Maternal Exposure to Air Pollutants and Risk of Gestational Diabetes Mellitus in Taiwan


Abstract
:1. Introduction
2. Materials and Methods
2.1. Research Data
2.2. Study Design and Participants
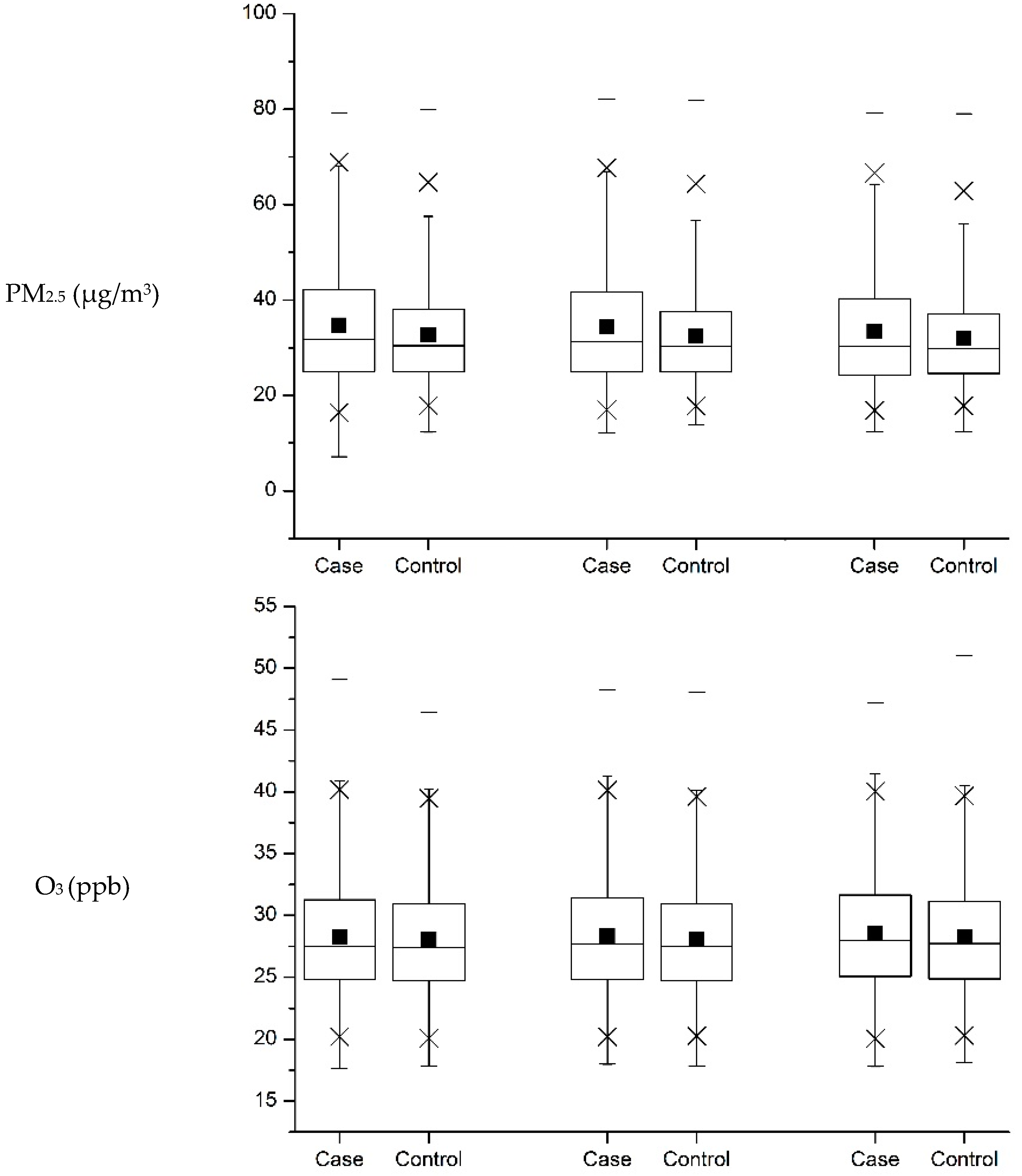
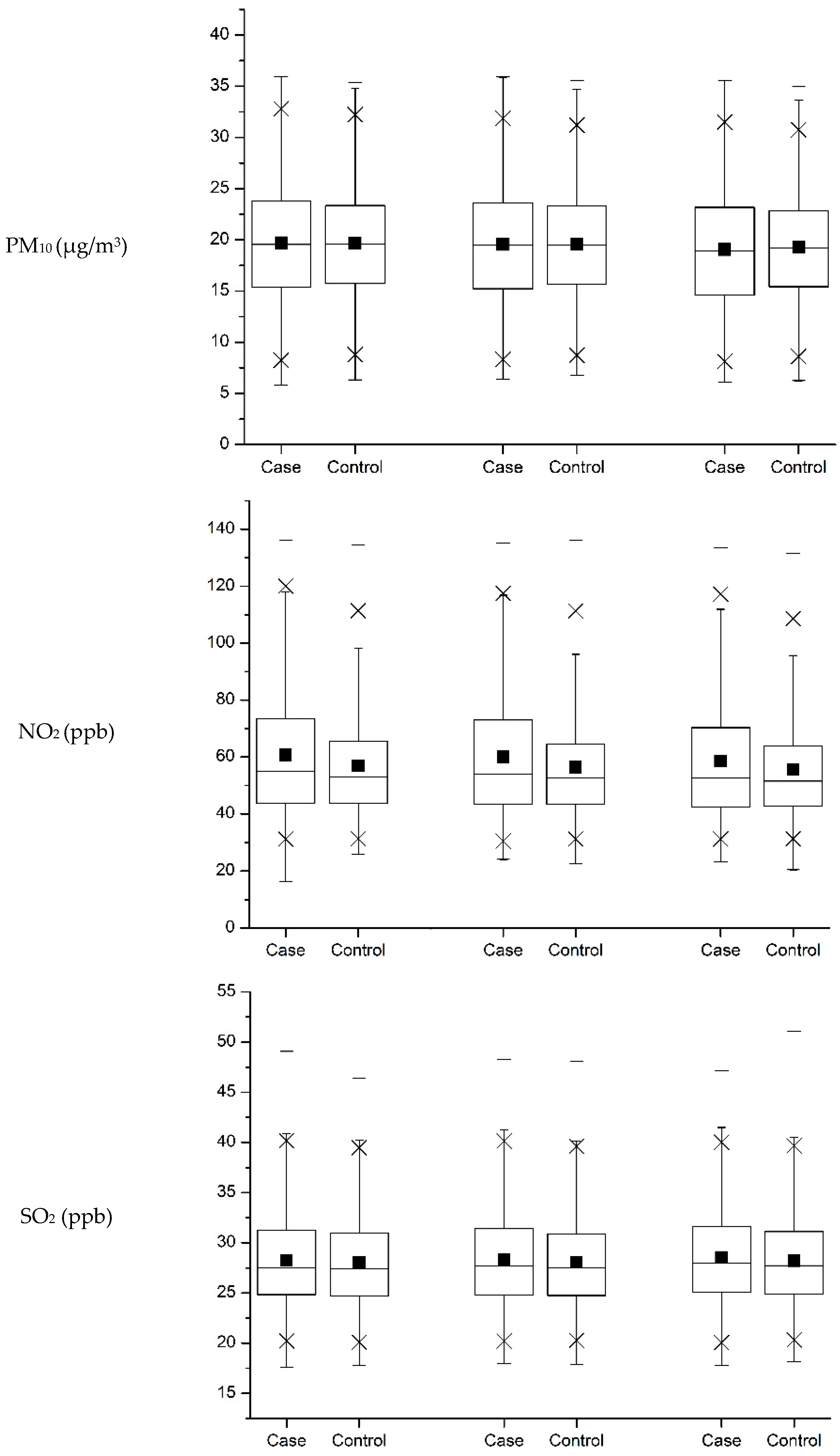
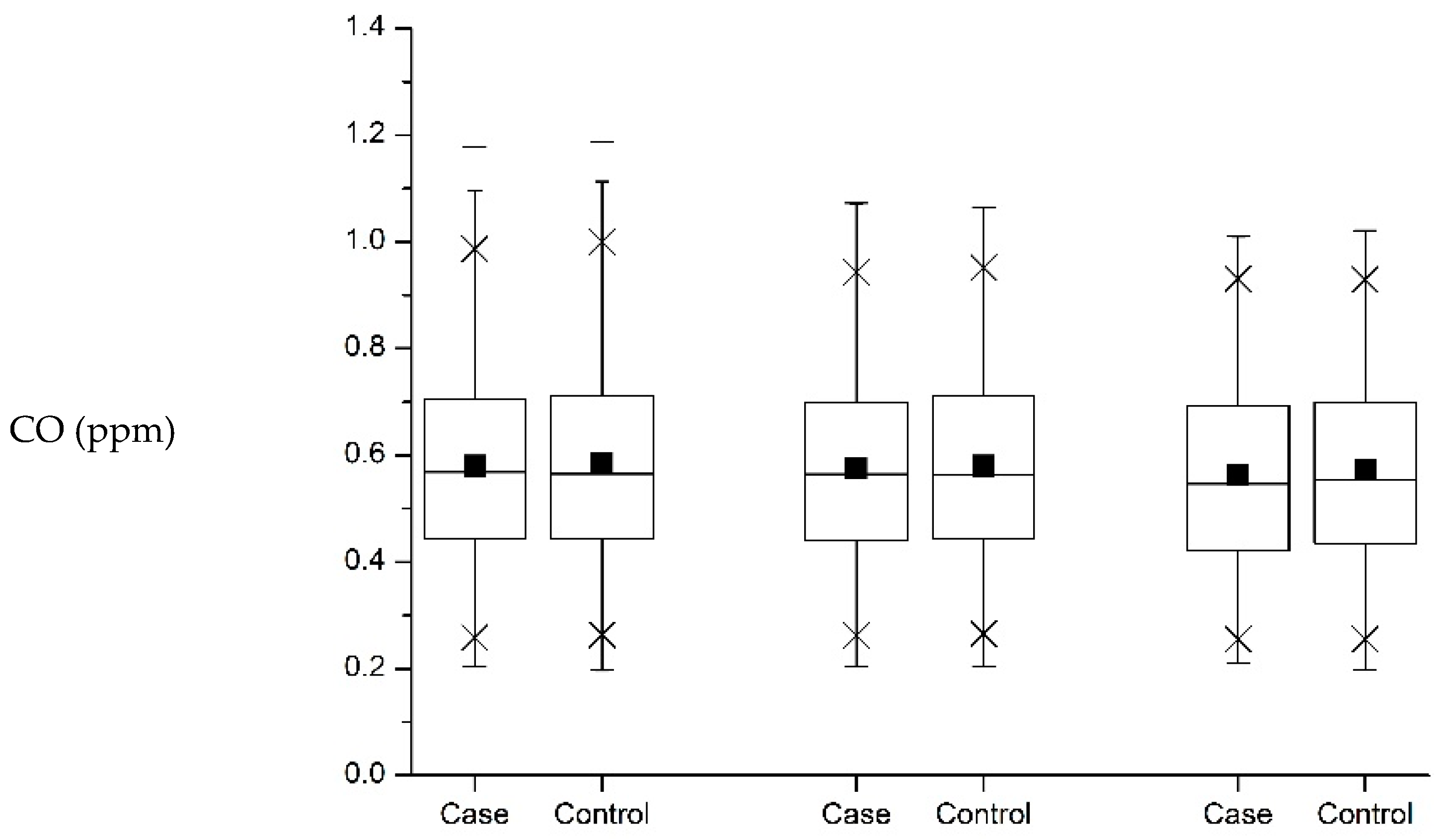
2.3. Assessment of Exposure to Air Pollution
2.4. Potential Confounders
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Balti, E.V.; Echouffo-Tcheugui, J.B.; Yako, Y.Y.; Kengne, A.P. Air pollution and risk of type 2 diabetes mellitus: A systematic review and meta-analysis. Diabetes Res. Clin. Pract. 2014, 106, 161–172. [Google Scholar] [CrossRef] [PubMed]
- Eze, I.C.; Hemkens, L.G.; Bucher, H.C.; Hoffmann, B.; Schindler, C.; Künzli, N.; Schikowski, T.; Probst-Hensch, N.M. Association between ambient air pollution and diabetes mellitus in Europe and North America: Systematic review and meta-analysis. Environ. Health Perspect. 2015, 123, 381–389. [Google Scholar] [CrossRef] [PubMed]
- Esposito, K.; Petrizzo, M.; Maiorino, M.I.; Bellastella, G.; Giugliano, D. Particulate matter pollutants and risk of type 2 diabetes: A time for concern? Endocrine 2016, 51, 32–37. [Google Scholar] [CrossRef] [PubMed]
- Van den Hooven, E.H.; Jaddoe, V.W.; de Kluizenaar, Y.; Hofman, A.; Mackenbach, J.P.; Steegers, E.A.; Miedema, H.M.; Pierik, F.H. Residential traffic exposure and pregnancy-related outcomes: A prospective birth cohort study. Environ. Health 2009, 8, 59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yorifuji, T.; Naruse, H.; Kashima, S.; Murakoshi, T.; Doi, H. Residential proximity to major roads and obstetrical complications. Sci. Total Environ. 2015, 508, 188–192. [Google Scholar] [CrossRef] [PubMed]
- Malmqvist, E.; Jakobsson, K.; Tinnerberg, H.; Rignell-Hydbom, A.; Rylander, L. Gestational diabetes and preeclampsia in association with air pollution at levels below current air quality guidelines. Environ. Health Perspect. 2013, 121, 488–493. [Google Scholar] [CrossRef] [PubMed]
- Fleisch, A.F.; Gold, D.R.; Rifas-Shiman, S.L.; Koutrakis, P.; Schwartz, J.D.; Kloog, I.; Melly, S.; Coull, B.A.; Zanobetti, A.; Gillman, M.W.; et al. Air pollution exposure and abnormal glucose tolerance during pregnancy: The project Viva cohort. Environ. Health Perspect. 2014, 122, 378–383. [Google Scholar] [CrossRef] [PubMed]
- Hu, H.; Ha, S.; Henderson, B.H.; Warner, T.D.; Roth, J.; Kan, H.; Xu, X. Association of atmospheric particulate matter and ozone with gestational diabetes mellitus. Environ. Health Perspect. 2015, 123, 853–859. [Google Scholar] [CrossRef] [PubMed]
- Fleisch, A.F.; Kloog, I.; Luttmann-Gibson, H.; Gold, D.R.; Oken, E.; Schwartz, J.D. Air pollution exposure and gestational diabetes mellitus among pregnant women in Massachusetts: A cohort study. Environ. Health 2016, 15, 40. [Google Scholar] [CrossRef] [PubMed]
- Robledo, C.A.; Mendola, P.; Yeung, E.; Mannisto, T.; Sundaram, R.; Liu, D.; Ying, Q.; Sherman, S.; Grantz, K.L. Preconception and early pregnancy air pollution exposures and risk of gestational diabetes mellitus. Environ. Res. 2015, 137, 316–322. [Google Scholar] [CrossRef] [PubMed]
- Pan, S.C.; Huang, C.C.; Lin, S.J.; Chen, B.Y.; Chang, C.C.; Leon Guo, Y.L. Gestational diabetes mellitus was related to ambient air pollutant nitric oxide during early gestation. Environ. Res. 2017, 158, 318–323. [Google Scholar] [CrossRef] [PubMed]
- Guariguata, L.; Linnenkamp, U.; Beagley, J.; Whiting, D.R.; Cho, N.H. Global estimates of the prevalence of hyperglycaemia in pregnancy. Diabetes Res. Clin. Pract. 2014, 103, 176–185. [Google Scholar] [CrossRef] [PubMed]
- Bellamy, L.; Casas, J.P.; Hingorani, A.D.; Williams, D. Type 2 diabetes mellitus after gestational diabetes: A systematic review and meta-analysis. Lancet 2009, 373, 1773–1779. [Google Scholar] [CrossRef]
- Zhu, Y.; Zhang, C. Prevalence of gestational diabetes and risk of progression to type 2 diabetes: A global perspective. Curr. Diabete Rep. 2016, 16, 7. [Google Scholar] [CrossRef] [PubMed]
- Shen, H.N.; Lu, C.L.; Li, C.Y. Effect of diabetes on severity and hospital mortality in patients with acute pancreatitis: A national population-based study. Diabetes Care 2012, 35, 1061–1066. [Google Scholar] [CrossRef] [PubMed]
- Environmental Protection Administration Executive Yuan, R.O.C. Taiwan Air Quality Monitoring Network. Available online: http://taqm.epa.gov.tw/taqm/en/b1300.aspx (accessed on 22 June 2017).
- Lin, H.C.; Lin, Y.J.; Hsiao, F.H.; Li, C.Y. Prenatal care visits and associated costs for treatment-seeking women with depressive disorder. Psychiatr. Serv. 2009, 60, 1261–1264. [Google Scholar] [CrossRef] [PubMed]
- Coogan, P.F.; White, L.F.; Jerrett, M.; Brook, R.D.; Su, J.G.; Seto, E.; Burnett, R.; Palmer, J.R.; Rosenberg, L. Air pollution and incidence of hypertension and diabetes mellitus in black women living in Los Angeles. Circulation 2012, 125, 767–772. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.C.; Wen, H.J.; Chen, P.C.; Chiang, T.L.; Lin, S.J.; Guo, Y.L. Prenatal air pollutant exposure and occurrence of atopic dermatitis. Br. J. Dermatol. 2015, 173, 981–988. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Ying, Y.; Wu, Q.; Zhang, H.; Ma, D.; Xiao, W. A GIS-based spatial correlation analysis for ambient air pollution and AECOPD hospitalizations in Jinan, China. Respir. Med. 2015, 109, 372–378. [Google Scholar] [CrossRef] [PubMed]
- Kan, H.; London, S.J.; Chen, G.; Zhang, Y.; Song, G.; Zhao, N.; Jiang, L.; Chen, B. Season, sex, age, and education as modifiers of the effects of outdoor air pollution on daily mortality in Shanghai, China: The Public Health and Air Pollution in Asia (PAPA) Study. Environ. Health Perspect. 2008, 116, 1183–1188. [Google Scholar] [CrossRef] [PubMed]
- Ben-Haroush, A.; Yogev, Y.; Hod, M. Epidemiology of gestational diabetes mellitus and its association with Type 2 diabetes. Diabete Med. 2004, 21, 103–113. [Google Scholar] [CrossRef]
- Buchanan, T.A.; Xiang, A.H.; Page, K.A. Gestational diabetes mellitus: Risks and management during and after pregnancy. Nat. Rev. Endocrinol. 2012, 8, 639–649. [Google Scholar] [CrossRef] [PubMed]
- Pan, M.L.; Chen, L.R.; Tsao, H.M.; Chen, K.H. Relationship between Polycystic Ovarian Syndrome and Subsequent Gestational Diabetes Mellitus: A Nationwide Population-Based Study. PLoS ONE 2015, 10, e0140544. [Google Scholar] [CrossRef] [PubMed]
- Yu, H.F.; Chen, H.S.; Rao, D.P.; Gong, J. Association between polycystic ovary syndrome and the risk of pregnancy complications: A PRISMA-compliant systematic review and meta-analysis. Medicine 2016, 95, e4863. [Google Scholar] [CrossRef] [PubMed]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Kirke, A.B.; Evans, S.F.; Walters, B.N. Gestational diabetes in a rural, regional centre in south Western Australia: Predictors of risk. Rural Remote Health 2014, 14, 2667. [Google Scholar] [PubMed]
- Collier, A.; Abraham, E.C.; Armstrong, J.; Godwin, J.; Monteath, K.; Lindsay, R. Reported prevalence of gestational diabetes in Scotland: The relationship with obesity, age, socioeconomic status, smoking and macrosomia, and how many are we missing? J. Diabetes Investig. 2017, 8, 161–167. [Google Scholar] [CrossRef] [PubMed]
- Tan, H.F.; Tseng, H.F.; Chang, C.K.; Lin, W.; Hsiao, S.H. Accessibility assessment of the health care improvement program in rural Taiwan. J. Rural Health 2005, 21, 372–377. [Google Scholar] [CrossRef] [PubMed]
- Hsu, C.Y.; Chiang, H.C.; Chen, M.J.; Chuang, C.Y.; Tsen, C.M.; Fang, G.C.; Tsai, Y.I.; Chen, N.T.; Lin, T.Y.; Lin, S.L.; et al. Ambient PM2.5 in the residential area near industrial complexes: Spatiotemporal variation, source apportionment, and health impact. Sci. Total Environ. 2017, 590–591, 204–214. [Google Scholar] [CrossRef] [PubMed]
- Wang, B.; Xu, D.; Jing, Z.; Liu, D.; Yan, S.; Wang, Y. Effect of long-term exposure to air pollution on type 2 diabetes mellitus risk: A systemic review and meta-analysis of cohort studies. Eur. J. Endocrinol. 2014, 171, R173–R182. [Google Scholar] [CrossRef] [PubMed]
- Lu, M.C.; Wang, P.; Cheng, T.J.; Yang, C.P.; Yan, Y.H. Association of temporal distribution of fine particulate matter with glucose homeostasis during pregnancy in women of Chiayi City, Taiwan. Environ. Res. 2017, 152, 81–87. [Google Scholar] [CrossRef] [PubMed]
- Hernandez, T.L.; Friedman, J.E.; Van Pelt, R.E.; Barbour, L.A. Patterns of glycemia in normal pregnancy should the current therapeutic targets be challenged? Diabetes Care 2011, 34, 1660–1668. [Google Scholar] [CrossRef] [PubMed]
- Teichert, T.; Vossoughi, M.; Vierkotter, A.; Sugiri, D.; Schikowski, T.; Schulte, T.; Roden, M.; Luckhaus, C.; Herder, C.; Kramer, U. Association between traffic-related air pollution, subclinical inflammation and impaired glucose metabolism: Results from the SALIA study. PLoS ONE 2013, 8, e83042. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pedersen, M.; Andersen, Z.J.; Stafoggia, M.; Weinmayr, G.; Galassi, C.; Sørensen, M.; Eriksen, K.T.; Tjønneland, A.; Loft, S.; Jaensch, A.; et al. Ambient air pollution and primary liver cancer incidence in four European cohorts within the ESCAPE project. Environ. Res. 2017, 154, 226–233. [Google Scholar] [CrossRef] [PubMed]
- Chu, S.Y.; Callaghan, W.M.; Kim, S.Y.; Schmid, C.H.; Lau, J.; England, L.J.; Dietz, P.M. Maternal obesity and risk of gestational diabetes mellitus. Diabetes Care 2007, 30, 2070–2076. [Google Scholar] [CrossRef] [PubMed]
- Ryckman, K.K.; Spracklen, C.N.; Smith, C.J.; Robinson, J.G.; Saftlas, A.F. Maternal lipid levels during pregnancy and gestational diabetes: A systematic review and meta-analysis. BJOG 2015, 122, 643–651. [Google Scholar] [CrossRef] [PubMed]
- Lu, M.; Xu, Y.; Lv, L.; Zhang, M. Association between vitamin D status and the risk of gestational diabetes mellitus: A meta-analysis. Arch. Gynecol. Obstet. 2016, 293, 959–966. [Google Scholar] [CrossRef] [PubMed]
- Lin, P.C.; Hung, C.H.; Chan, T.F.; Lin, K.C.; Hsu, Y.Y.; Ya-Ling, T. The risk factors for gestational diabetes mellitus: A retrospective study. Midwifery 2016, 42, 16–20. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Cases | Controls | p-Value a | |||
|---|---|---|---|---|---|
| n | % | n | % | ||
| Age at delivery, years | |||||
| <25 | 468 | 7.0 | 470 | 7.0 | |
| 25–29 | 1782 | 26.5 | 1780 | 26.5 | |
| 30–34 | 2946 | 43.9 | 2949 | 43.9 | |
| >35 | 1521 | 22.6 | 1518 | 22.6 | |
| Mean ± SD | 31.30 ± 4.54 | 31.12 ± 4.51 | 0.0042 | ||
| Primipara | <0.0001 | ||||
| Yes | 3560 | 53.0 | 4532 | 67.5 | |
| No | 3157 | 47.0 | 2185 | 32.5 | |
| Monthly income, NTD | <0.0001 | ||||
| Dependent | 1484 | 22.1 | 1355 | 20.2 | |
| ≤15,840 | 981 | 14.6 | 959 | 14.3 | |
| 15,841–22,800 | 1854 | 27.6 | 1833 | 27.3 | |
| 22,801–28,800 | 719 | 10.7 | 749 | 11.2 | |
| 28,801–36,300 | 725 | 10.8 | 733 | 10.9 | |
| 36,301–45,800 | 672 | 10.0 | 718 | 10.7 | |
| >45,800 | 282 | 4.2 | 370 | 5.5 | |
| Urbanization | <0.0001 | ||||
| Urban | 1847 | 27.5 | 1855 | 27.6 | |
| Satellite | 2613 | 38.9 | 3081 | 45.9 | |
| Rural | 2257 | 33.6 | 1781 | 26.5 | |
| Township-specific median family annual income quartiles a, NTD | <0.0001 | ||||
| ≤Q1 | 1686 | 25.1 | 1374 | 20.5 | |
| >Q1–Q2 | 1679 | 25.0 | 1647 | 24.5 | |
| >Q2–Q3 | 1679 | 25.0 | 1753 | 26.1 | |
| >Q3 | 1673 | 24.9 | 1943 | 28.9 | |
| Mean ± SD | 873,000 ± 224,000 | 893,000 ± 228,000 | 0.0143 | ||
| Diagnosed co-morbidity | |||||
| Polycystic ovary syndrome | 504 | 7.5 | 3509 | 5.2 | <0.0001 |
| Obesity | 82 | 1.2 | 47 | 0.7 | <0.0001 |
| Charlson Comorbidity Index | |||||
| 0 | 4442 | 66.1 | 4628 | 68.9 | <0.0001 |
| 1 | 1680 | 25.0 | 1605 | 23.9 | |
| 2 | 442 | 6.6 | 363 | 5.4 | |
| ≧3 | 153 | 2.3 | 121 | 1.8 | |
| Mean ± SD | 0.47 ± 0.80 | 0.41 ± 0.74 | |||
| Season of delivery | 0.0143 | ||||
| Spring (March–May) | 1545 | 23.0 | 1619 | 24.1 | |
| Summer (June–August) | 1587 | 23.6 | 1652 | 24.6 | |
| Fall (September–November) | 1888 | 28.1 | 1780 | 26.5 | |
| Winter (December–February) | 1697 | 25.3 | 1666 | 24.8 | |
| Total | 6717 | 6717 | |||
| Time Period and Increase in Exposure | Odds Ratio (95% CI) | |
|---|---|---|
| Crude | Adjusted a | |
| Within the 12-week period prior to pregnancy | ||
| PM2.5 (μg/m3) | ||
| Per 1 IQR increase | 1.22 (1.17–1.26) | 1.10 (1.03–1.18) b |
| Per 1 SD increase | 1.17 (1.13–1.21) | 1.08 (1.03–1.14) |
| SO2 (ppb) | ||
| Per 1 IQR increase | 1.28 (1.24–1.33) | 1.37 (1.30–1.45) |
| Per 1 SD increase | 1.24 (1.21–1.28) | 1.32 (1.26–1.38) |
| O3 (ppb) | ||
| Per 1 IQR increase | 1.08 (1.03–1.13) | 1.01 (0.96–1.07) |
| Per 1 SD increase | 1.05 (1.02–1.09) | 1.01 (0.97–1.05) |
| NO2 (ppb) | ||
| Per 1 IQR increase | 1.01 (0.96–1.06) | 0.96 (0.90–1.02) |
| Per 1 SD increase | 1.01 (0.97–1.04) | 0.97 (0.93–1.02) |
| During the 1st trimester | ||
| PM2.5 (μg/m3) | ||
| Per 1 IQR increase | 1.20 (1.16–1.25) | 1.09 (1.02–1.17) |
| Per 1 SD increase | 1.16 (1.13–1.20) | 1.08 (1.02–1.13) |
| SO2 (ppb) | ||
| Per 1 IQR increase | 1.28 (1.23–1.32) | 1.37 (1.30–1.45) |
| Per 1 SD increase | 1.23 (1.19–1.27) | 1.31 (1.25–1.37) |
| O3 (ppb) | ||
| Per 1 IQR increase | 1.07 (1.03–1.13) | 1.02 (0.96–1.08) |
| Per 1 SD increase | 1.05 (1.02–1.09) | 1.01 (0.97–1.06) |
| NO2 (ppb) | ||
| Per 1 IQR increase | 1.00 (0.95–1.05) | 0.93 (0.88–1.00) |
| Per 1 SD increase | 1.00 (0.97–1.03) | 0.95 (0.91–1.00) |
| During the 2nd trimester | ||
| PM2.5 (μg/m3) | ||
| Per 1 IQR increase | 1.16 (1.12–1.21) | 1.07 (1.01–1.14) |
| Per 1 SD increase | 1.13 (1.10–1.17) | 1.06 (1.01–1.11) |
| SO2 (ppb) | ||
| Per 1 IQR increase | 1.27 (1.22–1.31) | 1.38 (1.31–1.46) |
| Per 1 SD increase | 1.23 (1.19–1.26) | 1.32 (1.26–1.38) |
| O3 (ppb) | ||
| Per 1 IQR increase | 1.11 (1.06–1.16) | 1.04 (0.99–1.11) |
| Per 1 SD increase | 1.07 (1.04–1.11) | 1.03 (0.99–1.07) |
| NO2 (ppb) | ||
| Per 1 IQR increase | 0.95 (0.91–0.99) | 0.97 (0.93–1.02) |
| Per 1 SD increase | 0.97 (0.94–0.99) | 0.98 (0.93–1.03) |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shen, H.-N.; Hua, S.-Y.; Chiu, C.-T.; Li, C.-Y. Maternal Exposure to Air Pollutants and Risk of Gestational Diabetes Mellitus in Taiwan. Int. J. Environ. Res. Public Health 2017, 14, 1604. https://doi.org/10.3390/ijerph14121604
Shen H-N, Hua S-Y, Chiu C-T, Li C-Y. Maternal Exposure to Air Pollutants and Risk of Gestational Diabetes Mellitus in Taiwan. International Journal of Environmental Research and Public Health. 2017; 14(12):1604. https://doi.org/10.3390/ijerph14121604
Chicago/Turabian StyleShen, Hsiu-Nien, Sheng-Yuan Hua, Chang-Ta Chiu, and Chung-Yi Li. 2017. "Maternal Exposure to Air Pollutants and Risk of Gestational Diabetes Mellitus in Taiwan" International Journal of Environmental Research and Public Health 14, no. 12: 1604. https://doi.org/10.3390/ijerph14121604