
Relationships of Community and Individual Level Social Capital with Activities of Daily Living and Death by Gender

 , ,
, ,
Abstract
:1. Introduction
2. Methods
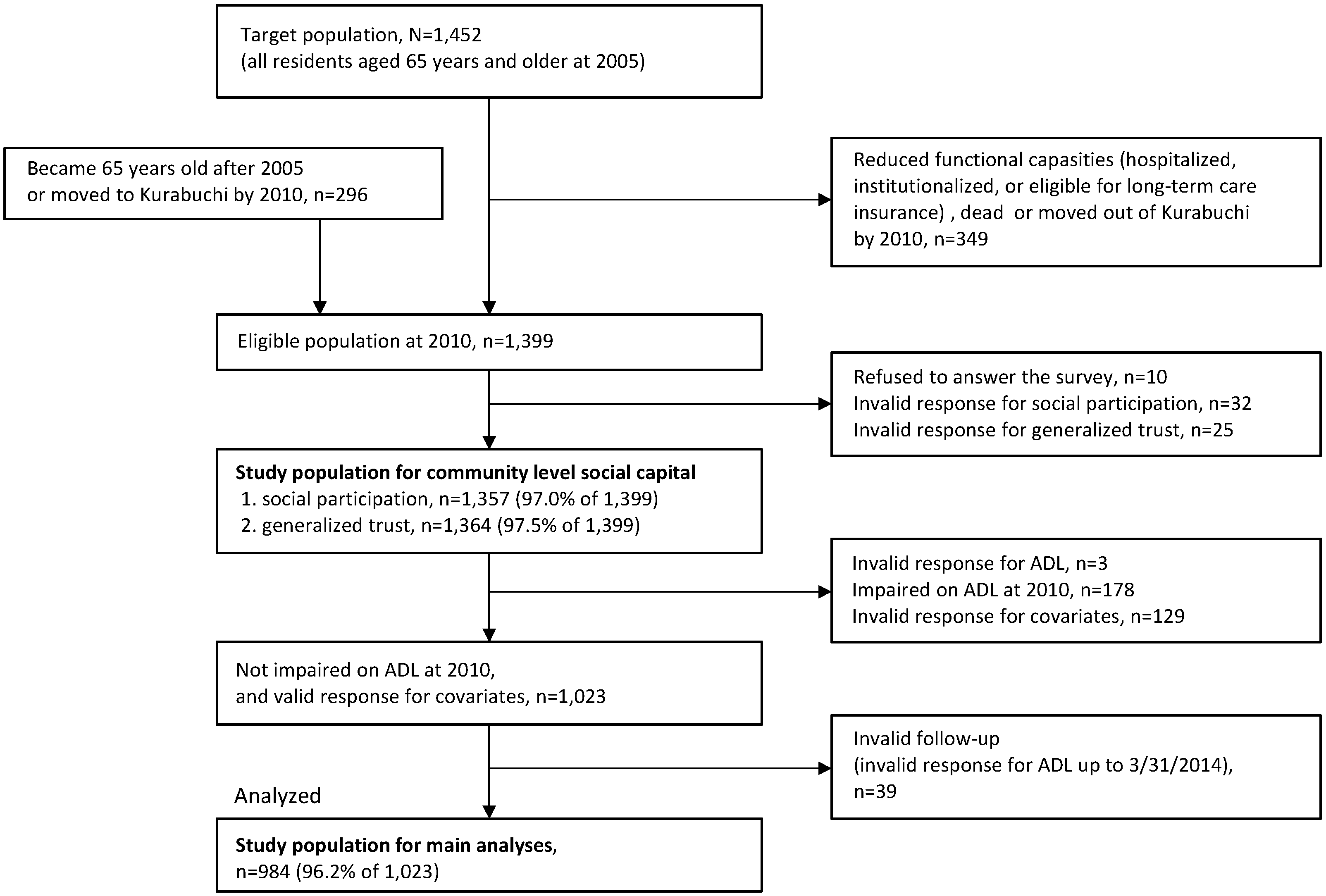
2.1. Study Population
2.2. Outcome Measurements
2.3. Social Capital
2.4. Covariates
2.5. Statistical Analysis
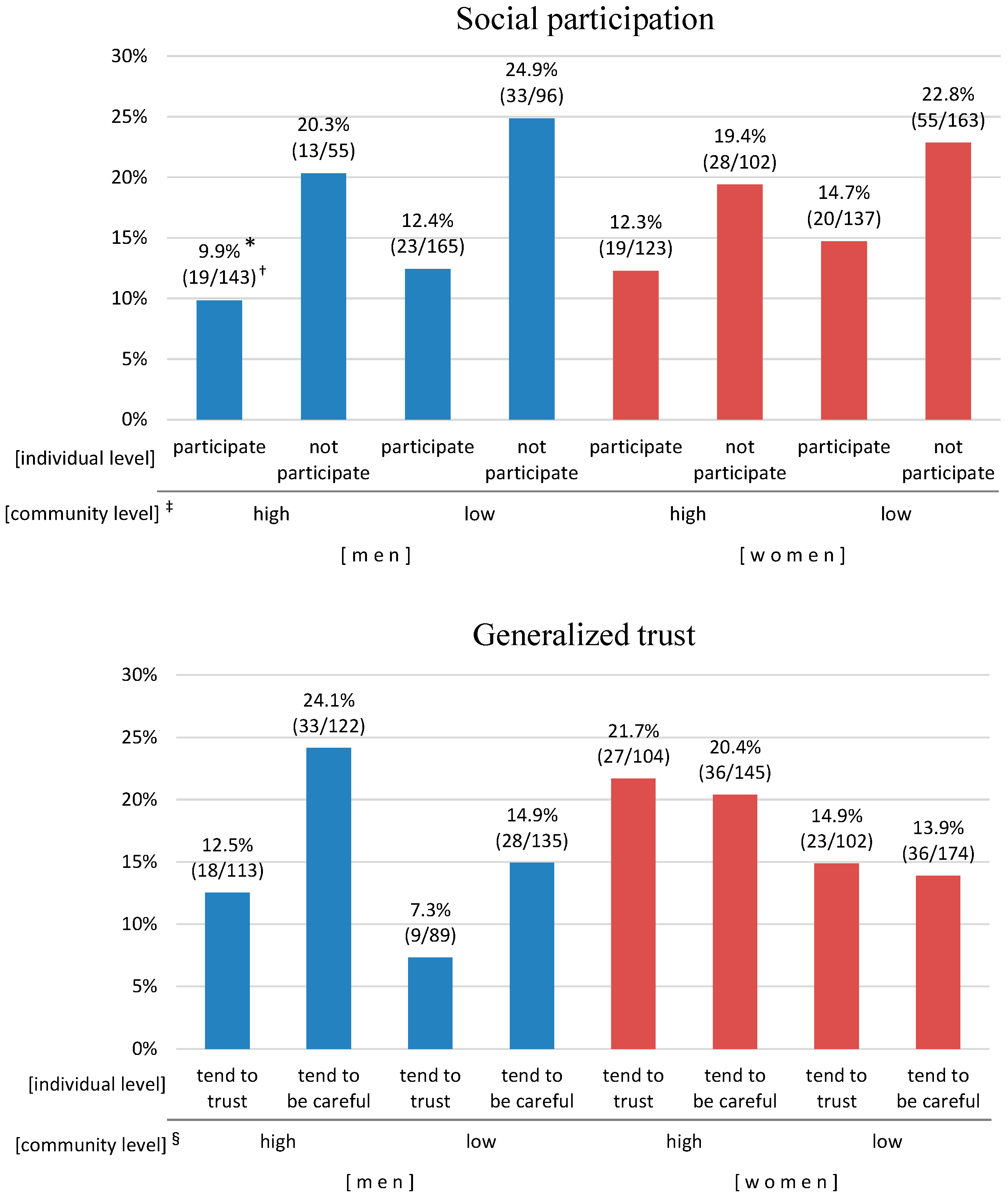
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| ADL | Activities of Daily Living |
| OR | odds ratio |
| CI | confidence interval |
References
- Putnam, R.D. Making Democracy Work: Civic Traditions in Modern Italy; Princeton University Press: Princeton, NJ, USA, 1993. [Google Scholar]
- Szreter, S.; Woolcock, M. Health by association? Social capital, social theory, and the political economy of public health. Int. J. Epidemiol. 2004, 33, 650–667. [Google Scholar] [CrossRef] [PubMed]
- Islam, M.K.; Merlo, J.; Kawachi, I.; Lindstrom, M.; Gerdtham, U.G. Social capital and health: Does egalitarianism matter? A literature review. Int. J. Equity Health 2006, 5, 3. [Google Scholar] [CrossRef] [PubMed]
- Harpham, T. The measurement of community social capital through surveys. In Social Capital and Health; Kawachi, I., Subramanian, S.V., Kim, D.J., Eds.; Springer: New York, NY, USA, 2008; pp. 51–62. [Google Scholar]
- Krishna, A.; Shrader, E. Cross-cultural measures of social capital: A tool and results from India and Panama. In Social Capital Initiative Working Paper No. 21; World Bank: Washington, DC, USA, 2000. [Google Scholar]
- Lin, N. Building a network theory of social capital. Connections 1999, 22, 28–51. [Google Scholar]
- Kawachi, I.; Subramanian, S.V.; Kim, D.J. Social capital and health: A decade of progress and beyond. In Social Capital and Health; Kawachi, I., Subramanian, S.V., Kim, D.J., Eds.; Springer: New York, NY, USA, 2008; pp. 1–26. [Google Scholar]
- Kawachi, I.; Barkman, L. Social cohesion, social capital, and health. In Social Epidemiology; Barkman, L., Kawachi, I., Eds.; Oxford University Press: New York, NY, USA, 2000; pp. 174–190. [Google Scholar]
- Murayama, H.; Fujiwara, Y.; Kawachi, I. Social capital and health: A review of prospective multilevel studies. J. Epidemiol./Jpn. Epidemiol. Assoc. 2012, 22, 179–187. [Google Scholar] [CrossRef]
- Kawachi, I.; Kennedy, B.P.; Glass, R. Social capital and self-rated health: A contextual analysis. Am. J. Public Health 1999, 89, 1187–1193. [Google Scholar] [CrossRef] [PubMed]
- Subramanian, S.V.; Kim, D.J.; Kawachi, I. Social trust and self-rated health in us communities: A multilevel analysis. J. Urban Health 2002, 79, S21–S34. [Google Scholar] [CrossRef] [PubMed]
- Yip, W.; Subramanian, S.V.; Mitchell, A.D.; Lee, D.T.; Wang, J.; Kawachi, I. Does social capital enhance health and well-being? Evidence from rural China. Soc. Sci. Med. 2007, 64, 35–49. [Google Scholar] [CrossRef] [PubMed]
- Ferlander, S.; Makinen, I.H. Social capital, gender and self-rated health. Evidence from the moscow health survey 2004. Soc. Sci. Med. 2009, 69, 1323–1332. [Google Scholar] [CrossRef] [PubMed]
- Campos-Matos, I.; Subramanian, S.V.; Kawachi, I. The “dark side” of social capital: Trust and self-rated health in european countries. Eur. J. Public Health 2016, 26, 90–95. [Google Scholar] [CrossRef] [PubMed]
- Engstrom, K.; Mattsson, F.; Jarleborg, A.; Hallqvist, J. Contextual social capital as a risk factor for poor self-rated health: A multilevel analysis. Soc. Sci. Med. 2008, 66, 2268–2280. [Google Scholar] [CrossRef] [PubMed]
- Verhaeghe, P.P.; Tampubolon, G. Individual social capital, neighbourhood deprivation, and self-rated health in England. Soc. Sci. Med. 2012, 75, 349–357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murayama, H.; Wakui, T.; Arami, R.; Sugawara, I.; Yoshie, S. Contextual effect of different components of social capital on health in a suburban city of the greater Tokyo area: A multilevel analysis. Soc. Sci. Med. 2012, 75, 2472–2480. [Google Scholar] [CrossRef] [PubMed]
- Hamano, T.; Fujisawa, Y.; Ishida, Y.; Subramanian, S.V.; Kawachi, I.; Shiwaku, K. Social capital and mental health in Japan: A multilevel analysis. PLoS ONE 2010, 5, e13214. [Google Scholar] [CrossRef]
- Stafford, M.; De Silva, M.; Stansfeld, S.; Marmot, M. Neighbourhood social capital and common mental disorder: Testing the link in a general population sample. Health Place 2008, 14, 394–405. [Google Scholar] [CrossRef] [PubMed]
- Vyncke, V.; Hardyns, W.; Peersman, W.; Pauwels, L.; Groenewegen, P.; Willems, S. How equal is the relationship between individual social capital and psychological distress? A gendered analysis using cross-sectional data from Ghent (Belgium). BMC Public Health 2014, 14, 960. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kawachi, I.; Kennedy, B.P.; Lochner, K.; Prothrow-Stith, D. Social capital, income inequality, and mortality. Am. J. Public Health 1997, 87, 1491–1498. [Google Scholar] [CrossRef] [PubMed]
- Sundquist, K.; Hamano, T.; Li, X.; Kawakami, N.; Shiwaku, K.; Sundquist, J. Linking social capital and mortality in the elderly: A Swedish national cohort study. Exp. Gerontol. 2014, 55, 29–36. [Google Scholar] [CrossRef] [PubMed]
- Blakely, T.; Atkinson, J.; Ivory, V.; Collings, S.; Wilton, J.; Howden-Chapman, P. No association of neighbourhood volunteerism with mortality in New Zealand: A national multilevel cohort study. Int. J. Epidemiol. 2006, 35, 981–989. [Google Scholar] [CrossRef] [PubMed]
- Nieminen, T.; Harkanen, T.; Martelin, T.; Borodulin, K.; Koskinen, S. Social capital and all-cause mortality among Finnish men and women aged 30–79. Eur. J. Public Health 2015, 25, 972–978. [Google Scholar] [CrossRef] [PubMed]
- Aida, J.; Kondo, K.; Kawachi, I.; Subramanian, S.V.; Ichida, Y.; Hirai, H.; Kondo, N.; Osaka, K.; Sheiham, A.; Tsakos, G.; et al. Does social capital affect the incidence of functional disability in older Japanese? A prospective population-based cohort study. J. Epidemiol. Community Health 2013, 67, 42–47. [Google Scholar] [CrossRef] [PubMed]
- Kanamori, S.; Kai, Y.; Aida, J.; Kondo, K.; Kawachi, I.; Hirai, H.; Shirai, K.; Ishikawa, Y.; Suzuki, K. Social participation and the prevention of functional disability in older Japanese: The jages cohort study. PLoS ONE 2014, 9, e99638. [Google Scholar] [CrossRef] [PubMed]
- Legh-Jones, H.; Moore, S. Network social capital, social participation, and physical inactivity in an urban adult population. Soc. Sci. Med. 2012, 74, 1362–1367. [Google Scholar] [CrossRef] [PubMed]
- Ueshima, K.; Fujiwara, T.; Takao, S.; Suzuki, E.; Iwase, T.; Doi, H.; Subramanian, S.V.; Kawachi, I. Does social capital promote physical activity? A population-based study in Japan. PLoS ONE 2010, 5, e12135. [Google Scholar] [CrossRef] [PubMed]
- Paterson, D.H.; Warburton, D.E. Physical activity and functional limitations in older adults: A systematic review related to Canada’s physical activity guidelines. Int. J. Behav. Nutr. Phys. Act. 2010, 7, 38. [Google Scholar] [CrossRef] [PubMed]
- Ellaway, A.; Macintyre, S. Is social participation associated with cardiovascular disease risk factors? Soc. Sci. Med. 2007, 64, 1384–1391. [Google Scholar] [CrossRef] [PubMed]
- Eriksson, M.; Ng, N. Changes in access to structural social capital and its influence on self-rated health over time for middle-aged men and women: A longitudinal study from northern Sweden. Soc. Sci. Med. 2015, 130, 250–258. [Google Scholar] [CrossRef] [PubMed]
- Kavanagh, A.M.; Bentley, R.; Turrell, G.; Broom, D.H.; Subramanian, S.V. Does gender modify associations between self rated health and the social and economic characteristics of local environments? J. Epidemiol. Community Health 2006, 60, 490–495. [Google Scholar] [CrossRef] [PubMed]
- Stafford, M.; Cummins, S.; Macintyre, S.; Ellaway, A.; Marmot, M. Gender differences in the associations between health and neighbourhood environment. Soc. Sci. Med. 2005, 60, 1681–1692. [Google Scholar] [CrossRef] [PubMed]
- Michikawa, T.; Nishiwaki, Y.; Asakura, K.; Hillebrand, G.; Miyamoto, K.; Ono, M.; Kinjo, Y.; Akiba, S.; Takebayashi, T. Sunlight exposure may be a risk factor of hearing impairment: A community-based study in Japanese older men and women. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2013, 68, 96–103. [Google Scholar] [CrossRef] [PubMed]
- Nishiwaki, Y.; Michikawa, T.; Eto, N.; Takebayashi, T. Body mass index misclassification due to kyphotic posture in Japanese community-dwelling adults aged 65 years and older. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2011, 66, 326–331. [Google Scholar] [CrossRef] [PubMed]
- Yamada, M.; Nishiwaki, Y.; Michikawa, T.; Takebayashi, T. Self-reported hearing loss in older adults is associated with future decline in instrumental Activities of Daily Living but not in social participation. J. Am. Geriatr. Soc. 2012, 60, 1304–1309. [Google Scholar] [CrossRef] [PubMed]
- Katz, S.; Akpom, C.A. A measure of primary sociobiological functions. Int. J. Health Serv. Plan. Adm. Eval. 1976, 6, 493–508. [Google Scholar] [CrossRef]
- Tsutsui, T.; Muramatsu, N. Care-needs certification in the long-term care insurance system of Japan. J. Am. Geriatr. Soc. 2005, 53, 522–527. [Google Scholar] [CrossRef] [PubMed]
- Cabinet Office of the Government of Japan. Social Capital: Looking for a Good Circle of Rich Human Relationships and Civic Activities; Government Printing Office: Tokyo, Japan, 2003. (In Japanese)
- Subramanian, S.; Hamano, T.; Komatsu, H.; Fujisawa, Y. Multilevel analysis and population strategy. J. Natl. Inst. Public Health 2007, 56, 83–89. (In Japanese) [Google Scholar]
- Koyano, W.; Nishimura, M.; Ando, T.; Asakawa, T.; Horita, Y. Social relationships of senior men living in an urban area. Jpn. J. Gerontol. 2000, 22, 83–88. (In Japanese) [Google Scholar]
- Sugisawa, A.; Sugisawa, H.; Nakatani, Y.; Shibata, H. Effect of retirement on mental health and social well-being among elderly Japanese. Jpn. J. Public Health 1997, 44, 123–130. (In Japanese) [Google Scholar]
- Norris, P.; Inglehart, R. Gendering social capital. Bowling in women’s leagues? In Gender and Social Capital; O’Neill, B., Gidengil, E., Eds.; Routledge: New York, NY, USA, 2006; pp. 73–98. [Google Scholar]
- Chuang, Y.C.; Chuang, K.Y. Gender differences in relationships between social capital and individual smoking and drinking behavior in Taiwan. Soc. Sci. Med. 2008, 67, 1321–1330. [Google Scholar] [CrossRef] [PubMed]
- Subramanian, S.V.; Lochner, K.A.; Kawachi, I. Neighborhood differences in social capital: A compositional artifact or a contextual construct? Health Place 2003, 9, 33–44. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | Total, n = 984 n (%) | Composite Outcome * | ||
|---|---|---|---|---|
| No, n = 774 n (%) | Yes, n = 210 n (%) | p-Value † | ||
| Sex | ||||
| women | 525 (53.4) | 403 (52.1) | 122 (58.1) | 0.12 |
| men | 459 (46.6) | 371 (47.9) | 88 (41.9) | |
| Age (years) | ||||
| 65–69 | 232 (23.6) | 217 (28.0) | 15 (7.1) | <0.001 |
| 70–74 | 227 (23.1) | 203 (26.2) | 24 (11.4) | |
| 75–79 | 243 (24.7) | 200 (25.8) | 43 (20.5) | |
| 80–84 | 152 (15.4) | 101 (13.0) | 51 (24.3) | |
| ≥85 | 130 (13.2) | 53 (6.8) | 77 (36.7) | |
| Marital status | ||||
| Married | 669 (68.0) | 554 (71.6) | 115 (54.8) | <0.001 |
| Widowed, divorced, single | 315 (32.0) | 220 (28.4) | 95 (45.2) | |
| Educational attainment (years) | ||||
| ≥10 | 316 (32.1) | 275 (35.5) | 41 (19.5) | <0.001 |
| <10 | 668 (67.9) | 499 (64.5) | 169 (80.5) | |
| Number of people living together | ||||
| ≥1 person | 853 (86.7) | 671 (86.7) | 182 (86.7) | 0.99 |
| None | 131 (13.3) | 103 (13.3) | 28 (13.3) | |
| Self-rated health | ||||
| Very good, good, normal | 905 (92.0) | 717 (92.6) | 188 (89.5) | 0.14 |
| Bad, very bad | 79 (8.0) | 57 (7.4) | 22 (10.5) | |
| Social participation | ||||
| Participate | 568 (57.7) | 487 (62.9) | 81 (38.6) | <0.001 |
| Not participate | 416 (42.3) | 287 (37.1) | 129 (61.4) | |
| Generalized trust | ||||
| Tend to trust | 408 (41.5) | 331 (42.8) | 77 (36.7) | 0.11 |
| Tend to be careful | 576 (58.5) | 443 (57.2) | 133 (63.3) | |
| Area | Mean Age of Eligible Population (Years) | Community Level Social Participation (%) * | Community Level Generalized Trust (%) † | Composite Outcome/Study Population for Main Analyses (%) | ||
|---|---|---|---|---|---|---|
| Total | Men | Women | ||||
| A | 76.4 | 76/170 (44.7) L | 54/179 (30.2) L | 20/123 (16.3) | 6/54 (11.1) | 14/69 (20.3) |
| B | 75.6 | 82/143 (57.3) H | 53/142 (37.3) L | 14/96 (14.6) | 8/49 (16.3) | 6/47 (12.8) |
| C | 76.3 | 79/117 (67.5) H | 48/115 (41.7) H | 16/91 (17.6) | 6/40 (15.0) | 10/51 (19.6) |
| D | 76.5 | 87/158 (55.1) H | 72/158 (45.6) H | 28/125 (22.4) | 14/62 (22.6) | 14/63 (22.2) |
| E | 77.3 | 79/164 (48.2) H | 55/163 (33.7) L | 21/111 (18.9) | 4/47 (8.5) | 17/64 (26.6) |
| F | 76.5 | 85/194 (43.8) L | 91/192 (47.4) H | 34/147 (23.1) | 13/70 (18.6) | 21/77 (27.3) |
| G | 78.6 | 109/239 (45.6) L | 97/243 (39.9) L | 41/170 (24.1) | 19/74 (25.7) | 22/96 (22.9) |
| H | 77.6 | 80/172 (46.5) L | 69/172 (40.1) H | 36/121 (29.8) | 18/63 (28.6) | 18/58 (31.0) |
| Total | 77.0 | 677/1357 (49.9) | 539/1364 (39.5) | 210/984 (21.3) | 88/459 (19.2) | 122/525 (23.2) |
| Social Capital | Model 1 * | Model 2 † | Model 3 ‡ | |||
|---|---|---|---|---|---|---|
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | OR (95% CI) | p-Value | |
| Total (n = 984) | ||||||
| Social participation | ||||||
| Community level § | ||||||
| High | 1.00 | 1.00 | 1.00 | |||
| Low | 1.34 (0.95–1.89) | 0.10 | 1.26 (0.88–1.78) | 0.20 | 1.25 (0.88–1.78) | 0.22 |
| Individual level | ||||||
| Participate | 1.00 | 1.00 | ||||
| Not participate | 2.08 (1.47–2.96) | < 0.001 | 1.97 (1.38–2.81) | < 0.001 | ||
| Generalized trust | ||||||
| Community level || | ||||||
| High | 1.00 | 1.00 | 1.00 | |||
| Low | 0.65 (0.47–0.92) | 0.01 | 0.62 (0.44–0.87) | 0.006 | 0.62 (0.43–0.87) | 0.007 |
| Individual level | ||||||
| Tend to trust | 1.00 | 1.00 | ||||
| Tend to be careful | 1.33 (0.94–1.89) | 0.11 | 1.31 (0.92–1.88) | 0.13 | ||
| Men (n = 459) | ||||||
| Social participation | ||||||
| Community level | ||||||
| High | 1.00 | 1.00 | 1.00 | |||
| Low | 1.38 (0.83–2.30) | 0.22 | 1.30 (0.76–2.21) | 0.34 | 1.30 (0.75–2.23) | 0.35 |
| Individual level | ||||||
| Participate | 1.00 | 1.00 | ||||
| Not participate | 2.40 (1.40–4.09) | 0.001 | 2.33 (1.36–4.00) | 0.002 | ||
| Generalized trust | ||||||
| Community level | ||||||
| High | 1.00 | 1.00 | 1.00 | |||
| Low | 0.65 (0.39–1.07) | 0.09 | 0.57 (0.33–0.98) | 0.04 | 0.55 (0.32–0.96) | 0.04 |
| Individual level | ||||||
| Tend to trust | 1.00 | 1.00 | ||||
| Tend to be careful | 2.16 (1.25–3.74) | 0.006 | 2.22 (1.27–3.90) | 0.005 | ||
| Women (n = 525) | ||||||
| Social participation | ||||||
| Community level | ||||||
| High | 1.00 | 1.00 | 1.00 | |||
| Low | 1.31 (0.82–2.09) | 0.26 | 1.22 (0.76–1.96) | 0.41 | 1.23 (0.76–1.99) | 0.40 |
| Individual level | ||||||
| Participate | 1.00 | 1.00 | ||||
| Not participate | 1.87 (1.16–3.02) | 0.01 | 1.72 (1.05–2.81) | 0.03 | ||
| Generalized trust | ||||||
| Community level | ||||||
| High | 1.00 | 1.00 | 1.00 | |||
| Low | 0.66 (0.41–1.04) | 0.08 | 0.64 (0.40–1.02) | 0.06 | 0.63 (0.39–1.01) | 0.06 |
| Individual level | ||||||
| Tend to trust | 1.00 | 1.00 | ||||
| Tend to be careful | 0.93 (0.58–1.49) | 0.76 | 0.92 (0.57–1.49) | 0.75 | ||
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Imamura, H.; Hamano, T.; Michikawa, T.; Takeda-Imai, F.; Nakamura, T.; Takebayashi, T.; Nishiwaki, Y. Relationships of Community and Individual Level Social Capital with Activities of Daily Living and Death by Gender. Int. J. Environ. Res. Public Health 2016, 13, 860. https://doi.org/10.3390/ijerph13090860
Imamura H, Hamano T, Michikawa T, Takeda-Imai F, Nakamura T, Takebayashi T, Nishiwaki Y. Relationships of Community and Individual Level Social Capital with Activities of Daily Living and Death by Gender. International Journal of Environmental Research and Public Health. 2016; 13(9):860. https://doi.org/10.3390/ijerph13090860
Chicago/Turabian StyleImamura, Haruhiko, Tsuyoshi Hamano, Takehiro Michikawa, Fujimi Takeda-Imai, Takahiro Nakamura, Toru Takebayashi, and Yuji Nishiwaki. 2016. "Relationships of Community and Individual Level Social Capital with Activities of Daily Living and Death by Gender" International Journal of Environmental Research and Public Health 13, no. 9: 860. https://doi.org/10.3390/ijerph13090860