
Association of Serum Free Fatty Acids with Hypertension and Insulin Resistance among Rural Uyghur Adults in Far Western China

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics Statement
2.2. Settings and Participants
2.3. Definition of MS and HOMA-IR
2.4. Exclusion Criteria
2.5. Laboratory Tests
2.6. Statistical Analysis
3. Results
3.1. Balancing Tests for SBP, DBP and HOMA-IR among the Four Groups

{kind=link}
| Index | With IR (n = 87) | With Hypertension (n = 68) | With Hypertension and IR (n = 82) | Normal (n = 74) | p |
|---|---|---|---|---|---|
| SBP | - | 145.35 ± 13.24 | 146.90 ± 18.21 | - | 0.813 |
| 111.06 ± 10.24 | - | - | 114.26 ± 9.82 | 0.069 | |
| DBP | - | 92.37 ± 11.12 | 94.78 ± 12.51 | - | 0.996 |
| 71.15 ± 8.87 | - | - | 72.91 ± 7.42 | 0.223 | |
| HOMA-IR | - | 0.68 ± 0.28 | - | 0.69 ± 0.34 | 0.935 |
| 4.02 ± 2.36 | - | 4.22 ± 2.34 | - | 0.786 |
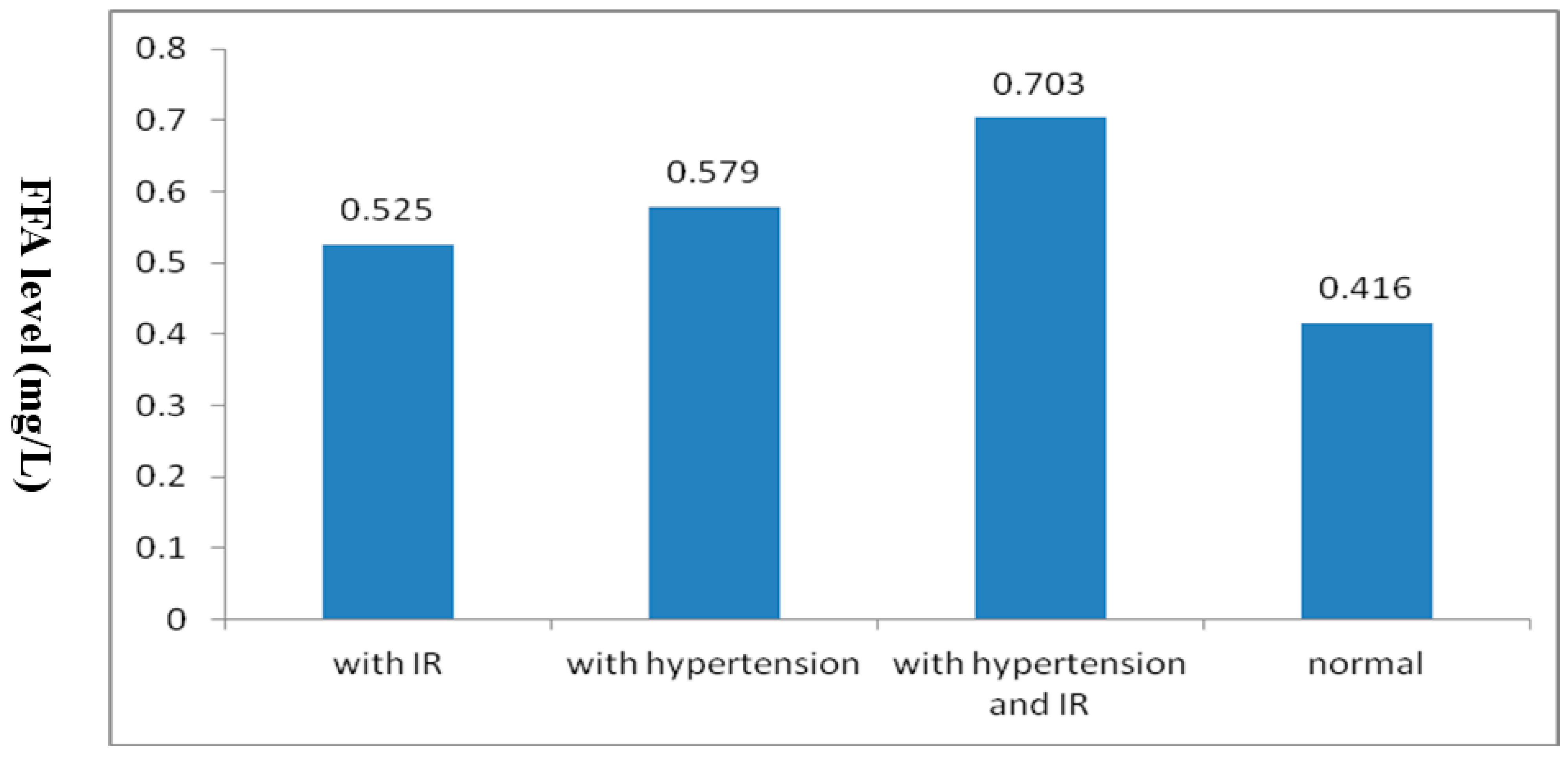
3.2. One-Factor Analysis of Variance
| Index | With IR | With Hypertension | With Hypertension and IR | Normal | χ2/F | p |
|---|---|---|---|---|---|---|
| (n = 87) | (n = 68) | (n = 82) | (n = 74) | |||
| Gender (male/female) | 46/41 | 38/30 | 48/34 | 36/38 | 1.651 | 0.648 |
| Age (year) | 39.30 ± 11.67 | 44.05 ± 10.91 | 45.43 ± 11.53 | 40.13 ± 11.67 | 4.883 | 0.003 |
| BMI (kg/m2) | 22.93 ± 3.50 | 24.58 ± 3.84 | 25.83 ± 3.79 | 22.06 ± 2.63 | 16.070 | <0.001 |
| TG (mmol/L) | 1.41 ± 0.98 | 1.35 ± 0.86 | 1.70 ± 0.97 | 1.02 ± 0.57 | 6.402 | <0.001 |
| TC (mmol/L) | 4.54 ± 1.04 | 4.75 ± 1.33 | 4.74 ± 0.96 | 4.22 ± 1.09 | 2.994 | 0.031 |
| HDL-C (mmol/L) | 1.19 ± 0.29 | 1.16 ± 0.30 | 1.08 ± 0.29 | 1.29 ± 0.26 | 5.796 | 0.001 |
| LDL-C (mmol/L) | 2.48 ± 0.84 | 2.67 ± 0.67 | 2.70 ± 0.62 | 2.32 ± 0.54 | 3.922 | 0.009 |
| FFA (mg/L) | 0.52 ± 0.15 | 0.58 ± 0.25 | 0.73 ± 0.22 | 0.39 ± 0.11 | 23.614 | <0.001 |
3.3. Analysis of Covariance

| Groups | p | 95% CI |
|---|---|---|
| With hypertension and IR/with IR | <0.001 | (0.114, 0.243) |
| With hypertension and IR/with hypertension | 0.002 | (0.048, 0.201) |
| With hypertension and IR/normal | <0.001 | (0.013, 0.162) |
| With IR/normal | 0.007 | (0.039, 0.277) |
| With hypertension/normal | <0.001 | (0.102, 0.247) |
| With IR/with hypertension | 0.170 | (−0.131, 0.023) |
3.4. Interaction of Hypertension and IR with Serum FFA Levels
| Source | Type β Sum of Squares | df | Mean Square | F | Sig. |
|---|---|---|---|---|---|
| Corrected Model | 1.074 a | 5 | 0.215 | 3.348 | 0.006 |
| Intercept | 0.736 | 1 | 0.736 | 11.462 | 0.001 |
| SBP | 0.022 | 1 | 0.022 | 3.745 | 0.048 |
| DBP | 0.377 | 1 | 0.377 | 5.876 | 0.016 |
| IR | 0.256 | 1 | 0.256 | 3.986 | 0.046 |
| IR * SBP | 0.012 | 1 | 0.012 | 1.220 | 0.270 |
| IR * DBP | 0.143 | 1 | 0.143 | 1.189 | 0.277 |
| Error | 28.751 | 448 | 0.064 | ||
| Total | 168.672 | 454 | |||
| Corrected Total | 29.826 | 453 |
3.5. Multivariate Logistic Regression Analysis
| Variable | Index | β | SE | Waldχ2 | p | OR | 95%CI for OR | |
|---|---|---|---|---|---|---|---|---|
| Hypertension | FFA (mmol/L) | <0.40 | - | - | - | - | - | - |
| 0.40~ | -0.41 | 0.61 | 0.446 | 0.504 | 0.66 | (0.20, 2.21) | ||
| 0.62~ | 0.96 | 0.59 | 2.599 | 0.107 | 2.60 | (0.81, 8.30) | ||
| 0.79~ | 1.878 | 0.65 | 8.273 | 0.004 | 6.54 | (1.82, 23.52) | ||
| HOMA-IR | FFA (mmol/L) | <0.40 | - | - | - | - | - | - |
| 0.40~ | 1.54 | 0.62 | 6.111 | 0.013 | 4.67 | (1.38, 15.84) | ||
| 0.62~ | 1.55 | 0.59 | 6.801 | 0009 | 4.72 | (1.47, 15.16) | ||
| 0.79~ | 1.69 | 0.58 | 8.250 | 0.004 | 5.40 | (1.71, 17.06) |
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Bastard, J.P.; Maachi, M.; Lagathu, C.; Kim, M.J.; Caron, M.; Vidal, H.; Capeau, J.; Feve, B. Recent advances in the relationship between obesity, inflammation and insulin resistance. Eur. Cytokine Netw. 2006, 17, 4–12. [Google Scholar] [PubMed]
- Mcgarry, J.D. Banting lecture 2001: Dysregulation of fatty acid metabolism in the etiology of type 2 diabetes. Diabetes 2002, 51, 7–18. [Google Scholar] [CrossRef] [PubMed]
- He, J.; Guo, S.; Liu, J.; Zhang, M.; Ding, Y.; Zhang, J.; Li, S.; Xu, S.; Niu, Q.; Guo, H.; et al. Ethnic Differences in Prevalence of General Obesity and Abdominal Obesity among Low-Income Rural Kazakh and Uyghur Adults in Far Western China and Implications in Preventive Public Health. PLoS ONE 2014, 9, e106723. [Google Scholar] [CrossRef] [PubMed]
- Guo, S.X.; Yang, Z.M.; Zhang, J.Y.; Guo, H.; Zhang, Y.H.; Xu, S.Z.; Niu, Q. Relationship of Free Fatty Acid and Insulin Resistance to Hypertension in Kazakh and Han Race of Xinjiang. Chin. J. Hypertens. 2010, 18, 459–464. [Google Scholar]
- China council for the prevention and control of hypertension guidelines revision. Guidelines for prevention and treatment of hypertension 2010. Chin. J. Hypertens. 2011, 19, 709–710. [Google Scholar]
- Alberti, K.G.; Zimmet, P.; Shaw, J.; IDF Epidemiology Task Force Consensus Group. The Metabolic Syndrome A New Worldwide Definition. Lancet 2005, 366, 1059–1062. [Google Scholar] [CrossRef]
- Li, G.W. The evaluation of insulin sensitivity and its application in clinical research. Chin. J. Endocrinol. Metab. 2000, 16, 198–200. [Google Scholar]
- Li, C.H.; Guo, S.X.; Ma, R.L.; Ding, Y.S.; Guo, H.; Liu, J.M.; Xu, S.Z.; Zhang, J.Y.; Li, S.G.; Zhang, M. The epidemic situation of metabolic syndrome among the Uyghur in Kazakhs of Xinjiang in 2010. Chin. J. Prev. Med. 2010, 46, 419–423. [Google Scholar]
- Guo, H.; Guo, S.X.; Zhang, J.Y.; Ma, R.L.; Rui, D.S.; Xu, S.Z.; Sun, F.; Hu, A.R.; Yang, Z.M. Study on the prevalence of metabolic syndrome among the Kazakh population in Xinjiang. Chin. J. Epidemiol. 2010, 31, 747–750. [Google Scholar]
- Gu, D.; Reynolds, K.; Wu, X.; Chen, J.; Duan, X.; Reynolds, R.F.; Whelton, P.K.; He, J.; InterASIA Collaborative Group. The prevalence of meta bolic syndrome in the general adult population aged 35–74 years in China. Chin. J. Diabetes 2005, 13, 181–186. [Google Scholar]
- Ma, X.J.; Zhang, M.; Guo, S.X.; Ma, R.L.; Ding, Y.S. Prevalence of hypertension in Uyghur, Kazakhs and Han people in rural areas of Xinjiang. Chin. J. Hypertens. 2013, 21, 1164–1168. [Google Scholar]
- Boden, G. Obesity, Insulin Resistance and Free Fatty Acids. Curr. Opin. Endocrinol. Diabetes Obes. 2011, 18, 139–143. [Google Scholar] [CrossRef] [PubMed]
- Tabara, Y.; Takahashi, Y.; Kawaguchi, T.; Setoh, K.; Terao, C.; Yamada, R.; Kosuqi, S.; Sekine, A.; Nakayama, T.; Matsuda, F.; et al. Association of serum-free fatty acid level with reduced reflection pressure wave magnitude and central blood pressure: The Nagahama study. Hypertension 2014, 64, 1212–1218. [Google Scholar] [CrossRef] [PubMed]
- Boden, G.; Homko, C.; Mozzoli, M.; Showe, L.C.; Nichols, C.; Cheung, P. Thiazolidine diones up regulate fatty acid uptake and oxidation in adipose tissue of diabetic patients. Diabetes 2005, 54, 880–885. [Google Scholar] [CrossRef] [PubMed]
- De Jongh, R.T.; Serné, E.H.; Ijzerman, R.G.; de Vries, G.; Stehouwer, C.D. Free fatty acid levels modulate microvascular function: Relevance for obesity-associated insulin resistance, hypertension, and microangiopathy. Diabetes 2004, 53, 2873–2882. [Google Scholar] [CrossRef] [PubMed]
- Meshkani, R.; Adeli, K. Hepatic insulin resistance, metabolic syndrome and cardiovascular disease. Clin. Biochem. 2009, 42, 1331–1346. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guo, S.-X.; Yan, Y.-Z.; Mu, L.-T.; Niu, Q.; He, J.; Liu, J.-M.; Li, S.-G.; Zhang, J.-Y.; Guo, H.; Rui, D.-S. Association of Serum Free Fatty Acids with Hypertension and Insulin Resistance among Rural Uyghur Adults in Far Western China. Int. J. Environ. Res. Public Health 2015, 12, 6582-6590. https://doi.org/10.3390/ijerph120606582
Guo S-X, Yan Y-Z, Mu L-T, Niu Q, He J, Liu J-M, Li S-G, Zhang J-Y, Guo H, Rui D-S. Association of Serum Free Fatty Acids with Hypertension and Insulin Resistance among Rural Uyghur Adults in Far Western China. International Journal of Environmental Research and Public Health. 2015; 12(6):6582-6590. https://doi.org/10.3390/ijerph120606582
Chicago/Turabian StyleGuo, Shu-Xia, Yi-Zhong Yan, La-Ti Mu, Qiang Niu, Jia He, Jia-Ming Liu, Shu-Gang Li, Jing-Yu Zhang, Heng Guo, and Dong-Sheng Rui. 2015. "Association of Serum Free Fatty Acids with Hypertension and Insulin Resistance among Rural Uyghur Adults in Far Western China" International Journal of Environmental Research and Public Health 12, no. 6: 6582-6590. https://doi.org/10.3390/ijerph120606582