
The Risk of Reported Cryptosporidiosis in Children Aged <5 Years in Australia is Highest in Very Remote Regions

Abstract
:1. Introduction
2. Methods
2.1. Data Sources
2.2. Analysis
3. Results
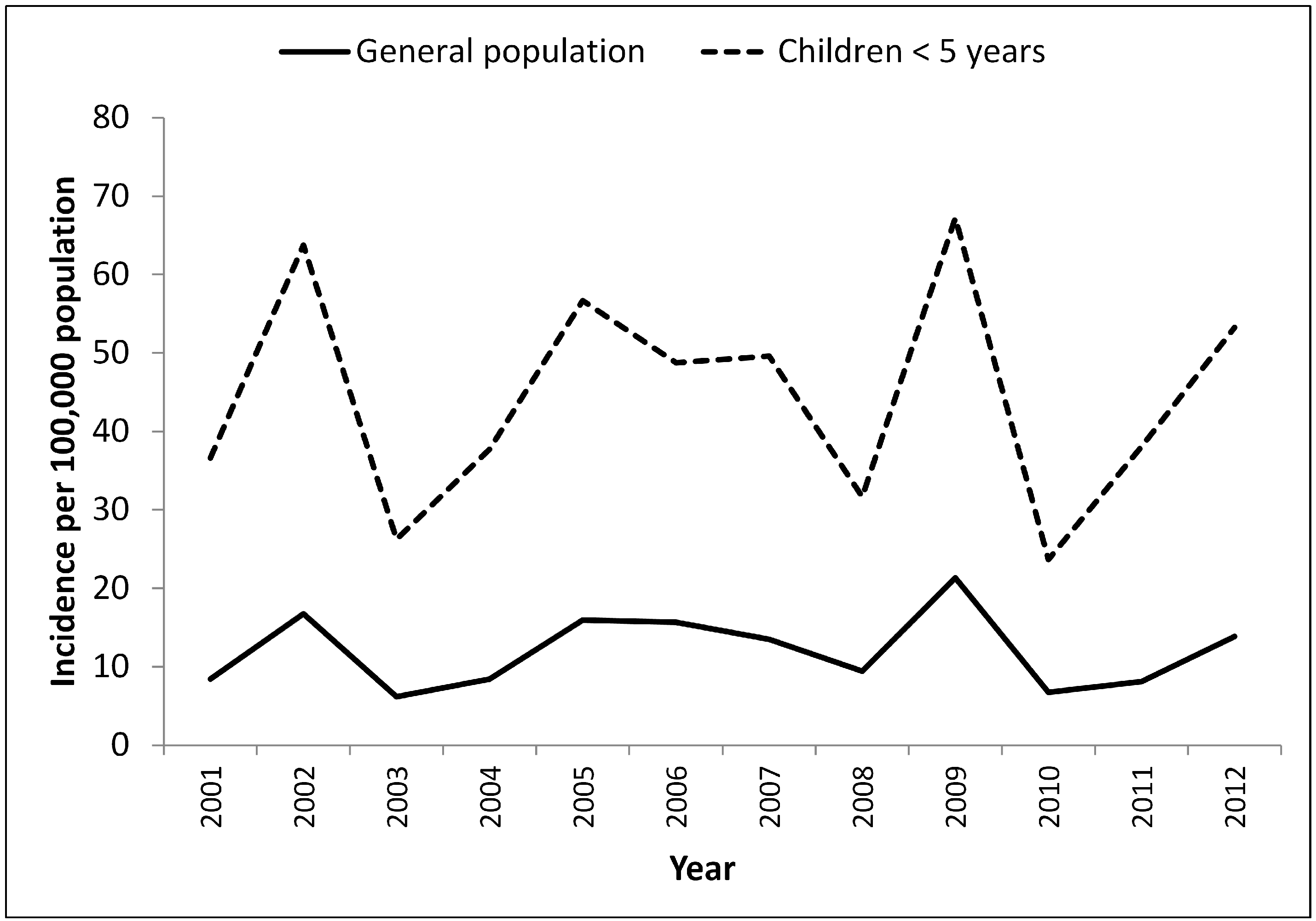
3.1. Time Trends and Seasonality in Cryptosporidiosis Reported in Children <5 Years
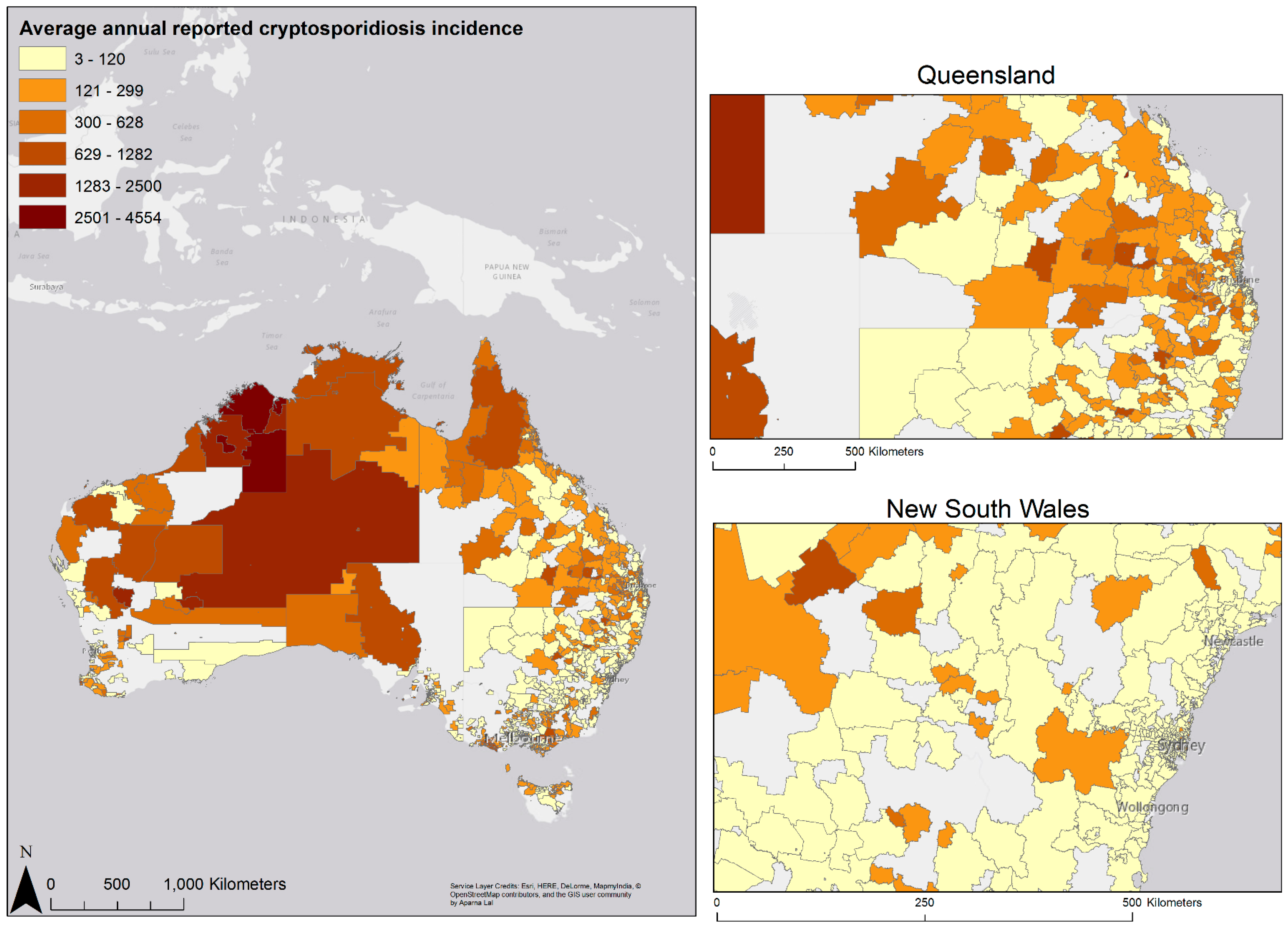
3.2. Geographic Variation in Disease Risk




{kind=link}
{kind=link}
{kind=link}
| Number of Reported Illnesses | Average Annual Incidence Risk per 100,000 Population | Incidence Risk Ratio | 95% CI+ | p-Value | |
|---|---|---|---|---|---|
| Regions | |||||
| Major cities | 2466 | 12.2 | 1.0 | ||
| Inner regional | 5355 | 16.0 | 1.4 | 1.2–1.7 | <0.001 |
| Outer regional | 2536 | 29.6 | 2.4 | 2.0–2.9 | <0.001 |
| Remote areas | 1029 | 62.6 | 5.2 | 4.3–6.2 | <0.001 |
| Very remote | 1563 | 89.1 | 8.2 | 6.9–9.8 | <0.001 |
| Gender | |||||
| Male | 7243 | 19.1 | 1.0 | ||
| Female | 5706 | 17.1 | 0.9 | 0.8–1.0 | >0.1 |
| Season | |||||
| Summer | 4727 | 22.0 | 1.0 | ||
| Autumn | 5077 | 21.1 | 0.7 | 0.6–0.8 | <0.001 |
| Winter | 1511 | 11.1 | 0.3 | 0.3–0.4 | <0.001 |
| Spring | 1634 | 13.4 | 0.4 | 0.3–0.5 | <0.001 |
4. Discussion
5. Conclusions
Supplementary Files
Supplementary File 1Acknowledgments
Author Contributions
Conflicts of Interest
References
- Fayer, R.; Morgan, U.; Upton, S.J. Epidemiology of Cryptosporidium: Transmission, detection and identification. Int. J. Parasitol. 2000, 30, 1305–1322. [Google Scholar] [CrossRef]
- Slifko, T.R.; Smith, H.V.; Rose, J.B. Emerging parasite zoonoses associated with water and food. Int. J. Parasitol. 2000, 30, 1379–1393. [Google Scholar] [CrossRef]
- Smith, H.V.; Cacciò, S.M.; Cook, N.; Nichols, R.A.B.; Tait, A. Cryptosporidium and Giardia as foodborne zoonoses. Vet. Parasitol. 2007, 149, 29–40. [Google Scholar] [CrossRef] [PubMed]
- Uehlinger, F.D.; Greenwood, S.J.; McClure, J.; Conboy, G.; O’Handley, R.; Barkema, H.W. Zoonotic potential of Giardia duodenalis and Cryptosporidium spp. and prevalence of intestinal parasites in young dogs from different populations on Prince Edward Island, Canada. Vet. Parasitol. 2013, 196, 509–514. [Google Scholar] [CrossRef] [PubMed]
- Chalmers, R.M.; Smith, R.; Elwin, K.; Clifton-Hadley, F.A.; Giles, M. Epidemiology of anthroponotic and zoonotic human cryptosporidiosis in England and Wales, 2004–2006. Epidemiol. Infect. 2011, 139, 700–712. [Google Scholar] [CrossRef] [PubMed]
- Robertson, L.J. Transmission routes and factors that lend themselves to foodborne transmission. In Cryptosporidium as a Foodborne Pathogen; Springer: New York, NY, USA, 2014; pp. 11–12. [Google Scholar]
- Heyman, D. Control of Communicable Diseases Manual; American Public Health Association Press: Washington, DC, USA, 2004. [Google Scholar]
- Meinhardt, P.L.; Casemore, D.P.; Miller, K.B. Epidemiologic aspects of human cryptosporidiosis and the role of waterborne transmission. Epidemiol. Rev. 1996, 18, 118–136. [Google Scholar] [CrossRef] [PubMed]
- Kotloff, K.L.; Nataro, J.P.; Blackwelder, W.C.; Nasrin, D.; Farag, T.H.; Panchalingam, S.; Wu, Y.; Sow, S.O.; Sur, D.; Breiman, R.F.; et al. Burden and aetiology of diarrhoeal disease in infants and young children in developing countries (the Global Enteric Multicenter Study, GEMS): A prospective, case-control study. Lancet 2013, 382, 209–222. [Google Scholar] [CrossRef]
- Koehler, K.M.; Lasky, T.; Fein, S.B.; Delong, S.M.; Hawkins, M.A.; Rabatsky-Ehr, T.; Ray, S.M.; Shiferaw, B.; Swanson, E.; Vugia, D.J. Population-based incidence of infection with selected bacterial enteric pathogens in children younger than five years of age, 1996–1998. Pediatr. Infect. Dis. J. 2006, 25, 129–134. [Google Scholar] [CrossRef] [PubMed]
- Snel, S.J.; Baker, M.G.; Kamalesh, V.; French, N.; Learmonth, J. A tale of two parasites: The comparative epidemiology of cryptosporidiosis and giardiasis. Epidemiol. Infect. 2009, 137, 1641–1650. [Google Scholar] [CrossRef] [PubMed]
- Barry, M.A.; Weatherhead, J.E.; Hotez, P.J.; Woc-Colburn, L. Childhood parasitic infections endemic to the United States. Pediatr. Clin. N. Am. 2013, 60, 471–485. [Google Scholar] [CrossRef]
- Checkley, W.; White, A.C., Jr.; Jaganath, D.; Arrowood, M.J.; Chalmers, R.M.; Chen, X.-M.; Fayer, R.; Griffiths, J.K.; Guerrant, R.L.; Hedstrom, L.; et al. A review of the global burden, novel diagnostics, therapeutics, and vaccine targets for cryptosporidium. Lancet Infect. Dis. 2015, 15, 85–94. [Google Scholar] [CrossRef]
- Iannotti, L.L.; Trehan, I.; Clitheroe, K.L.; Manary, M.J. Diagnosis and treatment of severely malnourished children with diarrhoea. J. Paediatr. Child Health 2015, 51, 387–395. [Google Scholar] [CrossRef] [PubMed]
- Guerrant, D.I.; Moore, S.R.; Lima, A.A.; Patrick, P.D.; Schorling, J.B.; Guerrant, R.L. Association of early childhood diarrhea and cryptosporidiosis with impaired physical fitness and cognitive function four-seven years later in a poor urban community in northeast Brazil. Am. J. Trop. Med. Hyg. 1999, 61, 707–713. [Google Scholar] [PubMed]
- Ravel, A.; Nesbitt, A.; Pintar, K.; Macarthur, A.; Wang, H.-L.; Marshall, B.; Pollari, F. Epidemiological and clinical description of the top three reportable parasitic diseases in a Canadian community. Epidemiol. Infect. 2013, 141, 431–442. [Google Scholar] [CrossRef] [PubMed]
- Yoder, J.S.; Wallace, R.M.; Collier, S.A.; Beach, M.J.; Hlavsa, M.C. Cryptosporidiosis surveillance—United States, 2009–2010. MMWR Surveill. Summ. 2012, 61, 1–12. [Google Scholar] [PubMed]
- Cruickshank, R.; Ashdown, L.; Croese, J. Human cryptosporidiosis in North Queensland. Austr. N. Z. J. Med. 1988, 18, 582–586. [Google Scholar] [CrossRef]
- Hu, W.; Mengersen, K.; Tong, S. Spatial analysis of notified cryptosporidiosis infections in Brisbane, Australia. Ann. Epidemiol. 2009, 19, 900–907. [Google Scholar] [CrossRef] [PubMed]
- Ng-Hublin, J.S.; Hargrave, D.; Combs, B.; Ryan, U. Investigation of a swimming pool-associated cryptosporidiosis outbreak in the Kimberley region of Western Australia. Epidemiol. Infect. 2015, 143, 1037–1041. [Google Scholar] [CrossRef] [PubMed]
- Mayne, D.J.; Ressler, K.-A.; Smith, D.; Hockey, G.; Botham, S.J.; Ferson, M.J. A community outbreak of cryptosporidiosis in Sydney associated with a public swimming facility: A case-control study. Interdiscip. Perspect. Infect. Dis. 2011. [Google Scholar] [CrossRef] [PubMed]
- Harper, C.M.; Cowell, N.A.; Adams, B.C.; Langley, A.J.; Wohlsen, T.D. Outbreak of Cryptosporidium linked to drinking unpasteurised milk. Commun. Dis. Intell. Q. Rep. 2002, 26, 449–450. [Google Scholar] [PubMed]
- Communicable Diseases Network Australia (CDNA). Available online: http://www.health.gov.au/cdna (accessed on 27 August 2015).
- Cryptosporidiosis Laboratory Case Definition. Available online: http://www.health.gov.au/internet/main/publishing.nsf/Content/cda-phlncd-cryptosporidiosis.htm (accessed on 27 August 2015).
- Australian Bureau of Statistics. Population Estimates by Age and Sex, Australia, 2011; Australian Bureau of Statistics: Canberra, Australia, 2011.
- Australian Bureau of Statistics. Australian Statistical Geography Standard (ASGS): Volume 5-Remoteness Structure; Australian Bureau of Statistics: Canberra, Australia, 2011; p. 7.
- De Graaf, D.C.; Vanopdenbosch, E.; Ortega-Mora, L.M.; Abbassi, H.; Peeters, J.E. A review of the importance of cryptosporidiosis in farm animals. Int. J. Parasitol. 1999, 29, 1269–1287. [Google Scholar]
- Zintl, A.; Proctor, A.F.; Read, C.; Dewaal, T.; Shanaghy, N.; Fanning, S.; Mulcahy, G. The prevalence of Cryptosporidium species and subtypes in human faecal samples in Ireland. Epidemiol. Infect. 2009, 137, 270–277. [Google Scholar] [CrossRef] [PubMed]
- Hoek, M.; Oliver, I.; Barlow, M.; Heard, L.; Paynter, S.; Chalmers, R. Outbreak of Cryptosporidium parvum among children after a school excursion to an adventure farm, south west England. J. Water Health 2008, 6, 333–338. [Google Scholar] [CrossRef] [PubMed]
- Robinson, T.J.; Scheftel, J.M.; Smith, K.E. Raw milk consumption among patients with non-outbreak-related enteric infections, Minnesota, USA, 2001–2010. Emerg. Infect. Dis. 2014, 20, 38–44. [Google Scholar] [PubMed]
- Jellison, K.L.; Lynch, A.E.; Ziemann, J.M. Source tracking identifies deer and geese as vectors of human-infectious Cryptosporidium genotypes in an urban/suburban watershed. Environ. Sci. Technol. 2009, 43, 4267–4272. [Google Scholar] [CrossRef] [PubMed]
- Power, M.L.; Slade, M.B.; Sangster, N.C.; Veal, D.A. Genetic characterisation of Cryptosporidium from a wild population of eastern grey kangaroos Macropus giganteus inhabiting a water catchment. Infect. Genet. Evol. 2004, 4, 59–67. [Google Scholar] [CrossRef] [PubMed]
- Ryan, U.; Power, M. Cryptosporidium species in Australian wildlife and domestic animals. Parasitology 2012, 139, 1673–1688. [Google Scholar] [CrossRef] [PubMed]
- Waldron, L.S.; Cheung-Kwok-Sang, C.; Power, M.L. Wildlife-associated Cryptosporidium fayeri in human, Australia. Emerg. Infect. Dis. 2010, 16, 2006–2007. [Google Scholar] [CrossRef] [PubMed]
- Smith, R.; Chalmers, R.; Elwin, K.; Clifton-Hadley, F.; Mueller-Doblies, D.; Watkins, J.; Paiba, G.; Giles, M. Investigation of the role of companion animals in the zoonotic transmission of cryptosporidiosis. Zoonoses Public Health 2009, 56, 24–33. [Google Scholar] [CrossRef] [PubMed]
- Lucio-Forster, A.; Griffiths, J.K.; Cama, V.A.; Xiao, L.; Bowman, D.D. Minimal zoonotic risk of cryptosporidiosis from pet dogs and cats. Trends Parasitol. 2010, 26, 174–179. [Google Scholar] [CrossRef] [PubMed]
- Learmonth, J.; Ionas, G.; Pita, A.; Cowie, R. Seasonal shift in Cryptosporidium parvum transmission cycles in New Zealand. J. Eukaryot. Microbiol. 2001, 48, 34s–35s. [Google Scholar] [CrossRef]
- Learmonth, J.J.; Ionas, G.; Ebbett, K.A.; Kwan, E.S. Genetic characterization and transmission cycles of Cryptosporidium species isolated from humans in New Zealand. Appl. Environ. Microbiol. 2004, 70, 3973–3978. [Google Scholar] [CrossRef] [PubMed]
- Abal-fabeiro, J.L.; Maside, X.; Llovo, J.; Bartolomé, C. Aetiology and epidemiology of human cryptosporidiosis cases in Galicia (NW Spain), 2000–2008. Epidemiol. Infect. 2015. [Google Scholar] [CrossRef] [PubMed]
- Kukuruzovic, R.; Robins-Browne, R.M.; Anstey, N.M.; Brewster, D.R. Enteric pathogens, intestinal permeability and nitric oxide production in acute gastroenteritis. Pediatr. Infect. Dis. J. 2002, 21, 730–739. [Google Scholar] [CrossRef] [PubMed]
- Schurer, J.M.; Ndao, M.; Quewezance, H.; Elmore, S.A.; Jenkins, E.J. People, pets, and parasites: One health surveillance in southeastern Saskatchewan. Am. J. Trop. Med. Hyg. 2014, 90, 1184–1190. [Google Scholar] [CrossRef] [PubMed]
- Kearns, T.; Clucas, D.; Connors, C.; Currie, B.J.; Carapetis, J.R.; Andrews, R.M. Clinic attendances during the first 12 months of life for Aboriginal children in five remote communities of northern Australia. PLoS ONE 2013, 8. [Google Scholar] [CrossRef] [PubMed]
- Baldursson, S.; Karanis, P. Waterborne transmission of protozoan parasites: Review of worldwide outbreaks—An update 2004–2010. Water Res. 2011, 45, 6603–6614. [Google Scholar] [CrossRef] [PubMed]
- Bailie, R.S.; Carson, B.E.; McDonald, E.L. Water supply and sanitation in remote Indigenous communities—Priorities for health development. Aust. N. Z. J. Public Health 2004, 28, 409–414. [Google Scholar] [CrossRef] [PubMed]
- Uejio, C.K.; Yale, S.H.; Malecki, K.; Borchardt, M.A.; Anderson, H.A.; Patz, J.A. Drinking water systems, hydrology, and childhood gastrointestinal illness in Central and Northern Wisconsin. Am. J. Public Health 2014, 104, 639–646. [Google Scholar] [CrossRef] [PubMed]
- Polgreen, P.; Sparks, J.; Polgreen, L.; Yang, M.; Harris, M.; Pentella, M.; Cavanaugh, J. A statewide outbreak of Cryptosporidium and its association with the distribution of public swimming pools. Epidemiol. Infect. 2012, 140, 1439–1445. [Google Scholar] [CrossRef] [PubMed]
- Karanis, P.; Kourenti, C.; Smith, H. Waterborne transmission of protozoan parasites: A worldwide review of outbreaks and lessons learnt. J. Water Health 2007, 5, 1–38. [Google Scholar] [PubMed]
- Naumova, E.; Jagai, J.; Matyas, B.; DeMaria, A.; MacNeill, I.; Griffiths, J. Seasonality in six enterically transmitted diseases and ambient temperature. Epidemiol. Infect. 2007, 135, 281–292. [Google Scholar] [CrossRef] [PubMed]
- Hall, G.V.; Kirk, M.D.; Ashbolt, R.; Stafford, R.; Lalor, K. Frequency of infectious gastrointestinal illness in Australia, 2002: Regional, seasonal and demographic variation. Epidemiol. Infect. 2006, 134, 111–118. [Google Scholar] [CrossRef] [PubMed]
- Cordell, R.L.; Addiss, D.G. Cryptosporidiosis in child care settings: A review of the literature and recommendations for prevention and control. Pediatr. Infect. Dis. J. 1994, 13, 310–317. [Google Scholar] [PubMed]
- Clavel, A.; Olivares, J.L.; Fleta, J.; Castillo, J.; Varea, M.; Ramos, F.J.; Arnal, A.C.; Quílez, J. Seasonally of cryptosporidiosis in children. Eur. J. Clin. Microbiol. Infect. Dis. 1996, 15, 77–79. [Google Scholar] [CrossRef] [PubMed]
- Koch, K.L.; Phillips, D.J.; Aber, R.C.; Current, W.L. Cryptosporidiosis in hospital personnel: Evidence for person-to-person transmission. Ann. Intern. Med. 1985, 102, 593–596. [Google Scholar] [CrossRef] [PubMed]
- Pardhan-Ali, A.; Wilson, J.; Edge, V.L.; Furgal, C.; Reid-Smith, R.; Santos, M.; McEwen, S.A. Community-level risk factors for notifiable gastrointestinal illness in the Northwest Territories, Canada, 1991–2008. BMC Public Health 2013, 13. [Google Scholar] [CrossRef] [PubMed]
- Shield, J.; Aland, K.; Kearns, T.; Gongdjalk, G.; Holt, D.; Currie, B.; Prociv, P. Intestinal parasites of children and adults in a remote Aboriginal community of the Northern Territory, Australia, 1994–1996. Western Pac. Surveill. Response J. 2015, 6, 44–51. [Google Scholar] [CrossRef] [PubMed]
- Mattioli, M.C.M.; Davis, J.; Boehm, A.B. Hand-to-mouth contacts result in greater ingestion of feces than dietary water consumption in Tanzania: A quantitative fecal exposure assessment model. Environ. Sci. Technol. 2015, 49, 1912–1920. [Google Scholar] [CrossRef] [PubMed]
- McDonald, E.; Slavin, N.; Bailie, R.; Schobben, X. No germs on me: A social marketing campaign to promote hand-washing with soap in remote Australian Aboriginal communities. Glob. Health Promot. 2011, 18, 62–65. [Google Scholar] [CrossRef] [PubMed]
- McDonald, E.; Bailie, R.; Grace, J.; Brewster, D. A case study of physical and social barriers to hygiene and child growth in remote Australian Aboriginal communities. BMC Public Health 2009, 9. [Google Scholar] [CrossRef] [PubMed]
- Soetens, L.C.; Boshuizen, H.C.; Korthals Altes, H. Contribution of seasonality in transmission of Mycobacterium tuberculosis to seasonality in tuberculosis disease: A simulation study. Am. J. Epidemiol. 2013, 178. [Google Scholar] [CrossRef] [PubMed]
- Jagai, J.S.; Castronovo, D.A.; Monchak, J.; Naumova, E.N. Seasonality of cryptosporidiosis: A meta-analysis approach. Environ. Res. 2009, 109, 465–478. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lal, A.; Fearnley, E.; Kirk, M. The Risk of Reported Cryptosporidiosis in Children Aged <5 Years in Australia is Highest in Very Remote Regions. Int. J. Environ. Res. Public Health 2015, 12, 11815-11828. https://doi.org/10.3390/ijerph120911815
Lal A, Fearnley E, Kirk M. The Risk of Reported Cryptosporidiosis in Children Aged <5 Years in Australia is Highest in Very Remote Regions. International Journal of Environmental Research and Public Health. 2015; 12(9):11815-11828. https://doi.org/10.3390/ijerph120911815
Chicago/Turabian StyleLal, Aparna, Emily Fearnley, and Martyn Kirk. 2015. "The Risk of Reported Cryptosporidiosis in Children Aged <5 Years in Australia is Highest in Very Remote Regions" International Journal of Environmental Research and Public Health 12, no. 9: 11815-11828. https://doi.org/10.3390/ijerph120911815