
Residential Proximity to Major Roadways and Risk of Type 2 Diabetes Mellitus: A Meta-Analysis

Abstract
:1. Introduction
2. Materials and Methods
2.1. Literature Search and Inclusion Criteria
2.2. Data Extraction and Quality Assessment
2.3. Statistical Analysis
3. Results
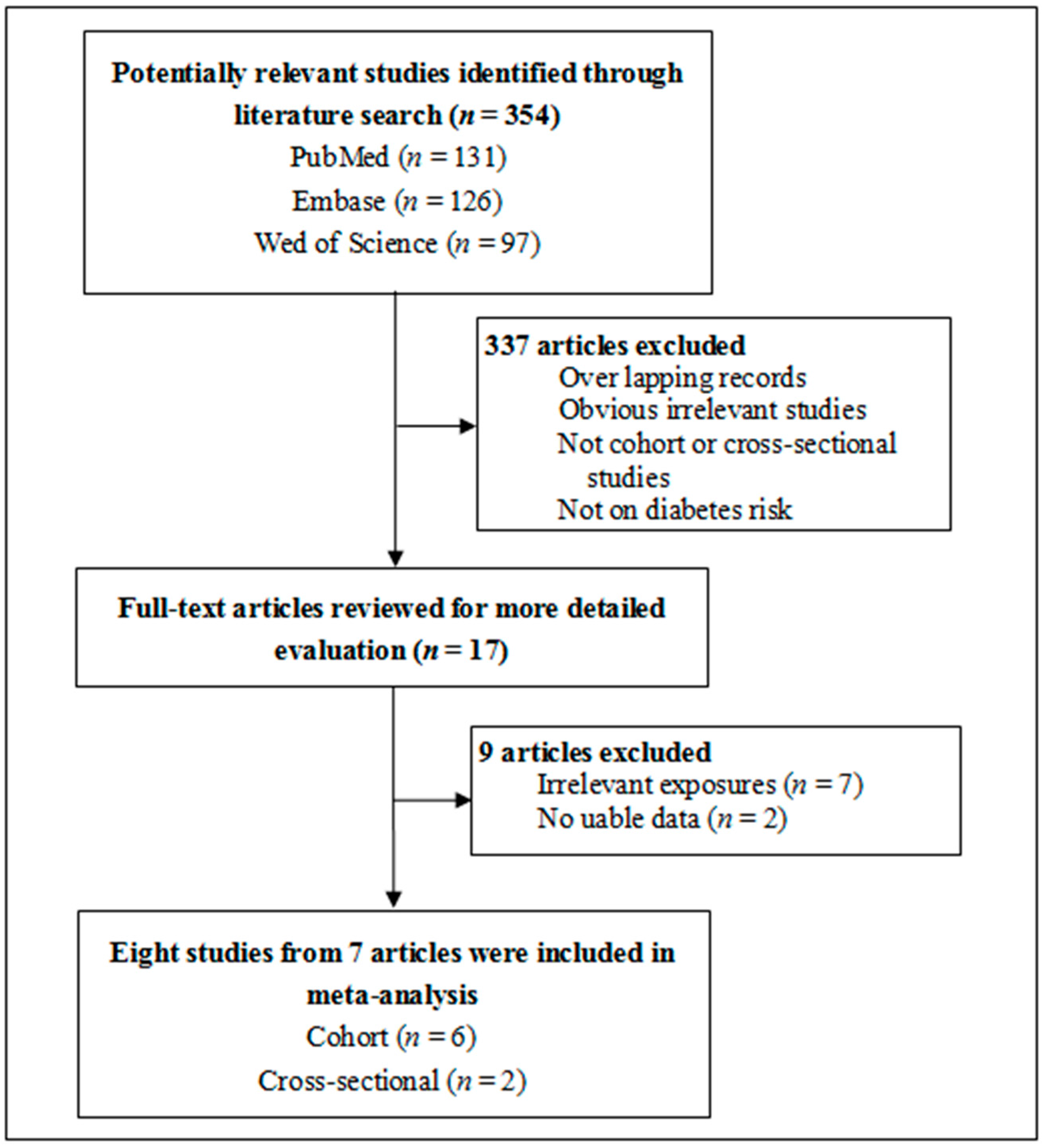
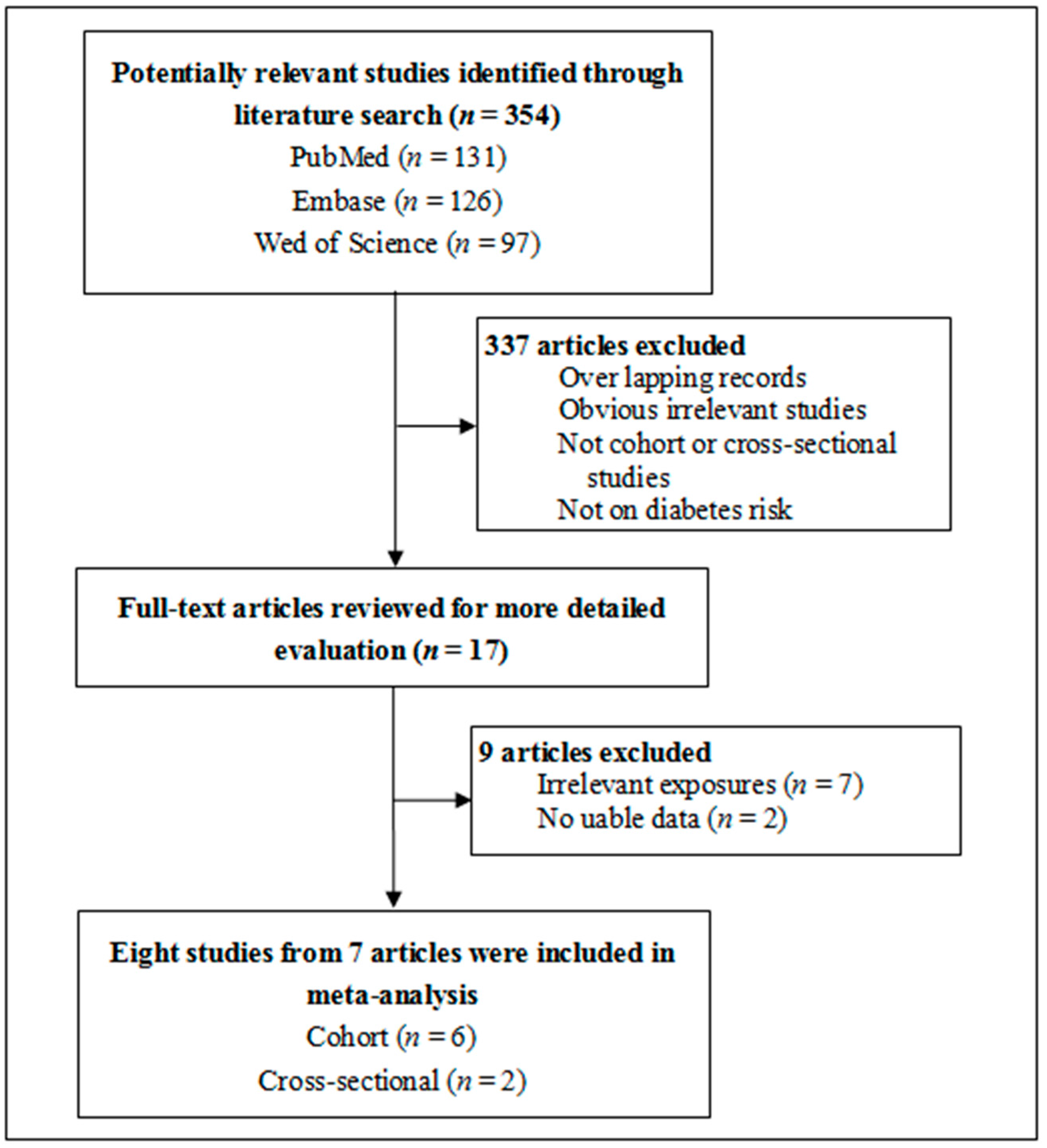
3.1. Study Selection and Characteristics
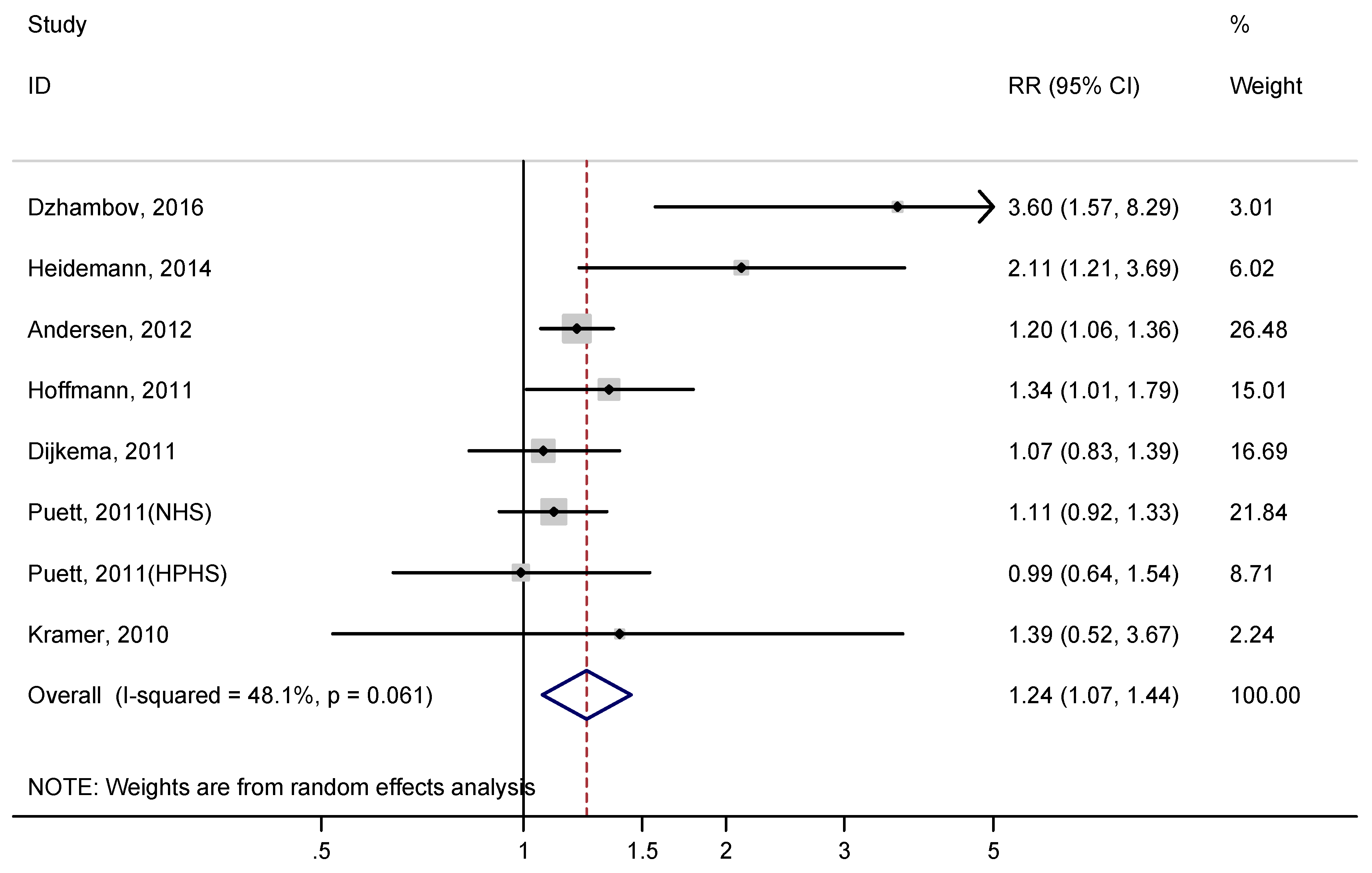
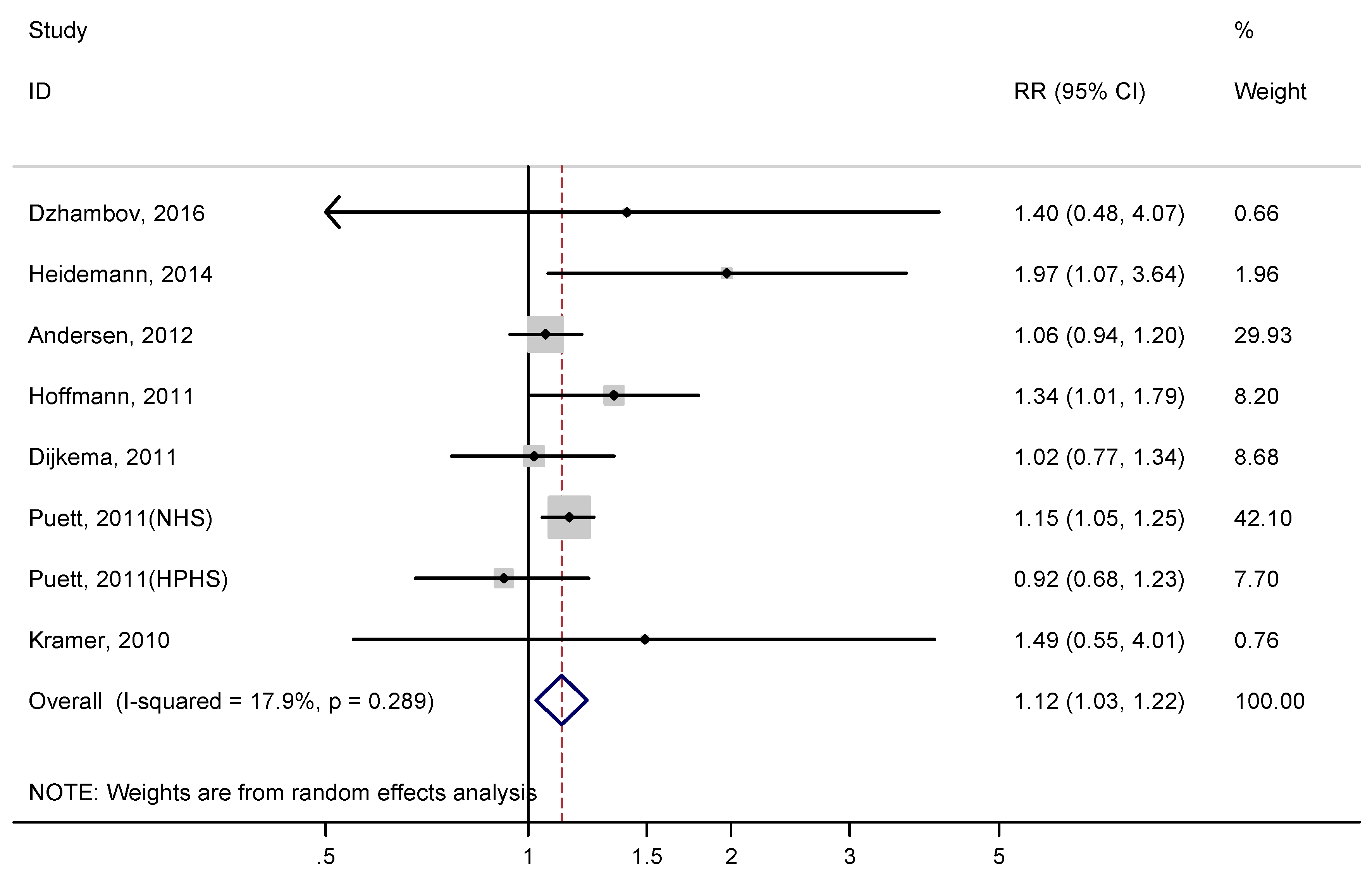
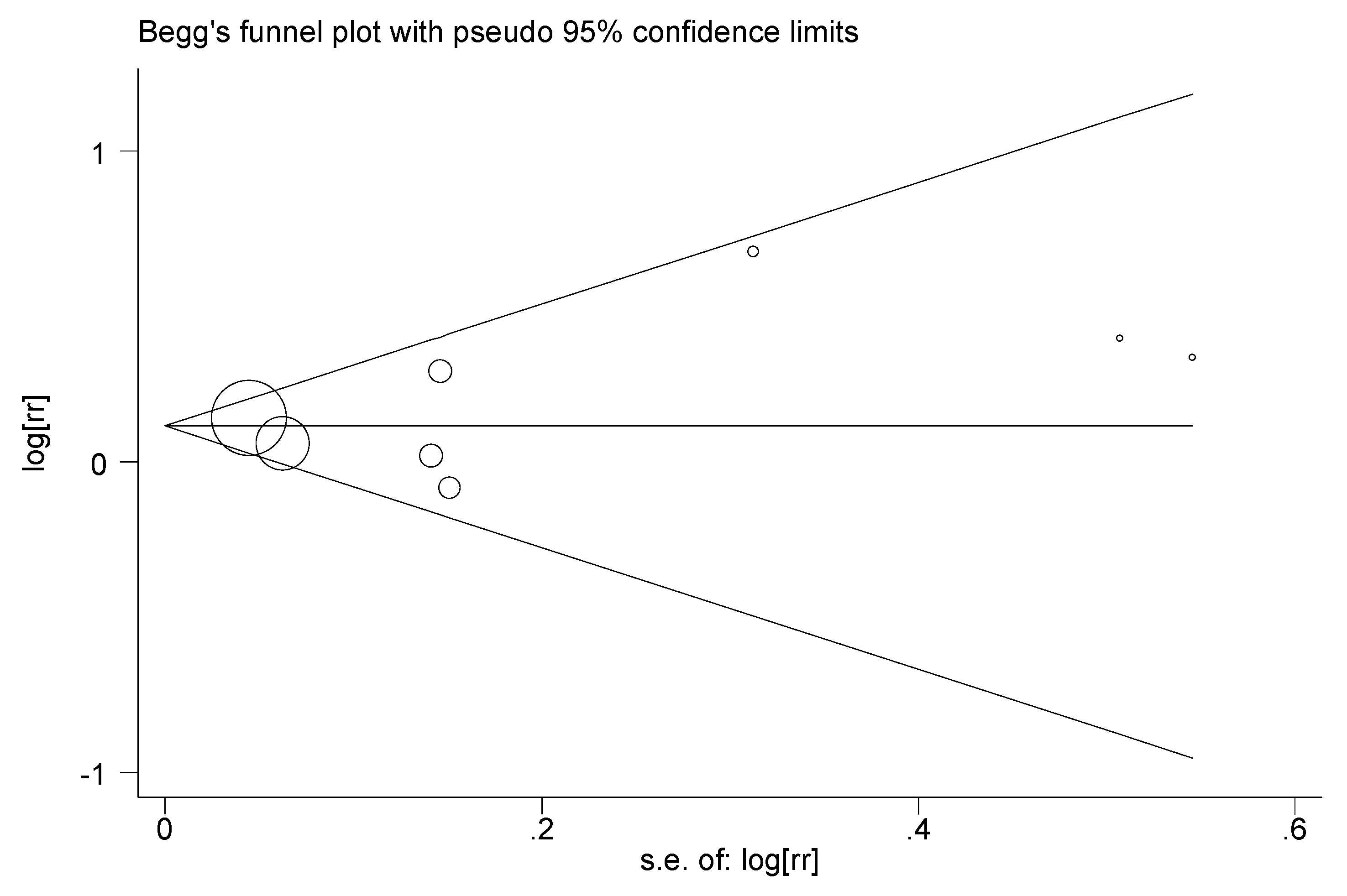
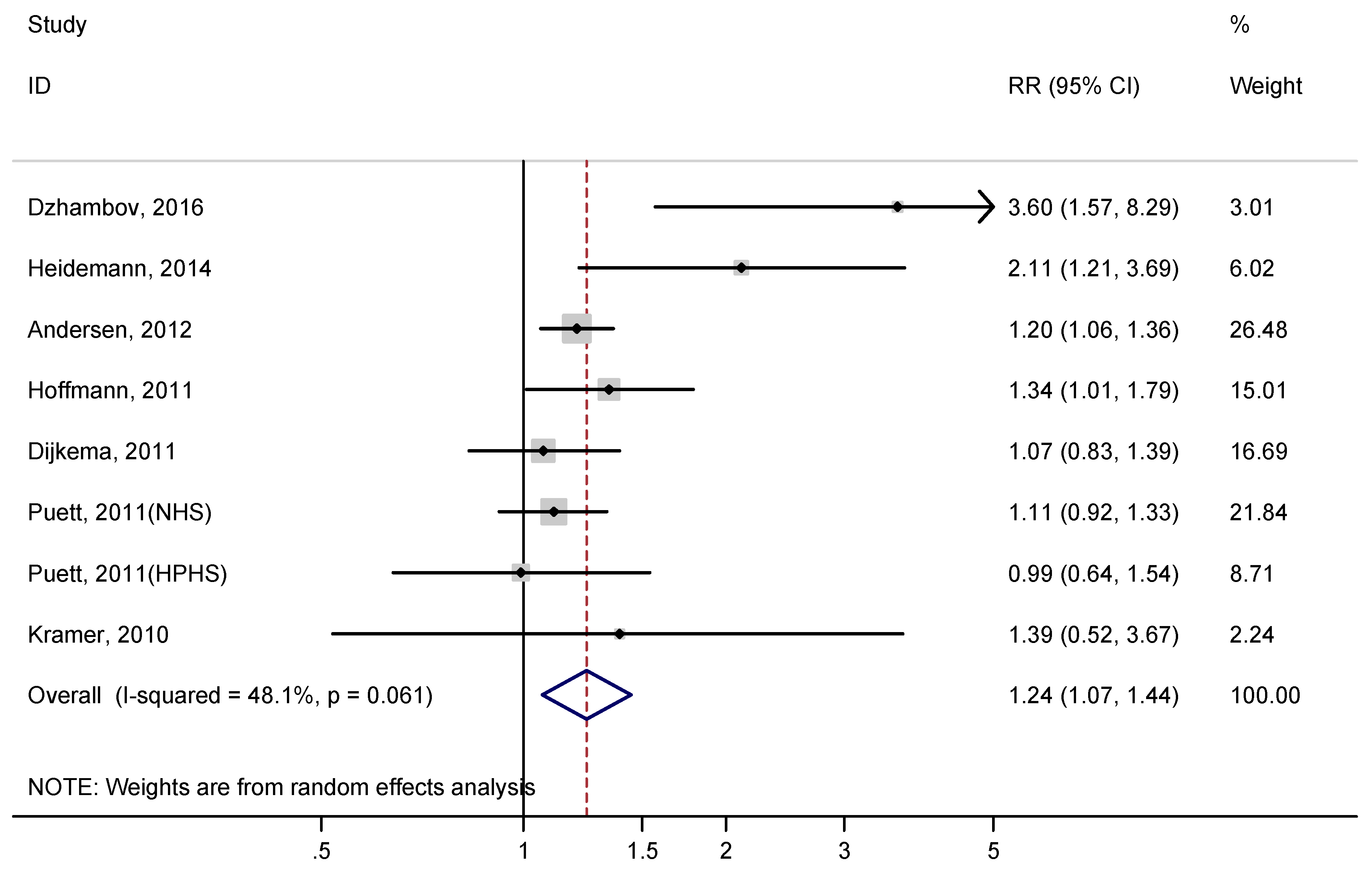
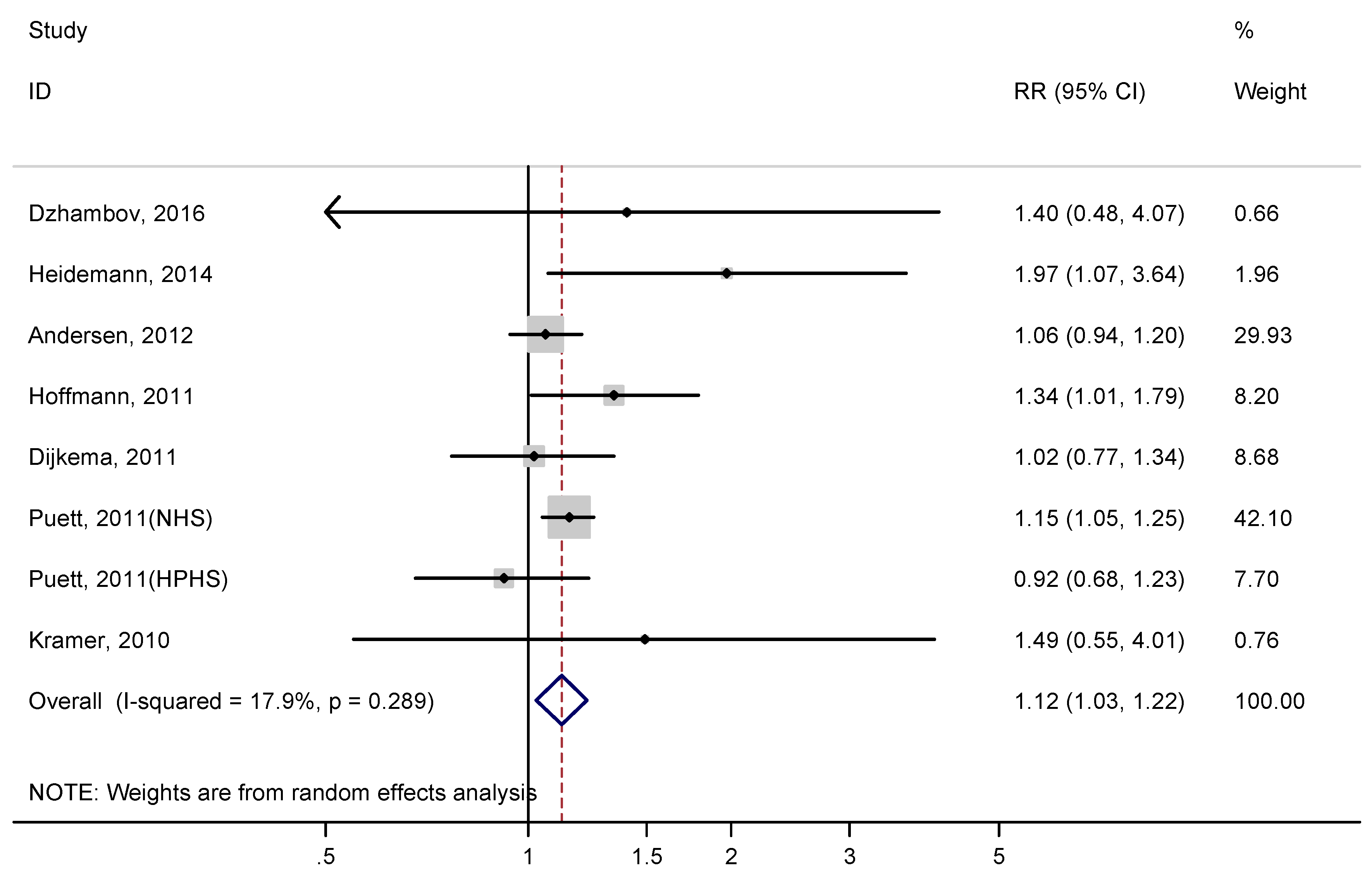
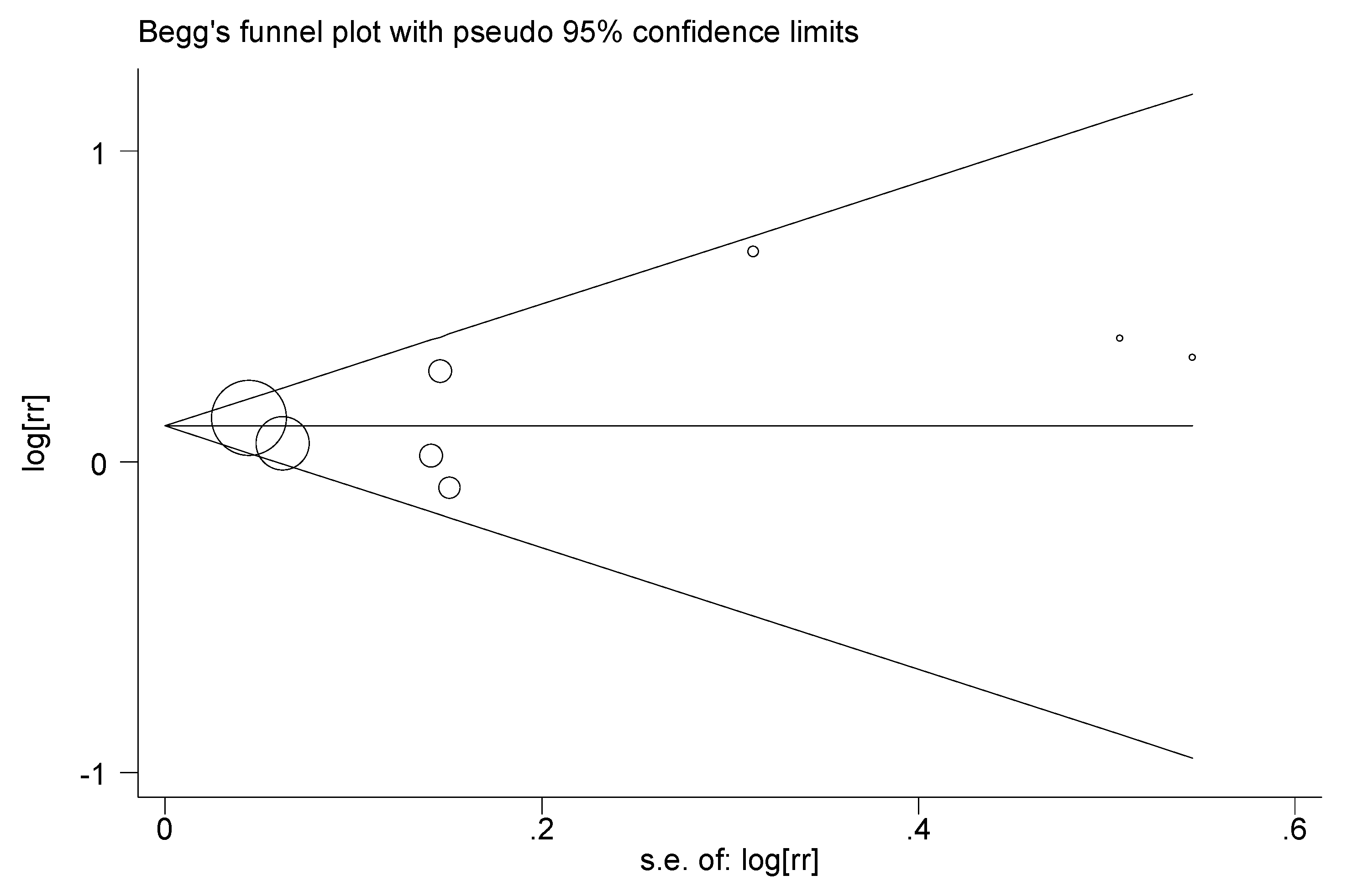
3.2. Meta-Analysis
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Polonsky, K.S. The past 200 years in diabetes. N. Engl. J. Med. 2012, 367, 1332–1340. [Google Scholar] [CrossRef] [PubMed]
- Van Crevel, R.; van de Vijver, S.; Moore, D.A. The global diabetes epidemic: What does it mean for infectious diseases in tropical countries? Lancet Diabetes Endocrinol. 2016. [Google Scholar] [CrossRef]
- Ley, S.H.; Hamdy, O.; Mohan, V.; Hu, F.B. Prevention and management of type 2 diabetes: Dietary components and nutritional strategies. Lancet 2014, 383, 1999–2007. [Google Scholar] [CrossRef]
- Garcia-Jimenez, C.; Gutierrez-Salmeron, M.; Chocarro-Calvo, A.; Garcia-Martinez, J.M.; Castano, A.; De la Vieja, A. From obesity to diabetes and cancer: Epidemiological links and role of therapies. Br. J. Cancer 2016, 114, 716–722. [Google Scholar] [CrossRef] [PubMed]
- Tsilidis, K.K.; Kasimis, J.C.; Lopez, D.S.; Ntzani, E.E.; Ioannidis, J.P. Type 2 diabetes and cancer: Umbrella review of meta-analyses of observational studies. BMJ 2015, 350, g7607. [Google Scholar] [CrossRef] [PubMed]
- Mozaffarian, D. Dietary and Policy Priorities for Cardiovascular Disease, Diabetes, and Obesity: A Comprehensive Review. Circulation 2016, 133, 187–225. [Google Scholar] [CrossRef] [PubMed]
- Verma, S.; Hussain, M.E. Obesity and diabetes: An update. Diabetes Metab. Syndr. 2016. [Google Scholar] [CrossRef] [PubMed]
- Spijkerman, A.M.; van Der, A.D.; Nilsson, P.M.; Ardanaz, E.; Gavrila, D.; Agudo, A.; Arriola, L.; Balkau, B.; Beulens, J.W.; Boeing, H.; et al. Smoking and long-term risk of type 2 diabetes: The EPIC-InterAct study in European populations. Diabetes Care 2014, 37, 3164–3171. [Google Scholar] [PubMed]
- Hoffmann, B.; Hertel, S.; Moebus, S.; Viehmann, A.; Nonnemacher, M.; Jakobs, H.; Mohlenkamp, S.; Erbel, R.; Jockel, K.H. Urban air pollution and incidence of diabetes mellitus. J. Respir. Crit. Care Med. 2011, 183. [Google Scholar] [CrossRef]
- Dijkema, M.B.; Mallant, S.F.; Gehring, U.; van den Hurk, K.; Alssema, M.; van Strien, R.T.; Fischer, P.H.; Nijpels, G.; Stehouwer, C.D.; Hoek, G.; et al. Long-term exposure to traffic-related air pollution and type 2 diabetes prevalence in a cross-sectional screening-study in The Netherlands. Environ. Health 2011, 10, 76. [Google Scholar] [CrossRef] [PubMed]
- Puett, R.C.; Hart, J.E.; Schwartz, J.; Hu, F.B.; Liese, A.D.; Laden, F. Are particulate matter exposures associated with risk of type 2 diabetes? Environ. Health Perspect. 2011, 119, 384–389. [Google Scholar] [CrossRef] [PubMed]
- Andersen, Z.J.; Raaschou-Nielsen, O.; Ketzel, M.; Jensen, S.S.; Hvidberg, M.; Loft, S.; Tjonneland, A.; Overvad, K.; Sorensen, M. Diabetes incidence and long-term exposure to air pollution: A cohort study. Diabetes Care 2012, 35, 92–98. [Google Scholar] [CrossRef] [PubMed]
- Dzhambov, A.M.; Dimitrova, D.D. Exposures to road traffic, noise, and air pollution as risk factors for type 2 diabetes: A feasibility study in Bulgaria. Noise Health 2016, 18, 133–142. [Google Scholar] [CrossRef] [PubMed]
- Weinmayr, G.; Hennig, F.; Fuks, K.; Nonnemacher, M.; Jakobs, H.; Mohlenkamp, S.; Erbel, R.; Jockel, K.H.; Hoffmann, B.; Moebus, S. Long-term exposure to fine particulate matter and incidence of type 2 diabetes mellitus in a cohort study: Effects of total and traffic-specific air pollution. Environ. Health 2015, 14, 53. [Google Scholar] [CrossRef] [PubMed]
- Coogan, P.F.; White, L.F.; Yu, J.; Burnett, R.T.; Marshall, J.D.; Seto, E.; Brook, R.D.; Palmer, J.R.; Rosenberg, L.; Jerrett, M. Long term exposure to NO2 and diabetes incidence in the Black Women’s Health Study. Environ. Res. 2016, 148, 360–366. [Google Scholar] [CrossRef] [PubMed]
- Batterman, S.; Ganguly, R.; Harbin, P. High resolution spatial and temporal mapping of traffic-related air pollutants. Int. J. Environ. Res. Public Health 2015, 12, 3646–3666. [Google Scholar] [CrossRef] [PubMed]
- Hart, J.E.; Chiuve, S.E.; Laden, F.; Albert, C.M. Roadway proximity and risk of sudden cardiac death in women. Circulation 2014, 130, 1474–1482. [Google Scholar] [CrossRef] [PubMed]
- Kramer, U.; Herder, C.; Sugiri, D.; Strassburger, K.; Schikowski, T.; Ranft, U.; Rathmann, W. Traffic-related air pollution and incident type 2 diabetes: Results from the SALIA cohort study. Environ. Health Perspect. 2010, 118, 1273–1279. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heidemann, C.; Niemann, H.; Paprott, R.; Du, Y.; Rathmann, W.; Scheidt-Nave, C. Residential traffic and incidence of type 2 diabetes: The German Health Interview and Examination Surveys. Diabet. Med. 2014, 31, 1269–1276. [Google Scholar] [CrossRef] [PubMed]
- Wells, G.; Shea, B.; O’connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses; Ottawa Health Research Institute Web Site: Ottawa, ON, USA, 2015. [Google Scholar]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G.; Spiegelhalter, D.J. A re-evaluation of random-effects meta-analysis. J. R. Stat. Soc. Ser. A Stat. Soc. 2009, 172, 137–159. [Google Scholar] [CrossRef] [PubMed]
- Ades, A.E.; Lu, G.; Higgins, J.P. The interpretation of random-effects meta-analysis in decision models. Med. Decis. Mak. 2005, 25, 646–654. [Google Scholar] [CrossRef] [PubMed]
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed]
- Underhill, L.; Bose, S.; Williams, D.; Romero, K.; Malpartida, G.; Breysse, P.; Klasen, E.; Combe, J.; Checkley, W.; Hansel, N. Association of Roadway Proximity with Indoor Air Pollution in a Peri-Urban Community in Lima, Peru. Int. J. Environ. Res. Public Health 2015, 12, 13466–13481. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.J.; Smorodinsky, S.; Lipsett, M.; Singer, B.C.; Hodgson, A.T.; Ostro, B. Traffic-related air pollution near busy roads: The East Bay Children’s Respiratory Health Study. Am. J. Respir. Crit. Care Med. 2004, 170, 520–526. [Google Scholar] [CrossRef] [PubMed]
- Levy, J.I.; Houseman, E.A.; Spengler, J.D.; Loh, P.; Ryan, L. Fine particulate matter and polycyclic aromatic hydrocarbon concentration patterns in Roxbury, Massachusetts: A community-based GIS analysis. Environ. Health Perspect. 2001, 109, 341–347. [Google Scholar] [CrossRef] [PubMed]
- Thiering, E.; Cyrys, J.; Kratzsch, J.; Meisinger, C.; Hoffmann, B.; Berdel, D.; von Berg, A.; Koletzko, S.; Bauer, C.P.; Heinrich, J. Long-term exposure to traffic-related air pollution and insulin resistance in children: Results from the GINIplus and LISAplus birth cohorts. Diabetologia 2013, 56, 1696–1704. [Google Scholar] [CrossRef] [PubMed]
- Rajagopalan, S.; Brook, R.D. Air pollution and type 2 diabetes: Mechanistic insights. Diabetes 2012, 61, 3037–3045. [Google Scholar] [CrossRef] [PubMed]
- Raaschou-Nielsen, O.; Sorensen, M.; Ketzel, M.; Hertel, O.; Loft, S.; Tjonneland, A.; Overvad, K.; Andersen, Z.J. Long-term exposure to traffic-related air pollution and diabetes-associated mortality: A cohort study. Diabetologia 2013, 56, 36–46. [Google Scholar] [CrossRef] [PubMed]
- Coogan, P.F.; White, L.F.; Jerrett, M.; Brook, R.D.; Su, J.G.; Seto, E.; Burnett, R.; Palmer, J.R.; Rosenberg, L. Air pollution and incidence of hypertension and diabetes mellitus in black women living in Los Angeles. Circulation 2012, 125, 767–772. [Google Scholar] [CrossRef] [PubMed]
- Rioux, C.L.; Tucker, K.L.; Brugge, D.; Gute, D.M.; Mwamburi, M. Traffic exposure in a population with high prevalence type 2 diabetes—Do medications influence concentrations of C-reactive protein? Environ. Pollut. 2011, 159, 2051–2060. [Google Scholar] [CrossRef] [PubMed]
- Mirowsky, J.E.; Peltier, R.E.; Lippmann, M.; Thurston, G.; Chen, L.C.; Neas, L.; Diaz-Sanchez, D.; Laumbach, R.; Carter, J.D.; Gordon, T. Repeated measures of inflammation, blood pressure, and heart rate variability associated with traffic exposures in healthy adults. Environ. Health 2015, 14, 66. [Google Scholar] [CrossRef] [PubMed]
- Siponen, T.; Yli-Tuomi, T.; Aurela, M.; Dufva, H.; Hillamo, R.; Hirvonen, M.R.; Huttunen, K.; Pekkanen, J.; Pennanen, A.; Salonen, I.; et al. Source-specific fine particulate air pollution and systemic inflammation in ischaemic heart disease patients. Occup. Environ. Med. 2015, 72, 277–283. [Google Scholar] [CrossRef] [PubMed]
- Neophytou, A.M.; Hart, J.E.; Cavallari, J.M.; Smith, T.J.; Dockery, D.W.; Coull, B.A.; Garshick, E.; Laden, F. Traffic-related exposures and biomarkers of systemic inflammation, endothelial activation and oxidative stress: A panel study in the US trucking industry. Environ. Health 2013, 12, 105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Donath, M.Y. Targeting inflammation in the treatment of type 2 diabetes: Time to start. Nat. Rev. Drug Discov. 2014, 13, 465–476. [Google Scholar] [CrossRef] [PubMed]
- Esser, N.; Legrand-Poels, S.; Piette, J.; Scheen, A.J.; Paquot, N. Inflammation as a link between obesity, metabolic syndrome and type 2 diabetes. Diabetes Res. Clin. Pract. 2014, 105, 141–150. [Google Scholar] [CrossRef] [PubMed]
- Sorensen, M.; Andersen, Z.J.; Nordsborg, R.B.; Becker, T.; Tjonneland, A.; Overvad, K.; Raaschou-Nielsen, O. Long-term exposure to road traffic noise and incident diabetes: A cohort study. Environ. Health Perspect. 2013, 121, 217–222. [Google Scholar] [PubMed]
- Li, W.; Dorans, K.; Wilker, E.; Rice, M.; Schwartz, J.; Coull, B.; Koutrakis, P.; Gold, D.; Fox, C.; Mittleman, M. Residential proximity to major roadways, fine particulate matter, and adiposity: The framingham heart study. Obesity 2016, 24, 2593–2599. [Google Scholar] [CrossRef] [PubMed]
- Yorifuji, T.; Naruse, H.; Kashima, S.; Takao, S.; Murakoshi, T.; Doi, H.; Kawachi, I. Residential proximity to major roads and adverse birth outcomes: A hospital-based study. Environ. Health 2013, 12, 34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DeJarnett, N.; Yeager, R.; Conklin, D.J.; Lee, J.; O’Toole, T.E.; McCracken, J.; Abplanalp, W.; Srivastava, S.; Riggs, D.W.; Hamzeh, I.; et al. Residential Proximity to Major Roadways Is Associated With Increased Levels of AC133+ Circulating Angiogenic Cells. Arterioscler. Thromb. Vasc. Biol. 2015, 35, 2468–2477. [Google Scholar] [CrossRef] [PubMed]
- Yorifuji, T.; Naruse, H.; Kashima, S.; Murakoshi, T.; Doi, H. Residential proximity to major roads and obstetrical complications. Sci. Total Environ. 2015, 508, 188–192. [Google Scholar] [CrossRef] [PubMed]
- Dorans, K.S.; Wilker, E.H.; Li, W.; Rice, M.B.; Ljungman, P.L.; Schwartz, J.; Coull, B.A.; Kloog, I.; Koutrakis, P.; D’Agostino, R.B., Sr.; et al. Residential Proximity to Major Roads, Exposure to Fine Particulate Matter, and Coronary Artery Calcium: The Framingham Heart Study. Arterioscler. Thromb. Vasc. Biol. 2016, 36, 1679–1685. [Google Scholar] [CrossRef] [PubMed]
- Weaver, A.M.; Wellenius, G.A.; Wu, W.C.; Hickson, D.A.; Kamalesh, M.; Wang, Y. Residential Proximity to Major Roadways Is Not Associated with Cardiac Function in African Americans: Results from the Jackson Heart Study. Int. J. Environ. Res. Public Health 2016, 13, 581. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bidoli, E.; Pappagallo, M.; Birri, S.; Frova, L.; Zanier, L.; Serraino, D. Residential Proximity to Major Roadways and Lung Cancer Mortality. Italy, 1990–2010: An Observational Study. Int. J. Environ. Res. Public Health 2016, 13, 191. [Google Scholar] [CrossRef] [PubMed]
- Houot, J.; Marquant, F.; Goujon, S.; Faure, L.; Honore, C.; Roth, M.H.; Hemon, D.; Clavel, J. Residential Proximity to Heavy-Traffic Roads, Benzene Exposure, and Childhood Leukemia-The GEOCAP Study, 2002–2007. Am. J. Epidemiol. 2015, 182, 685–693. [Google Scholar] [CrossRef] [PubMed]
- Kingsley, S.L.; Eliot, M.N.; Whitsel, E.A.; Wang, Y.; Coull, B.A.; Hou, L.; Margolis, H.G.; Margolis, K.L.; Mu, L.; Wu, W.C.; et al. Residential proximity to major roadways and incident hypertension in post-menopausal women. Environ. Res. 2015, 142, 522–528. [Google Scholar] [CrossRef] [PubMed]
- Kirwa, K.; Eliot, M.N.; Wang, Y.; Adams, M.A.; Morgan, C.G.; Kerr, J.; Norman, G.J.; Eaton, C.B.; Allison, M.A.; Wellenius, G.A. Residential proximity to major roadways and prevalent hypertension among postmenopausal women: Results from the Women’s Health Initiative San Diego Cohort. J. Am. Heart Assoc. 2014, 3, e000727. [Google Scholar] [CrossRef] [PubMed]
- Giles-Corti, B.; Vernez-Moudon, A.; Reis, R.; Turrell, G.; Dannenberg, A.L.; Badland, H.; Foster, S.; Lowe, M.; Sallis, J.F.; Stevenson, M.; et al. City planning and population health: A global challenge. Lancet 2016. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Baseline Study Dates | Country | Study Design | Follow-Up Time | Participants | Number of Events | Residential Distance to Major Roadways | Definitions of Major Roadways or High Traffic Intensity | Adjustment Factors | Quality * |
|---|---|---|---|---|---|---|---|---|---|---|
| Dzhambov, 2016 [13] | 2014 | Bulgaria | Cross-sectional | NA | 513 | 35 | Home located near to roads with high traffic intensity | Extreme traffic intensity reported by participants. | Sex, age, socioeconomic classes, occupations, dietary habits, alcohol consumption, PM2.5, loud noise, and smoking. | B |
| Heidemann, 2014 [19] | 1997–1998 | Germany | Cohort | 12.1 years | 3604 | 252 | Home located near to roads with high traffic intensity | Extremely busy traffic reported by participants. | Sex, age, smoking, heating of house, educational status, BMI, waist circumference, sport activity, and parental history of diabetes. | A |
| Andersen, 2012 [12] | 1993–1997 | Denmark | Cohort | 9.7 years | 51,818 | 2877 | <50 m from major roadways | A road with at least 10,000 vehicles/day which was determined by the residential address and the public traffic data. | Adjusted for sex, hypertension, hypercholesterolemia, myocardial infarction, BMI, waist-to-hip ratio, smoking status, smoking duration, smoking intensity, environmental tobacco smoke, educational level, physical/sports activity in leisure time, alcohol consumption, fruit consumption, fat consumption, and calendar year. | A |
| Hoffmann, 2011 | 2000–2003 | Germany | Cohort | 5 years | 3398 | 309 | <100 m from major roadways | A road with busy traffic but how it was defined in details was unclear. | Adjusted for sex, age, body mass index, education, smoking, physical activity, and city of residence. | B |
| Dijkema, 2011 [10] | 1998–2000 | Netherlands | Cross-sectional | NA | 8018 | 213 | <100 m from major roadways | A road with at least 5000 vehicles/day which was determined by the residential address and the traffic data from Geographical Information System. | Adjusted for average monthly income, age (continuous) and gender. | B |
| Puett, 2011 NHS [11] | 1989 | USA | Cohort | 13 years | 74,412 | 3784 | <100 m from major roadways | Major roadways, such as interstates highways and major noninterstate roads which was determined by the residential addresses and the public traffic data. | Adjusted for age, season, calendar year, state of residence, time-varying cigarette smoking (status and pack-years), time-varying hypertension, baseline BMI, time-varying alcohol intake, baseline physical activity, and time-varying diet. | A |
| Puett, 2011 HPHS [11] | 1989 | USA | Cohort | 13 years | 15,048 | 688 | <100 m from major roadways | Major roadways, such as interstates highways and major noninterstate roads which was determined by the residential addresses and the public traffic data. | Adjusted for age, season, calendar year, state of residence, time-varying cigarette smoking (status and pack-years), time-varying hypertension, baseline BMI, time-varying alcohol intake, baseline physical activity, and time-varying diet. | A |
| Kramer, 2010 [18] | 1985–1994 | Germany | Cohort | 16 years | 1775 | 187 | <100 m from major roadways | A road with more than 10,000 cars/day which was determined by the residential addresses and data on road traffic from environmental agency. | Adjusted for age, BMI, heating with fossil fuels, workplace exposure with dust/fumes, extreme temperatures, smoking, and education. | A |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhao, Z.; Lin, F.; Wang, B.; Cao, Y.; Hou, X.; Wang, Y. Residential Proximity to Major Roadways and Risk of Type 2 Diabetes Mellitus: A Meta-Analysis. Int. J. Environ. Res. Public Health 2017, 14, 3. https://doi.org/10.3390/ijerph14010003
Zhao Z, Lin F, Wang B, Cao Y, Hou X, Wang Y. Residential Proximity to Major Roadways and Risk of Type 2 Diabetes Mellitus: A Meta-Analysis. International Journal of Environmental Research and Public Health. 2017; 14(1):3. https://doi.org/10.3390/ijerph14010003
Chicago/Turabian StyleZhao, Zhiqing, Faying Lin, Bennett Wang, Yihai Cao, Xu Hou, and Yangang Wang. 2017. "Residential Proximity to Major Roadways and Risk of Type 2 Diabetes Mellitus: A Meta-Analysis" International Journal of Environmental Research and Public Health 14, no. 1: 3. https://doi.org/10.3390/ijerph14010003