Prevalence of Tobacco Smoking and Determinants of Success in Quitting Smoking among Patients with Chronic Diseases: A Cross-Sectional Study in Rural Western China


Abstract
:1. Introduction
2. Methods
2.1. Study Design and Sample
2.2. Data Collection and Measures
2.3. Statistical Analysis
3. Results
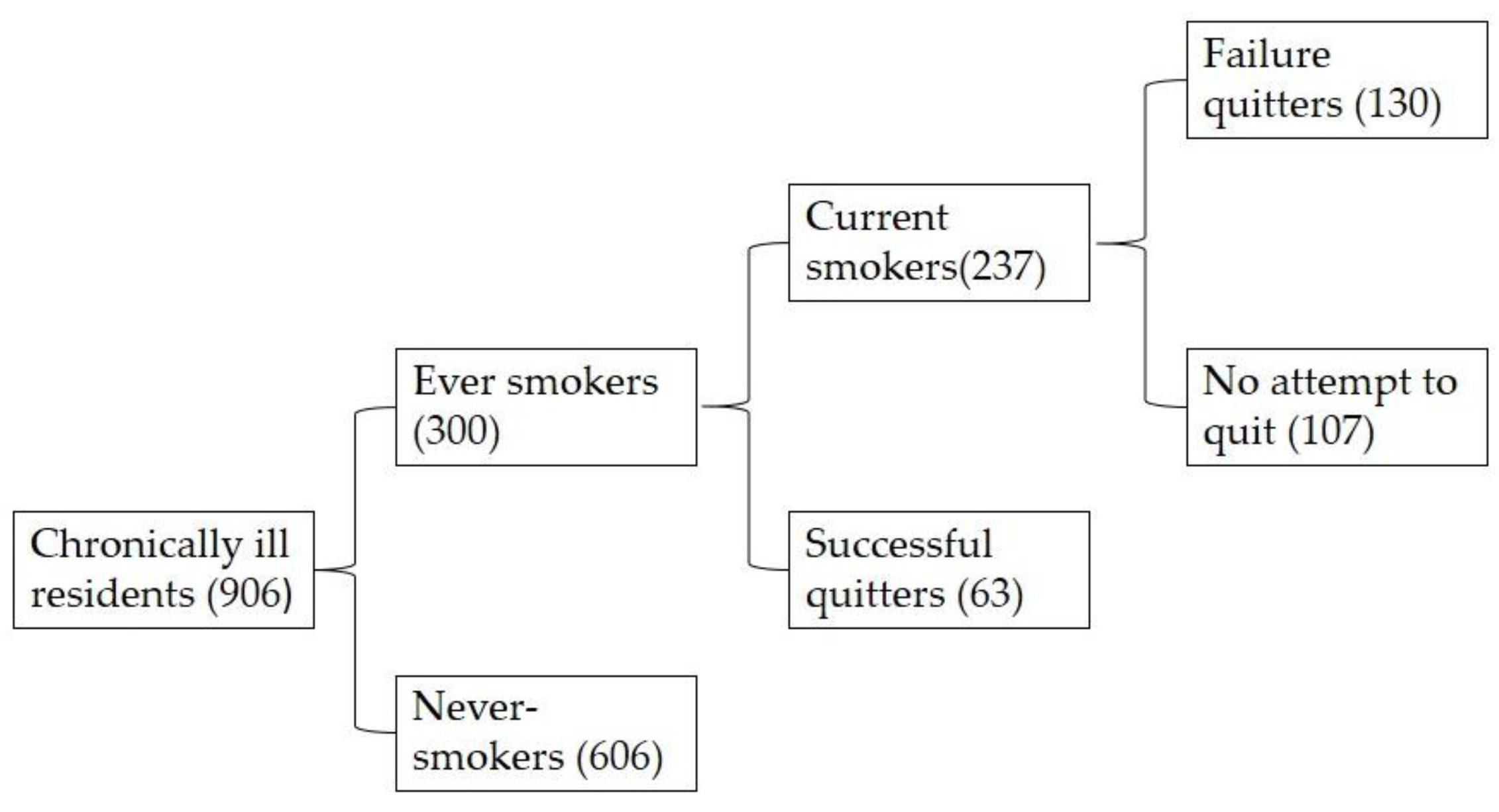
3.1. Classification of Participants
3.2. Characteristics of the Study Population and Smoking Prevalence
3.3. Smoking Behavior and Reasons for Quitting Smoking
3.4. Predictors Affecting Success in Quitting Smoking among Smokers with Chronic Diseases
4. Discussion
5. Limitations
6. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- World Health Organization. WHO Report on the Global Tobacco Epidemic; World Health Organization: Geneva, Switzerland, 2008. [Google Scholar]
- Li, C. The Political Mapping of China’s Tobacco Industry and Anti-Smoking Campaign; John L. Thornton China Center: Brookings, OR, USA, 2012. [Google Scholar]
- Hu, T.-W.; Mao, Z. Economic Analysis of Tobacco and Options for Tobacco Control: China Case Study; World Bank/WHO: Washington, DC, USA, 2002. [Google Scholar]
- Wu, F.; Guo, Y.; Chatterji, S.; Zheng, Y.; Naidoo, N.; Jiang, Y.; Biritwum, R.; Yawson, A.; Minicuci, N.; Salinas-Rodriguez, A. Common risk factors for chronic non-communicable diseases among older adults in China, Ghana, Mexico, India, Russia and South Africa: The study on global ageing and adult health (SAGE) wave 1. BMC Public Health 2015, 15, 88. [Google Scholar] [CrossRef] [PubMed]
- Erhardt, L. Cigarette smoking: An undertreated risk factor for cardiovascular disease. Atherosclerosis 2009, 205, 23–32. [Google Scholar] [CrossRef] [PubMed]
- Beaglehole, R.; Bonita, R.; Horton, R.; Adams, C.; Alleyne, G.; Asaria, P.; Baugh, V.; Bekedam, H.; Billo, N.; Casswell, S.; et al. Priority actions for the non-communicable disease crisis. Lancet 2011, 377, 1438–1447. [Google Scholar] [CrossRef]
- Epping-Jordan, J.E.; Galea, G.; Tukuitonga, C.; Beaglehole, R. Preventing chronic diseases: Taking stepwise action. Lancet 2005, 366, 1667–1671. [Google Scholar] [CrossRef]
- Unwin, N.; Alberti, K. Chronic non-communicable diseases. Ann. Trop. Med. Parasitol. 2006, 100, 455–464. [Google Scholar] [CrossRef] [PubMed]
- Campos, T.D.S.; Richter, K.P.; Cupertino, A.P.; Galil, A.G.; Banhato, E.F.; Colugnati, F.A.; Batos, M.G. Cigarette smoking among patients with chronic diseases. Int. J. Cardiol. 2014, 174, 808. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Kong, L.; Wu, F.; Bai, Y.; Burton, R. Preventing chronic diseases in China. Lancet 2005, 366, 1821–1824. [Google Scholar] [CrossRef]
- Liu, R.; Dang, S.; Yan, H.; Wang, D.; Zhao, Y.; Li, Q.; Liu, X. Association between dietary protein intake and the risk of hypertension: A cross-sectional study from rural western China. Hypertens. Res. 2013, 36, 972–979. [Google Scholar] [CrossRef] [PubMed]
- Pei, L.; Wang, D.; Ren, L.; Yan, H. Evaluation of the rural primary health care project on undernutrition equity among children in rural western China. Health Policy Plan. 2013, 28, 429–434. [Google Scholar] [CrossRef] [PubMed]
- Who, J.; Consultation, F.E. Diet, nutrition and the prevention of chronic diseases. World Health Organ. Tech. Rep. Ser. 2003, 916, 1–149. [Google Scholar]
- Dain, K.; Parsons-Perez, C.; John, S.; Watt, J. Translating global commitments on NCDs into national action: The role of civil society. Lancet Diabetes Endocrinol. 2016, 4, 12–14. [Google Scholar] [CrossRef]
- Yuan, F.; Qian, D.; Huang, C.; Tian, M.; Xiang, Y.; He, Z.; Feng, Z. Analysis of awareness of health knowledge among rural residents in western China. BMC Public Health 2015, 15, 55. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Song, H.; Wang, T.; Wang, T.; Yang, H.; Gong, J.; Shen, Y.; Dai, W.; Zhou, J.; Zhu, S. Determinants of tobacco smoking among rural-to-urban migrant workers: A cross-sectional survey in Shanghai. BMC Public Health 2015, 15, 131. [Google Scholar] [CrossRef] [PubMed]
- Wan, X.; Shin, S.S.; Wang, Q.; Raymond, H.F.; Liu, H.; Ding, D.; Yang, G.; Novotny, T.E. Smoking among young rural to urban migrant women in China: A cross-sectional survey. PLoS ONE 2011, 6, e23028. [Google Scholar] [CrossRef] [PubMed]
- Bian, J.; Du, M.; Liu, Z.; Fan, Y.; Eshita, Y.; Sun, J. Prevalence of and factors associated with daily smoking among Inner Mongolia medical students in China: A cross-sectional questionnaire survey. Subst. Abuse Treat. Prev. Policy 2012, 7, 20. [Google Scholar] [CrossRef] [PubMed]
- Im, P.K.; McNeill, A.; Thompson, M.E.; Fong, G.T.; Xu, S.; Quah, A.C.; Jiang, Y.; Shahab, L. Individual and interpersonal triggers to quit smoking in China: A cross-sectional analysis. Tob. Control 2015, 24, iv40–iv47. [Google Scholar] [CrossRef]
- Wang, J.; Li, C.; Jia, C.; Liu, Y.; Liu, J.; Yan, X.; Fang, Y. Smoking, smoking cessation and tobacco control in rural China: A qualitative study in Shandong province. BMC Public Health 2014, 14, 916. [Google Scholar] [CrossRef] [PubMed]
- Virdis, A.; Giannarelli, C.; Fritsch Neves, M.; Taddei, S.; Ghiadoni, L. Cigarette smoking and hypertension. Curr. Pharm. Des. 2010, 16, 2518–2525. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Curhan, G.C.; Hu, F.B.; Rimm, E.B.; Forman, J.P. Association between passive and active smoking and incident type 2 diabetes in women. Diabetes Care 2011, 34, 892–897. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tang, S.; Dong, D.; Ji, L.; Fu, H.; Feng, Z.; Bishwajit, G.; He, Z.; Ming, H.; Fu, Q.; Xian, Y. What contributes to the activeness of ethnic minority patients with chronic illnesses seeking allied health services? A cross-sectional study in rural western China. Int. J. Environ. Res. Public Health 2015, 12, 11579–11593. [Google Scholar] [CrossRef] [PubMed]
- Gu, D.; Reynolds, K.; Wu, X.; Chen, J.; Duan, X.; Muntner, P.; Huang, G.; Reynolds, R.F.; Su, S.; Whelton, P.K. Prevalence, awareness, treatment, and control of hypertension in China. Hypertension 2002, 40, 920–927. [Google Scholar] [CrossRef] [PubMed]
- Lorig, K.R.; Ritter, P.; Stewart, A.L.; Sobel, D.S.; Brown, B.W., Jr.; Bandura, A.; Gonzalez, V.M.; Laurent, D.D.; Holman, H.R. Chronic disease self-management program: 2-year health status and health care utilization outcomes. Med. Care 2001, 39, 1217–1223. [Google Scholar] [CrossRef] [PubMed]
- Barnett, K.; Mercer, S.W.; Norbury, M.; Watt, G.; Wyke, S.; Guthrie, B. Epidemiology of multimorbidity and implications for health care, research, and medical education: A cross-sectional study. Lancet 2012, 380, 37–43. [Google Scholar] [CrossRef]
- Sun, X.; Chen, Y.; Tong, X.; Feng, Z.; Wei, L.; Zhou, D.; Tian, M.; Lv, B.; Feng, D. The use of annual physical examinations among the elderly in rural China: A cross-sectional study. BMC Health Serv. Res. 2014, 14, 16. [Google Scholar] [CrossRef] [PubMed]
- He, Z.; Cheng, Z.; Shao, T.; Liu, C.; Shao, P.; Bishwajit, G.; Feng, D.; Feng, Z. Factors influencing health knowledge and behaviors among the elderly in rural China. Int. J. Environ. Res. Public Health 2016, 13, 975. [Google Scholar] [CrossRef] [PubMed]
- Yang, G.; Ma, J.; Liu, N.; Zhou, L. Smoking and passive smoking in Chinese, 2002. Chin. J. Epidemiol. 2005, 26, 77–83. [Google Scholar]
- National Health and Family Planning Commission of the People’s Republic of China. China Family Development Report 2015. Available online: http://sanwen8.cn/p/181YD6J.html (accessed on 6 January 2017).
- Hesketh, T.; Lu, L.; Jun, Y.X.; Mei, W.H. Smoking, cessation and expenditure in low income Chinese: Cross sectional survey. BMC Public Health 2007, 7, 29. [Google Scholar] [CrossRef] [PubMed]
- Mou, J.; Fellmeth, G.; Griffiths, S.; Dawes, M.; Cheng, J. Tobacco smoking among migrant factory workers in Shenzhen, China. Nicotine Tob. Res. 2013, 15, 69–76. [Google Scholar] [CrossRef] [PubMed]
- Yang, G.; Jason, H.; Yang, Y. Global Adult Tobacco Survey (Gats) China 2010 Country Report; China Three Gorges Publishing House: Beijing, China, 2011. [Google Scholar]
- Yang, T.; Wu, J.; Rockett, I.; Abdullah, A.; Beard, J.; Ye, J. Smoking patterns among Chinese rural–urban migrant workers. Public Health 2009, 123, 743–749. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Hammond, D.; Driezen, P.; O’Connor, R.J.; Li, Q.; Yong, H.-H.; Fong, G.T.; Jiang, Y. The use of cessation assistance among smokers from China: Findings from the ITC China survey. BMC Public Health 2011, 11, 75. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Ou, J.X.; Bai, C.X. Tobacco smoking in China: Prevalence, disease burden, challenges and future strategies. Respirology 2011, 16, 1165–1172. [Google Scholar] [CrossRef] [PubMed]
- Poureslami, I.; Nimmon, L.; Rootman, I.; Fitzgerald, M.J. Health literacy and chronic disease management: Drawing from expert knowledge to set an agenda. Health Promot. Int. 2016. [Google Scholar] [CrossRef] [PubMed]
- Taggart, J.; Williams, A.; Dennis, S.; Newall, A.; Shortus, T.; Zwar, N.; Denney-Wilson, E.; Harris, M.F. A systematic review of interventions in primary care to improve health literacy for chronic disease behavioral risk factors. BMC Fam. Pract. 2012, 13, 49. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Feng, G.; Jiang, Y.; Yong, H.H.; Borland, R.; Fong, G.T. Prospective predictors of quitting behaviours among adult smokers in six cities in China: Findings from the international tobacco control (ITC) China survey. Addiction 2011, 106, 1335–1345. [Google Scholar] [CrossRef] [PubMed]
- Shi, Y.; Yu, C.; Luo, A.; Huang, Y.; Warner, D.O. Perioperative tobacco interventions by Chinese anesthesiologistspractices and attitudes. J. Am. Soc. Anesthesiol. 2010, 112, 338–346. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Hammond, D.; Driezen, P.; Fong, G.T.; Jiang, Y. Health knowledge and perception of risks among Chinese smokers and non-smokers: Findings from the wave 1 ITC China survey. Tob. Control 2010, 19, i18–i23. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.; Zheng, R.; Emery, S. Assessing the impact of the national smoking ban in indoor public places in China: Evidence from quit smoking related online searches. PLoS ONE 2013, 8, e65577. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable | Total (N) | Current Smokers | χ2 | p | |
|---|---|---|---|---|---|
| N | % | ||||
| Gender | 250.183 | <0.001 | |||
| Male | 472 | 228 | 48.3 | ||
| Female | 434 | 9 | 2.1 | ||
| Age | 1.866 | 0.389 | |||
| <50 | 129 | 39 | 30.2 | ||
| 50–65 | 370 | 99 | 26.8 | ||
| >65 | 407 | 99 | 24.3 | ||
| Number of people in household | 5.414 | 0.067 | |||
| 1–2 | 97 | 34 | 35.1 | ||
| 3–5 | 470 | 124 | 26.4 | ||
| >6 | 339 | 79 | 23.3 | ||
| Educational level | 60.390 | <0.001 | |||
| Less than 6 years study | 512 | 83 | 16.2 | ||
| 6–9 years study | 271 | 107 | 39.5 | ||
| Over 9 years study | 123 | 47 | 38.2 | ||
| Annual disposable household income * | 0.383 | 0.658 | |||
| <RMB10,000 | 242 | 68 | 28.1 | ||
| RMB10,000–RMB29,999 | 422 | 105 | 24.9 | ||
| >RMB30,000 | 242 | 64 | 26.4 | ||
| Comorbidity of diseases | 1.932 | 0.165 | |||
| Yes | 481 | 135 | 28.1 | ||
| No | 425 | 102 | 24.0 | ||
| Health knowledge level | 1.661 | 0.198 | |||
| Below | 411 | 116 | 28.2 | ||
| Higher | 495 | 121 | 24.4 | ||
| Exercise | 2.444 | 0.295 | |||
| Always | 562 | 157 | 27.9 | ||
| Sometime | 221 | 52 | 23.5 | ||
| Hardly | 123 | 28 | 22.8 | ||
| Frequency of physical examination | 10.413 | 0.005 | |||
| Once a year | 710 | 170 | 23.9 | ||
| Occasion | 110 | 42 | 38.2 | ||
| Hardly | 86 | 25 | 29.1 | ||
| Take medicine on time | 11.966 | 0.001 | |||
| Yes | 747 | 178 | 23.8 | ||
| No | 159 | 59 | 37.1 | ||
| Total | 906 | 237 | 26.2 | ||
| Variable | N | % |
|---|---|---|
| Family member smoker | ||
| Yes | 113 | 47.7 |
| No | 124 | 52.3 |
| Average number of cigarettes smoked per day | ||
| <5 | 84 | 35.4 |
| 5–10 | 59 | 24.9 |
| 11–20 | 60 | 25.3 |
| >20 | 34 | 14.3 |
| Quit attempts previously | ||
| Yes (=failure quitters) | 130 | 54.9 |
| No | 107 | 45.1 |
| Smoking restrictions in home | ||
| Yes | 113 | 47.7 |
| No | 124 | 52.3 |
| Smoking restrictions in work place | ||
| Yes | 141 | 59.5 |
| No | 96 | 40.5 |
| Smoking restrictions in public place | ||
| Yes | 108 | 45.6 |
| No | 129 | 54.4 |
| Reasons | Total N (%) | Failure Quitters N (%) | Successful Quitters N (%) | χ2 | p |
|---|---|---|---|---|---|
| Disease effect | 125 (64.8) | 85 (65.4) | 40 (63.5) | 0.067 | 0.796 |
| Doctor’s advice | 35 (18.1) | 28 (21.5) | 7 (11.1) | 3.108 | 0.078 |
| Family member pressure | 33 (17.1) | 26 (20.0) | 7 (11.1) | 2.365 | 0.124 |
| Economic factor | 16 (8.3) | 9 (6.9) | 7 (11.1) | 0.979 | 0.322 |
| Others | 18 (9.3) | 10 (7.7) | 8 (12.7) | 1.258 | 0.262 |
| Variable | Failure Quitters N (%) | Successful Quitters N (%) | χ2 | p |
|---|---|---|---|---|
| Gender | - | 0.011 a | ||
| Male | 130 (100.0) | 59 (93.7) | ||
| Female | 0 (0.0) | 4 (6.3) | ||
| Comorbidity of diseases | 7.593 | 0.006 | ||
| Yes | 79 (60.8) | 25 (39.7) | ||
| No | 51 (39.2) | 38 (60.3) | ||
| Exercise | 7.632 | 0.022 | ||
| Always | 85 (65.4) | 29 (46.0) | ||
| Sometime | 27 (20.8) | 24 (38.1) | ||
| Never | 18 (13.8) | 10 (15.9) | ||
| Smoking restrictions in work place | 10.099 | 0.001 | ||
| Yes | 45 (34.6) | 37 (58.7) | ||
| No | 85 (65.4) | 26 (41.3) | ||
| Smoking restrictions in public place | 10.293 | 0.001 | ||
| Yes | 61 (46.9) | 45 (71.4) | ||
| No | 69 (53.1) | 18 (28.6) |
| Predictors | Reference | B | p | OR | 95% CI | |
|---|---|---|---|---|---|---|
| Lower | Upper | |||||
| Gender | Female | −21.708 | 0.999 | 0.000 | 0.000 | 0.000 |
| Comorbidity of diseases | Yes | 0.711 | 0.033 | 2.037 | 1.060 | 3.912 |
| Smoking restrictions in public place | No | 0.783 | 0.023 | 2.188 | 1.116 | 4.291 |
| Constants | 20.103 | 0.999 | 5.377 | |||
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license ( http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fu, H.; Feng, D.; Tang, S.; He, Z.; Xiang, Y.; Wu, T.; Wang, R.; Shao, T.; Liu, C.; Shao, P.; et al. Prevalence of Tobacco Smoking and Determinants of Success in Quitting Smoking among Patients with Chronic Diseases: A Cross-Sectional Study in Rural Western China. Int. J. Environ. Res. Public Health 2017, 14, 167. https://doi.org/10.3390/ijerph14020167
Fu H, Feng D, Tang S, He Z, Xiang Y, Wu T, Wang R, Shao T, Liu C, Shao P, et al. Prevalence of Tobacco Smoking and Determinants of Success in Quitting Smoking among Patients with Chronic Diseases: A Cross-Sectional Study in Rural Western China. International Journal of Environmental Research and Public Health. 2017; 14(2):167. https://doi.org/10.3390/ijerph14020167
Chicago/Turabian StyleFu, Hang, Da Feng, Shangfeng Tang, Zhifei He, Yuanxi Xiang, Tailai Wu, Ruoxi Wang, Tian Shao, Chunyan Liu, Piaopiao Shao, and et al. 2017. "Prevalence of Tobacco Smoking and Determinants of Success in Quitting Smoking among Patients with Chronic Diseases: A Cross-Sectional Study in Rural Western China" International Journal of Environmental Research and Public Health 14, no. 2: 167. https://doi.org/10.3390/ijerph14020167
APA StyleFu, H., Feng, D., Tang, S., He, Z., Xiang, Y., Wu, T., Wang, R., Shao, T., Liu, C., Shao, P., & Feng, Z. (2017). Prevalence of Tobacco Smoking and Determinants of Success in Quitting Smoking among Patients with Chronic Diseases: A Cross-Sectional Study in Rural Western China. International Journal of Environmental Research and Public Health, 14(2), 167. https://doi.org/10.3390/ijerph14020167