These data represent cumulative incidence of childhood cancer in the state of Delaware between 2004 and 2014, implying a decade experience with the leading cause of disease- related death among children 0 to 14 years. A total of 481 childhood cancers were diagnosed during this period. The population of children ages 0 to 17 in Delaware was 205,765 children. The cumulative incidence (CI) of childhood cancer was 234 per 100,000 children, while the annual cumulative incidence was 23 per 100,000 children.
3.1. Cancer Description by Geographic Locale
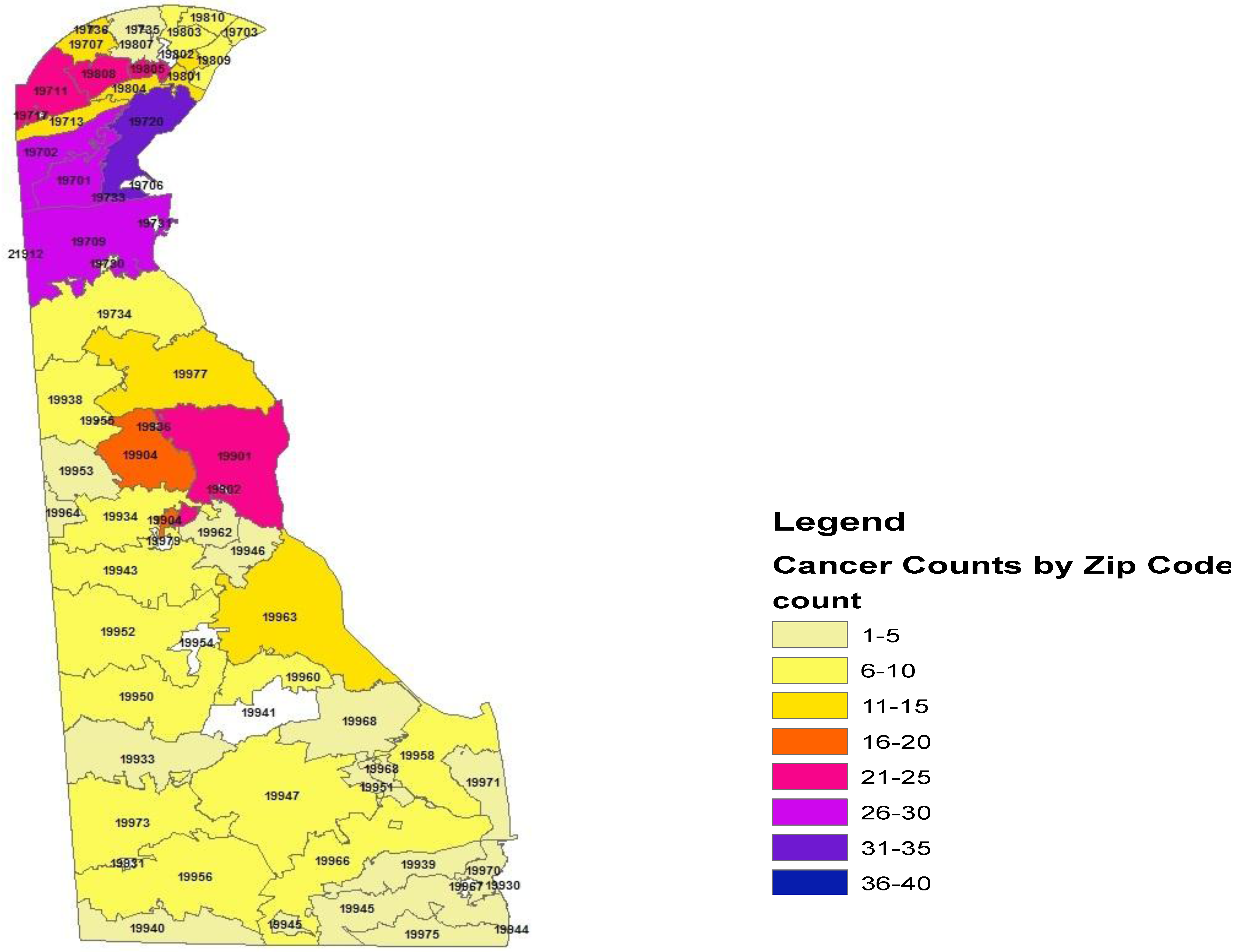
Within the state of Delaware, the proportionate cancer morbidity (tumor counts per zip code) indicated the distribution by zip codes: 19701 (
n = 26, 5.4%), 19702 (
n = 30, 6.2%), 19709 (
n = 28, 5.8%), 19720 (
n = 35, 7.2%), 19805 (
n = 23, 4.7%), 19808 (
n = 25, 5.1%), 19901 (
n = 21, 4.3%), and 19904 (
n = 20, 4.2%).
Figure 1 demonstrates the distribution of pediatric cancer throughout the state of Delaware.
Figure 1.
Geo-mapping of the State of Delaware Childhood Cancer, 2004–2014.
Figure 1.
Geo-mapping of the State of Delaware Childhood Cancer, 2004–2014.
Table 1 illustrates the distribution of cancers as frequencies (proportionate morbidity) in the three counties within the state of Delaware. The cancer counts in New Castle
n = 296 (65%), Kent County
n = 91 (18.9%), and Sussex County
n = 94 (19.5%). These data reflect the proportionate morbidity of cancer within these geographic areas. The cumulative incidence was comparable among the three counties during this time period, New Castle County (
n = 296, population size = 125,079, CI = 237 per 100,000 children), Kent County (
n = 91, population size = 40,379, CI = 225 per 100,000), and Sussex County (
n = 94, population size = 40,307, CI = 233 per 100,000).
Table 1.
Proportion of pediatric malignancies in the three counties of Delaware relative to the state of Delaware.
Table 1.
Proportion of pediatric malignancies in the three counties of Delaware relative to the state of Delaware.
| County | Cancer Count | Proportion | Standard Error |
|---|
| New Castle | 296 | 0.6515 | 0.022 |
| Kent County | 91 | 0.1891 | 0.0179 |
| Sussex | 94 | 0.195 | 0.0181 |
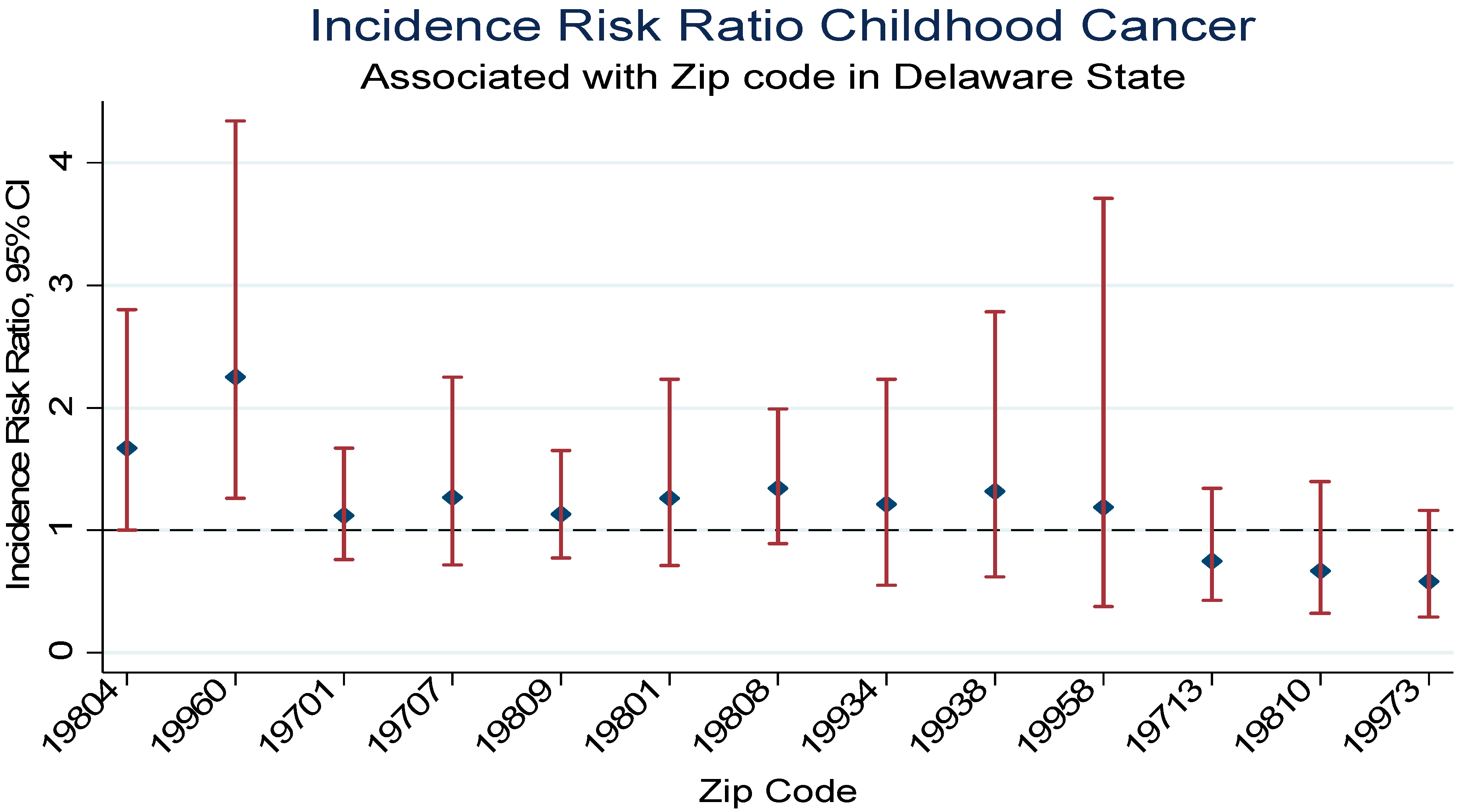
Table 2 demonstrates the incidence risk ratio of pediatric malignancy by zip code using the state of Delaware as the reference group and the 2010 Census data as the population size for the pediatric age (0 to 17 years). Relative to the state of Delaware the cumulative incidence rate was higher in zip code 19804 with a significant 68% increase risk of developing pediatric cancer of all sites IRR = 1.68, 95% Confidence 1nterval (CI), 1.0–2.8,
p = 0.04. There were a total of 15 cancers diagnosed with seven malignancies between 2004 and 2008 and eight malignancies between 2009 and 2014 in zip code 19804. Additionally, an estimated nine malignancies were diagnosed among boys and six among girls. Acute lymphocytic leukemia accounted for three cases, CNS/Brain two cases, and lymphoma two cases. Other malignancies diagnosed included Acute myeloid leukemia (AML), renal, Hodgkin’s, endocrine gland, salivary gland, skin, placenta, and cancer of no specific site. Similarly, relative to the state of Delaware children in zip code 19960 were two times as likely to be diagnosed with childhood malignancy (IRR = 2.25, 95% CI, 1.26–4.34). Although imprecise, there were increased risk of childhood malignancies in 19701 (IRR 1.12), 19707 (IRR = 1.27), 19709 (IRR = 1.13), 19801 (IRR = 1.26), 19808 (IRR = 1.34), 19934 (IRR = 1.21), 19938 (IRR = 1.32), 19958 (IRR = 1.19) relative to the state of Delaware. In contrast, childhood malignancies were lower in zip codes 19713 (IRR = 0.75), 19810 (IRR = 0.67), 19966 (IRR = 0.67), 19973 (IRR = 0.58) compared to the state of Delaware.
Figure 2 demonstrates the incidence risk ratio for selected zip codes.
Table 2.
Incidence risk ratio of pediatric cancer by zip code.
Table 2.
Incidence risk ratio of pediatric cancer by zip code.
| Zip Code | Cancer (n) | Population Size | IRR | 95% CI |
|---|
| 19701 | 26 | 9885 | 1.12 | 0.76–1.67 |
| 19702 | 30 | 13732 | 0.93 | 0.65–1.35 |
| 19703 | 8 | 3416 | 1.00 | 0.50–2.01 |
| 19707 | 12 | 4033 | 1.27 | 0.72–2.25 |
| 19709 | 28 | 10628 | 1.13 | 0.77–1.65 |
| 19711 | 22 | 9131 | 1.03 | 0.67–1.58 |
| 19713 | 12 | 6806 | 0.75 | 0.43–1.34 |
| 19720 | 35 | 14748 | 1.01 | 0.72–1.43 |
| 19730 | 1 | 106 | 4.04 | 0.57–28.7 |
| 19734 | 6 | 3275 | 0.78 | 0.35–1.75 |
| 19801 | 12 | 4066 | 1.26 | 0.71–2.23 |
| 19802 | 14 | 6290 | 0.95 | 0.56–1.62 |
| 19803 | 9 | 4482 | 0.86 | 0.44–1.66 |
| 19804 | 15 | 3827 | 1.68 | 1.00–2.80 |
| 19805 | 23 | 10989 | 0.89 | 0.59–1.36 |
| 19807 | 3 | 1614 | 0.79 | 0.26–2.47 |
| 19808 | 25 | 7994 | 1.34 | 0.89–1.99 |
| 19809 | 7 | 2943 | 1.02 | 0.48–2.15 |
| 19810 | 8 | 5117 | 0.67 | 0.33–1.34 |
| 19901 | 21 | 8618 | 1.04 | 0.67–1.61 |
| 19904 | 20 | 8061 | 1.06 | 0.68–1.66 |
| 19933 | 5 | 2201 | 0.97 | 0.40–2.34 |
| 19934 | 8 | 3084 | 1.21 | 0.55–2.23 |
| 19938 | 7 | 2271 | 1.32 | 0.62–2.78 |
| 19939 | 3 | 1075 | 1.19 | 0.38–3.71 |
| 19940 | 1 | 1395 | 0.31 | 0.04–2.18 |
| 19943 | 6 | 2671 | 0.96 | 0.43–2.14 |
| 19945 | 3 | 1376 | 0.93 | 0.30–2.90 |
| 19946 | 1 | 1132 | 0.38 | 0.05–2.69 |
| 19947 | 8 | 4440 | 0.77 | 0.38–1.55 |
| 19950 | 7 | 1603 | 1.87 | 0.89–3.94 |
| 19951 | 2 | 334 | 2.56 | 0.64–10.3 |
| 19952 | 7 | 2557 | 1.17 | 0.55–2.47 |
| 19953 | 2 | 1097 | 0.78 | 0.19–3.13 |
| 19955 | 1 | 13 | 32.9 | 4.63–234 |
| 19956 | 10 | 3992 | 1.07 | 0.57–2.00 |
| 19958 | 8 | 2866 | 1.19 | 0.59–2.40 |
| 19960 | 9 | 1714 | 2.25 | 1.16–4.34 |
| 19962 | 5 | 2923 | 0.73 | 0.30–1.77 |
| 19963 | 11 | 4477 | 1.05 | 0.58–1.91 |
| 19964 | 1 | 325 | 1.31 | 0.18–9.36 |
| 19966 | 7 | 4497 | 0.67 | 0.32–1.40 |
| 19968 | 3 | 2017 | 0.64 | 0.20–1.98 |
| 19970 | 4 | 769 | 2.22 | 0.83–5.95 |
| 19971 | 3 | 1491 | 0.86 | 0.28–2.68 |
| 19973 | 8 | 5942 | 0.58 | 0.29–1.16 |
| 19975 | 2 | 1382 | 0.62 | 0.15–2.48 |
| 19977 | 12 | 5352 | 0.96 | 0.54–1.70 |
Figure 2.
Pediatric Cancer Incidence Risk Ratio Associated with Selective Delaware Zip Codes, 2004–2014.
Figure 2.
Pediatric Cancer Incidence Risk Ratio Associated with Selective Delaware Zip Codes, 2004–2014.
Table 3 presents the incidence risk ratio (
Poisson Regression Model) of pediatric malignancy by county using the state of Delaware as the reference group and the 2010 Census data as the population size for the children age (0–17 years). The cumulative cancer incidence risk was comparable for the three counties albeit a 1% imprecise increased risk in New Castle County during the study period (IRR = 0.01, 95% CI 0.88–1.17).
Table 3.
Cummulative incidence risk ratio of pediatric cancer by county in DE, 2004–2014.
Table 3.
Cummulative incidence risk ratio of pediatric cancer by county in DE, 2004–2014.
| County | Cancer (n) | Population Size | IRR | 95% CI |
|---|
| New Castle | 296 | 125079 | 1.012 | 0.88–1.17 |
| Kent | 91 | 40379 | 0.964 | 0.77–1.20 |
| Sussex | 94 | 40307 | 0.997 | 0.80–1.24 |
3.5. Discussion
The basis for analytic cancer epidemiology is the descriptive finding, which allows for hypotheses generation in order to examine cancer determinants, risk markers, progression, and survival. With the limitations in this area (descriptive childhood cancer epidemiologic data) in the state of Delaware, we proposed to characterize childhood malignancies by geographic locale (zip code), sex, race, as well as temporal trends, and age at onset. There are a few relevant findings from our study. First, the cumulative incidence (period prevalence) was 234 per 100,000 children, implying an annual cumulative incidence of 23 per 100,000 children. Secondly, childhood cancer varies by geographic locale namely zip code. Thirdly, ALL significantly varied by race and brain/CNS was statistically marginally significant, while renal, endocrine gland, AML, lymphoma, and osteosarcoma although imprecise varied by sex and age at onset.
Cumulative incidence of cancer remains an important finding in understanding the burden of malignancies across specified populations. We have demonstrated that the cumulative incidence (period prevalence) of childhood cancer in the state of Delaware is 234 per 100,000 children, implying an annual cumulative incidence of 23 per 100,000 children. Our findings indicate an increase relative to the National Cancer Institute (NCI) data on the annual incidence for childhood cancer in the nation [
21]. The observed increase in annual cumulative incidence in DE may be due to several individual and ecologic factors including though not limited to the environment, parental lifestyle and occupation, exposure such as passive and first-hand smoking, socio-economic status as well as exposure of children to ionizing radiation [
16]. In contrast, this increase may be due to changes or differences in the classification of childhood malignancy and the age categories used to define childhood tumors. We used the ICD-9 classification code, implying cancer registries or systems that use different classification code may have different pediatric tumor prevalence. We were unable to compare the observed cumulative incidence with the Delaware Cancer Registry which is maintained by the Delaware Health and Social Services (DHSS) Division of Public Health, since the DHSS presented their recent findings on age- specific all site cancer incidence in the years 2007 to 2011 with an overlapping interval of 0 to 39 years of age (incidence rate = 54.6 per 100,000 population) for age at diagnosis [
18].
We observed significant geographic variation in our data using geo-coding mapping based on the zip codes in the state of Delaware. The zip codes with highest cumulative incidence were 19804 (Newport) and 19960 (Lincoln). The observed cumulative incidence in these zip codes is indicative of some environmental factors or other known or unmeasured potential carcinogens as well as cancer predisposing factors including, though not limited to, lifestyle variables, paternal occupation, pre and postnatal exposure, maternal hormone, host factor (Fanconi’s anemia, ataxia-telangiectasia, Down syndrome, neurofibromatosis), family history or gene-environment interaction [
16]. Risk and predisposing factors assessment in childhood cancer remains complex and often inconclusive, given the small size of these studies, and the lack of rigorous examination of records which tends to limit the inference drawn from these studies. Additionally some studies do not assess or control for confounding, resulting in biased findings leading to inconsistent associations (none, positive, negative).
While cancer has a very long induction period and insulting pathogens may never be known [
22], the presence of potential carcinogens in a physical environment may predispose to cancers hence, evidence of excessive cumulative incidence in some geographic locale. Whereas environmental data were not available to us at the time of this study, it is plausible to expect these zip codes to be affiliated with industrial areas or zones in the state of Delaware that may have a relatively excess poor air quality and other environmental toxins. Parental occupation mainly hydrocarbon-related work, metal-related work and radiation-related work had been implicated in childhood cancer development. Some studies have shown association between lead and Wilms tumors, as well as acute non-lymphocytic leukemia, metals and hepatocellular carcinoma, and metal-related work and brain tumor [
16]. The zip code 19804 in Newport is affiliated with chemical companies as well as automotive industries. Some epidemiologic data associate hydrocarbon- related work namely service station attendants, motor vehicle mechanics, machinists, lumberman, painters, dyers and cleaners with childhood cancer [
23], while paternal occupation mainly gas station attendants, automobile or truck repair, and aircraft maintenance is linked with infant leukemia, and maternal occupation mainly laundry/dry cleaning has been related with Wilm’s tumor [
24]. Brain and CNS tumors in children has been associated with parental occupation namely electricians, electrical and electronic workers [
16,
23]. The companies in this zip code, and the products generated have been implicated as potential carcinogens [
25,
26,
27,
28]. In effect, this may very well explain why childhood cancer cumulative incidence was excessive in Newport compared to the state of Delaware cumulative incidence. While the timing of exposure around preconception, and gestation is important in the implication of these potential carcinogens in childhood cancer, it is relevant to note the difficulties in conclusive inference, given several limitations of these often case-control studies, namely recall bias, broad categories of employment, information abstraction from administrative data not intended for research purpose, and multiple agents exposure. Notwithstanding the uncertainties in the implications these parental occupation related carcinogens, our findings of excess pediatric cancer in this zip code support other data associating this geographic locale with all age highest cancer incidence in the state of Delaware [
28].
Lincoln, zip code 19960, is a largely agriculturally-based community, indicating the possibility for potential carcinogens around the environment, given the nature of pesticides used on the land that may affect the respiratory tract as well as other organ systems involving inhalation or ingestion [
27]. Paternal, gestational and postnatal exposure to pesticides among agricultural workers had been associated with childhood cancer [
16,
23]. This geographic locale is associated with a large area of farmland, implying the potential use of parental pesticide as well as external exposure on clothing to drive the excessive childhood cancer incidence in Lincoln. While pesticide exposure has been implicated in cancer carcinogenesis, the specific mechanism with a given pesticide has not been fully understood, however the pathway to carcinogenesis involves bioaccumulation and the potential damage to the DNA, inhibiting apoptosis (programmed cell death) [
27,
29].
Additionally, because of the genetic predisposition to cancer, it is not unlikely to expect the populations in these zip codes with the highest cumulative incidence of pediatric cancer to have a family history of cancer relatively higher than other zip codes, indicative of epi-genetic predisposition. Despite this possibility, it is highly unlikely that the excessive cumulative incidence of childhood cancer in these zip codes (19804 and 19960) is due to genetic, family history of cancer or host factors only, but gene-environment interaction remains a possible explanation. Overall, our findings support previously published data on cancer incidence in both adult and childhood population by geographic locale in Delaware [
26].
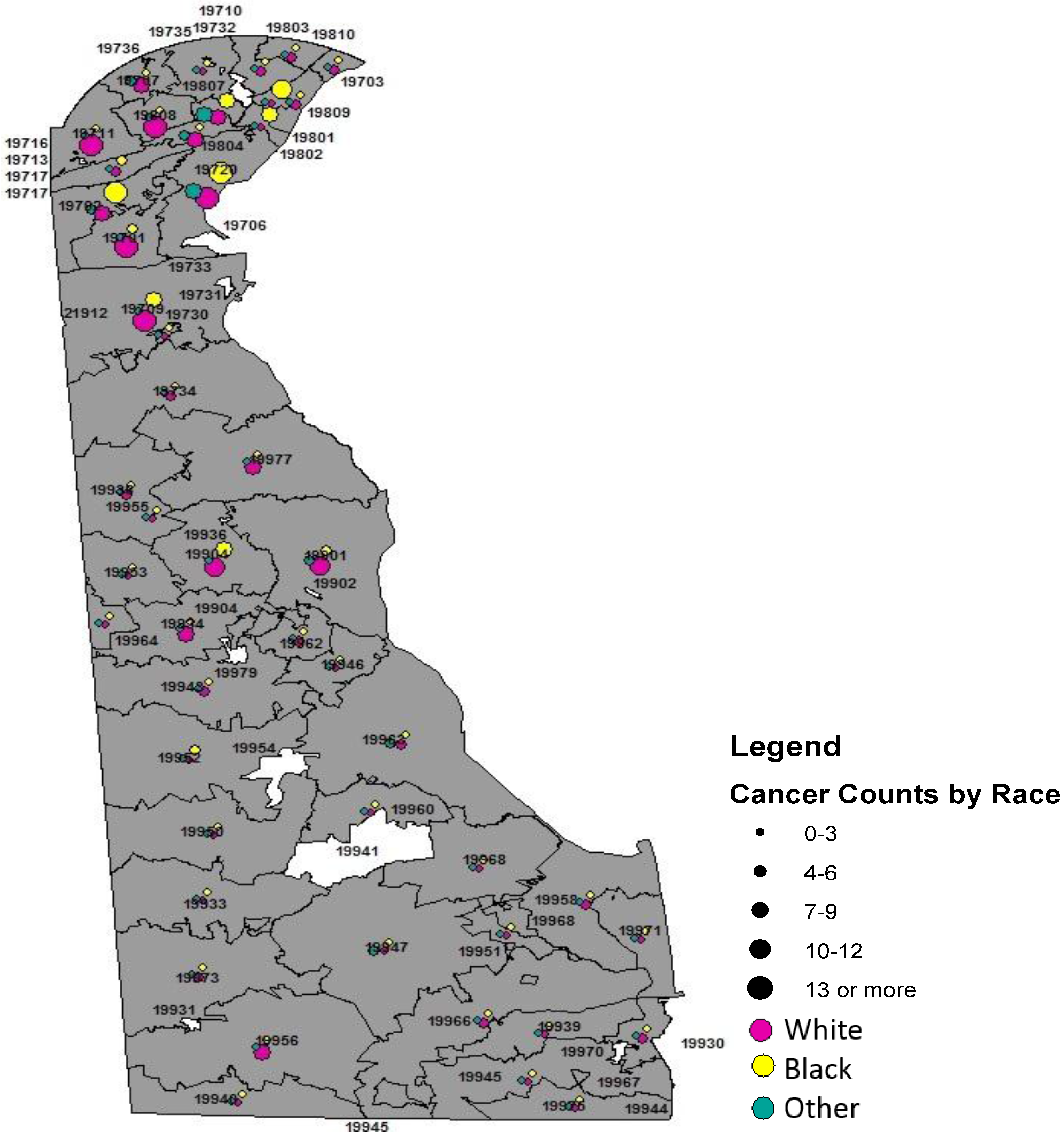
Black children had a higher cumulative incidence of cancer of all sites than whites (223 per 100,000
vs. 210 per 100,000). Epidemiologic data continue to associate higher incidence of childhood cancer, ALL, and thyroid with white children [
6,
7], however our data did not support this observation with overall childhood cancer. Acute lymphoblastic leukemia (ALL) was more common among white children, affirming previous data [
7,
8]. Studies on social class had shown the link between higher socio-economic status (SES) and increased risk of leukemia [
16], and the increased risk of ALL among whites may reflect race as SES surrogate. Data are lacking on overall childhood cancer incidence and SES. However it is worthy to note that these studies may be difficult to interpret without data completeness for the assessment of confounding and effect measure modifier prior to the inference drawn. The current study supports previous finding by Holmes
et al. on leukemia using SEER data from the 13 registries, 1973–2006 [
8], as well as recent findings that clearly illustrated the incidence disadvantage of whites [
7]. Renal carcinoma was more common among blacks relative to whites in our sample. This observation is comparable to other data sources and previous studies in this direction [
7].
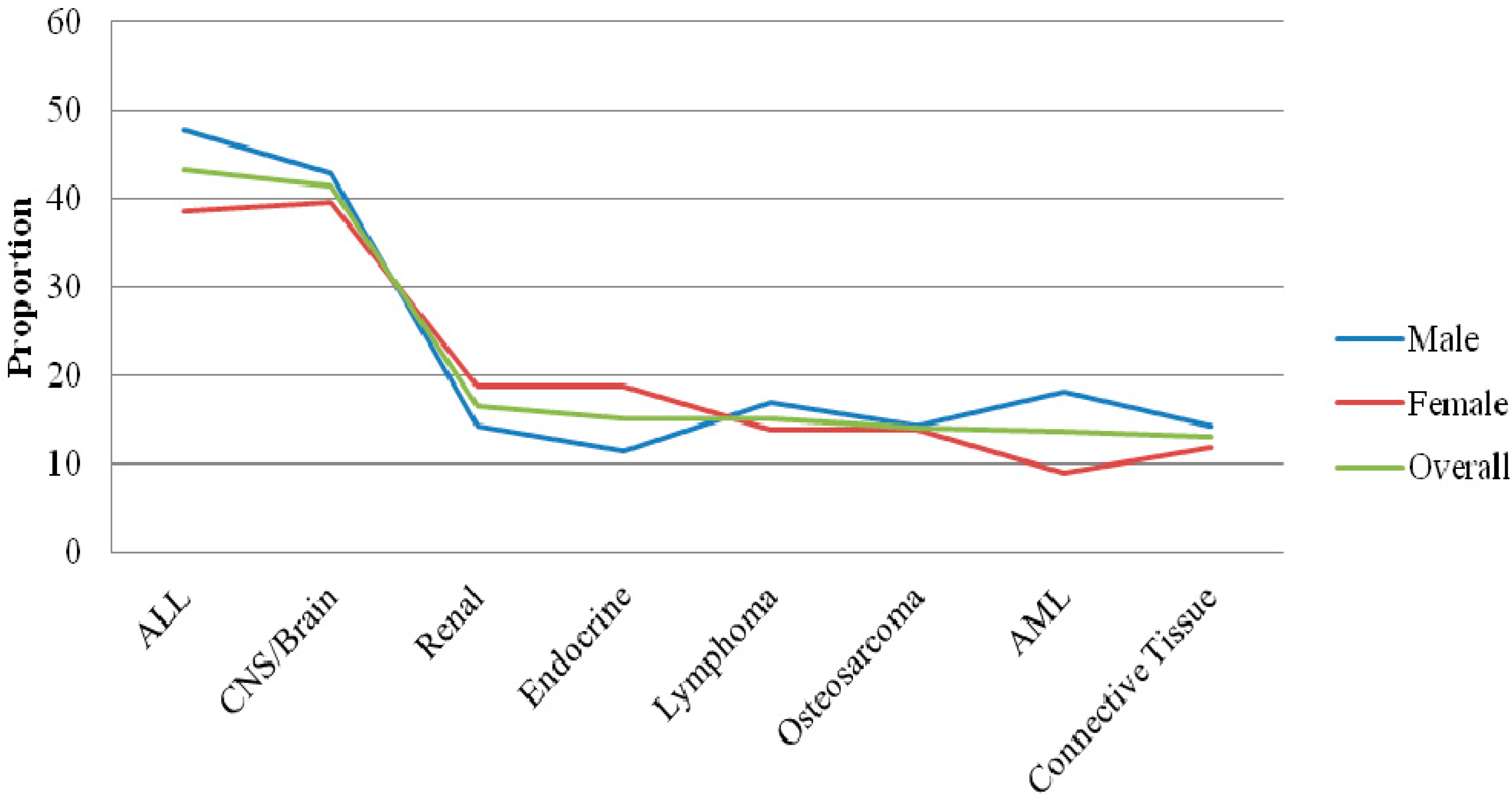
This study observed sex variability in renal carcinoma, thus affirming previous studies comparing the incidence of renal carcinoma between boys and girls [
7]. Furthermore, our data supports biologic variation in female urethra and the potentials for increasing anatomic insult compared to male urethra. While infection with in utero viral pathogens mainly influenza in childhood leukemia, herpesviruses with childhood cancer, as well as Wilm’s tumor with mothers diagnosed vaginal infections [
16], these data remain very inconclusive. Additionally, endocrine gland malignancy was more common among white girls relative to black girls and white boys. Endocrine tumors tend to be more prevalent in women compared to men [
9]. This observation has been explained by the predominant role of estrogen in endocrine tumors in women. While specific data are not available to our knowledge, it is plausible that the increased prevalence of endocrine tumors in girls is associated with hormonal involvement and imbalance between estrogen and progesterone [
9]. AML as well as lymphoma was more common in boys relative to girls. AML, which is relatively more common among boys being a very aggressive malignancy, may explain why boys have survival disadvantage following overall childhood cancer diagnosis and specifically leukemias. However, there is no clear and specific biologic mechanism to account for the preferential occurrence of this malignancy in boys.
Although difficult to establish, we observed temporal trends or patterns in pediatric cancer in our sample. The observation of increasing trend in 2004–2008 may be due to the spike in tumor cumulative incidence in 2004. A possible explanation for the spike was that local private oncology practices paired with A.I. duPont Hospital for Children, implying increased patient volume.
Despite the strength of this descriptive clinical epidemiology of childhood cancer in the state of Delaware, there are some limitations. First, the population sizes for the overall pediatric population in the state as well as the zip codes vary from year to year. In effect, using the Census population size for 2010 may indicate an underestimation of the children population size. However, this underestimation because it is a non-differential misclassification may not affect the cumulative incidence risk ratio of childhood cancer by geographic locale (zip code) if the population projection is comparable across the zip codes. Secondly, our inability to compare these findings with that of the state of Delaware Health and Social Services as a result of the state’s cancer registry recent findings that lump pediatric cancer with adult malignancy by using the age at diagnosis category of 0 to 39 years. Thirdly, Nemours Data Warehouse does not communicate in terms of record linkage with the Delaware Cancer Registry, which may result in the possibility of tumor diagnosis misrepresentation. Fourthly, due to the lack of individual level income data, we were unable to characterize tumor distribution by income level, restricting our ability to examine the effect of SES on childhood cancer incidence in our sample. Lastly, our descriptive cancer estimates may indicate underestimation due to children from the state of Delaware receiving cancer treatment from other hospitals, namely, the Children’s Hospital of Philadelphia (CHOP). Despite this flux to other states for care, our cancer patients represent an estimated 80+% of children with cancer in the state of Delaware, implying a representative sample for a reliable estimate.




{kind=link}
{kind=link}
{kind=link}
{kind=link}


