Occupational Respiratory Diseases of Miners from Two Gold Mines in Ghana

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Data Collection and Instruments
2.3. Statistical Analysis
3. Results
3.1. Background Characteristics
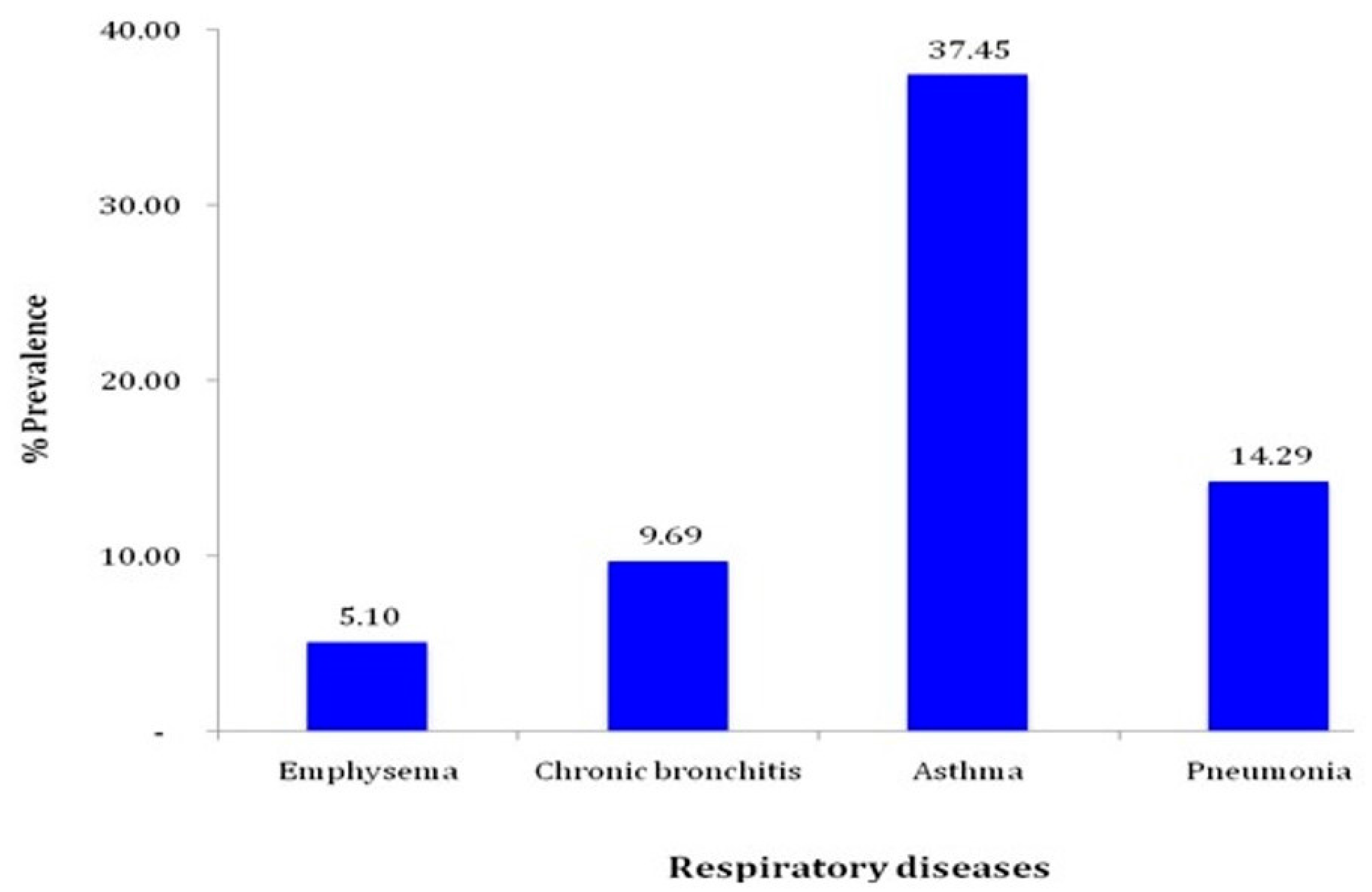
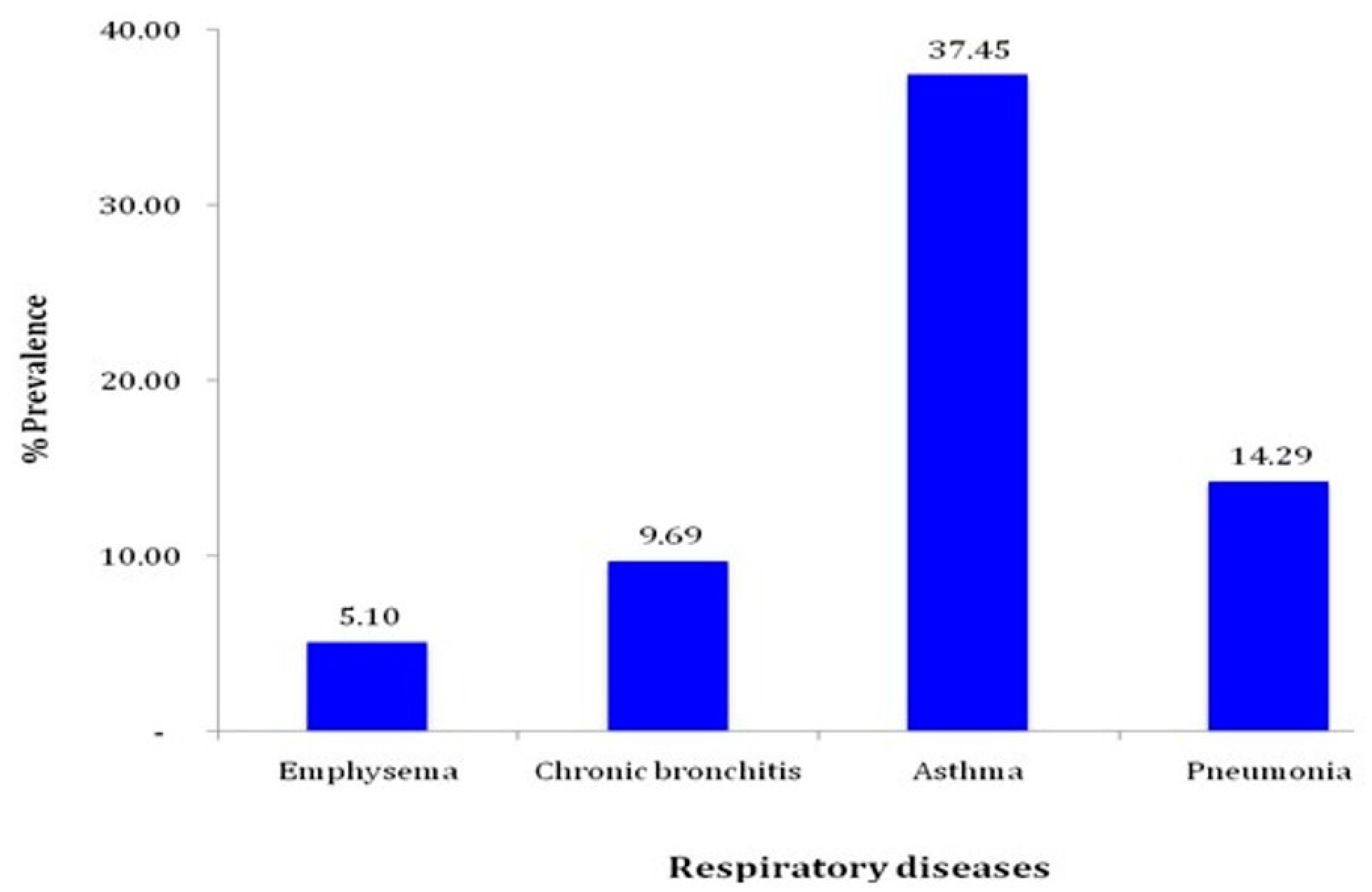
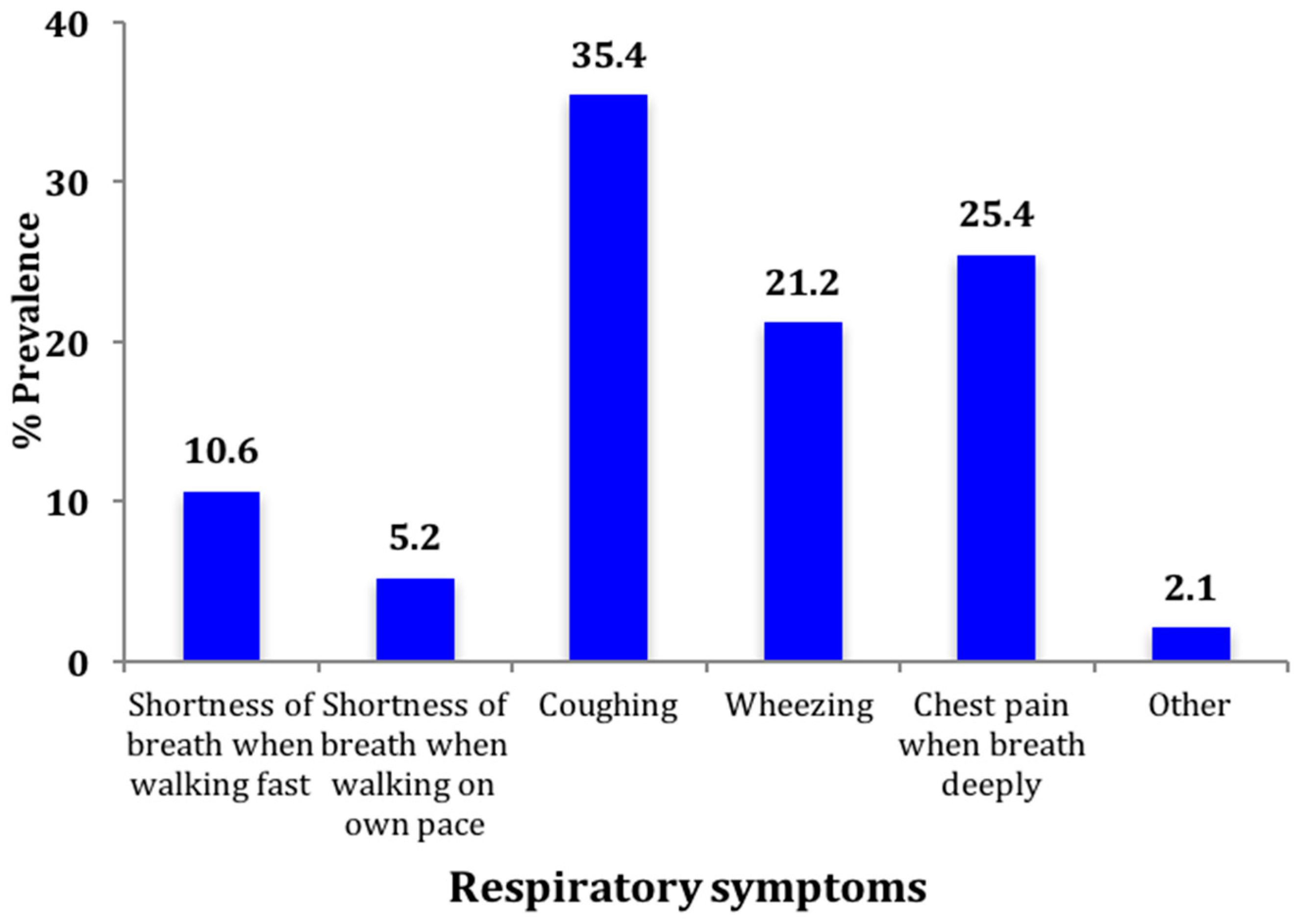
3.2. Prevalence of Respiratory Diseases and Symptoms
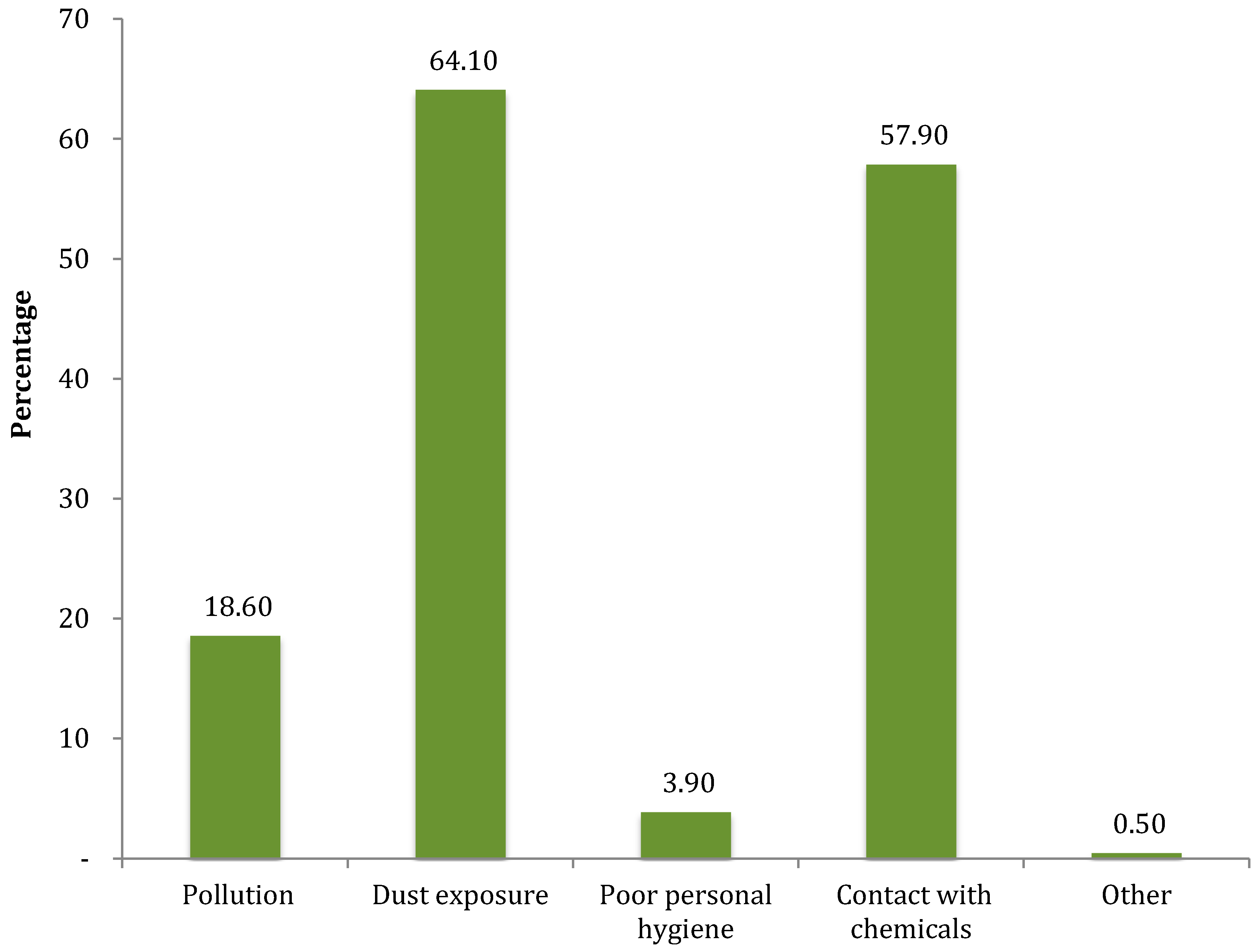
3.3. Factors Influencing Respiratory Diseases
3.4. Multivariable Logistic Regression
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- International Labour Organisation. The Prevention of Occupational Diseases. Available oline: http://www.ilo.org/safework/info/publications/WCMS_208226/lang--en/index.htm (accessed on 20 November 2016).
- Fernandes, A.L.G.; Stelmach, R.; Algranti, E. Occupational asthma. J. Bras. Pneumol. 2006, 32, S27–S34. [Google Scholar] [CrossRef] [PubMed]
- Ross, M.H.; Murray, J. Occupational respiratory disease in mining. Occup. Med. 2004, 54, 304–310. [Google Scholar] [CrossRef] [PubMed]
- International Labour Organization. ILO Introductory Report: Global Trends and Challenges on Occupational Safety and Health. Available online: http://www.ilo.org/wcmsp5/groups/public/@ed_protect/@protrav/@safework/documents/publication/wcms_162662.pdf (accessed on 20 November 2016).
- De Borges, R.C.C.O.; Barros Júnior, J.C.; Oliveira, F.B.; Brunherotti, M.A.; Quemelo, P.R.V. Evaluation of pulmonary function and respiratory symptoms in pyrochlore mine workers. J. Bras. Pneumol. 2016, 42, 279–285. [Google Scholar] [CrossRef] [PubMed]
- Plumlee, G.S.; Morman, S.A. Mine wastes and human health. Elements 2011, 7, 399–404. [Google Scholar] [CrossRef]
- Rees, D.; Murray, J. Silica, silicosis and tuberculosis. Int. J. Tuberc. Lung Dis. 2007, 11, 474–484. [Google Scholar] [PubMed]
- Sonnenberg, P.; Glynn, J.R.; Fielding, K.; Murray, J.; Godfrey-Faussett, P.; Shearer, S. How soon after infection with HIV does the risk of tuberculosis start to increase? A retrospective cohort study in South African gold miners. J. Infect. Dis. 2005, 191, 150–158. [Google Scholar] [CrossRef] [PubMed]
- Bermúdez-Lugo, O. The Mineral Industry of Ghana. Available online: http://minerals.usgs.gov/minerals/pubs/country/2006/myb3-2006-gh.pdf (accessed on 12 December 2016).
- Mamuya, S.H.D.; Moen, B.; Bråtveit, M. Quartz exposure and increased respiratory symptoms among coal mine workers in Tanzania. East Afr. J. Public Health 2011, 8, 190–195. [Google Scholar] [PubMed]
- Mamuya, S.H.D.; Bråtveit, M.; Mashalla, Y.; Moen, B.E. High prevalence of respiratory symptoms among workers in the development section of a manually operated coal mine in a developing country: A cross sectional study. BMC Public Health 2007, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Naidoo, R.N.; Robins, T.G.; Seixas, N.; Lalloo, U.G.; Becklake, M. Respirable coal dust exposure and respiratory symptoms in South-African coal miners: A comparison of current and ex-miners. J. Occup. Environ. Med. 2006, 48, 581–590. [Google Scholar] [CrossRef] [PubMed]
- Cowie, R.L.; Mabena, S.K. Silicosis, Chronic airflow limitation, and chronic bronchitis in South African gold miners. Am. Rev. Respir. Dis. 1991, 143, 80–84. [Google Scholar] [CrossRef] [PubMed]
- Henneberger, P.K.; Attfield, M.D. Respiratory symptoms and spirometry in experienced coal miners: Effects of both distant and recent coal mine dust exposures. Am. J. Ind. Med. 1997, 32, 268–274. [Google Scholar] [CrossRef]
- Seixas, N.S.; Robins, T.G.; Attfield, M.D.; Moulton, L.H. Exposure-response relationships for coal mine dust and obstructive lung disease following enactment of the federal coal mine health and safety act of 1969. Am. J. Ind. Med. 1992, 21, 715–734. [Google Scholar] [CrossRef] [PubMed]
- Kibelstis, J.A.; Morgan, E.J.; Reger, R.; Lapp, N.L.; Seaton, A.; Morgan, W.K. Prevalence of bronchitis and airway obstruction in American bituminous coal miners. Am. Rev. Respir. Dis. 1973, 108, 886–893. [Google Scholar] [PubMed]
- Marine, W.M.; Gurr, D.; Jacobsen, M. Clinically important respiratory effects of dust exposure and smoking in British coal miners. Am. Rev. Respir. Dis. 1988, 137, 106–112. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Yu, I.T.; Wong, T.W.; Yano, E. Respiratory symptoms and pulmonary function in coal miners: Looking into the effects of simple pneumoconiosis. Am. J. Ind. Med. 1999, 35, 124–131. [Google Scholar] [CrossRef]
- Carlos, A. World’s Top 10 Gold Deposits. Available online: http://www.mining.com/web/worlds-top-10-gold-deposits/ (accessed on 26 February 2017).
- Anglogold Ashanti. Country Report Ghana—Obuasi; Anglogold Ashanti: Obuasi, Ghana, 2009. [Google Scholar]
- Oxman, A.D.; Muir, D.C.; Shannon, H.S.; Stock, S.R.; Hnizdo, E.; Lange, H.J. Occupational dust exposure and chronic obstructive pulmonary disease: A systematic overview of the evidence. Am. Rev. Respir. Dis. 1993, 148, 38–48. [Google Scholar] [CrossRef] [PubMed]
- Naidoo, R.N.; Robins, T.G.; Murray, J. Respiratory Outcomes among South African coal miners at Autopsy. Am. J. Ind. Med. 2005, 48, 217–224. [Google Scholar] [CrossRef] [PubMed]
- Mehrotra, A.; Oluwole, A.M.; Gordon, S.B. The burden of COPD in Africa: A literature review and prospective survey of the availability of spirometry for COPD diagnosis in Africa. Trop. Med. Int. Health 2009, 14, 840–848. [Google Scholar] [CrossRef] [PubMed]
- Bio, F.Y.; Sadhra, S.; Jackson, C.; Burge, P.S. Respiratory symptoms and lung function impairment in underground gold miners in Ghana. Ghana Med. J. 2007, 41, 38–47. [Google Scholar] [CrossRef]
- Ball, P.; Make, B. Acute exacerbations of chronic bronchitis: An international comparison. Chest 1998, 113, 199S–204S. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.R.; Christiani, D.C. Respiratory symptoms and functional status in workers exposed to silica, asbestos, and coal mine dusts. J. Occup. Environ. Med. 2000, 42, 1076–1084. [Google Scholar] [CrossRef] [PubMed]
- Last, J. A Dictionary of Epidemiology; Oxford University Press: Oxford, UK, 1995. [Google Scholar]
- National Institute for Occupational Safety and Health. Coal Mine Dust Exposures and Associated Health Outcomes; National Institute for Occupational Safety and Health: Washington, DC, USA, 2011. [Google Scholar]
- National Institute for Occupational Safety and Health. Current Intelligence Bulletin 64: Coal Mine Dust Exposures and Associated Health Outcomes—A Review of Information Published Since 1995. Available online: https://www.cdc.gov/niosh/docs/2011-172/ (accessed on 12 December 2016).
- Nkosi, V.; Wichmann, J.; Voyi, K. Chronic respiratory disease among the elderly in South Africa: Any association with proximity to mine dumps? Environ. Health 2015, 14. [Google Scholar] [CrossRef] [PubMed]
- Kamal, A.; Malik, R.N. Hematological evidence of occupational exposure to chemicals and other factors among auto-repair workers in Rawalpindi, Pakistan. Osong Public Health Res. Perspect. 2012, 3, 229–238. [Google Scholar] [CrossRef] [PubMed]
- Armah, F.A.; Boamah, S.A.; Quansah, R.; Obiri, S.; Luginaah, I. Unsafe occupational health behaviors: Understanding mercury-related environmental health risks to artisanal gold miners in Ghana. Front. Environ. Sci. 2016, 4, 1–16. [Google Scholar] [CrossRef]
- Rugulies, R. Studying the effect of the psychosocial work environment on risk of ill-health: Towards a more comprehensive assessment of working conditions. Scand. J. Work Environ. Health 2012, 38, 187–191. [Google Scholar] [CrossRef]
- Gamble, L.; Mason, C.M.; Nelson, S. The effects of alcohol on immunity and bacterial infection in the lung. Méd. Maladies Infect. 2006, 36, 72–77. [Google Scholar] [CrossRef] [PubMed]
- Laney, A.S.; Weissman, D.N. Respiratory diseases caused by coal mine dust. J. Occup. Environ. Med. 2014, 56, S18–S22. [Google Scholar] [CrossRef] [PubMed]
- Viegas, S.; Faísca, V.M.; Dias, H.; Clérigo, A.; Carolino, E.; Viegas, C. Occupational exposure to poultry dust and effects on the respiratory system in workers. J. Toxicol. Environ. Health A 2013, 76, 230–239. [Google Scholar] [CrossRef] [PubMed]
- Davis, R.E.; Rossier, C.E.; Enfield, K.B. The impact of weather on influenza and pneumonia mortality in New York City, 1975–2002: A retrospective study. PLoS ONE 2012, 7, e34091. [Google Scholar]


{kind=link}
{kind=link}
{kind=link}
| Variables | Frequency N = 1001 | Percentage |
|---|---|---|
| Age, years | ||
| <30 | 149 | 14.9 |
| 30–40 | 686 | 68.5 |
| 40–50 | 135 | 13.5 |
| >50 | 31 | 3.1 |
| Median (range) | 35 (20–73) | |
| Religion | ||
| Christianity | 774 | 77.3 |
| Islamic | 215 | 21.5 |
| Traditional/other | 12 | 1.2 |
| Marital status | ||
| Married/living together | 854 | 85.3 |
| Single | 137 | 13.7 |
| Divorced/separated | 10 | 1.0 |
| Number of children | ||
| 1 | 100 | 10.0 |
| 2 | 145 | 14.5 |
| 3 | 296 | 29.6 |
| 4 and above | 460 | 45.9 |
| Mean (SD) | 3 (1.4) | |
| Nationality | 878 | 87.7 |
| Ghanaian | 21 | 2.1 |
| Non-Ghanaian | 102 | 10.2 |
| Educational level | ||
| Junior Secondary | 466 | 46.5 |
| Senior Secondary | 376 | 37.6 |
| Diploma | 75 | 7.5 |
| Tertiary | 84 | 8.4 |
| Employment status | ||
| Permanent staff | 829 | 82.8 |
| Temporary staff | 107 | 10.7 |
| Contract | 48 | 4.8 |
| Other | 17 | 1.7 |
| Smoke cigarette | 22 | 2.2 |
| Drink alcohol | 534 | 53.3 |
| Variables | Frequency | Percentage |
|---|---|---|
| Job category | ||
| Tunneling areas | 274 | 27.4 |
| Mining areas | 121 | 12.1 |
| Combining areas | 110 | 11.0 |
| Helping areas | 314 | 31.3 |
| Managerial and others | 182 | 18.2 |
| Duration of work, years; mean (SD) | 13.1 (6.8) | |
| Range | 1.0–47.0 | |
| Hours spent at work per day, mean (SD) | 11.9 (0.6) | |
| Range | 2.0–14.0 | |
| Worked in environment predisposed to dust | 935 | 93.4 |
| Work in high/low temperature conditions | 895 | 89.4 |
| Place bath before going home after days work | ||
| Bathroom at workplace | 837 | 83.6 |
| Home | 164 | 16.4 |
| Who washes working clothes | ||
| Yourself | 853 | 85.2 |
| Family | 123 | 12.3 |
| Company laundry service | 8 | 0.8 |
| Other | 17 | 1.7 |
| Where eat at work place | ||
| Worker’s canteen | 953 | 95.2 |
| At the work place | 46 | 4.6 |
| Somewhere far off | 2 | 0.2 |
| Experienced flooding while on duty | 833 | 83.2 |
| Variables | Asthma | Pneumonia | Bronchitis | Emphysema | ||||
|---|---|---|---|---|---|---|---|---|
| N = 375 | N = 143 | N = 97 | N = 51 | |||||
| % Affected | p-Value | % Affected | p-Value | % Affected | p-Value | % Affected | p-Value | |
| Age | <0.001 | <0.001 | 0.006 | 0.001 | ||||
| 30 | 44.3 | 2.0 | 14.8 | 2.7 | ||||
| 30–40 | 52.9 | 17.6 | 7.6 | 4.2 | ||||
| 40–50 | 27.4 | 12.6 | 12.6 | 11.9 | ||||
| >50 | 32.3 | 6.5 | 19.4 | 6.5 | ||||
| Educational level | <0.001 | <0.001 | 0.008 | 0.043 | ||||
| Junior Secondary | 48.1 | 20.6 | 5.8 | 6.4 | ||||
| Senior Secondary | 55.6 | 7.8 | 12.4 | 4.0 | ||||
| Diploma | 40.0 | 5.3 | 10.7 | 0.0 | ||||
| Tertiary | 29.8 | 13.1 | 11.9 | 2.4 | ||||
| Employment status | 0.460 | 0.001 | 0.197 | <0.001 | ||||
| Permanent staff | 48.3 | 16.8 | 5.4 | 4.2 | ||||
| Temporary staff | 43.0 | 3.7 | 7.5 | 6.5 | ||||
| Contract/other | 41.7 | 0.0 | 0.0 | 16.1 | ||||
| Smoking | 0.481 | 0.077 | 0.173 | 0.389 | ||||
| Yes | 9.1 | 13.6 | 18.2 | 9.1 | ||||
| No | 14.4 | 5.1 | 9.5 | 5.0 | ||||
| Drink alcohol | 0.130 | <0.001 | 0.009 | 0.003 | ||||
| Yes | 44.6 | 0.130 | 23.0 | 7.1 | 7.3 | |||
| No | 51.0 | 4.3 | 12.7 | 2.6 | ||||
| Variables | Asthma | Pneumonia | Bronchitis | Emphysema | ||||
|---|---|---|---|---|---|---|---|---|
| % Affected | p-Value | % Affected | p-Value | % Affected | p-Value | % Affected | p-Value | |
| Job category | 0.143 | 0.837 | 0.324 | 0.587 | ||||
| Tunneling areas | 45.3 | 15.3 | 7.7 | 5.5 | ||||
| Mining areas | 47.9 | 14.0 | 9.9 | 4.1 | ||||
| Combining areas | 59.1 | 12.7 | 7.3 | 2.7 | ||||
| Helping areas | 46.4 | 15.3 | 10.2 | 6.4 | ||||
| Managerial and others | 45.6 | 12.1 | 13.2 | 4.4 | ||||
| Duration of work, years | 0.027 | <0.001 | 0.120 | 0.157 | ||||
| <5 | 39.0 | 9.1 | 18.2 | 9.1 | ||||
| 5–10 | 52.2 | 4.9 | 9.3 | 5.5 | ||||
| 10–15 | 25.9 | 22.2 | 11.1 | 3.7 | ||||
| 15–20 | 47.5 | 21.7 | 8.5 | 3.7 | ||||
| >20 | 42.6 | 11.8 | 10.3 | 8.8 | ||||
| Cumulative dust exposure, years | 0.549 | <0.001 | 0.561 | |||||
| <10 | 49.8 | 5.7 | 10.9 | 6.2 | ||||
| 10–20 | 46.4 | 21.9 | 8.9 | 3.4 | <0.001 | |||
| 20–30 | 44.3 | 11.5 | 9.8 | 3.3 | ||||
| ≥30 | 33.3 | 11.1 | 0.0 | 55.6 | ||||
| Level of dust exposure | 0.001 | 0.003 | <0.001 | 0.343 | ||||
| High | 49.1 | 15.2 | 0.003 | 25.8 | 7.6 | 0.343 | ||
| Low | 27.7 | 1.6 | 8.6 | 4.9 | ||||
| Work in high/low temperature conditions | <0.001 | 0.071 | <0.001 | 0.012 | ||||
| Yes | 50.9 | 15.0 | 8.5 | 5.7 | ||||
| No | 18.9 | 8.5 | 19.8 | 0.0 | ||||
| Place bath after work | <0.001 | <0.001 | <0.001 | 0.193 | ||||
| Bathroom at workplace | 50.0 | 16.5 | 8.2 | 5.5 | ||||
| Home | 34.1 | 3.0 | 17.1 | 3.0 | ||||
| Where eat at work place | 0.005 | 0.018 | <0.001 | 0.258 | ||||
| Worker’s canteen | 48.7 | 13.6 | 9.1 | 5.4 | ||||
| At the work place/Somewhere far off | 26.1 | 28.3 | 17.4 | 0.0 | ||||
| Experienced flooding on duty | <0.001 | 0.004 | <0.001 | |||||
| Yes | 51.1 | 15.7 | 8.2 | 5.3 | ||||
| No | 29.8 | 7.1 | 17.3 | 4.2 | ||||
| Covariates | Asthma | Pneumonia | Bronchitis | Emphysema | ||||
|---|---|---|---|---|---|---|---|---|
| Model 1 | Model 2 | Model 1 | Model 2 | Model 1 | Model 2 | Model 1 | Model 2 | |
| OR [95% CI] | OR [95% CI] | OR [95% CI] | OR [95% CI] | OR [95% CI] | OR [95% CI] | OR [95% CI] | OR [95% CI] | |
| Socio-demographic characteristics and lifestyle | ||||||||
| Age | 1.08 [1.04, 1.13] *** | 1.12 [1.06, 1.19] *** | 1.04 [1.00, 1.08] * | 1.03 [0.98, 1.07] | 1.01 [0.98, 1.05] | 0.99 [0.94, 1.03] | 0.95 [0.93, 0.98] *** | 0.95 [0.92, 0.98] *** |
| Educational level (ref = JSS) | ||||||||
| Senior Secondary | 0.90 [0.44, 1.83] | 0.65 [0.29, 1.44] | 0.56 [0.38, 0.93] * | 0.60 [0.35, 1.03] | 1.01 [0.92, 3.50] | 1.06 [0.89, 3.40] | 1.31 [0.95, 1.80] | 1.46 [0.98, 2.05] |
| Diploma/Tertiary | 0.46 [0.10, 2.12] | 1.12 [0.17, 7.37] | 0.24 [0.08, 0.69] ** | 0.25 [0.08, 0.77] * | 1.59 [0.67, 3.81] | 1.48 [0.60, 3.64] | 0.85 [0.50, 1.44] | 1.09 [0.62, 1.99] |
| Married | 0.47 [0.20, 1.12] | 0.68 [0.27, 1.74] | 1.93 [0.87, 4.30] | 1.14 [0.59, 3.20] | 1.66 [0.78, 3.52] | 1.82 [0.82, 4.04] | 0.60 [0.37, 0.85] ** | 0.53 [0.34, 0.82] ** |
| Permanent employment status | 0.40 [0.20, 0.79] ** | 0.35 [0.17, 0.71] ** | 14.3 [4.6, 44.9] ** | 13.3 [4.19, 42.4] ** | 0.52 [0.30, 0.90] * | 0.60 [0.34, 1.06] | 1.23 [0.86, 1.75] | 1.23 [0.86, 1.75] |
| Smoking | 1.49 [0.32, 6.94] | 1.43 [0.30, 6.83] | 0.71 [0.15, 3.36] | 0.84 [0.17, 3.96] | 2.19 [0.69, 6.98] | 2.21 [0.69, 7.09] | 0.58 [0.23, 1.48] | 0.59 [0.23, 1.50] |
| Drink alcohol | 2.65 [1.41, 5.01] ** | 2.35 [1.25, 4.78] * | 5.05 [2.84, 8.95] *** | 5.29 [3.21, 8.72] *** | 0.65 [0.39, 1.08] | 0.83 [0.48, 1.42] | 0.88 [0.66, 1.18] | 0.72 [0.52, 0.98] * |
| Job and environmental exposures | ||||||||
| Job category (ref = Tunnelling areas) | ||||||||
| Mining areas | 0.54 [0.12, 1.72] | 1.41 [0.70, 2.84] | 1.04 [0.46, 2.31] | 1.24 [0.78, 1.97] | ||||
| Combining areas | 0.31 [0.07, 1.45] | 1.11 [0.54, 2.28] | 0.87 [0.37, 2.06] | 1.70 [1.06, 2.73] * | ||||
| Helping areas | 1.24 [0.59, 2.64] | 1.00 [0.61, 1.68] | 1.17 [0.64, 2.12] | 1.11 [0.78, 1.56] | ||||
| Managerial and others | 0.92 [0.34, 2.49] | 1.31 [0.70, 2.47] | 1.03 [0.51, 2.07] | 1.15 [0.76, 1.74] | ||||
| Duration of mining | 0.96 [0.91, 1.02] | 1.04 [1.00, 1.07] * | 0.97 [0.94, 1.01] | 1.04 [1.01, 1.06] ** | ||||
| Work in high/low temperature conditions | - | 4.62 [1.65, 12.96] ** | 1.99 [0.94, 4.26] | 1.86 [0.98, 2.35] | ||||
| Place bath after work (ref = Bathroom at workplace) | - | |||||||
| Home | - | - | 1.50 [0.57, 3.98] | 0.74 [0.33, 1.66] | ||||
| Where eat at work place (ref = Worker’s canteen) | ||||||||
| At the work place/Somewhere far off | 1.97 [0.43, 8.90] | 0.04 [0.01, 0.23] ** | 1.26 [0.58, 2.76] | 0.93 [0.55, 1.59] | ||||
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license ( http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ayaaba, E.; Li, Y.; Yuan, J.; Ni, C. Occupational Respiratory Diseases of Miners from Two Gold Mines in Ghana. Int. J. Environ. Res. Public Health 2017, 14, 337. https://doi.org/10.3390/ijerph14030337
Ayaaba E, Li Y, Yuan J, Ni C. Occupational Respiratory Diseases of Miners from Two Gold Mines in Ghana. International Journal of Environmental Research and Public Health. 2017; 14(3):337. https://doi.org/10.3390/ijerph14030337
Chicago/Turabian StyleAyaaba, Esther, Yan Li, Jiali Yuan, and Chunhui Ni. 2017. "Occupational Respiratory Diseases of Miners from Two Gold Mines in Ghana" International Journal of Environmental Research and Public Health 14, no. 3: 337. https://doi.org/10.3390/ijerph14030337