
Mortality during a Large-Scale Heat Wave by Place, Demographic Group, Internal and External Causes of Death, and Building Climate Zone

Abstract
:1. Introduction
2. Materials and Methods
2.1. Mortality Data Source
2.2. Definitions of Heat Wave Deaths and Expected Deaths
2.3. Statistical Analysis: Relative Risk and Excess Deaths
2.4. Definitions of Subgroups and Temperature Data
3. Results
3.1. Place of Death
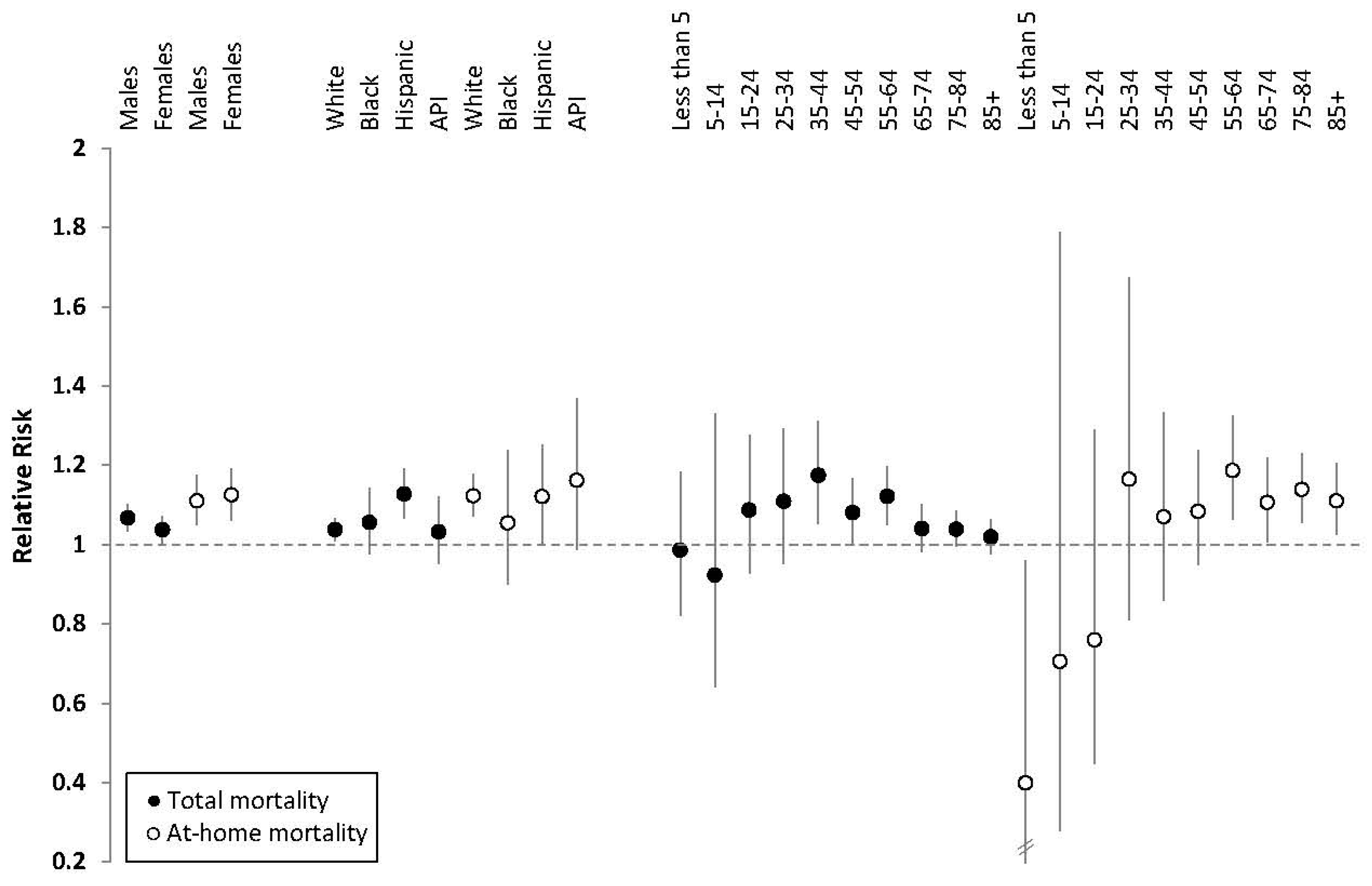
3.2. Demographics
3.3. Internal and External Causes of Death
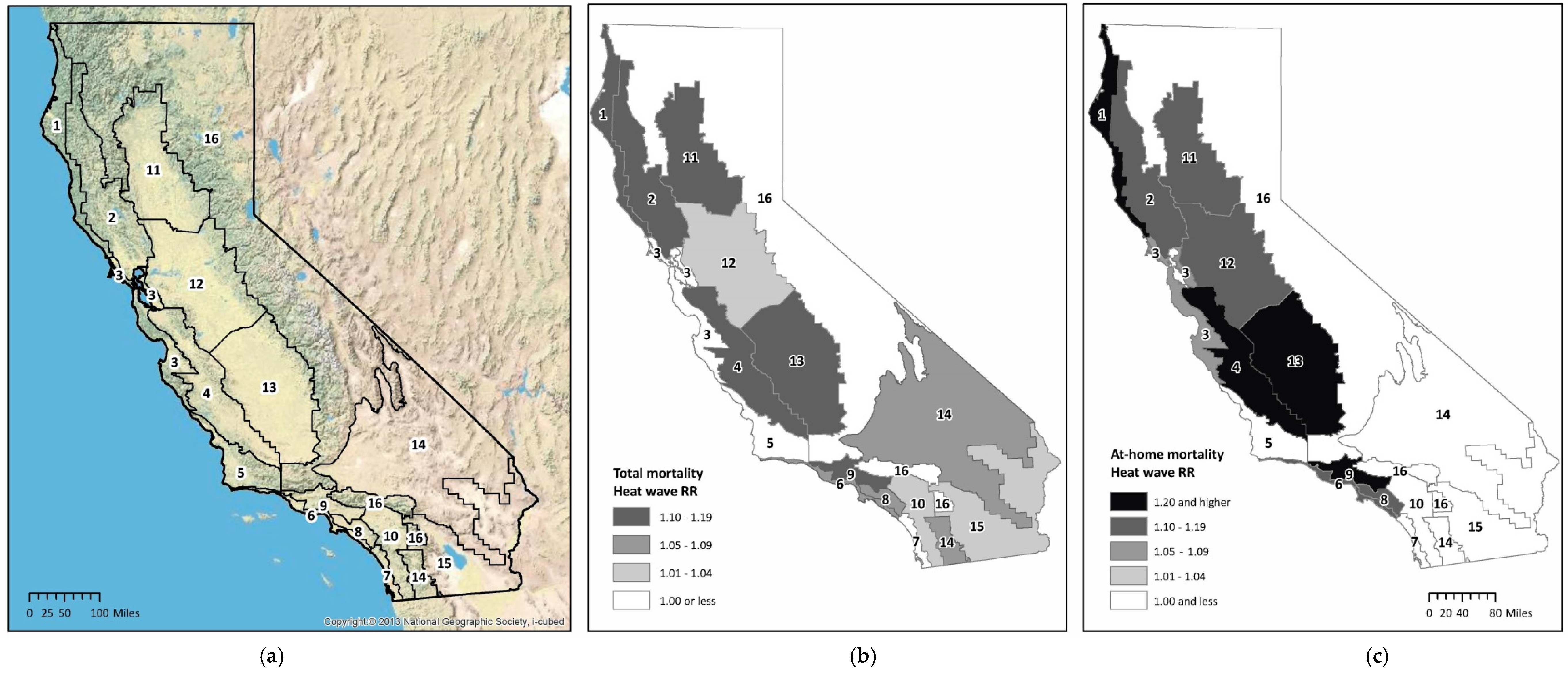
3.4. Geography
4. Discussion
Other Considerations and Limitations
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| AC | Air conditioning |
| API | Asian/Hawaiian/Pacific Islanders |
| CI | Confidence interval |
| RR | Relative risk |
References
- Intergovernmental Panel on Climate Change (IPCC). Climate Change 2014: Synthesis Report; IPCC: Geneva, Switzerland, 2014. [Google Scholar]
- Cayan, D.; Tyree, M.; Dettinger, M.; Hidalgo, H.; Das, T.; Maurer, E.; Bromirski, P.; Graham, N.; Flick, R. Climate Change Scenarios and Sea Level Rise Estimates for the California 2009 Climate Change Scenarios Assessment; California Energy Comission: Sacramento, CA, USA, 2012. [Google Scholar]
- Matthies, F.; Bickler, G.; Marin, N.C.; Hales, S. Heat-Health Action Plans Guidance; World Health Organization: Copenhagen, Denmark, 2008. [Google Scholar]
- Lowe, D.; Ebi, K.L.; Forsberg, B. Heatwave early warning systems and adapation advice to reduce human health consequences of heatwaves. Int. J. Environ. Res. Public Health 2011, 8, 4623–4648. [Google Scholar] [CrossRef] [PubMed]
- Climate Action Team, California Department of Public Health (CDPH). Preparing California for Extreme Heat: Guidance and Recommendations; CDPH: Sacramento, CA, USA, 2013. [Google Scholar]
- Interagency Working Group on Climate Change and Health (IWGCCH). A Human Health Perspective on Climate Change: A Report Outlining the Research Needs on the Human Health Effects of Climate Change; Environmental Health Perspectives/National Institute of Environmental Health Sciences: Research Triangle Park, NC, USA, 2010. [Google Scholar]
- Kovats, R.S.; Hajat, S. Heat stress and public health: A critical review. Annu. Rev. Public Health 2008, 29, 41–55. [Google Scholar] [CrossRef] [PubMed]
- Benmarhnia, T.; Deguen, S.; Kaufman, J.S.; Smargiassi, A. Vulnerability to heat-related mortality: A systematic review, meta-analysis, and meta-regression analysis. Epidemiology 2015, 26, 781–793. [Google Scholar] [CrossRef] [PubMed]
- Semenza, J.C.; Rubin, C.H.; Falter, K.H.; Selanikio, J.D.; Flanders, W.D.; Howe, H.L.; Wilhelm, J.L. Heat-related deaths during the July 1995 heat wave in Chicago. N. Engl. J. Med. 1996, 335, 84–90. [Google Scholar] [CrossRef] [PubMed]
- Medina-Ramon, M.; Zanobetti, A.; Cavanagh, D.P.; Schwartz, J. Extreme temperatures and mortality: Assessing effect modification by personal characteristics and specific cause of death in a multi-city case-only analysis. Environ. Health Perspect. 2006, 114, 1331–1336. [Google Scholar] [CrossRef] [PubMed]
- Kosatsky, T.; Henderson, S.B.; Pollock, S.L. Shifts in mortality during a hot weather event in Vancouver, British Columbia: Rapid assessment with case-only analysis. Am. J. Public Health 2012, 102, 2367–2371. [Google Scholar] [CrossRef] [PubMed]
- Price, K.; Perron, S.; King, N. Implementation of the Montreal heat response plan during the 2010 heat wave. Can. J. Public Health 2013, 104, e96–e100. [Google Scholar] [PubMed]
- Gronlund, C.J. Racial and socioeconomic disparities in heat-related health effects and their mechanisms: A review. Curr. Epidemiol. Rep. 2014, 1, 165–173. [Google Scholar] [CrossRef] [PubMed]
- Basu, R. High ambient temperature and mortality: A review of epidemiologic studies from 2001 to 2008. Environ. Health 2009, 8. [Google Scholar] [CrossRef] [PubMed]
- Anderson, B.G.; Bell, M.L. Weather-related mortality: How heat, cold, and heat waves affect mortality in the United States. Epidemiology 2009, 20, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Basu, R.; Ostro, B.D. A multicounty analysis identifying the populations vulnerable to mortality associated with high ambient temperature in California. Am. J. Epidemiol. 2008, 168, 632–637. [Google Scholar] [CrossRef] [PubMed]
- Anderson, G.B.; Bell, M.L. Heat waves in the United States: Mortality risk during heat waves and effect modification by heat wave characteristics in 43 U.S. communities. Environ. Health Perspect. 2011, 119, 210–218. [Google Scholar] [CrossRef] [PubMed]
- Curriero, F.C.; Heiner, K.S.; Samet, J.M.; Zeger, S.L.; Strug, L.; Patz, J.A. Temperature and mortality in 11 cities of the Eastern United States. Am. J. Epidemiol. 2002, 155, 80–87. [Google Scholar] [CrossRef] [PubMed]
- Hajat, S.; Armstrong, B.; Baccini, M.; Biggeri, A.; Bisanti, L.; Russo, A.; Paldy, A.; Menne, B.; Kosatsky, T. Impact of high temperatures on mortality: Is there an added heat wave effect? Epidemiology 2006, 17, 632–638. [Google Scholar] [CrossRef] [PubMed]
- Ostro, B.D.; Roth, L.A.; Green, R.S.; Basu, R. Estimating the mortality effect of the July 2006 California heat wave. Environ. Res. 2009, 109, 614–619. [Google Scholar] [CrossRef] [PubMed]
- Rocklöv, J.; Ebi, K.; Forsberg, B. Mortality related to temperature and persistent extreme temperatures: A study of cause-specific and age-stratified mortality. Occup. Environ. Med. 2011, 68, 531–536. [Google Scholar] [CrossRef] [PubMed]
- Rocklöv, J.; Barnett, A.G.; Woodward, A. On the estimation of heat-intensity and heat-duration effects in time series models of temperature-related mortality in Stockholm, Sweden. Environ. Health 2012, 11. [Google Scholar] [CrossRef] [PubMed]
- D’Ippoliti, D.; Michelozzi, P.; Marino, C.; De’donato, F.; Menne, B.; Katsouyanni, K.; Kirchmayer, U.; Analitis, A.; Medina-Ramon, M.; Paldy, A.; et al. The impact of heat waves on mortality in 9 European cities: Results from the Euroheat Project. Environ. Health 2010, 9. [Google Scholar] [CrossRef] [PubMed]
- Schifano, P.; Leone, M.; de Sario, M.; De’donato, F.; Bargagli, A.M.; D’Ippoliti, D.; Marino, C.; Michelozzi, P. Changes in the effects of heat on mortality among the elderly from 1998–2010: Results from a multicenter time series study in Italy. Environ. Health 2012, 11. [Google Scholar] [CrossRef] [PubMed]
- Son, J.Y.; Lee, J.T.; Anderson, G.B.; Bell, M.L. The impact of heat waves on mortality in seven major cities in Korea. Environ. Health Perspect. 2012, 120, 566–571. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.; Nordio, F.; Zanobetti, A.; Kinney, P.; Vautard, R.; Schwartz, J. Acclimatization across space and time in the effects of temperature on mortality: A time-series analysis. Environ. Health 2014, 13. [Google Scholar] [CrossRef] [PubMed]
- Peng, R.D.; Bobb, J.F.; Tebaldi, C.; McDaniel, L.; Bell, M.L.; Dominici, F. Toward a quantitative estimate of future heat wave mortality under global climate change. Environ. Health Perspect. 2011, 119, 701–706. [Google Scholar] [CrossRef] [PubMed]
- Reid, C.E.; Mann, J.K.; Alfasso, R.; English, P.B.; King, G.C.; Lincoln, R.A.; Margolis, H.G.; Rubado, D.J.; Sabato, J.E.; West, N.L.; et al. Evaluation of a heat vulnerability index on abnormally hot days: An environmental public health tracking study. Environ. Health Perspect. 2012, 120, 715–720. [Google Scholar] [CrossRef] [PubMed]
- Nitschke, M.; Tucker, G.R.; Hansen, A.L.; Williams, S.; Zhang, Y.; Bi, P. Impact of two recent extreme heat episodes on morbidity and mortality in Adelaide, South Australia: A case-series analysis. Environ. Health 2011, 10. [Google Scholar] [CrossRef] [PubMed]
- Basagana, X.; Sartini, C.; Barrera-Gomez, J.; Dadvand, P.; Cunillera, J.; Ostro, B.; Sunyer, J.; Medina-Ramon, M. Heat waves and cause-specific mortality at all ages. Epidemiology 2011, 22, 765–772. [Google Scholar] [CrossRef] [PubMed]
- Schuman, S.H. Patterns of urban heat-wave deaths and implications for prevention: Data from New York and St. Louis during July, 1966. Environ. Res. 1972, 5, 59–75. [Google Scholar] [CrossRef]
- Becker, J.A.; Stewart, L.K. Heat-related illness. Am. Fam. Phys. 2011, 83, 1325–1330. [Google Scholar]
- Gershunov, A.; Cayan, D.R.; Lacobellis, S.F. The Great 2006 Heat Wave over California and Nevada: Signal of an increasing trend. J. Clim. 2009, 22, 6181–6203. [Google Scholar] [CrossRef]
- Knowlton, K.; Rotkin-Ellman, M.; King, G.; Margolis, H.G.; Smith, D.; Solomon, G.; Trent, R.; English, P. The 2006 California heat wave: Impacts on hospitalizations and emergency department visits. Environ. Health Perspect. 2009, 117, 61–67. [Google Scholar] [CrossRef] [PubMed]
- Hoshiko, S.; English, P.; Smith, D.; Trent, R. A simple method for estimating excess mortality due to heat waves, as applied to the 2006 California heat wave. Int. J. Public Health 2010, 55, 133–137. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). International Classification of Diseases, 10th Revision (ICD-10); WHO: Geneva, Switzerland, 2006. [Google Scholar]
- Blier, W. The Record-Breaking Central California Heat Wave of July 2006. In Proceedings of the 22nd Conference on Weather Analysis and Forecasting/18th Conference on Numerical Weather Prediction, Park City, Utah, USA, 25–29 June 2007.
- Rothman, K.; Greenland, S.; Lash, T. Modern Epidemiology; Lippencott Williams & Wilkins: Philadelphia, PA, USA, 2008; pp. 243–244. [Google Scholar]
- Centers for Disease Control and Prevention. U.S. Standard Certificate of Death (rev. 11/2003). Available online: http://www.cdc.gov/nchs/data/dvs/DEATH11–03final-ACC.pdf (accessed on 15 December 2014).
- California Energy Commission. Energy Building Regulations for New Residential and Nonresidential Buildings: New Residential Buildings; Title 24, California Energy Commission: Sacramento, CA, USA, 1981. [Google Scholar]
- California Energy Commission. California Energy Maps—California Building Climate Zone Areas. Available online: http://www.energy.ca.gov/maps/renewable/building_climate_zones.html (accessed 30 Jan 2013).
- California Environmental Protection Agency, Air Resources Board. Air Quality and Meteorological Information System. Available online: http://www.arb.ca.gov/airqualitytoday (accessed on 22 December 2011).
- Ostro, B.; Rauch, S.; Green, R.; Malig, B.; Basu, R. The effects of temperature and use of air conditioning on hospitalizations. Am. J. Epidemiol. 2010, 172, 1053–1061. [Google Scholar] [CrossRef] [PubMed]
- National Weather Service Prediction Center. The Heat Index Equation. Available online: http://www.wpc.ncep.noaa.gov/html/heatindex_equation.shtml (accessed on 23 November 2015).
- Bassil, K.L.; Cole, D.C. Effectiveness of public health interventions in reducing morbidity and mortality during heat episodes: A structured review. Int. J. Environ. Res. Public Health 2010, 7, 991–1001. [Google Scholar] [CrossRef] [PubMed]
- Trent, R.B. Review of July 2006 Heat Wave Related Fatalities in California. Available online: http://www.cdph.ca.gov/HealthInfo/injviosaf/Documents/HeatPlanAssessment-EPIC.pdf (accessed on 2 December 2015).
- Luginbuhl, R.; Jackson, L.; Castillo, D.; Loringer, K. Heat-related deaths among crop workers—United States, 1992–2006. MMWR Morb. Mortal Wkly. Rep. 2008, 57, 649–653. [Google Scholar]
- Toloo, G.S.; Fitzgerald, G.; Aitken, P.; Verrall, K.; Tong, S. Are heat warning systems effective? Environ. Health 2013, 12. [Google Scholar] [CrossRef] [PubMed]
- Gasparrini, A.; Armstrong, B. The impact of heat waves on mortality. Epidemiology 2011, 22, 68–73. [Google Scholar] [CrossRef] [PubMed]
- Hertel, S.; le Tertre, A.; Jockel, K.H.; Hoffmann, B. Quantification of the heat wave effect on cause-specific mortality in Essen, Germany. Eur. J. Epidemiol. 2009, 24, 407–414. [Google Scholar] [CrossRef] [PubMed]
- Xu, Z.; Sheffield, P.E.; Su, H.; Wang, X.; Bi, Y.; Tong, S. The impact of heat waves on children’s health: A systematic review. Int. J. Biometeorol. 2014, 58, 239–247. [Google Scholar] [CrossRef] [PubMed]
- Basu, R.; Pearson, D.; Sie, L.; Broadwin, R. A case-crossover study of temperature and infant mortality in California. Paediatr. Perinat. Epidemiol. 2015, 29, 407–415. [Google Scholar] [CrossRef] [PubMed]
- Rogers, P.; Buttice, M.K. Farmworkers in California: A Brief Introduction; California Research Bureau: Sacramento, CA, USA, 2013. [Google Scholar]
- Basu, R.; Pearson, D.; Malig, B.; Broadwin, R.; Green, R. The effect of high ambient temperature on emergency room visits. Epidemiology 2012, 23, 813–820. [Google Scholar] [CrossRef] [PubMed]
- Noe, R.S.; Jin, J.O.; Wolkin, A.F. Exposure to natural cold and heat: Hypothermia and hyperthermia medicare claims, United States, 2004–2005. Am. J. Ppublic Health 2012, 102, e11–e18. [Google Scholar] [CrossRef] [PubMed]
- Bohnert, A.S.; Prescott, M.R.; Vlahov, D.; Tardiff, K.J.; Galea, S. Ambient temperature and risk of death from accidental drug overdose in New York City, 1990–2006. Addiction 2010, 105, 1049–1054. [Google Scholar] [CrossRef] [PubMed]
- Mayo Clinic. Heatstroke. Available online: http://www.mayoclinic.org/diseases-conditions/heat-stroke/basics/risk-factors/CON-20032814 (accessed on 4 January 2016).
- Anderson, C.A.; Bushman, B.J.; Groom, R.W. Hot years and serious deadly assault: Empirical tests of the heat hypothesis. J. Personal. Soc. Psychol. 1997, 73, 1213–1223. [Google Scholar] [CrossRef]
- Deisenhammer, E.A.; Kemmler, G.; Parson, P. Association of meteorlogical factors with suicide. Acta Psychiatr. Scand. 2003, 108, 455–459. [Google Scholar] [CrossRef] [PubMed]
- Morabito, M.; Crisci, A.; Moriondo, M.; Profili, F.; Francesconi, P.; Trombi, G.; Bindi, M.; Gensini, G.F.; Orlandini, S. Air temperature-related human health outcomes: Current impact and estimations of future risks in Central Italy. Sci. Total Environ. 2012, 441, 28–40. [Google Scholar] [CrossRef] [PubMed]
- Zhou, W.; Ji, S.; Chen, T.H.; Hou, Y.; Zhang, K. The 2011 heat wave in greater Houston: Effects of land use on temperature. Environ. Res. 2014, 135. [Google Scholar] [CrossRef] [PubMed]
- De la Rue du Can, S.; Leventis, G.; Shah, N.; McNeil, M.A. Cooling the Growth of Air Conditioners Energy Consumption; Berkeley National Laboratory, International Energy Studies Group: Berkeley, CA, USA, 2015. [Google Scholar]
- Dahl, R. Cooling concepts: Alternatives to air conditioning for a warm world. Environ. Health Perspect. 2013, 121, A18–A25. [Google Scholar] [CrossRef] [PubMed]
- Mills, E. Climate change, insurance and the buildings sector: Technological synergisms between adaptation and mitigation. Build. Res. Inf. 2003, 31, 257–277. [Google Scholar] [CrossRef]
- Vandentorren, S.; Bretin, P.; Zeghnoun, A.; Mandereau-Bruno, L.; Croisier, A.; Cochet, C.; Riberon, J.; Siberan, I.; Declercq, B.; Ledrans, M. August 2003 heat wave in France: Risk factors for death of elderly people living at home. Eur. J. Public Health 2006, 16, 583–591. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Place of Death | Heat Wave Deaths a | Reference Day Deaths/2 b | RR (CI) | Excess Deaths c |
|---|---|---|---|---|
| All deaths | 11,727 | 11,144 | 1.05 (1.03–1.08) | 582 |
| Inside hospital d | 4933 | 4820 | 1.02 (0.99–1.06) | 113 |
| Outside hospital | 6670 | 6197 | 1.08 (1.05–1.11) | 473 |
| Decedent‘s home | 3646 | 3262 | 1.12 (1.07–1.16) | 384 |
| Hospice or nursing home | 2218 | 2156 | 1.03 (0.98–1.08) | 62 |
| Other | 806 | 779 | 1.04 (0.95–1.13) | 27 |
| Unknown | 124 | 127 | 0.97 (0.79–1.21) | −3 |
| Underlying Cause of Death (ICD-10 Codes) | Total Mortality | At-Home Mortality | ||||||
|---|---|---|---|---|---|---|---|---|
| Heat Wave a | Reference/2 b | Relative Risk (CI) | Excess Deaths | Heat Wave | Reference/2 | Relative Risk (CI) | Excess Deaths | |
| Internal causes (A00–R94) | 10,575 | 10,167 | 1.04 (1.02–1.07) * | 408 | 3382 | 3053 | 1.11 (1.06–1.16) * | 330 |
| Mental/nervous system (F00–H95) | 935 | 841 | 1.11 (1.03–1.20) * | 94 | 259 | 212 | 1.22 (1.05–1.43) * | 47 |
| Endocrine Disease (E00–88) | 483 | 448 | 1.08 (0.97–1.20) | 35 | 163 | 119 | 1.38 (1.13–1.68) * | 45 |
| Respiratory system (J00–99) | 1042 | 973 | 1.07 (0.99–1.16) | 69 | 243 | 217 | 1.12 (0.95–1.31) | 26 |
| Other internal diseases (L00–R99) | 515 | 488 | 1.06 (0.95–1.17) | 27 | 88 | 77 | 1.14 (0.87–1.48) | 11 |
| Cardiovascular (I00–99) | 4169 | 4014 | 1.04 (1.00–1.08) | 155 | 1292 | 1095 | 1.18 (1.10–1.26) * | 198 |
| Digestive system (K00–92) | 443 | 434 | 1.02 (0.91–1.14) | 9 | 67 | 71 | 0.94 (0.70–1.25) | −5 |
| Neoplasms (C00–D48) | 2769 | 2739 | 1.01 (0.97–1.06) | 30 | 1249 | 1231 | 1.01 (0.95–1.09) | 18 |
| Infectious and parasitic (A00–B99) | 219 | 230 | 0.95 (0.81–1.12) | −11 | 21 | 29 | 0.71 (0.43–1.17) | −9 |
| External causes (V01–Y89.9) | 1152 | 977 | 1.18 (1.10–1.27) * | 175 | 264 | 210 | 1.26 (1.08–1.47) * | 54 |
| External causes, excluding X30 | 1053 | 971 | 1.09 (1.01–1.17) * | 83 | 221 | 209 | 1.05 (0.90–1.24) | 12 |
| Related to extreme heat (X30) | 99 | 7 | 15.2 (8.54–27.1) * | 92 | 43 | 1 | 86.0 (11.8–624.5) * | 43 |
| Accidental drowning (W65–74) | 57 | 43 | 1.33 (0.95–1.85) | 14 | 8 | 1 | 8.00 (1.70–37.67) * | 7 |
| Accidental poisoning (X40–49) | 182 | 145 | 1.26 (1.04–1.51) * | 37 | 88 | 69 | 1.28 (0.98–1.67) | 19 |
| Homicide (X85–Y09, Y87.1) | 170 | 145 | 1.17 (0.97–1.42) | 25 | 16 | 18 | 0.89 (0.49–1.60) | −2 |
| Falls (W00–19) | 91 | 83 | 1.09 (0.84–1.41) | 8 | 5 | 7 | 0.67 (0.24–1.83) | −3 |
| Transport accidents (V01–99, Y85) | 292 | 278 | 1.05 (0.91–1.21) | 14 | 1 | 1 | 0.67 (0.07–6.41) | −1 |
| Other external c | 92 | 91 | 1.01 (0.79–1.30) | 1 | 12 | 16 | 0.75 (0.39–1.46) | −4 |
| Suicide (X60–84, Y87.0) | 169 | 185 | 0.91 (0.76–1.10) | −16 | 91 | 97 | 0.94 (0.73–1.21) | −6 |
| Climate Zone | Representative City/Climate Type a | Total Mortality | At-Home Mortality | ADAT during Peak Heat Wave b °F (°C) | Peak Heat Wave ADAT Differential (°F) c | % AC Ownership d | ||
|---|---|---|---|---|---|---|---|---|
| Relative Risk (CI) | Excess Deaths | Relative Risk (CI) | Excess Deaths | |||||
| 1 | Arcata/coastal | 1.19 (0.89–1.59) | 12 | 1.58 (1.01–2.48) * | 13 | 81 (27) | 23 | 4% |
| 4 | Sunnyvale/coastal interior | 1.14 (1.02–1.26) * | 65 | 1.22 (1.01–1.46) * | 32 | 82 (28) | 17 | 48% |
| 2 | Santa Rosa/coastal interior | 1.14 (1.00–1.29) | 45 | 1.10 (0.89–1.36) | 13 | 85 (29) | 10 | 43% |
| 11 | Red Bluff/N Central Valley | 1.12 (1.00–1.26) | 50 | 1.18 (0.97–1.44) | 24 | 87 (31) | 14 | 89% |
| 13 | Fresno/S Central Valley | 1.11 (1.02–1.22) * | 74 | 1.43 (1.21–1.68) * | 75 | 88 (31) | 13 | 89% |
| 9 | Pasadena/coastal interior | 1.10 (1.04–1.17) * | 168 | 1.20 (1.08–1.34) * | 86 | 84 (29) | 15 | 76% |
| n/a e | n/a | 1.10 (0.98–1.23) | 42 | 1.32 (0.92–1.91) | 12 | n/a | n/a | n/a |
| 6 | Los Angeles/coastal | 1.06 (0.98–1.15) | 51 | 1.10 (0.95–1.27) | 26 | 74 (23) | 11 | 31% |
| 8 | El Toro/coastal | 1.05 (0.98–1.13) | 61 | 1.19 (1.05–1.36) * | 58 | 79 (26) | 11 | 55% |
| 14 | China Lake/desert | 1.05 (0.91–1.21) | 14 | 0.98 (0.77–1.24) | −2 | 85 (29) | 10 | 88% |
| 10 | Riverside/coastal interior | 1.03 (0.96–1.11) | 39 | 0.97 (0.86–1.10) | -11 | 84 (29) | 13 | 87% |
| 12 | Sacramento/Central Valley | 1.02 (0.96–1.08) | 27 | 1.11 (0.99–1.25) | 48 | 88 (31) | 19 | 86% |
| 15 | El Centro/desert | 1.02 (0.87–1.20) | 6 | 0.98 (0.75–1.29) | −2 | 94 (34) | 8 | 97% |
| 3 | Oakland/coastal | 0.99 (0.92–1.06) | −11 | 1.06 (0.93–1.21) | 21 | 72 (22) | 14 | 11% |
| 7 | San Diego/coastal | 0.97 (0.88–1.07) | −20 | 0.97 (0.81–1.15) | −7 | 78 (26) | 12 | 32% |
| 5 | Santa Maria/coastal | 0.90 (0.72–1.11) | −14 | 0.98 (0.68–1.40) | −1 | 76 (24) | 15 | 15% |
| 16 | Mount Shasta/mountainous | 0.90 (0.76–1.06) | −24 | 1.00 (0.76–1.31) | 0 | 78 (26) | 13 | 56% |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Joe, L.; Hoshiko, S.; Dobraca, D.; Jackson, R.; Smorodinsky, S.; Smith, D.; Harnly, M. Mortality during a Large-Scale Heat Wave by Place, Demographic Group, Internal and External Causes of Death, and Building Climate Zone. Int. J. Environ. Res. Public Health 2016, 13, 299. https://doi.org/10.3390/ijerph13030299
Joe L, Hoshiko S, Dobraca D, Jackson R, Smorodinsky S, Smith D, Harnly M. Mortality during a Large-Scale Heat Wave by Place, Demographic Group, Internal and External Causes of Death, and Building Climate Zone. International Journal of Environmental Research and Public Health. 2016; 13(3):299. https://doi.org/10.3390/ijerph13030299
Chicago/Turabian StyleJoe, Lauren, Sumi Hoshiko, Dina Dobraca, Rebecca Jackson, Svetlana Smorodinsky, Daniel Smith, and Martha Harnly. 2016. "Mortality during a Large-Scale Heat Wave by Place, Demographic Group, Internal and External Causes of Death, and Building Climate Zone" International Journal of Environmental Research and Public Health 13, no. 3: 299. https://doi.org/10.3390/ijerph13030299
APA StyleJoe, L., Hoshiko, S., Dobraca, D., Jackson, R., Smorodinsky, S., Smith, D., & Harnly, M. (2016). Mortality during a Large-Scale Heat Wave by Place, Demographic Group, Internal and External Causes of Death, and Building Climate Zone. International Journal of Environmental Research and Public Health, 13(3), 299. https://doi.org/10.3390/ijerph13030299