
Epidemiology of Fall Injury in Rural Bangladesh

Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Fatal Fall Injury
3.2 Non-Fatal Fall Injury
3.3. Factors Associated with Fatal Falls
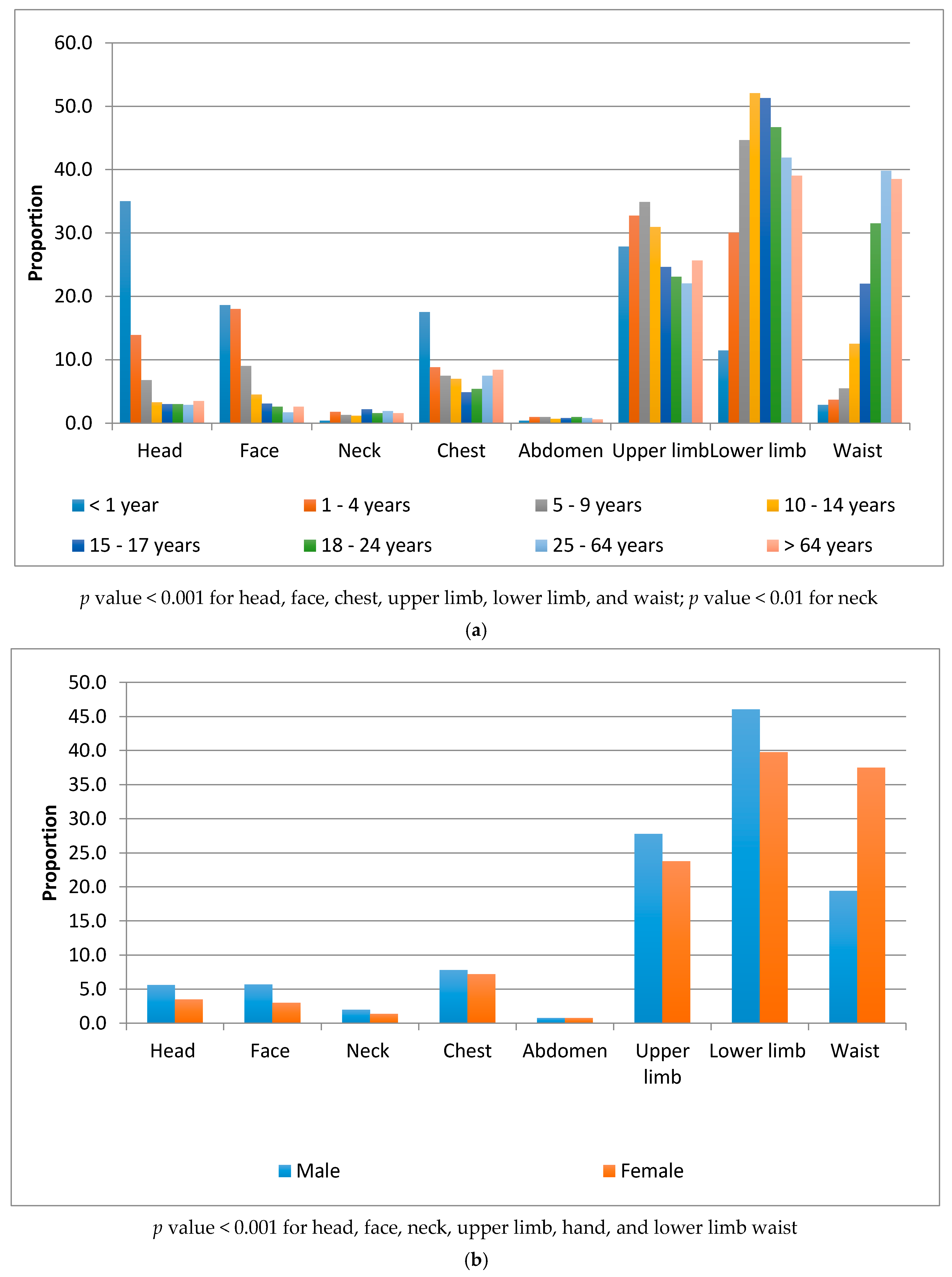
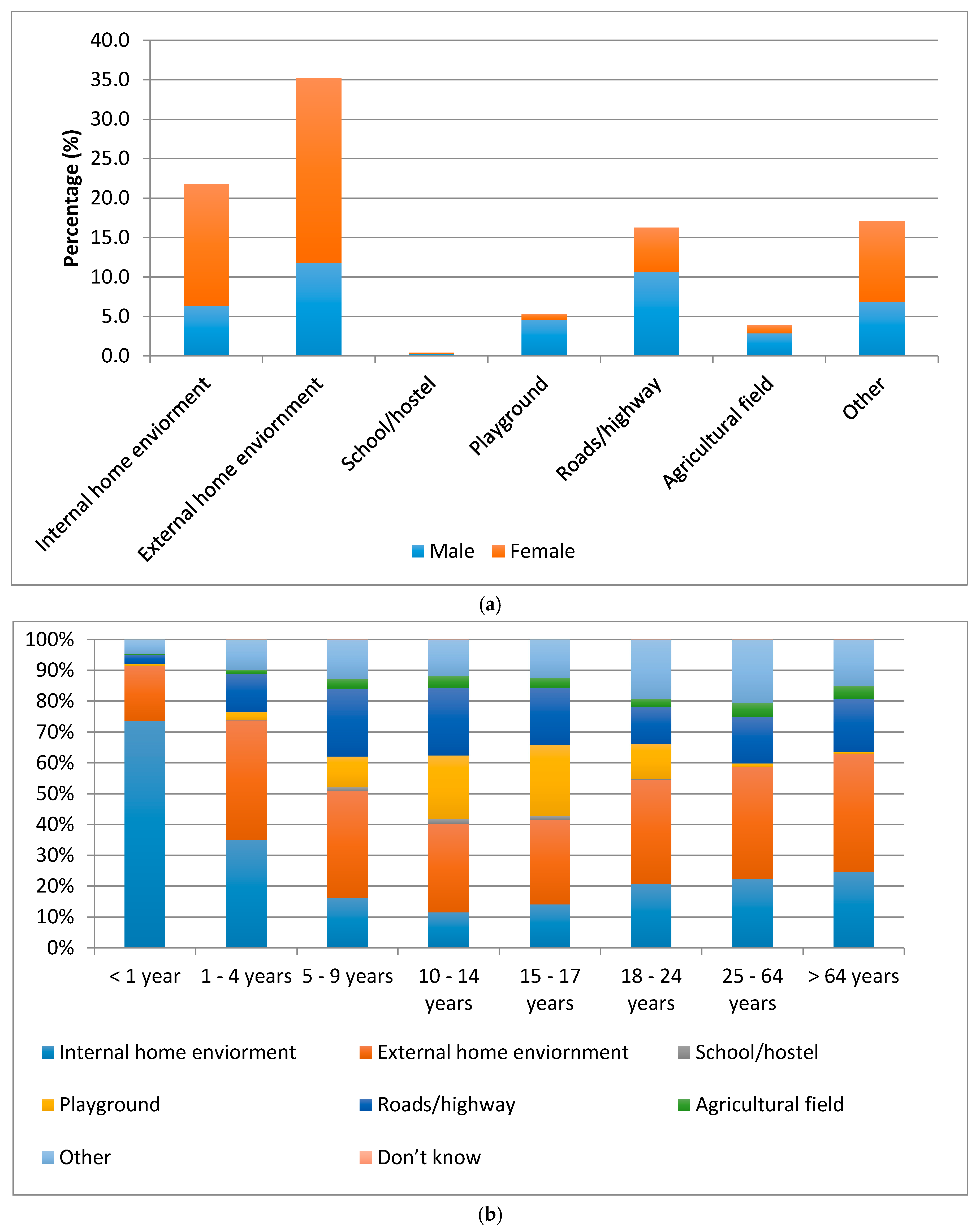
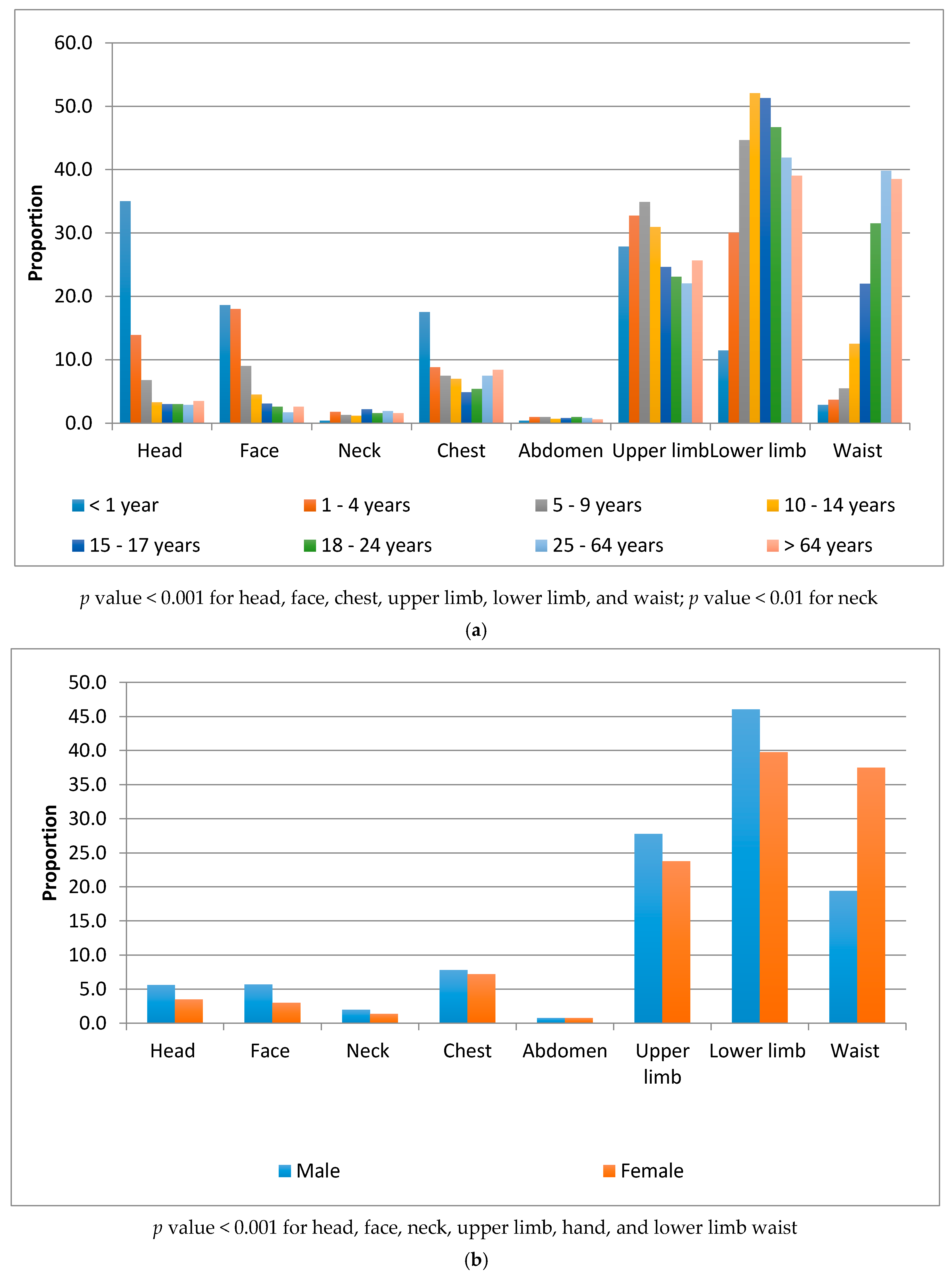
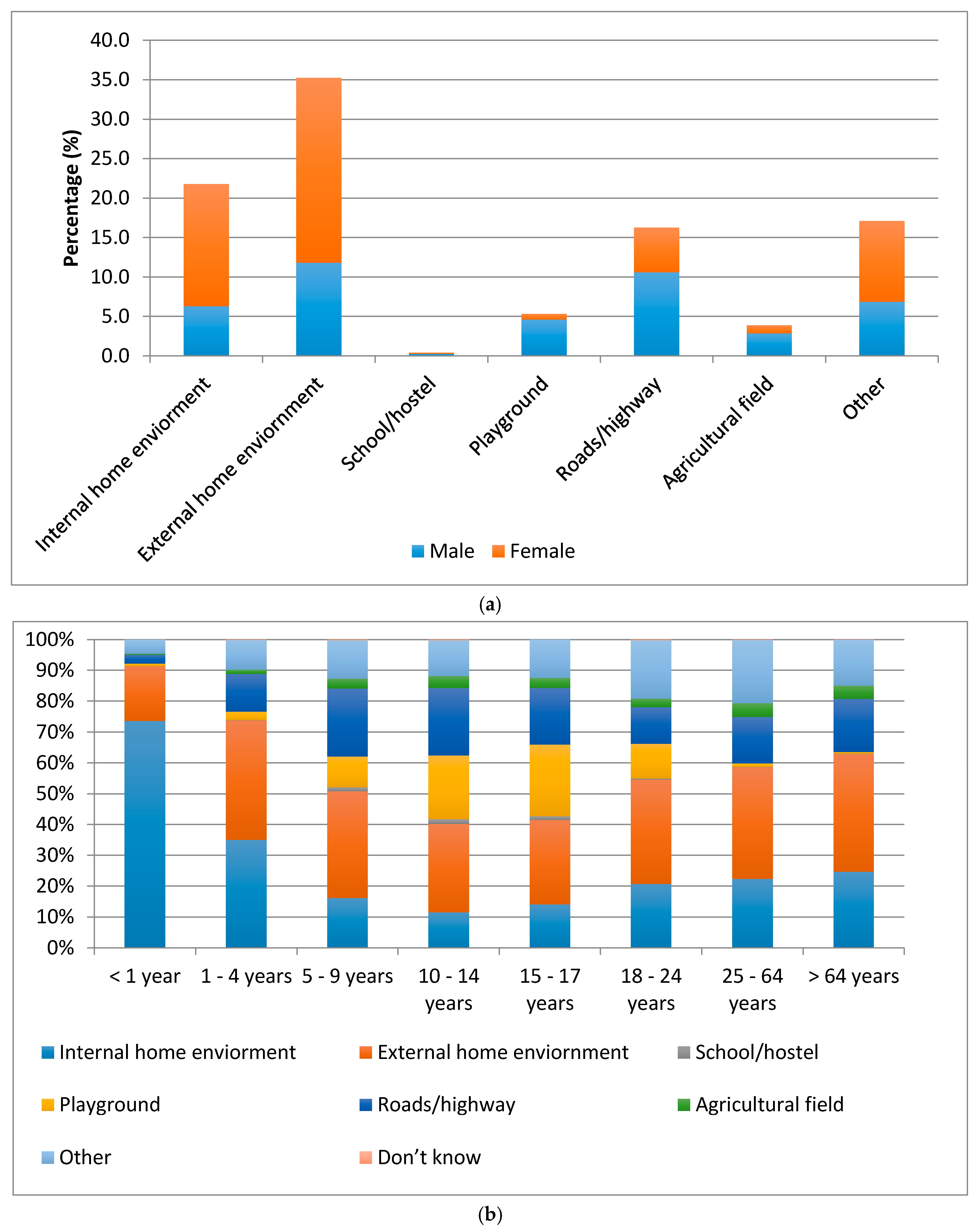
3.4. Factors Associated with Non-Fatal Falls
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| aOR | Adjusted odds ratio |
| CIPRB | Center for Injury Prevention and Research, Bangladesh |
| CI | Confidence interval |
| icddr, b | International Center for Diarrhoeal Disease Research, Bangladesh |
| JHSPH | Johns Hopkins Bloomberg School of Public Health |
| LMIC | Low-and middle-income countries |
| MLR | Multivariate logistic regressions |
| OR | Odds ratio |
| SES | Socioeconomic status |
| YLD | Years lived with disability |
References
- GBD 2015 Mortality and Causes of Death Collaborators. Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1459–1544. [Google Scholar]
- Falls: Fact Sheet. Available online: http://www.who.int/mediacentre/factsheets/fs344/en/ (accessed on 18 April 2016).
- Chandran, A.; Hyder, A.A.; Peek-Asa, C. The global burden of unintentional injuries and an agenda for progress. Epidemiol. Rev. 2010, 32, 110–120. [Google Scholar] [CrossRef] [PubMed]
- Injuries and Violence: The Facts 2014; World Health Organization: Geneva, Switzerland, 2014; Available online: http://apps.who.int/iris/bitstream/10665/149798/1/9789241508018_eng.pdf (accessed on 22 July 2013).
- WHO Global Report on Falls Prevention in Older Age; World Health Organization: Geneva, Switzerland, 2007; Available online: http://www.who.int/ageing/publications/Falls_prevention7March.pdf (accessed on 25 March 2014).
- Hyder, A.A.; Sugerman, D.E.; Puvanachandra, P.; Razzak, J.; El-Sayed, H.; Isaza, A.; Rahman, F.; Peden, M. Global childhood unintentional injury surveillance in four cities in developing countries: A pilot study. Bull. World Health Organ. 2009, 87, 345–352. [Google Scholar] [CrossRef] [PubMed]
- He, S.; Lunnen, J.C.; Puvanachandra, P.; Amar-Singh; Zia, N.; Hyder, A.A. Global childhood unintentional injury study: Multisite surveillance data. Am. J. Public Health 2014, 103, e79–84. [Google Scholar] [CrossRef] [PubMed]
- Prevention of Injuries and Disabilities. Available online: http://www.searo.who.int/bangladesh/areas/injuriesanddisabilities/en/ (accessed on 10 September 2016).
- Rahman, A.; Rahmna, A.F.; Shafinaz, S.; Linnan, M. Bangladesh Health and Injury Survey Report on Children. Available online: https://www.unicef.org/bangladesh/Bangladesh_Health_and_Injury_Survey-Report_on_Children.pdf (accessed on 27 April 2016).
- Chowdhury, S.M.; Rahman, A.; Mashreky, S.R.; Giashuddin, S.M.; Svanstrm, L.; Hrte, L.G.; Rahman, F. The horizon of unintentional injuries among children in low-income setting: An overview from Bangladesh health and injury survey. J. Environ. Public Health 2009. [Google Scholar] [CrossRef] [PubMed]
- Rahman, F.; Andersson, R.; Svanström, L. Health impact of injuries: A population-based epidemiological investigation in a local community of Bangladesh. J. Saf. Res. 1998, 29, 213–222. [Google Scholar] [CrossRef]
- Hyder, A.A.; Alonge, O.; He, S.; Wadhwaniya, S.; Rahman, F.; Rahman, A.; Arifeen, S.E. A framework for addressing implementation gap in global drowning prevention interventions: Experiences from Bangladesh. J. Health Popul. Nutr. 2014, 32, 564–576. [Google Scholar] [PubMed]
- Hyder, A.A.; Alonge, O.; He, S.; Wadhwaniya, S.; Rahman, F.; Rahman, A.; Arifeen, S.E. Saving of children’s lives from drowning project in Bangladesh. Am. J. Prev. Med. 2014, 47, 842–845. [Google Scholar] [CrossRef] [PubMed]
- He, S.; Alonge, O.; Agrawal, P.; Sharmin, S.; Islam, I.; Mashreky, S.R.; Arifeen, S.E. Epidemiology of burns in rural Bangladesh: An update. Int. J. Environ. Res. Public Health 2017, 14, 381. [Google Scholar] [CrossRef] [PubMed]
- Armitage, P.; Berry, G.; Mathhews, J.N.S. Statistical Methods in Medical Research, 4th ed.; Blackwell Science: Oxford, UK, 2002. [Google Scholar]
- StataCorp. Stata: Release 12; StataCorp LP: College Station, TX, USA, 2011. [Google Scholar]
- Chowdhury, S.M.; Rahman, A.; Mashreky, S.R.; Giashuddin, S.; Svanslröm, L.; Hörte, L.G.; Linnan, M.; Shafinaz, S.; Uhaa, I.J.; Rahman, A.K.M.F. Childhood fall: Epidemiologic findings from a population-based survey in Bangladesh. Int. J. Disabil. Hum. Dev. 2008, 7, 81–87. [Google Scholar] [CrossRef]
- Chowdhury, S.M.; Svanström, L.; Hörte, L.G.; Chowdhury, R.A.; Rahman, F. Children’s perceptions about falls and their prevention: A qualitative study from a rural setting in Bangladesh. BMC Public Health 2013. [Google Scholar] [CrossRef] [PubMed]
- World Bank Open Data. Available online: http://data.worldbank.org (accessed on 10 September 2016).
- Jagnoor, J.; Keay, L.; Ivers, R. A slip and a trip? Falls in older people in Asia. Injury 2013, 44, 701–702. [Google Scholar] [CrossRef] [PubMed]
- Chang, J.T.; Morton, S.C.; Rubenstein, L.Z.; Mojica, W.A.; Maglione, M.; Suttorp, M.J.; Roth, E.A.; Shekelle, P.G. Interventions for the prevention of falls in older adults: Systematic review and meta-analysis of randomised clinical trials. BMJ 2004, 328, 680. [Google Scholar] [CrossRef] [PubMed]
- Jagnoor, J.; Keay, L.; Jaswal, N.; Kaur, M.; Ivers, R. A qualitative study on the perceptions of preventing falls as a health priority among older people in Northern India. Inj. Prev. 2014, 20, 29–34. [Google Scholar] [CrossRef] [PubMed]
- Romli, M.H.; Tan, M.P.; Mackenzie, L.; Lovarini, M.; Suttanon, P.; Clemson, L. Falls amongst older people in Southeast Asia: A scoping review. Public Health 2017, 145, 96–112. [Google Scholar] [CrossRef] [PubMed]
- Bachani, A.M.; Ghaffar, A.; Hyder, A.A. Burden of fall injuries in Pakistan—Analysis of the national injury survey of Pakistan. East Mediterr. Health J. 2011, 17, 375–381. [Google Scholar] [PubMed]
- Pant, P.R.; Towner, E.; Pilkington, P.; Ellis, M. Epidemiology of unintentional child injuries in the South-East Asia Region: A systematic review. Int. J. Inj. Control Saf. Promot. 2015, 22, 24–32. [Google Scholar] [CrossRef] [PubMed]
- Moshiro, C.; Heuch, I.; Åstrøm, A.N.; Setel, P.; Hemed, Y.; Kvåle, G. Injury morbidity in an urban and a rural area in Tanzania: An epidemiological survey. BMC Public Health 2005. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fayyaz, J.; Wadhwaniya, S.; Shahzad, H.; Feroze, A.; Zia, N.; Mir, M.U.; Khan, U.R.; Iram, S.; Ali, S.; Razzak, J.A.; et al. Pattern of fall injuries in Pakistan: The Pakistan National Emergency Department Surveillance (Pak-NEDS) study. BMC Emerg. Med. 2015. [Google Scholar] [CrossRef] [PubMed]
- Shields, B.J.; Burkett, E.; Smith, G.A. Epidemiology of balcony fall-related injuries, United States, 1990–2006. Am. J. Emerg. Med. 2011, 29, 174–180. [Google Scholar] [CrossRef] [PubMed]
- Stewart Williams, J.; Kowal, P.; Hestekin, H.; O’Driscoll, T.; Peltzer, K.; Yawson, A.; Biritwum, R.; Maximova, T.; Salinas Rodríguez, A.; Manrique Espinoza, B.; et al. Prevalence, risk factors and disability associated with fall-related injury in older adults in low-and middle-incomecountries: Results from the WHO Study on global AGEing and adult health (SAGE). BMC Med. 2015. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Fatal Fall Injury (N = 59) | p Value | Non-Fatal Fall Injury (N = 42,259) | p Value | Total (N = 1,169,593) | |||
|---|---|---|---|---|---|---|---|
| N | Rate Per 100,000 Population (95% CI) | N | Rate Per 1000 Population (95% CI) | N (%) | |||
| Sub-district | |||||||
| Matlab North | 21 | 7.9 (4.5–11.3) | 0.030 * | 12,058 | 45.6 (44.8–46.4) | <0.001 *** | 265,897 (22.7) |
| Matlab South | 15 | 7.2 (3.5–10.8) | 11,435 | 54.8 (53.8–55.8) | 209,772 (17.9) | ||
| Chandpur Sadar | 3 | 2.3 (0.0–5.0) | 4570 | 35.8 (34.8–36.8) | 128,356 (11.0) | ||
| Raiganj | 2 | 1.9 (0.0–4.6) | 3554 | 34.3 (33.1–35.4) | 104,357 (8.9) | ||
| Sherpur Sadar | 8 | 3.5 (1.1–5.9) | 4059 | 17.9 (17.3–18.4) | 228,519 (19.5) | ||
| Manohardi | 7 | 3.4 (0.9–6.0) | 4680 | 23.0 (22.4–23.7) | 204,319 (17.5) | ||
| Daudkandi | 3 | 10.6 (0.0–22.5) | 1903 | 67.5 (64.6–70.5) | 28,373 (2.4) | ||
| Age group | |||||||
| <1 year | 0 | - | - | 280 | 13.0 (11.5–14.5) | <0.001 *** | 22,141 (1.9) |
| 1–4 years | 0 | - | 2927 | 32.5 (31.3–33.6) | 90,523 (7.7) | ||
| 5–9 years | 3 | 2.2 (0.0–4.6) | 4453 | 31.9 (31.0–32.8) | 139,728 (12.0) | ||
| 10–14 years | 1 | 0.7 (0.0–2.1) | 3848 | 27.1 (26.2–27.9) | 142,121 (12.2) | ||
| 15–17 years | 0 | - | 1435 | 23.1 (21.9–24.3) | 62,098 (5.3) | ||
| 18–24 years | 2 | 1.5 (0.0–3.6) | 2879 | 21.6 (20.8–22.4) | 133,534 (11.4) | ||
| 25–64 years | 14 | 2.8 (1.3–4.2) | 22,273 | 44.0 (43.4–44.6) | 508,059 (43.4) | ||
| >64 years | 39 | 54.6 (37.5–71.8) | 4164 | 61.0 (59.2–62.8) | 71,389 (6.1) | ||
| Sex | |||||||
| Male | 31 | 5.5 (3.5–7.4) | 0.538 | 18,312 | 32.4 (32.0–32.9) | <0.001 *** | 567,674 (48.5) |
| Female | 28 | 4.7 (2.9–6.4) | 23,947 | 40.0 (39.5–40.5) | 601,919 (51.5) | ||
| Education | |||||||
| No education | 39 | 13.2 (9.1–17.4) | <0.001 *** | 12,608 | 43.2 (42.5–43.9) | <0.001 *** | 295,314 (25.3) |
| Primary | 10 | 2.5 (0.9–4.0) | 15,734 | 38.7 (38.1–39.2) | 407,923 (34.9) | ||
| Secondary | 8 | 2.8 (0.8–4.7) | 9228 | 31.9 (31.3–32.6) | 289,658 (24.8) | ||
| A levels | 1 | 2.2 (0.0–6.5) | 1079 | 23.7 (22.3–25.1) | 45,618 (3.9) | ||
| College | 0 | - | 299 | 22.2 (19.7–24.7) | 13,526 (1.2) | ||
| Advanced/Professional degree | 0 | - | 100 | 21.3 (17.2–25.4) | 4729 (0.4) | ||
| Not applicable (under 5 children) | 0 | - | 3207 | 28.7 (27.7–29.7) | 112,664 (9.6) | ||
| Marital status | |||||||
| Married | 33 | 5.8 (3.8–7.8) | <0.001 *** | 23,845 | 42.0 (41.5–42.5) | <0.001 *** | 571,206 (48.8) |
| Never married | 2 | 0.9 (0.0–2.1) | 5052 | 22.2 (21.6–22.9) | 227,319 (19.4) | ||
| Divorced | 0 | - | 116 | 36.3 (29.8–42.8) | 3220 (0.3) | ||
| Widowed | 20 | 37.7 (21.2–54.2) | 3695 | 71.6 (69.3–73.8) | 53,096 (4.5) | ||
| Separated | 0 | - | 128 | 47.4 (39.4–55.4) | 2717 (0.2) | ||
| Not applicable | 4 | 1.3 (0.0–2.5) | 9423 | 30.3 (29.7–30.9) | 312,035 (26.7) | ||
| Occupation | |||||||
| Agriculture | 9 | 8.6 (3.0–14.2) | - | 3440 | 33.1 (32.1–34.2) | <0.001 *** | 104,956 (9.0) |
| Business | 3 | 4.9 (0.0–10.4) | 1518 | 24.8 (23.5–26.0) | 61,661 (5.3) | ||
| Skilled labor (Professional) | 5 | 5.6 (0.7–10.5) | 2250 | 25.3 (24.3–26.4) | 89,151 (7.6) | ||
| Unskilled/domestic labor | 0 | - | 894 | 36.6 (34.3–39.0) | 24,520 (2.1) | ||
| Rickshaw/bus (transport worker) | 1 | 5.9 (0.0–17.4) | 445 | 26.2 (23.8–28.6) | 17,037 (1.5) | ||
| Students | 3 | 1.0 (0.0–2.1) | 8580 | 27.5 (26.9–28.0) | 312,537 (26.7) | ||
| Retired/unemployed/housewife | 36 | 8.8 (5.9–11.7) | 20,716 | 51.1 (50.4–51.7) | 408,583 (34.9) | ||
| Not applicable (children) | 0 | - | 4195 | 29.3 (28.4–30.1) | 144,454 (12.4) | ||
| Not applicable (others) | 2 | 33.6 (0.0–80.2) | 195 | 33.7 (29.1–38.4) | 5948 (0.5) | ||
| Socioeconomic status | |||||||
| Lowest | 7 | 3.3 (0.9–5.8) | 0.653 | 7714 | 36.7 (35.9–37.5) | <0.001 *** | 211,601 (18.1) |
| Low | 11 | 5.0 (2.1–8.0) | 7927 | 36.4 (35.6–37.2) | 218,695 (18.7) | ||
| Middle | 11 | 4.6 (1.9–7.3) | 9051 | 38.2 (37.4–39.0) | 238,371 (20.4) | ||
| High | 16 | 6.5 (3.3–9.6) | 9051 | 36.7 (36.0–37.4) | 247,716 (21.2) | ||
| Highest | 14 | 5.5 (2.6–8.4) | 8516 | 33.8 (33.1–34.5) | 253,201 (21.7) | ||
| Unadjusted | Adjusted ^ | |||
|---|---|---|---|---|
| Odds Ratio (95% CI) | p Value | Odds Ratio (95% CI) | p Value | |
| Sub-district | ||||
| Matlab North | 1 | - | 1 | - |
| Matlab South | 0.9 (0.5–1.8) | 0.769 | 1.0 (0.5–1.9) | 0.976 |
| Chandpur Sadar | 0.3 (0.1–1.0) | 0.049 * | 0.4 (0.1–1.2) | 0.111 |
| Raiganj | 0.2 (0.1–1.0) | 0.056 | 0.3 (0.1–1.2) | 0.098 |
| Sherpur Sadar | 0.4 (0.2–1.0) | 0.050 | 0.6 (0.3–1.4) | 0.229 |
| Manohardi | 0.4 (0.2–1.0) | 0.056 | 0.5 (0.2–1.2) | 0.123 |
| Daudkandi | 1.3 (0.4–4.5) | 0.636 | 1.4 (0.4–4.3) | 0.567 |
| Age group | ||||
| <18 years | 1 | - | 1 | - |
| 18–24 years | 1.7 (0.3–9.3) | 0.536 | 5.0 (0.1–333.1) | 0.456 |
| 25–64 years | 3.1 (1.0–9.6) | 0.043 * | 5.9 (0.1–500.6) | 0.431 |
| >64 years | 62.4 (22.3–174.6) | <0.001 *** | 71.7 (0.8–6285.6) | 0.061 |
| Sex | ||||
| Male | 1 | - | 1 | - |
| Female | 0.9 (0.5–1.4) | 0.538 | 0.5 (0.3–1.1) | 0.107 |
| Education | ||||
| No education (includes under 5 children) | 1 | - | 1 | - |
| Primary | 0.3 (0.1–0.5) | <0.001 *** | 0.4 (0.2–0.9) | 0.023 * |
| Secondary and higher | 0.3 (0.1–0.5) | <0.001 *** | 0.5 (0.2–1.1) | 0.099 |
| Marital status | ||||
| Married | 1 | - | 1 | - |
| Never married | 0.2 (0.0–0.6) | 0.010 ** | 1.5 (0.3–8.3) | 0.655 |
| Divorced/widowed/separated | 5.9 (3.4–10.2) | <0.001 *** | 2.1 (1.0–4.3) | 0.053 |
| Not applicable | 0.2 (0.1–0.6) | 0.004 ** | 11.1 (0.1–996.8) | 0.294 |
| Occupation | ||||
| Agriculture | 1 | - | 1 | - |
| Business | 0.6 (0.2–2.1) | 0.395 | 1.2 (0.3–4.2) | 0.784 |
| Skilled labor (Professional) | 0.7 (0.2–2.0) | 0.447 | 1.8 (0.6–5.7) | 0.291 |
| Unskilled/semi-skilled labor | 0.3 (0.0–2.2) | 0.228 | 0.8 (0.1–4.5) | 0.779 |
| Students | 0.1 (0.0–0.4) | 0.001 ** | 0.5 (0.0–5.7) | 0.598 |
| Retired/unemployed/housewife | 1.0 (0.5–2.1) | 0.942 | 1.1 (0.4–2.7) | 0.843 |
| Not applicable | 0.2 (0.0–0.7) | 0.017 * | 0.1 (0.0–1.9) | 0.138 |
| Socioeconomic status | ||||
| Lowest | 1 | 1 | ||
| Low | 1.5 (0.6–3.9) | 0.386 | 1.6 (0.6–4.2) | 0.303 |
| Middle | 1.4 (0.5–3.6) | 0.491 | 1.5 (0.6–3.9) | 0.362 |
| High | 2.0 (0.8–4.7) | 0.140 | 2.1 (0.9–5.2) | 0.094 |
| Highest | 1.7 (0.7–4.1) | 0.267 | 1.8 (0.7–4.6) | 0.203 |
| Unadjusted | Adjusted # | |||
|---|---|---|---|---|
| Odds Ratio (95% CI) | p Value | Odds Ratio (95% CI) | p Value | |
| Sub-district | ||||
| Matlab North | 1 | - | 1 | - |
| Matlab South | 1.2 (1.2–1.2) | <0.001 *** | 1.2 (1.2–1.3) | <0.001 *** |
| Chandpur Sadar | 0.8 (0.8–0.8) | <0.001 *** | 0.8 (0.8–0.8) | <0.001 *** |
| Raiganj | 0.7 (0.7–0.8) | <0.001 *** | 0.7 (0.7–0.8) | <0.001 *** |
| Sherpur Sadar | 0.4 (0.4–0.4) | <0.001 *** | 0.4 (0.4–0.4) | <0.001*** |
| Manohardi | 0.5 (0.5–0.5) | <0.001 *** | 0.5 (0.5–0.5) | <0.001 *** |
| Daudkandi | 1.5 (1.4–1.6) | <0.001 *** | 1.5 (1.4–1.6) | <0.001 *** |
| Age group | ||||
| <1 year | 1 | - | 1 | - |
| 1–4 years | 2.5 (2.3–2.9) | <0.001 *** | 2.9 (2.4–3.4) | <0.001 *** |
| 5–9 years | 2.5 (2.2–2.8) | <0.001 *** | 1.1 (0.9–1.2) | 0.349 |
| 10–14 years | 2.1 (1.9–2.4) | <0.001 *** | 1.0 (0.9–1.1) | 0.640 |
| 15–17 years | 1.8 (1.6–2.0) | <0.001 *** | 0.9 (0.8–1.0) | 0.012 * |
| 18–24 years | 1.7 (1.5–1.9) | <0.001 *** | 0.7 (0.6–0.8) | <0.001 *** |
| 25–64 years | 3.5 (3.1–3.9) | <0.001 *** | 0.8 (0.7–0.8) | <0.001 *** |
| > 64 years | 4.9 (4.4–5.6) | <0.001 *** | - | - |
| Sex | ||||
| Male | 1 | - | 1 | - |
| Female | 1.2 (1.2–1.3) | <0.001 *** | 0.9 (0.7–1.2) | 0.550 |
| Education | ||||
| No education | 1 | - | 1 | - |
| Primary | 0.9 (0.9–0.9) | <0.001 *** | 1.1 (1.0–1.1) | <0.001 *** |
| Secondary | 0.7 (0.7–0.8) | <0.001 *** | 0.9 (0.9–0.9) | <0.001 *** |
| A levels | 0.5 (0.5–0.6) | <0.001 *** | 0.8 (0.7–0.8) | <0.001 *** |
| College | 0.5 (0.4–0.6) | <0.001 *** | 0.7 (0.6–0.8) | <0.001 *** |
| Advanced/Professional degree | 0.5 (0.4–0.6) | <0.001 *** | 0.6 (0.5–0.8) | <0.001 *** |
| Not applicable (under 5 children) | 0.7 (0.6–0.7) | <0.001 *** | 0.3 (0.3–0.4) | <0.001 *** |
| Marital status | ||||
| Married | 1 | - | 1 | - |
| Never married | 0.5 (0.5–0.5) | <0.001 *** | 0.6 (0.6–0.7) | <0.001 *** |
| Divorced | 0.9 (0.7–1.0) | 0.108 | 0.9 (0.7–1.0) | 0.115 |
| Widowed | 1.8 (1.7–1.8) | <0.001 *** | 1.2 (1.2–1.3) | <0.001 *** |
| Separated | 1.1 (0.9–1.4) | 0.165 | 1.1 (0.9–1.3) | 0.302 |
| Not applicable | 0.7 (0.7–0.7) | <0.001 *** | 0.7 (0.6–0.7) | <0.001 *** |
| Occupation | ||||
| Agriculture | 1 | - | 1 | - |
| Business | 0.7 (0.7–0.8) | <0.001 *** | 0.7 (0.7–0.8) | <0.001 *** |
| Skilled labor (Professional) | 0.8 (0.7–0.8) | <0.001 *** | 0.8 (0.8–0.8) | <0.001 *** |
| Unskilled/domestic labor | 1.1 (1.0–1.2) | 0.006 ** | 1.1 (1.0–1.2) | 0.029 * |
| Rickshaw/bus (transport worker) | 0.8 (0.7–0.9) | <0.001 *** | 0.8 (0.7–0.9) | <0.001 *** |
| Students | 0.8 (0.8–0.9) | <0.001 *** | 1.2 (1.1–1.3) | <0.001 *** |
| Retired/unemployed/housewife | 1.6 (1.5–1.6) | <0.001 *** | 1.1 (1.0–1.1) | 0.079 |
| Not applicable (children) | 0.9 (0.8–0.9) | <0.001 *** | 1.2 (1.1–1.3) | 0.001 ** |
| Not applicable (others) | 1.0 (0.9–0.2) | 0.807 | 1.3 (1.1–1.5) | 0.002 ** |
| Socioeconomic status | ||||
| Lowest | 1 | - | 1 | - |
| Low | 1.0 (1.0–1.0) | 0.650 | 1.0 (0.9–1.0) | 0.145 |
| Middle | 1.0 (1.0–1.1) | 0.009 ** | 1.0 (0.9–1.0) | 0.043 * |
| High | 1.0 (1.0–1.0) | 0.942 | 1.0 (0.9–1.0) | 0.002 * |
| Highest | 0.9 (0.9–0.9) | <0.001 *** | 0.9 (0.9–0.9) | <0.001 *** |
| Odds Ratio (95% CI) | p-Value | |
|---|---|---|
| <1 year female compared to <1 year male | 0.1 (0.0–0.1) | <0.001 *** |
| 1–4 years female compared to 1–4 years male | 2.7 (1.9–3.9) | <0.001 *** |
| 5–9 years female compared to 5–9 years male | 1.0 (0.8–1.3) | 0.894 |
| 10–14 years female compared to 10–14 years male | 1.0 (0.7–1.2) | 0.710 |
| 15–17 years female compared to 15–17 years male | 0.8 (0.6–1.1) | 0.115 |
| 18–24 years female compared to 18–24 years male | 0.7 (0.5–0.8) | 0.001 ** |
| 25–64 years female compared to 25–64 years male | 0.7 (0.6–0.9) | 0.006 ** |
| >65 years female compared to >65 years male | 0.9 (0.7–1.2) | 0.550 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wadhwaniya, S.; Alonge, O.; Ul Baset, M.K.; Chowdhury, S.; Bhuiyan, A.-A.; Hyder, A.A. Epidemiology of Fall Injury in Rural Bangladesh. Int. J. Environ. Res. Public Health 2017, 14, 900. https://doi.org/10.3390/ijerph14080900
Wadhwaniya S, Alonge O, Ul Baset MK, Chowdhury S, Bhuiyan A-A, Hyder AA. Epidemiology of Fall Injury in Rural Bangladesh. International Journal of Environmental Research and Public Health. 2017; 14(8):900. https://doi.org/10.3390/ijerph14080900
Chicago/Turabian StyleWadhwaniya, Shirin, Olakunle Alonge, Md. Kamran Ul Baset, Salim Chowdhury, Al-Amin Bhuiyan, and Adnan A. Hyder. 2017. "Epidemiology of Fall Injury in Rural Bangladesh" International Journal of Environmental Research and Public Health 14, no. 8: 900. https://doi.org/10.3390/ijerph14080900