Improved Housing Accessibility for Older People in Sweden and Germany: Short Term Costs and Long-Term Gains


Abstract
:1. Introduction
2. Materials and Methods
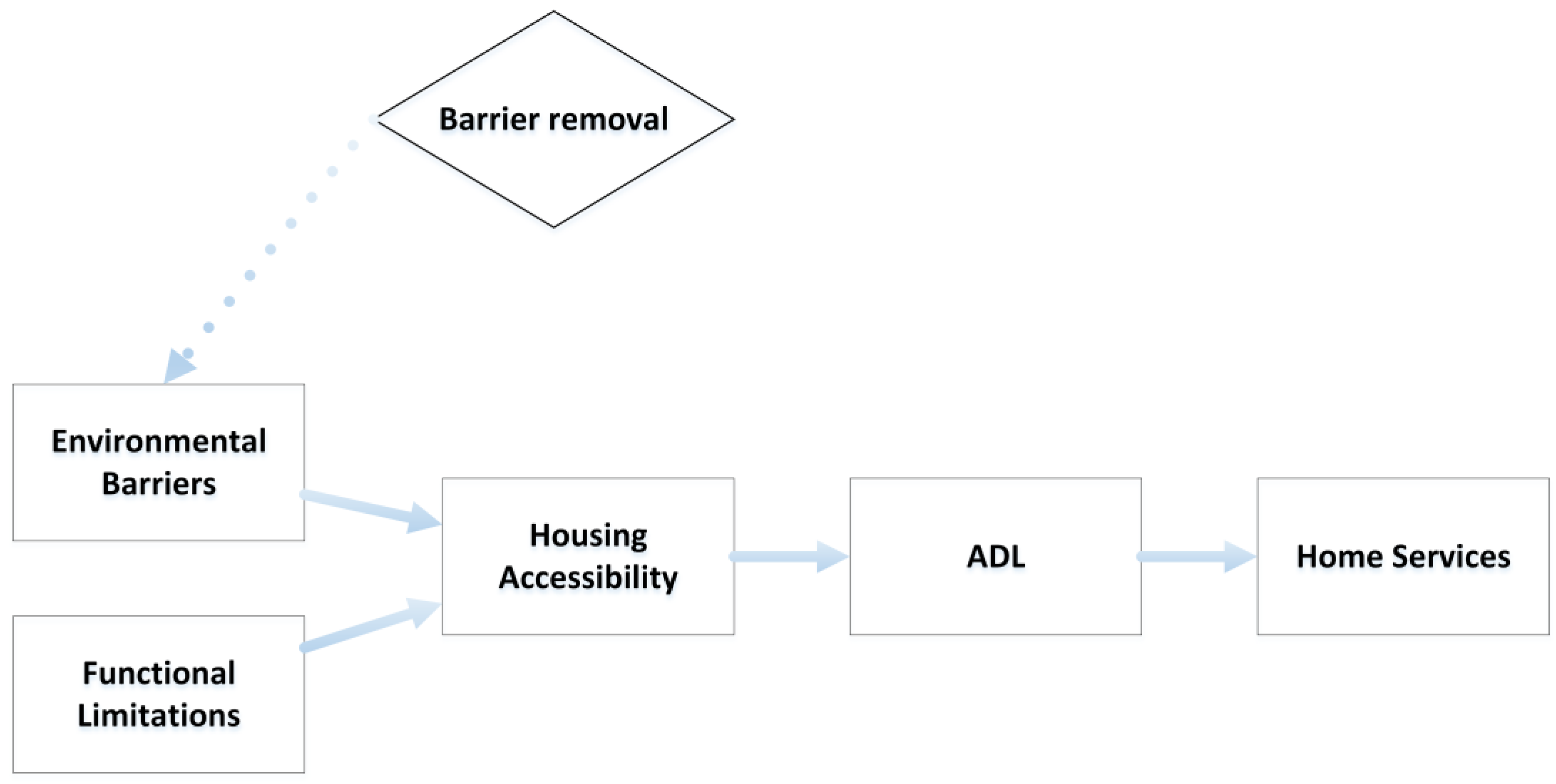
2.1. Theoretical Model
2.2. Data Sets and Variables
2.3. Simulation Methodology
- the most prominent barriers in the two national housing stocks;
- the association of accessibility problem score and I-ADL dependence;
- the overall reduction of accessibility problems following the barrier’s removal;
- the cost of the barrier removal policy;
- the potential savings (in terms of home care provision cost) related to the policy impact.
2.3.1. Step 1: Criteria to Prioritize Barriers for Removal
- the barriers should be located indoors or at entrances;
- the barriers should have high impact on the range of potential accessibility problems generated, i.e., generating problems in relation to several functional capacities, such as vision, movement, handling and gripping etc., as shown by Slaug and colleagues [25];
- the impact should also be potentially high in terms of severity, i.e., barriers more difficult to overcome, scoring at least 3 on the 1–4 scale;
- the barriers should be prevalent in ordinary housing, i.e., occurring in at least 33% of the surveyed dwellings.
2.3.2. Step 2: Estimating the Association between Housing Accessibility Problems and I-ADL Dependence Using ENABLE-AGE Data
2.3.3. Step 3: Simulating the Impact of Barrier Removal Policy Using ENABLE-AGE Data
2.3.4. Step 4: Estimating Potential Costs of the New Barrier Removal Policy
2.3.5. Step 5: Estimating Potential Savings
2.4. Ethical Approval
3. Results
3.1. Step 1: Barriers Prioritized for Removal
3.2. Step 2: Estimating the Relation between Accessibility Problem Score and I-ADL Dependence
3.3. Step 3: Simulating the Impact of the Policy on I-ADL
3.4. Step 4: Costs for Barrier Removal Policy
3.5. Step 5: Potential Savings
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- European Commission. Europe 2020: A Strategy for Smart, Sustainable and Inclusive Growth; European Commission: Brussels, Belgium, 2010. [Google Scholar]
- Oswald, F.; Wahl, H.W.; Schilling, O.; Nygren, C.; Fange, A.; Sixsmith, A.; Sixsmith, J.; Szeman, Z.; Tomsone, S.; Iwarsson, S. Relationships between housing and healthy aging in very old age. Gerontologist 2007, 47, 96–107. [Google Scholar] [CrossRef] [PubMed]
- Lawrence, R.J. Housing and health promotion: Moving forward. Int. J. Public Health 2010, 55, 145–146. [Google Scholar] [CrossRef] [PubMed]
- Lawton, M.P.; Nahemow, L. Ecology and the aging process. In The Psychology of Adult Development and Aging; Eisdorfer, C., Lawton, M.P., Eds.; American Psychological Association: Washington, DC, USA, 1973; pp. 619–674. [Google Scholar]
- Boverket. Handbook on Housing Adaptation Grants in Sweden; Boverket: Karlskrona, Sweden, 2000. [Google Scholar]
- Gitlin, L.N.; Winter, L.; Dennis, M.P.; Corcoran, M.; Schinfeld, S.; Hauck, W.W. A randomized trial of a multicomponent home intervention to reduce functional difficulties in older adults. J. Am. Geriatr. Soc. 2006, 54, 809–816. [Google Scholar] [CrossRef] [PubMed]
- Boverket. Bostadsanpassningsbidragen 2014. Available online: http://www.boverket.se/sv/om-boverket/publicerat-av-boverket/publikationer/2015/bostadsanpassningsbidragen-2014/ (accessed on 29 June 2017).
- Bundesinstitut für Bau-, Stadt- und Raumforschung. Potenzialanalyse Altersgerechte Wohnungs-Anpassung; Bundesamt für Bauwesen und Raumordnung: Bonn, Germany, 2014. [Google Scholar]
- Iwarsson, S.; Wahl, H.W.; Nygren, C.; Oswald, F.; Sixsmith, A.; Sixsmith, J.; Szeman, Z.; Tomsone, S. Importance of the home environment for healthy aging: Conceptual and methodological background of the european enable-age project. Gerontologist 2007, 47, 78–84. [Google Scholar] [CrossRef]
- Gitlin, L.N. Conducting research on home environments: Lessons learned and new directions. Gerontologist 2003, 43, 628–637. [Google Scholar] [CrossRef] [PubMed]
- Oswald, F.; Wahl, H.W. Creating and sustaining homelike places in own home environments. In Environmental Gerontology; Rowles, G.D., Bernard, M., Eds.; Springer: New York, NY, USA, 2013; pp. 53–77. [Google Scholar]
- Henning-Smith, C.; Shippee, T.; Capistrant, B. Later-life disability in environmental context: Why living arrangements matter. Gerontologist 2017. [Google Scholar] [CrossRef] [PubMed]
- Wahl, H.-W.; Fänge, A.; Oswald, F.; Gitlin, L.N.; Iwarsson, S. The home environment and disability-related outcomes in aging individuals: What is the empirical evidence? Gerontologist 2009, 49, 355–367. [Google Scholar] [CrossRef] [PubMed]
- Oswald, F.; Rowles, G.D. Beyond the relocation trauma in old age: New trends in today’s elders’ residential decisions. In New Dynamics in Old Age: Environmental and Societal Perspectives; Wahl, H.W., Tesch-Römer, C., Hoff, A., Eds.; Baywood Publ.: Amityville, NY, USA, 2006; pp. 127–152. [Google Scholar]
- Chiatti, C.; Iwarsson, S. Evaluation of housing adaptation interventions: Integrating the economic perspective into occupational therapy practice. Scand. J. Occup. Ther. 2014, 21, 323–333. [Google Scholar] [CrossRef] [PubMed]
- Iwarsson, S. Housing adaptations: Current practices and challenges for the future. In International Handbook of Occupational Therapy Interventions; Söderback, I., Ed.; Springer: New York, NY, USA, 2009; pp. 63–69. [Google Scholar]
- Schütze, B. SGB XI - Soziale Pflegeversicherung (13., überarbeitete Auflage, Stand: 11. Mai 2017); dtv: München, Germany, 2017. [Google Scholar]
- Kuratorium Deutsche Altershilfe (KDA). Wohnatlas; Eigenverlag: Köln, Germany, 2014. [Google Scholar]
- Bundesministerium für Verkehr, Bau und Stadtentwicklung (BMVBS). Stadtquartiere für Jung und Alt—Eine Zukunftsaufgabe; Eigenverlag: Berlin, Germany, 2010. [Google Scholar]
- Granbom, M.; Slaug, B.; Lofqvist, C.; Oswald, F.; Iwarsson, S. Community relocation in very old age: Changes in housing accessibility. Am. J. Occup. Ther. 2016, 70, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Sandberg, M.; Kristensson, J.; Midlov, P.; Fagerstrom, C.; Jakobsson, U. Prevalence and predictors of healthcare utilization among older people (60+): Focusing on adl dependency and risk of depression. Arch. Gerontol. Geriatr. 2012, 54, e349–e363. [Google Scholar] [CrossRef]
- Evashwick, C.; Rowe, G.; Diehr, P.; Branch, L. Factors explaining the use of health care services by the elderly. Health Serv. Res. 1984, 19, 357–382. [Google Scholar] [PubMed]
- Iwarsson, S.; Slaug, B. Housing Enabler: An Instrument for Assessing and Analysing Accessibility Problems in Housing; Veten & Skapen HB, Slaug Data Management: Nävlinge and Staffanstorp, Sweden, 2001. [Google Scholar]
- Sonn, U.; Asberg, K.H. Assessment of activities of daily living in the elderly. A study of a population of 76-year-olds in Gothenburg, Sweden. Scand. J. Rehabil. Med. 1991, 23, 193–202. [Google Scholar] [PubMed]
- Slaug, B.; Schilling, O.; Iwarsson, S.; Carlsson, G. Defining profiles of functional limitations in groups of older persons: How and why? J. Aging Health 2011, 23, 578–604. [Google Scholar] [CrossRef]
- Hamilton, L. Statistics with Stata: Version 10; Brooks/Cole: Belmont, Calif, 2008. [Google Scholar]
- Christensen, P.M.; Kristiansen, I.S. Number-needed-to-treat (NNT)—Needs treatment with care. Basic Clin. Pharmacol. Toxicol. 2006, 99, 12–16. [Google Scholar] [CrossRef] [PubMed]
- Statistics Sweden. Available online: http://www.statistikdatabasen.scb.se/pxweb/en/ssd/START__BE__BE0101__BE0101A/BefolkningNy/?rxid=9693c161–6689–4919–95d1–403bb8dc8fad (accessed on 29 June 2017).
- Statistisches Bundesamt (Destatis). Available online: https://www.destatis.de/EN/FactsFigures/SocietyState/Population/CurrentPopulation/CurrentPopulation.html (accessed on 29 June 2017).
- National Board of Health and Welfare. Available online: http://www.socialstyrelsen.se/publikationer2013/2013-4-15 (accessed on 29 June 2017).
- Statistisches Bundesamt. Pflegestatistik 2013; Statistisches Bundesamt: Wiesbaden, Germany, 2015. [Google Scholar]
- Medizinischer Dienst des Spitzenverbandes, Bund der Krankenkassen. Richtlinien des GKV-Spitzenverbandes zur Begutachtung von Pflegebedürftigkeit nach dem XI. Buch des Sozialgesetzbuches; Medizinischer Dienst des Spitzenverbandes, Bund der Krankenkassen: Düsseldorf, Germany, 2009. [Google Scholar]
- Rothgang, H. Vergütung von Leistungen der Häuslichen Krankenpflege nach § 37 SGB V; Universität Bremen: Bremen, Germany, 2011. [Google Scholar]
- Sveriges Kommuner och Landsting. Kostnad Per Brukare: Jämförelser Inom Omsorg om Äldre personer med Funktionsnedsättning—Utfall 2012; Sveriges Kommuner och Landsting: Stockholm, Sweden, 2013. [Google Scholar]
- Pettersson, C.; Slaug, B.; Granbom, M.; Kylberg, M.; Iwarsson, S. Housing accessibility for senior citizens in Sweden: Estimation of the effects of targeted elimination of environmental barriers. Scand. J. Occup. Ther. 2017. [Google Scholar] [CrossRef] [PubMed]
- Statens Offentliga Utredningar (SOU). Bostäder att bo Kvar i—Bygg för Gemenskap i Tillgänglighetssmarta Boendemiljöer; Statens Offentliga Utredningar (SOU): Stockholm, Sweden, 2015. [Google Scholar]
- Greiman, L.; Ravesloot, C. Housing characteristics of households with wheeled mobility device users from the american housing survey: Do people live in homes that facilitate community participation? Community Dev. 2016, 47, 63–74. [Google Scholar] [CrossRef]
- Shutes, I.; Chiatti, C. Migrant labour and the marketisation of care for older people: The employment of migrant care workers by families and service providers. J. Eur. Soc. Policy 2012, 22, 392–405. [Google Scholar] [CrossRef]


{kind=link}
| Germany | Sweden |
|---|---|
| 1. Wall-mounted cupboards and shelves placed extremely high in the kitchen | 1. Wall-mounted cupboards and shelves placed extremely high in the kitchen |
| 2. Doors at entrance that do not stay in open position/close quickly | 2. No grab bars at shower/bath and/or toilet |
| 3. Insufficient maneuvering areas in the kitchen | 3. Doors at entrance that do not stay in open position/close quickly |
| 4. Heavy doors without automatic opening at entrance | 4. Insufficient maneuvering areas in the kitchen |
| 5. Very high, very low, and/or irregular heights of risers at entrance stair | 5. High thresholds and/or steps at the entrance |
| I-ADL Type by Country | a1. Cases of I-ADL Dependence Baseline n (%) | a2. Cases of I-ADL Dependence: Follow Up n (%) | * b. Risk of Dependence in I-ADL or (95% CI) | c. Cases of I-ADL Dependence—Simulated Intervention Effect | d. Absolute Risk Reduction (c–a2, %) | f. Number Needed to ”Treat” |
|---|---|---|---|---|---|---|
| Germany (n = 322) | ||||||
| Cooking | 56 (17.5%) | 64 (19.9%) | 1.004 (1.000 to 1.008) | 60 (18.7%) | 1.2% | 86 |
| Shopping | 118 (36.8%) | 150 (46.6%) | 1.003 (1.000 to 1.007) | 143 (44.3%) | 2.2% | 45 |
| Cleaning | 141 (44.1%) | 143 (44.4%) | 1.001 (0.998 to 1.005) | 141 (43.6%) | 0.8% | 130 |
| Transportation | 44 (14.7%) | 80 (25.7%) | 1.005 (1.001 to 1.008) | 75 (24.0%) | 1.7% | 58 |
| Sweden (n = 314) | ||||||
| Cooking | 54 (17.2%) | 65 (20.7%) | 1.005 (1.002 to 1.009) | 59 (18.9%) | 1.8% | 56 |
| Shopping | 64 (20.4%) | 88 (28.0%) | 1.004 (1.001 to 1.008) | 82 (26.0%) | 2.0% | 50 |
| Cleaning | 95 (30.4%) | 122 (38.9%) | 1.011 (1.007 to 1.015) | 100 (32.0%) | 6.8% | 15 |
| Transportation | 127 (40.4%) | 125 (39.9%) | 1.004 (1.001 to 1.007) | 117 (37.4%) | 2.5% | 39 |
| Sub-Steps to Calculate Policy Cost | Germany | Sweden |
|---|---|---|
| Target Population | ||
| Total population age 80–90 * | 3,740,395 a | 427,940 b |
| Estimated proportion living in assisted living | 9% a | 14% c |
| Number of people living in private homes | 3,399,072 | 368,028 |
| Number of people independent in I-ADL but with difficulty (estimation from ENABLE-AGE samples) | 1,142,088 (34%) | 134,330 (37%) |
| Number currently receiving home services | 664,496 a | 82,774 c |
| Number to target for barrier removal policy | 477,592 | 51,556 |
| Home modifications | ||
| Number of home modifications | 477,592 | 50,913 |
| Cost per home modification (Euro) | 2557 d | 1570 e |
| Total Cost (Euro) | 1,221,203,235 | 79,933,207 |
| I-ADL Dependence | Cases Averted (95% CI) | Reduction of Hours/Week a (95% CI) | Reduction of Cost/Year (Euro) b (95% CI) |
|---|---|---|---|
| Germany | |||
| Shopping | 10,684 (701 to 20,694) | 138,886 (9111 to 269,026) | 312,065,586 (20,470,775 to 604,479,229) |
| Transportation | 8275 (2011 to 14,563) | 107,571 (26,138 to 189,316) | 241,702,602 (58,730,065 to 425,378,494) |
| Cooking | 5555 (367 to 10,765) | 72,215 (4768 to 139,939) | 162,261,974 (10,713,949 to 314,431,098) |
| Cleaning | 3673 (−6319 to 13,695) | 47,751 (−82,145 to 178,032) | 107,291,727 (−184,572,996 to 400,023,804) |
| Weighted total | 434,362,835 (−49,939,164 to 920,253,167) | ||
| Sweden | |||
| Shopping | 1035 (314 to 1757) | 8083 (2456 to 13,725) | 19,241,787 (5,847,783 to 32,674,489) |
| Transportation | 1313 (199 to 2432) | 10,262 (1552 to 19,000) | 24,429,313 (3,694,727 to 45,231,298) |
| Cooking | 914 (269 to 1562) | 7143 (2104 to 12,202) | 17,005,439 (5,008,795 to 29,045,992) |
| Cleaning | 3531 (2282 to 4784) | 27,585 (17,831 to 37,373) | 65,667,948 (42,449,297 to 88,970,055) |
| Weighted total | 62,662,789 (28,270,459 to 97,170,909) |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Slaug, B.; Chiatti, C.; Oswald, F.; Kaspar, R.; Schmidt, S.M. Improved Housing Accessibility for Older People in Sweden and Germany: Short Term Costs and Long-Term Gains. Int. J. Environ. Res. Public Health 2017, 14, 964. https://doi.org/10.3390/ijerph14090964
Slaug B, Chiatti C, Oswald F, Kaspar R, Schmidt SM. Improved Housing Accessibility for Older People in Sweden and Germany: Short Term Costs and Long-Term Gains. International Journal of Environmental Research and Public Health. 2017; 14(9):964. https://doi.org/10.3390/ijerph14090964
Chicago/Turabian StyleSlaug, Björn, Carlos Chiatti, Frank Oswald, Roman Kaspar, and Steven M. Schmidt. 2017. "Improved Housing Accessibility for Older People in Sweden and Germany: Short Term Costs and Long-Term Gains" International Journal of Environmental Research and Public Health 14, no. 9: 964. https://doi.org/10.3390/ijerph14090964