
Wayfinding the Live 5-2-1-0 Initiative—At the Intersection between Systems Thinking and Community-Based Childhood Obesity Prevention


Abstract
:1. Introduction
- Supporting the development of meaningful partnerships and networks in new Live 5-2-1-0 communities;
- Achieving sustained partnerships in existing Live 5-2-1-0 communities that are functioning with tangible results (i.e., implementation of community action plans, development of new or enhancement of existing initiatives, or broadening multi-sector engagement); and
- Transferring knowledge gained in SCOPE’s first phase between communities while still responding and adapting to complex, non-linear community dynamics by identifying: (i) the key knowledge that is necessary to share between communities (i.e., sharing of common resources, collaborative program planning between Live 5-2-1-0 communities); and (ii) the model features that are best implemented with fidelity vs. those requiring modification to suit local conditions.
2. Materials and Methods
2.1. The KE Model
- The Live 5-2-1-0 Online Resource Map [13] houses SCOPE’s resources (by sector) that can be downloaded for free and used across multiple community settings to share and support Live 5-2-1-0. These include videos, posters, fact sheets, newspaper/magazine advertisements, and a marketing guide to share the message; toolkits and checklists to build capacity among community stakeholders (i.e., service providers, recreation facilitators, health professionals, and educators) to support the message; and ‘how to’ guides that outline key steps in action implementation to facilitate broader dissemination of innovative ideas. These resources represent a key outcome of SCOPE’s collaborative partnerships where they were conceptualized by community partners and their creation was supported by the SCOPE team who provided insights on best practice and strategies to align with regional and provincial programs as well as the financial support necessary to create high quality materials. (Resources; Facilitation, coaching and training)
- Webinars are organized and held quarterly by the SCOPE team to provide the opportunity for new communities to interact with coordinators and stakeholders from existing Live 5-2-1-0 communities so that challenges and solutions to implementation, experiential learning, ongoing adaptation, and new ideas are shared. (Exchange of knowledge; Adaptation; Facilitation, coaching and training)
- The SCOPE team (2 full time staff and the principal investigator) is the backbone organization that supports BC communities in sharing and supporting Live 5-2-1-0 and facilitates the alignment of community- and provincial-level activities. SCOPE provides coordination, facilitation and training, and resource development and/or adaptation while also supporting local and provincial stakeholder engagement, communications, and evaluation. The SCOPE team leads the implementation of the KE model through a comprehensive community engagement process that involves engaging with community champions and leaders who express interest in implementing the initiative, and coaching stakeholders as they proceed through the various stages of implementation. This is achieved via presentations to community groups representing multiple sectors (i.e., healthy partnership table) or a single sector (i.e., schools, health, community services), formal workshops, and practical continuous ad hoc communication via email and phone. SCOPE also mobilizes funding to support local coordination, action implementation, and evaluation. (Engagement; Facilitation, coaching, and training; Resources; Adaptation; Mobilization of champions; Exchange of knowledge)
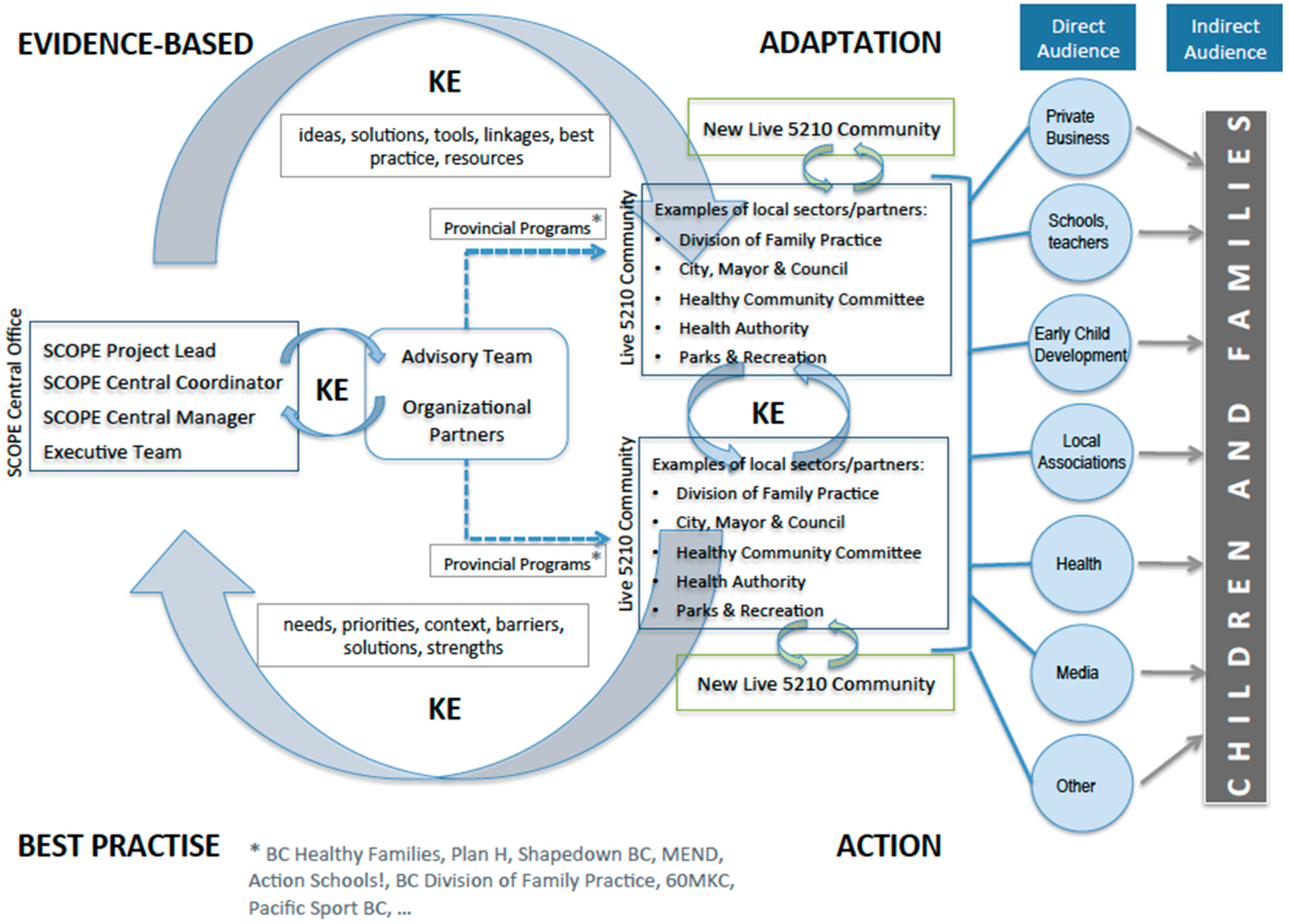
- A linking system (Figure 1) connects knowledge providers and knowledge users so that there is a ‘two-way’ exchange of knowledge. In our initiative, the central SCOPE team, advised by an executive of researchers and provincial- and community-level stakeholders, translate knowledge to community stakeholders (i.e., ideas, solutions, tools, linkages, best practice, resources) but also receive knowledge on the needs, priorities, contexts, and strengths of the local community, as well as their ideas for innovative local action. The linking system supports a process of continuous tailoring to meet the needs of local settings, contexts, and priorities (Adaptation) and also supports opportunities for Exchange of knowledge and Facilitation, coaching and training. The linking system allows for the SCOPE team to advise community stakeholders on best-practice so that community-tailored messaging and/or initiatives are aligned with evidence-based principles. For example, in community C, an intervention using ‘nudge’ theory has recently been implemented in a local grocery store that was informed by the evidence-base [14] and is currently being evaluated in the local context.
2.2. Theoretical Framework
2.3. Participating Communities
2.4. Data Collection and Analysis
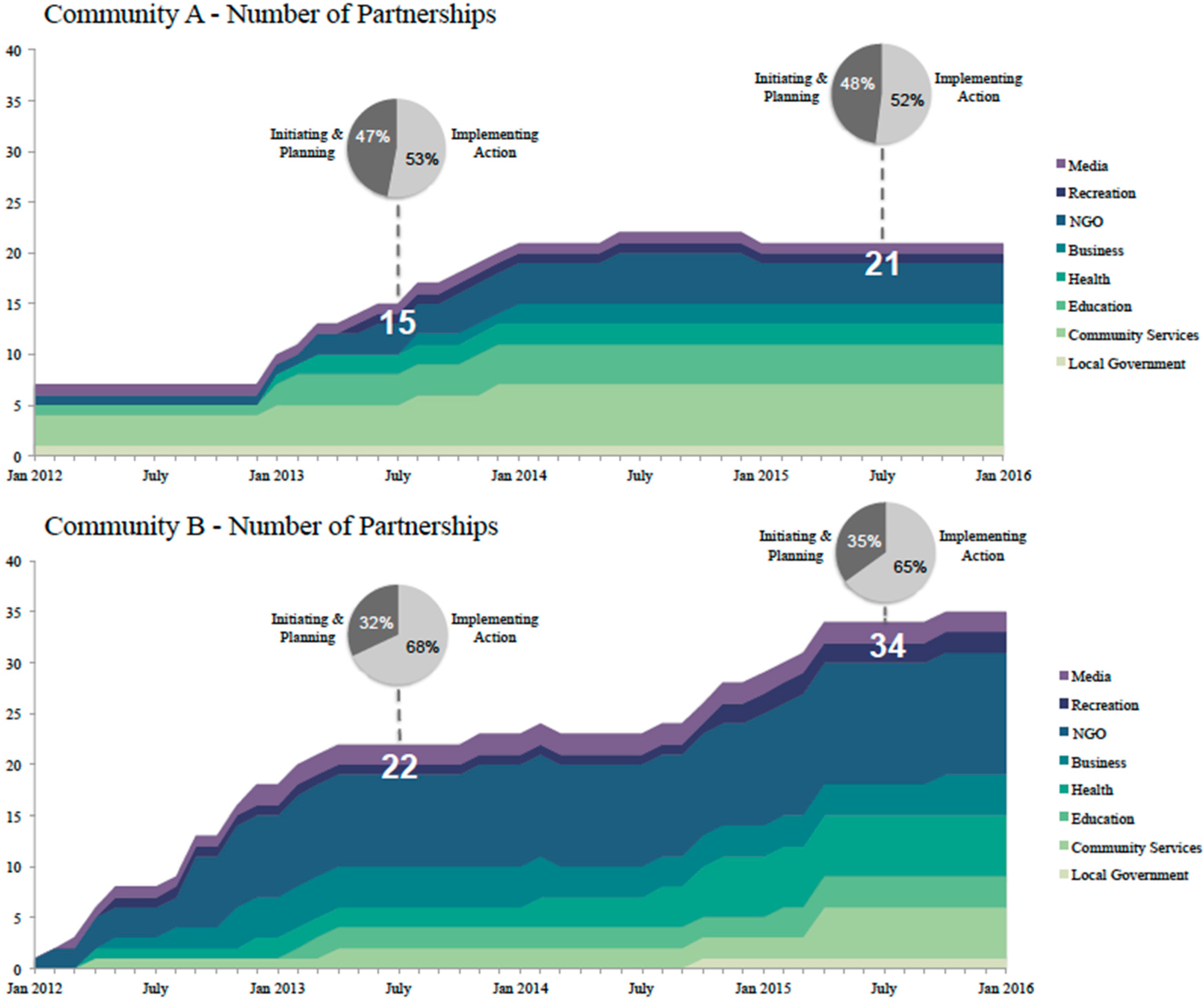
- Partnership Tracking Tool (PTT): The PTT is a shared data collection and management tool that was established in SCOPE’s first phase and since then has been adapted multiple times in response to the feedback provided by community stakeholders on ease of use and usability of the data. Today, the PTT is a data collection platform that can be accessed online (with a username and password) by the SCOPE team and key stakeholders within Live 5-2-1-0 communities. The overall objective of the platform is to track new and existing community partners engaged in sharing and supporting Live 5-2-1-0. Data collected includes information on the partner organization (i.e., sector represented), characteristics of the partnership (i.e., when the partnership was established, stage of partnership), and outcomes of the partnership (actions implemented, Live 5-2-1-0 resources disseminated, etc.). Data on each partnership is updated so that the progress of partnerships over time is captured in terms of whether they evolve from action planning to action implementation, or lapse over time. The PTT data are analyzed bi-annually both in aggregate form and by community.
- Community Capacity Building Tool (CCBT): The Public Health Agency of Canada’s (PHAC) CCBT is a valid, reliable tool that measures the community capacity building that occurs during the course of a project [19]. It measures change in community capacity over time with questions that cover nine domains (participation; leadership; community structures; role of external supports; asking why; obtaining resources; skills, knowledge, and learning; linking with others; sense of community). Responses are either yes/no or are on a four-point ordinal scale: (1) just started; (2) on the road; (3) nearly there; or (4) we’re there. Space is also available for free text to further describe each response. The CCBT was completed by each community at baseline with a plan to repeat the survey yearly for the duration of the project.
- Surveys: Community stakeholders who participate in SCOPE’s KE initiatives (i.e., webinars, workshops) are requested to complete a short survey asking about their satisfaction with the event, what aspects were most and/or least helpful, whether information received will influence action in their own community, and suggestions for improvement.
- Semi-structured Interviews (n = 35) (Table S1): Local community coordinators who lead the Live 5-2-1-0 initiative within their communities (n = 4) and who are the main liaison to the SCOPE central team participated in semi-structured qualitative interviews at the start of the study with the plan to repeat these interviews yearly. A convenience sample of other community stakeholders who are involved in delivering the Live 5-2-1-0 initiative within their own organizations or sectors also participated in semi-structured interviews where questions assessed awareness of Live 5-2-1-0, the utility of Live 5-2-1-0 resources, facilitators and barriers to use, and resource adaptation. These stakeholders represented various sectors (education, health, community services, local government, recreation, media, early childhood, businesses) who were engaged in implementing Live 5-2-1-0 in their organization or local business (C-A: n = 6; C-B: n = 9; C-C: n = 6; C-D: n = 10). Qualitative interviews were conducted at baseline with a plan to repeat them annually for the duration of the project.
- Web Analytics: The website [13] is monitored quarterly using web analytics where number of visitors to the resource page and resource downloads are tracked over time.
3. Results
3.1. Reach
3.2. Resources
3.3. Engagement and Mobilization of Champions
- “Our experience here in (community A), we really need to have a common cause, a common project, something that we’re working on with our partners to keep them engaged.” (C-A)
- “We’re keeping an actively engaged community that already has a really strong table for child and youth issues and an understanding of group organizations.” (C-B)
- “…just finding somebody who truly believes in the message so that you have a champion…, if you have somebody that is a champion then you will get really far but if you don’t have that champion in place, it sort of stalls the whole progress.” (C-C)
3.4. Facilitation, Coaching and Training, and Exchange of Knowledge
- “I love that it is a simple message and that it is very concise and easy to do…., and I think because it’s a community initiative, the piece for me is that it makes sense to do it because other people are doing it as well.” (C-D)
- “…yes we feel very confident in the messaging. It’s very simple and straightforward and the toolkit has really helped give staff the resources to deliver that message…” (C-A)
- “I do feel confident in implementing changes and I believe my fellow staff members feel confident. I think part of the reason we feel so confident is that we’ve gotten such excellent support from staff at your agency (SCOPE) and the materials you have provided us have given us excellent tools to work with.” (C-B)
- “I do feel confident sharing the message but I’m also very happy that the (SCOPE community partner organization) staff have been able to provide us with the support with staff that can actually come in and share the message. Whenever I’ve had questions about ways that I can creatively implement the message in my day-to-day programming, the staff has been available…” (C-B)
4. Discussion
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviation
| SCOPE | Sustainable Childhood Obesity Prevention through Community Engagement |
References
- Waters, E.; de Silva-Sanigorski, A.; Hall, B.J.; Brown, T.; Campbell, K.J.; Gao, Y.; Armstrong, R.; Prosser, L.; Summerbell, C.D. Interventions for preventing obesity in children. Cochrane Database Syst. Rev. 2011. [Google Scholar] [CrossRef]
- Skinner, A.C.; Foster, E.M. Systems Science and Childhood Obesity: A Systematic Review and New Directions. J. Obesity 2013, 2013, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Allender, S.; Owen, B.; Kuhlberg, J.; Lowe, J.; Nagorcka-Smith, P.; Whelan, J.; Bell, C. A Community Based Systems Diagram of Obesity Causes. PLoS ONE 2015. [Google Scholar] [CrossRef] [PubMed]
- Israel, B.A.; Schulz, A.J.; Parker, E.A.; Becker, A.B. Review of Community-based Research: Assessing Partnership Approaches to Improve Public Health. Annu. Rev. Public Health 1998, 19, 173–202. [Google Scholar] [CrossRef] [PubMed]
- Willows, N.D.; Hanley, A.J.G.; Delormier, T. A socioecological framework to understand weight-related issues in Aboriginal children in Canada. Appl. Physiol. Nutr. Metab. 2012, 37, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Kania, J.; Kramer, M. Collective impact. 2011. [Google Scholar]
- Amed, S.; Naylor, P.-J.; Pinkney, S.; Shea, S.; Mâsse, L.C.; Berg, S.; Collet, J.-P.; Wharf-Higgins, J. Creating a collective impact on childhood obesity: Lessons from the SCOPE initiative. Can. J. Public Health 2015. [Google Scholar] [CrossRef] [PubMed]
- McIntosh, B.; Daly, A.; Mâsse, L.C.; Collet, J.-P.; Higgins, J.W.; Naylor, P.-J.; Amed, S. Sustainable childhood obesity prevention through community engagement (SCOPE) program: Evaluation of the implementation phase. Biochem. Cell Biol. 2015, in press. [Google Scholar] [CrossRef] [PubMed]
- Orlandi, M.A. Health promotion technology transfer: organizational perspectives. Can. J. Public Health 1996, 87 (Suppl. S2), S28–S33. [Google Scholar] [PubMed]
- Robinson, K. Using linking systems to build capacity and enhance dissemination in heart health promotion: A Canadian multiple-case study. Health Educ. Res. 2005, 20, 499–513. [Google Scholar] [CrossRef] [PubMed]
- Glasgow, R.E.; Vogt, T.M.; Boles, S.M. Evaluating the Public Health Impact of Health Promotion Interventions: The RE-AIM Framework. Am. J. Public Health 1999, 89, 1322–1327. [Google Scholar] [CrossRef] [PubMed]
- Gaglio, B.; Glasgow, R.E. Evaluation approaches for dissemination and implementation research. In Dissemination and Implementation Research in Health—Translating Science into Action; Brownson, R.C., Colditz, G.A., Proctor, E.K., Eds.; Oxford University Press: New York, NY, USA, 2012. [Google Scholar]
- Live 5-2-1-0 Online Resource Map. Available online: http://www.live5210.ca/ (accessed on 15 June 2016).
- Payne, C.R.; Niculescu, M.; Just, D.R.; Kelly, M.P. Shopper marketing nutrition interventions: Social norms on grocery carts increase produce spending without increasing shopper budgets. Prev. Med. Rep. 2015, 2, 287–291. [Google Scholar] [CrossRef] [PubMed]
- Graham, I.D.; Logan, J.; Harrison, M.B.; Straus, S.E.; Tetroe, J.; Caswell, W.; Robinson, N. Lost in knowledge translation: Time for a map? J. Contin. Educ. Health Prof. 2006, 26, 13–24. [Google Scholar] [CrossRef] [PubMed]
- Economos, C.D.; Hyatt, R.R.; Goldberg, J.P.; Must, A.; Naumova, E.N.; Collins, J.J.; Nelson, M.E. A community intervention reduces BMI z-score in children: Shape up Somerville first year results. Obesity (Silver Spring) 2007, 15, 1325–1336. [Google Scholar] [CrossRef] [PubMed]
- Swinburn, B.; Malakellis, M.; Moodie, M.; Waters, E.; Gibbs, L.; Millar, L.; Herbert, J.; Virgo-Milton, M.; Mavoa, H.; Kremer, P.; et al. Large reductions in child overweight and obesity in intervention and comparison communities 3 years after a community project. Pediatr. Obes. 2014, 9, 455–462. [Google Scholar] [CrossRef] [PubMed]
- Sanigorski, A.M.; Bell, A.C.; Kremer, P.J.; Cuttler, R.; Swinburn, B.A. Reducing unhealthy weight gain in children through community capacity-building: Results of a quasi-experimental intervention program, Be Active Eat Well. Int. J. Obes. Relat. Metab. Disord 2008, 32, 1060–1067. [Google Scholar] [CrossRef] [PubMed]
- Maclellan-Wright, M.F.; Anderson, D.; Barber, S.; Smith, N.; Cantin, B.; Felix, R.; Raine, K. The development of measures of community capacity for community-based funding programs in Canada. Health Promot. Int. 2007, 22, 299–306. [Google Scholar] [CrossRef] [PubMed]
- Patton, M.Q. Qualitative Research & Evaluation Methods; Sage Publications: Thousand Oaks, CA, USA, 2001. [Google Scholar]
- Kessler, R.; Glasgow, R.E. A Proposal to Speed Translation of Healthcare Research into Practice. Am. J. Prev. Med. 2011, 40, 637–644. [Google Scholar] [CrossRef] [PubMed]
- Davies, R.; Dart, J. The “most significant change” (MSC) technique. In A Guide to Its Use; CARE International: Atlanta, GA, USA, 2005. [Google Scholar]
- Wilder, L.; Walpole, M. Measuring social impacts in conservation: Experience of using the Most Significant Change method. Oryx 2008, 42, 529. [Google Scholar] [CrossRef]
- Hawe, P.; Ghali, L. Use of social network analysis to map the social relationships of staff and teachers at school. Health Educ. Res. 2008, 23, 62–69. [Google Scholar] [CrossRef] [PubMed]
- Homer, J.B.; Hirsch, G.B. System dynamics modeling for public health: Background and opportunities. Am. J. Public Health 2006, 96, 452–458. [Google Scholar] [CrossRef] [PubMed]
- Hemming, K.; Haines, T.P.; Chilton, P.J.; Girling, A.J.; Lilford, R.J. The stepped wedge cluster randomised trial: rationale, design, analysis, and reporting. BMJ-Br. Med. J. 2015, 350. [Google Scholar] [CrossRef] [PubMed]
- Wharf, B.; McKenzie, B. Connecting Policy to Practice in the Human Services, 3rd ed.; McLelland & Stewart: Oxford, UK, 2009. [Google Scholar]
- Chinn, D.J.; White, M.; Howel, D.; Harland, J.O.E.; Drinkwater, C.K. Factors associated with non-participation in a physical activity promotion trial. Public Health 2006, 120, 309–319. [Google Scholar] [CrossRef] [PubMed]
- Sallis, J.F.; Cervero, R.B.; Ascher, W.; Henderson, K.A.; Kraft, M.K.; Kerr, J. An ecological approach to creating active living communities. Annu. Rev. Public Health 2006, 27, 297–322. [Google Scholar] [CrossRef] [PubMed]
- Green, L.W.; Glasgow, R.E. Evaluating the relevance, generalization, and applicability of research: Issues in external validation and translation methodology. Evaluat. Health Profess. 2006, 29, 126–153. [Google Scholar] [CrossRef] [PubMed]
- Green, L.W. Translation 2 research: The roadmap less traveled. Am. J. Prev. Med. 2007, 331, 137–138. [Google Scholar] [CrossRef]
- Dearing, J.W.; Maibach, E.W.; Buller, D.B. A convergent diffusion and social marketing approach for disseminating proven approaches to physical activity promotion. Am. J. Prev. Med. 2006, 31, S11–S23. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Model Component | Description |
|---|---|
| Reach | The extent of the key players, partnerships, and collaborations that are actively participating in the development and implementation of the project |
| Engagement | Developing, sustaining and fostering relationships that facilitate knowledge exchange and sharing |
| Facilitation, coaching, training | Technical support and sharing of expertise through active participation of knowledge-users and on-site coaching |
| Resources | Development of new or contextualization of existing resources to enhance self-efficacy and skills around administering childhood obesity prevention initiatives |
| Adaptation | Continuous tailoring and adapting of activities to local settings, contexts, needs and priorities |
| Mobilization of champions | Identifying and mobilizing key champions and early adopters who represent various community sectors |
| Exchange of knowledge | Multiple levels of continuous, bi-directional exchange of knowledge, learning, and expertise |
| Existing Communities | New Community | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| C-A | C-B | C-C | |||||||
| 2012 | 2013 | 2014 | 2015 | 2012 | 2013 | 2014 | 2015 | 2015 | |
| Community event | -- | 12 | 3 | 7 | 14 | 19 | 11 | 22 | 28 |
| Community presentation | -- | 4 | 3 | 6 | 2 | 6 | 9 | 18 | 15 |
| Policy/practice change | -- | -- | 2 | -- | -- | -- | 2 | 4 | 1 |
| Stakeholder engagement | 2 | 14 | 8 | 3 | 12 | 16 | 11 | 11 | 6 |
| Resource development/adaptation | -- | -- | -- | -- | -- | 1 | 3 | 4 | -- |
| Environmental change | -- | -- | 1 | 2 | -- | 1 | -- | 8 | -- |
| Funding | -- | -- | -- | -- | 6 | 14 | 3 | 6 | 2 |
| Training Workshop | -- | 3 | 4 | 2 | -- | -- | 6 | 2 | 3 |
| Other | -- | 2 | -- | -- | 3 | 9 | -- | 1 | 4 |
| Total | 2 | 35 | 21 | 21 | 37 | 66 | 45 | 76 | 59 |
| Mean Score * | ||||
|---|---|---|---|---|
| Existing | New | |||
| CCBT Domain (Description) Community: | A | B | C | D |
| Participation (active involvement of community stakeholders) | 3.00 | 3.75 | 2.25 | 2.00 |
| Leadership (engagement of and support from formal and informal local leaders) | 3.33 | 2.00 | 1.33 | 2.33 |
| Community structures (engagement of community groups and committees) | 2.33 | 3.00 | 1.67 | 1.67 |
| Role of external supports (support from local government, foundations, or regional health authorities) | 3.33 | 3.33 | 2.75 | 3.25 |
| Asking why (a process for uncovering root causes for community health issues and potential solutions) | 2.67 | 4.00 | 2.33 | 1.33 |
| Obtaining resources (finding time, money, leadership, volunteers, and information from both inside and outside the community) | 3.50 | 4.00 | 4.00 | 4.00 |
| Skills, knowledge, learning (qualities in the project team and broader community stakeholders) | 2.50 | 3.50 | 2.50 | 3.00 |
| Links with others (links with individuals and organizations through partnerships, networks, and coalitions) | 3.25 | 4.00 | 2.50 | 2.50 |
| Sense of community (People coming together to work on shared community problems through collaboration) | 3.00 | 4.00 | 2.00 | 3.00 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Amed, S.; Shea, S.; Pinkney, S.; Wharf Higgins, J.; Naylor, P.-J. Wayfinding the Live 5-2-1-0 Initiative—At the Intersection between Systems Thinking and Community-Based Childhood Obesity Prevention. Int. J. Environ. Res. Public Health 2016, 13, 614. https://doi.org/10.3390/ijerph13060614
Amed S, Shea S, Pinkney S, Wharf Higgins J, Naylor P-J. Wayfinding the Live 5-2-1-0 Initiative—At the Intersection between Systems Thinking and Community-Based Childhood Obesity Prevention. International Journal of Environmental Research and Public Health. 2016; 13(6):614. https://doi.org/10.3390/ijerph13060614
Chicago/Turabian StyleAmed, Shazhan, Stephanie Shea, Susan Pinkney, Joan Wharf Higgins, and Patti-Jean Naylor. 2016. "Wayfinding the Live 5-2-1-0 Initiative—At the Intersection between Systems Thinking and Community-Based Childhood Obesity Prevention" International Journal of Environmental Research and Public Health 13, no. 6: 614. https://doi.org/10.3390/ijerph13060614