Identification and Selection of Studies
| Section/Topic | # | Checklist Item | Reported on Page # |
|---|---|---|---|
| TITLE | |||
| Title | 1 | Identify the report as a systematic review, meta-analysis, or both. | 1 |
| ABSTRACT | |||
| Structured summary | 2 | Provide a structured summary including, as applicable: background; objectives; data sources; study eligibility criteria, participants, and interventions; study appraisal and synthesis methods; results; limitations; conclusions and implications of key findings; systematic review registration number. | 1-2 |
| INTRODUCTION | |||
| Rationale | 3 | Describe the rationale for the review in the context of what is already known. | 2-4–5 |
| Objectives | 4 | Provide an explicit statement of questions being addressed with reference to participants, interventions, comparisons, outcomes, and study design (PICOS). | 3-4 |
| METHODS | |||
| Protocol and registration | 5 | Indicate if a review protocol exists, if and where it can be accessed (e.g., Web address), and, if available, provide registration information including registration number. | N/A |
| Eligibility criteria | 6 | Specify study characteristics (e.g., PICOS, length of follow-up) and report characteristics (e.g., years considered, language, publication status) used as criteria for eligibility, giving rationale. | 6 |
| Information sources | 7 | Describe all information sources (e.g., databases with dates of coverage, contact with study authors to identify additional studies) in the search and date last searched. | 6 |
| Search | 8 | Present full electronic search strategy for at least one database, including any limits used, such that it could be repeated. | Online appendix |
| Study selection | 9 | State the process for selecting studies (i.e., screening, eligibility, included in systematic review, and, if applicable, included in the meta-analysis). | 6 + Figures |
| Data collection process | 10 | Describe method of data extraction from reports (e.g., piloted forms, independently, in duplicate) and any processes for obtaining and confirming data from investigators. | N/A |
| Data items | 11 | List and define all variables for which data were sought (e.g., PICOS, funding sources) and any assumptions and simplifications made. | 6–7 |
| Risk of bias in individual studies | 12 | Describe methods used for assessing risk of bias of individual studies (including specification of whether this was done at the study or outcome level), and how this information is to be used in any data synthesis. | 7. EPOC checklist |
| Summary measures | 13 | State the principal summary measures (e.g., risk ratio, difference in means). | 7 |
| Synthesis of results | 14 | Describe the methods of handling data and combining results of studies, if done, including measures of consistency (e.g., I2) for each meta-analysis. | 7 |
| Risk of bias across studies | 15 | Specify any assessment of risk of bias that may affect the cumulative evidence (e.g., publication bias, selective reporting within studies). | 12 |
| Additional analyses | 16 | Describe methods of additional analyses (e.g., sensitivity or subgroup analyses, meta-regression), if done, indicating which were pre-specified. | N/A |
| RESULTS | |||
| Study selection | 17 | Give numbers of studies screened, assessed for eligibility, and included in the review, with reasons for exclusions at each stage, ideally with a flow diagram. | 8 + Figures |
| Study characteristics | 18 | For each study, present characteristics for which data were extracted (e.g., study size, PICOS, follow-up period) and provide the citations. | 7 |
| Risk of bias within studies | 19 | Present data on risk of bias of each study and, if available, any outcome level assessment (see item 12). | 7. EPOC checklist |
| Results of individual studies | 20 | For all outcomes considered (benefits or harms), present, for each study: (a) simple summary data for each intervention group (b) effect estimates and confidence intervals, ideally with a forest plot. | N/A |
| Synthesis of results | 21 | Present results of each meta-analysis done, including confidence intervals and measures of consistency. | N/A |
| Risk of bias across studies | 22 | Present results of any assessment of risk of bias across studies (see Item 15). | N/A |
| Additional analysis | 23 | Give results of additional analyses, if done (e.g., sensitivity or subgroup analyses, meta-regression (see Item 16)). | N/A |
| DISCUSSION | |||
| Summary of evidence | 24 | Summarize the main findings including the strength of evidence for each main outcome; consider their relevance to key groups (e.g., healthcare providers, users, and policy makers). | 10–13 |
| Limitations | 25 | Discuss limitations at study and outcome level (e.g., risk of bias), and at review-level (e.g., incomplete retrieval of identified research, reporting bias). | 12 |
| Conclusions | 26 | Provide a general interpretation of the results in the context of other evidence, and implications for future research. | 13 |
| FUNDING | |||
| Funding | 27 | Describe sources of funding for the systematic review and other support (e.g., supply of data); role of funders for the systematic review. | 13 |
Conflicts of Interest
References
- Chaloupka, F.J.; The World Bank. Curbing the epidemic: Governments and the economics of tobacco control. Tob. Control 1999, 8, 196–201. [Google Scholar]
- Ezzati, M.; Lopez, A.D. Estimates of global mortality attributable to smoking in 2000. Lancet 2003, 362, 847–852. [Google Scholar] [CrossRef]
- Australian Institute of Health and Welfare. 2010 National Drug Strategy Household Survey Report. Available online: http://www.aihw.gov.au/publication-detail/?id=32212254712 (accessed on 15 January 2014).
- Centers for Disease Control & Prevention. Cigarette smoking among adults and trends in smoking cessation—United States, 2008. Morb. Mort. Wkly. Rep. 2008, 58, 1227–1258. [Google Scholar]
- Reid, J.L.; Hammond, D.; Boudreau, C.; Fong, G.T.; Siahpush, M. Socioeconomic disparities in quit intentions, quit attempts, and smoking abstinence among smokers in four western countries: Findings from the International Tobacco Control Four Country Survey. Nicotine Tob. Res. 2010, 12, S20–S33. [Google Scholar] [CrossRef] [PubMed]
- Siahpush, M.; McNeill, A.; Borland, R.; Fong, G.T. Socioeconomic variations in nicotine dependence, self-efficacy, and intention to quit across four countries: Findings from the International Tobacco Control (ITC) Four Country Survey. Tob. Control 2006, 15, iii71–iii75. [Google Scholar] [CrossRef] [PubMed]
- Global Tobacco Surveillance System. Available online: http://www.who.int/tobacco/surveillance/en/ (accessed on 15 February 2014).
- STEPwise Approach to Surveillance. Available online: http://www.who.int/chp/steps/en/ (accessed on 17 February 2014).
- World Health Survey. Available online: http://www.who.int/healthinfo/survey/en/ (accessed on 12 February 2014).
- Hozzeinpoor, A.R.; Parker, L.A.; d’Espaignet, E.T.; Chatterji, S. Social determinants of smoking in low- and middle-income countries: Results from the World Health Survey. PLoS ONE 2011, 6. [Google Scholar] [CrossRef]
- Le Cook, B.; Wayne, G.F.; Kafali, N.; Liu, Z.; Shu, C.; Flores, M. Trends in smoking among adults with mental illness and association between mental health treatment and smoking cessation. JAMA 2014, 311, 177–182. [Google Scholar]
- Baggett, T.P.; Rigotti, N.A. Cigarette smoking and advice to quit in a national sample of homeless adults. Am. J. Prev. Med. 2010, 39, 164–172. [Google Scholar] [CrossRef] [PubMed]
- Connor, S.E.; Cook, R.L.; Herbert, M.I.; Neal, S.M.; Williams, J.T. Smoking cessation in a homeless population: There is a will, but is there a way? J. Gen. Intern. Med. 2002, 17, 369–372. [Google Scholar] [CrossRef] [PubMed]
- Robertson, J.; Conigrave, K.; Ivers, R.; Hindmarsh, E.; Clough, A. Addressing high rates of smoking in remote Aboriginal communities: New evidence for GPs. Aust. Fam. Phys. 2013, 42, 492–496. [Google Scholar]
- Thomas, D.P. Changes in smoking intensity among Aboriginal and Torres Strait Islander people. 1994–2008. Med. J. Aust. 2012, 197, 503–506. [Google Scholar] [CrossRef] [PubMed]
- Binswanger, I.A.; Carson, A.E.; Krueger, P.M.; Mueller, S.R.; Steiner, J.F.; Sabol, W.J. Prison tobacco control policies and deaths from smoking in United States prisons: Population based retrospective analysis. BMJ 2014, 349. [Google Scholar] [CrossRef] [PubMed]
- Sharma, A.; Lewis, S.; Szatkowski, L. Insights into social disparities in smoking prevalence using Mosaic, a novel measure of socioeconomic status: An analysis using a large primary care dataset. BMC Public Health 2010, 10. [Google Scholar] [CrossRef] [PubMed]
- Jha, P.; Peto, R.; Zatonski, W.; Boreham, J.; Jarvis, M.J.; Lopez, A.D. Social inequalities in male mortality, and in male mortality from smoking: Indirect estimation from national death rates in England and Wales, Poland, and North America. Lancet 2006, 368, 367–370. [Google Scholar] [CrossRef]
- Wanless, D. Securing Good Health for the Whole Population. Final Report. Available online: http:/www.hm-treasury.gov.uk/media/D/3/Wanless04_summary.pdf (accessed on 16 January 2014).
- Wu, Q.; Szatkowski, L.; Britton, J.; Parrott, S. Economic cost of smoking in people with mental disorders in the UK. Tob. Control 2014, 7. [Google Scholar] [CrossRef] [PubMed]
- WHO Framework Convention on Tobacco Control. Available online: http://whqlibdoc.who.int/publications/2003/9241591013.pdf?ua=1 (accessed on 8 January 2014).
- World Health Organisation Framework Convention on Tobacco Control: Guidelines for implementation. Available online: http://apps.who.int/iris/bitstream/10665/80510/1/9789241505185_eng.pdf?ua=1 (accessed on 19 January 2014).
- Courtney, R.J.; Bradford, D.; Martire, K.A.; Bonevski, B.; Borland, R.; Doran, C.; Hall, W.; Farrell, M.; Siahpush, M.; Sanson-Fisher, R.; et al. A randomized clinical trial of a financial education intervention with nicotine replacement therapy (NRT) for low socio-economic status Australian smokers: A study protocol. Addiction 2014, 109, 1602–1611. [Google Scholar] [CrossRef] [PubMed]
- Bailey, L.J.; Sanson-Fisher, R.; Aranda, S.; D’Este, C.; Sharkey, K.; Schofield, P. Quality of life research: Types of publication output over time for cancer patients, a systematic review. Eur. J. Cancer Care 2010, 19, 581–588. [Google Scholar] [CrossRef] [PubMed]
- Sanson-Fisher, R.W.; Campbell, E.M.; Htun, A.T.; Bailey, L.J.; Millar, C.J. We are what we do: Research outputs of public health. Am. J. Prev. Med. 2008, 35, 380–385. [Google Scholar] [CrossRef] [PubMed]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339. [Google Scholar] [CrossRef] [PubMed]
- Sanson-Fisher, R.W.; Campbell, E.M.; Perkins, J.J.; Blunden, S.V.; Davis, B.B. Indigenous health research: A critical review of outputs over time. Med. J. Aust. 2006, 184, 502–505. [Google Scholar] [PubMed]
- Cochrane Effective Practice and Organisation of Care Review Group. Data Collection Checklist. Available online: http://epoc.cochrane.org/sites/epoc.cochrane.org/files/uploads/datacollectionchecklist.pdf (accessed on 7 November 2013).
- Pan, W.; Connett, J.E. Selecting the working correlation structure in generalized estimating equations with application to the lung health study. Stat. Sinica 2002, 12, 475–490. [Google Scholar]
- Hawkins, N.G.; Sanson-Fisher, R.W.; Shakeshaft, A.; D’Este, C.; Green, L.W. The multiple baseline design for evaluating population-based research. Am. J. Prev. Med. 2007, 33, 162–168. [Google Scholar] [CrossRef] [PubMed]
- Sanson-Fisher, R.W.; Bonevski, B.; Green, L.W.; D’Este, C.A. Limitations of the randomised controlled trial in evaluating population-based health interventions. Am. J. Prev. Med. 2007, 33, 155–161. [Google Scholar] [CrossRef]
- Stewart, J.M.; Sanson-Fisher, R.W.; Eades, S.J.; Mealing, N.M. Strategies for increasing high-quality intervention research in Aboriginal and Torres Strait Islander health: Views of leading researchers. Med. J. Aust. 2010, 192, 612–615. [Google Scholar] [PubMed]
- Bonevski, B.; Randell, M.; Paul, C.; Chapman, K.; Twyman, L.; Bryant, J.; Brozek, I.; Hughes, C. Reaching the hard-to-reach: A systematic review of strategies for improving health and medical research with socially disadvantaged groups. BMC Med. Res. Methodol. 2014, 14. [Google Scholar] [CrossRef] [PubMed]
- Leeman, J.; Harrell, J.S.; Funk, S.G. Building a research program focused on vulnerable people. West. J. Nurs. Res. 2002, 24, 103–111. [Google Scholar] [CrossRef] [PubMed]
- Sanson-Fisher, R.; Brand, M.; Shakeshaft, A.; Haber, P.; Day, C.; Conigrave, K.; Mattick, R.; Lintzeris, N.; Teesson, M. Forming a national multicentre collaboration to conduct clinical trials: Increasing high-quality research in the drug and alcohol field. Drug Alcohol. Rev. 2010, 29, 469–474. [Google Scholar] [CrossRef] [PubMed]
- Pyatak, E.A.; Blanche, E.I.; Garber, S.L.; Diaz, J.; Blanchard, J.; Florindez, L.; Clark, F.A. Conducting intervention research among underserved populations: Lessons learned and recommendations for researchers. Arch. Phys. Med. Rehabil. 2013, 94, 1190–1198. [Google Scholar] [CrossRef] [PubMed]
- Bryant, J.; Bonevski, B.; Paul, C.; O’Brien, J.; Oakes, W. Delievering smoking cessation support to disadvantaged groups: A qualitative study of the potential of community welfare organisations. Health Educ. Res. 2010, 25, 979–990. [Google Scholar] [CrossRef] [PubMed]
- Cunnigham, J.A.; Kushnir, V. Could the use of biochemical validation of smoking abstinence introduce a confound into the interpretation of randomized controlled trials of tobacco cessation? Addiction 2013, 108, 826–828. [Google Scholar]
- Noonan, D.; Jiang, Y.; Duffy, S.A. Utility of biochemical verification of tobacco cessation in the Department of Veteran Affairs. Addict. Behav. 2013, 38, 1792–1795. [Google Scholar] [CrossRef] [PubMed]
- Shipton, D.; Tappin, D.M.; Vadiveloo, T.; Crossley, J.A.; Aitken, D.A.; Chalmers, J. Reliability of self reported smoking status by pregnant women for estimating smoking prevalence: A retrospective, cross sectional study. BMJ 2009, 339. [Google Scholar] [CrossRef] [PubMed]
- West, R.; Zatonski, W.; Przewozniak, K.; Jarvis, M.J. Can we trust national smoking prevalence figures? Discrepancies between biochemically assessed and self-reported smoking rates in three countries? Cancer Epidemiol. Biomark. 2007, 16, 820–822. [Google Scholar] [CrossRef] [PubMed]
- McCambridge, J.; Witton, J.; Elbourne, D.R. Systematic review of the Hawthorne effect: New concepts are needed to study research participation effects. J. Clin. Epidemiol. 2014, 67, 267–277. [Google Scholar] [CrossRef] [PubMed]
- McCambridge, J.; Kypros, K.; Elbourne, D. In randomization we trust? There are overlooked problems in experimenting with people in behavioral intervention trials. J. Clin. Epidemiol. 2014, 67, 247–253. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions. Available online: http://handbook.cochrane.org/ (accessed on 3 February 2014).
- Bryant, J.; Bonevski, B.; Paul, C.; McElduff, P.; Attia, J. A systematic review and meta-analysis of the effectiveness of behavioural smoking cessation interventions in selected disadvantaged groups. Addiction 2011, 106, 1568–1585. [Google Scholar] [CrossRef] [PubMed]
- Paul, C.; Sanson-Fisher, R.; Stewart, J.; Anderson, A.E. Being sorry is not enough: The sorry state of the evidence base for improving the health indigenous populations. Am. J. Prev. Med. 2010, 38, 566–568. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Courtney, R.J.; Naicker, S.; Shakeshaft, A.; Clare, P.; Martire, K.A.; Mattick, R.P. Smoking Cessation among Low-Socioeconomic Status and Disadvantaged Population Groups: A Systematic Review of Research Output. Int. J. Environ. Res. Public Health 2015, 12, 6403-6422. https://doi.org/10.3390/ijerph120606403
Courtney RJ, Naicker S, Shakeshaft A, Clare P, Martire KA, Mattick RP. Smoking Cessation among Low-Socioeconomic Status and Disadvantaged Population Groups: A Systematic Review of Research Output. International Journal of Environmental Research and Public Health. 2015; 12(6):6403-6422. https://doi.org/10.3390/ijerph120606403
Chicago/Turabian StyleCourtney, Ryan J., Sundresan Naicker, Anthony Shakeshaft, Philip Clare, Kristy A. Martire, and Richard P. Mattick. 2015. "Smoking Cessation among Low-Socioeconomic Status and Disadvantaged Population Groups: A Systematic Review of Research Output" International Journal of Environmental Research and Public Health 12, no. 6: 6403-6422. https://doi.org/10.3390/ijerph120606403