Child Nutritional Status in the Changing Socioeconomic Region of the Northern Amazon, Brazil

Abstract
:1. Introduction
2. Methods
3. Results and Discussion
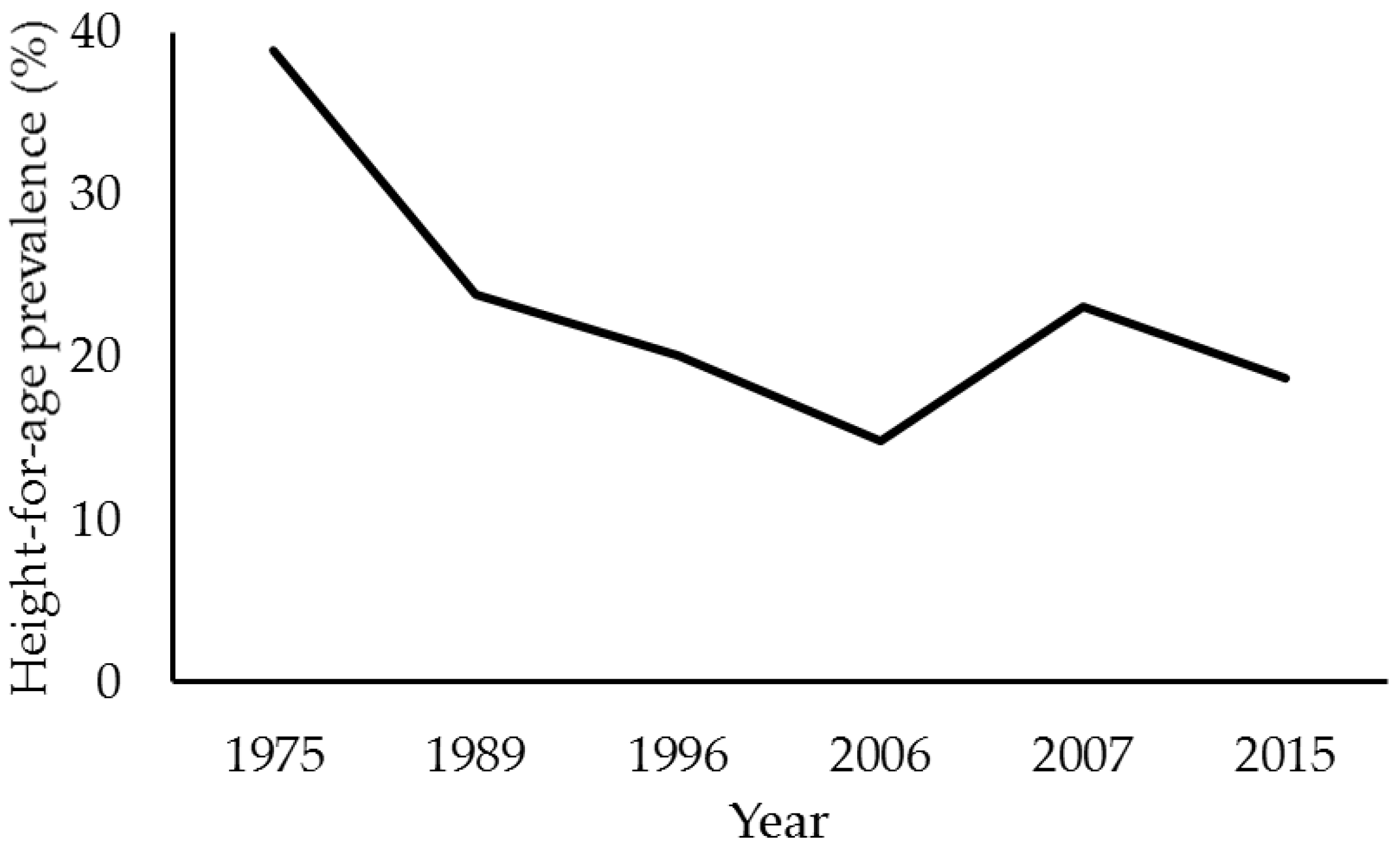
3.1. Height and Weight Deficits
3.2. Anthropometric Indices and Environmental Influences
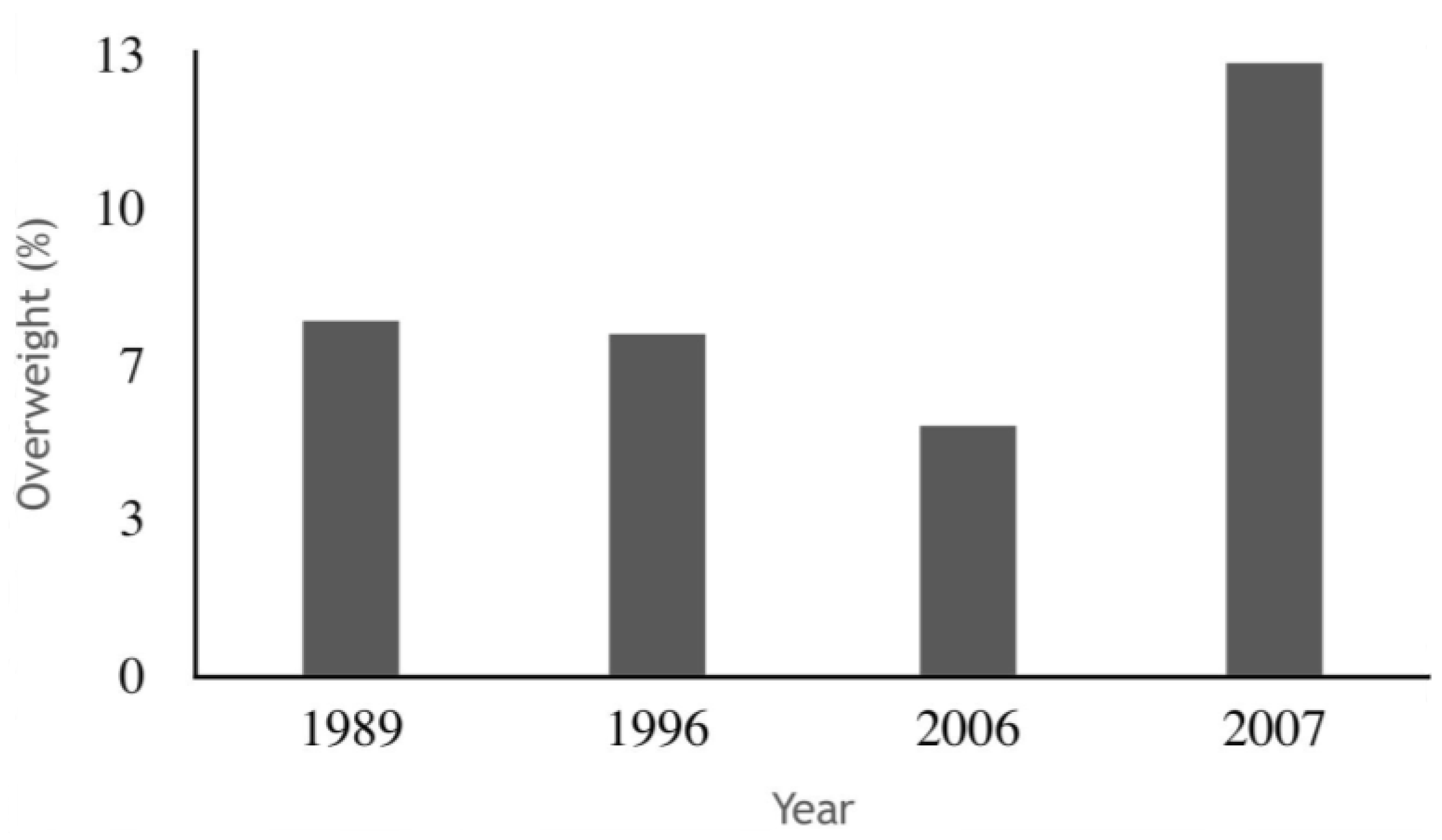
3.3. Overweight
3.4. Feeding Practices and Children’s Growth
3.5. Limitations
4. Conclusions
Author Contributions
Conflicts of Interest
References
- Black, R.E.; Victora, C.G.; Walker, S.P.; Bhutta, Z.A.; Christian, P.; de Onis, M.; Ezzati, M.; Grantham-McGregor, S.; Katz, J.; Martorell, R.; et al. Maternal and child undernutrition and overweight in low-income and middle-income countries. Lancet 2013, 382, 427–451. [Google Scholar] [CrossRef]
- Villar, J.; Cheikh Ismail, L.; Victora, C.G.; Ohuma, E.O.; Bertino, E.; Altman, D.G.; Lambert, A.; Papageorghiou, A.T.; Carvalho, M.; Jaffer, Y.A.; et al. International standards for newborn weight, length, and head circumference by gestational age and sex: The Newborn Cross-Sectional Study of the INTERGROWTH-21st Project. Lancet 2014, 384, 857–868. [Google Scholar] [CrossRef]
- Victora, C.G.; Aquino, E.M.; do Carmo Leal, M.; Monteiro, C.A.; Barros, F.C.; Szwarcwald, C.L. Maternal and child health in Brazil: Progress and challenges. Lancet 2011, 377, 1863–1876. [Google Scholar] [CrossRef]
- Fearnside, P.M. Impacts of Brazil’s Madeira River Dams: Unlearned lessons for hydroelectric development in Amazonia. Environ. Sci. Policy 2014, 38, 164–172. [Google Scholar] [CrossRef]
- Hacon, S.S.; Dórea, J.G.; Fonseca, Mde F.; Oliveira, B.A.; Mourão, D.S.; Ruiz, C.M.; Gonçalves, R.A.; Mariani, C.F.; Bastos, W.R. The influence of changes in lifestyle and mercury exposure in riverine populations of the Madeira River (Amazon Basin) near a hydroelectric project. Int. J. Environ. Res. Public. Health 2014, 11, 2437–2455. [Google Scholar] [CrossRef] [PubMed]
- Instituto Brasileiro de Geografia e Estatística (IBGE). Síntese de Indicadores Sociais: Uma Análise das Condições de vida da População Brasileira: 2015. Available online: http://biblioteca.ibge.gov.br/visualizacao/livros/liv95011.pdf (accessed on 18 December 2016).
- Instituto Brasileiro de Geografia e Estatística (IBGE); United Nations Children’s Fund. Perfil Estatístico de Crianças e Mães No Brasil: Aspectos Nutricionais, 1974–1975; IBGE, UNICEF: Rio de Janeiro, Brazil, 1982. [Google Scholar]
- Instituto Nacional de Alimentação e Nutrição (INAN). Pesquisa Nacional Sobre Saúde e Nutrição—PNSN-1989; Arquivo de Dados da Pesquisa: Brasília, Brazil, 1990. [Google Scholar]
- Sociedade Civil de Bem-Estar Familiar/ORT Macro. Brazil DHS 1996. Final report. Rio de Janeiro: Sociedade Civil Bem-Estar Familiar no Brasil (BEMFAM). 1996. Available online: http://dab.saude.gov.br/portaldab/ape_vigilancia_alimentar.php?conteudo=pnds (accessed on 2 January 2014).
- Ministério da Saúde. PNDS 2006, Pesquisa Nacional de Demografia e Saúde da Criança e da Mulher; Ministério da Saúde: Brasília, Brazil, 2008. [Google Scholar]
- Ministério da Saúde, Secretaria de Atenção à Saúde, Departamento de Atenção Básica, Coordenação-Geral da Política de Alimentação e Nutrição. Chamada Nutricional da Região Norte 2007: Resumo Executivo; Ministério da Saúde: Brasília, Brazil, 2009. [Google Scholar]
- Ministério da Saúde. Secretaria de Atenção à Saúde, Departamento de Ações Programáticas e Estratégicas. II Pesquisa de Prevalência de Aleitamento Materno nas Capitais Brasileiras e Distrito Federal; Editora do Ministério da Saúde: Brasília, Brazil, 2009. [Google Scholar]
- Instituto Brasileiro de Geografia e Estatística (IBGE). Pesquisa de Orçamentos Familiares 2002–2003: Antropometria e Análise do Estado Nutricional de Crianças e Adolescentes No Brasil. 2006. Available online: http://biblioteca.ibge.gov.br/visualizacao/livros/liv81847.pdf (accessed on 19 September 2015).
- Instituto Brasileiro de Geografia e Estatística (IBGE). Pesquisa de Orçamentos Familiares 2008–2009: Antropometria e Análise do Estado Nutricional de Crianças e Adolescentes No Brasil. 2010. Available online: http://biblioteca.ibge.gov.br/visualizacao/livros/liv45130.pdf (accessed on 19 September 2015).
- Ministério da Saúde. Coordenação Geral de Alimentação e Nutrição. Módulo Gerador de Relatórios do Sisvan Web. 2015. Available online: http://dabsistemas.saude.gov.br/sistemas/sisvan/relatorios_publicos/relatorios.php (accessed 24 on January 2015).
- Secretaria de Vigilância em Saúde, Ministério da Saúde. Vigilância em Saúde Ambiental: Dados e Indicadores Selecionados—2014. Available online: http://bvsms.saude.gov.br/bvs/folder/vigilancia_saude_ambiental_indicadores_2014.pdf (accessed on 25 November 2015).
- Victora, C.G.; Gigante, D.P.; Barros, A.J.; Monteiro, C.A.; de Onis, M. Estimating the prevalence of height for age deficits based on the prevalence of weight for age deficits among Brazilian children. Rev. Saude Publ. 1998, 32, 321–327. [Google Scholar] [CrossRef]
- Monteiro, C.A.; Benicio, M.H.; Conde, W.L.; Konno, S.; Lovadino, A.L.; Barros, A.J.; Victora, C.G. Narrowing socioeconomic inequality in child stunting: The Brazilian experience, 1974–2007. Bull. World Health Organ. 2010, 88, 305–311. [Google Scholar] [CrossRef] [PubMed]
- Ghana Statistical Service (GSS). Ghana Demographic and Health Survey 2014; GSS; GHS: Accra, Ghana; ICF International: Rockville, MD, USA, 2015.
- Wamani, H.; Astrom, A.N.; Peterson, S.; Tumwine, J.K.; Tylleskär, T. Boys are more stunted than girls in sub-Saharan Africa: A meta-analysis of 16 demographic and health surveys. BMC Pediatr. 2007, 7, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Onyango, A.W.; Borghi, E.; de Onis, M.; Frongillo, E.A.; Victora, C.G.; Dewey, K.G.; Lartey, A.; Bhandari, N.; Baerug, A.; Garza, C.; et al. Successive 1-month weight increments in infancy Can Be used to screen for faltering linear growth. J. Nutr. 2015, 145, 2725–2731. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Global Health Observatory (GHO) Data. 2015. Available online: http://www.who.int/gho/publications/mdgs-sdgs/MDGs-SDGs2015_chapter4.pdf?ua=1 (accessed on 17 February 2016).
- World Health Organization (WHO). Global Health Observatory (GHO). Available online: http://apps.who.int/gho/data/view.main.NUTWHOUNDERWEIGHTv?lang=en (accessed on 30 October 2017).
- Richard, S.A.; Black, R.E.; Checkley, W. Revisiting the relationship of weight and height in early childhood. Adv. Nutr. 2012, 3, 250–254. [Google Scholar] [CrossRef] [PubMed]
- Saaka, M.; Galaa, S.Z. Relationships between wasting and stunting and their concurrent occurrence in Ghanaian preschool children. J. Nutr. Metab. 2016. [Google Scholar] [CrossRef] [PubMed]
- Froes Asmus, C.I.; Camara, V.M.; Landrigan, P.J.; Claudio, L. A systematic review of children’s environmental health in Brazil. Ann. Glob. Health 2016, 82, 132–148. [Google Scholar] [CrossRef] [PubMed]
- Grantham-McGregor, S.; Cheung, Y.; Cueto, S.; Glewwe, P.; Richter, L.; The International Child Development Steering Group. Developmental potential in the first 5 years for children in developing countries. Lancet 2007, 369, 60–70. [Google Scholar] [CrossRef]
- Prass, T.S.; Lopes, S.R.; Dórea, J.G.; Marques, R.C.; Brandão, K.G. Amazon forest fires between 2001 and 2006 and birth weight in Porto Velho. Bull. Environ. Contam. Toxicol. 2012, 89, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Cândido da Silva, A.M.; Moi, G.P.; Mattos, I.E.; de Hacon, S.S. Low birth weight at term and the presence of fine particulate matter and carbon monoxide in the Brazilian Amazon: A population-based retrospective cohort study. BMC Pregnancy Childbirth 2014, 6, 309. [Google Scholar] [CrossRef] [PubMed]
- Botelho, C.; Correia, A.L.; da Silva, A.M.; Macedo, A.G.; Silva, C.O.S. Environmental factors and hospitalization of under-five children with acute respiratory infection. Cad. Saúde Pública 2003, 19, 1771–1780. [Google Scholar] [CrossRef] [PubMed]
- Johnson, W.B.; Aderele, W.I.; Gbadero, D.A. Host factors and acute lower respiratory infections in pre-school children. J. Trop. Pediatr. 1992, 38, 132–136. [Google Scholar] [CrossRef] [PubMed]
- Ministério da Saúde. Secretaria de Vigilância em Saúde, Coordenação Geral de Vigilância Ambiental em Saúde. Programa Nacional de Vigilância em Saúde de Populações Expostas a solo Contaminado. Available online: http://portalarquivos.saude.gov.br/images/pdf/2017/abril/Ficha_Sissolo.pdf (accessed on 27 October 2017).
- De Onis, M.; Frongillo, E.A.; Blössner, M. Is malnutrition declining? An analysis of changes in levels of child malnutrition since 1980. Bull. World Health Organ. 2000, 78, 1222–1233. [Google Scholar] [PubMed]
- Güngör, N.K. Overweight and obesity in children and adolescents. J. Clin. Res. Pediatr. Endocrinol. 2014, 6, 129–143. [Google Scholar] [CrossRef] [PubMed]
- Emmett, P.M.; Jones, L.R. Diet, growth, and obesity development throughout childhood in the Avon Longitudinal Study of Parents and Children. Nutr. Rev. 2015, 73 (Suppl. 3), 175–206. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Global Health Observatory (GHO). Available online: http://apps.who.int/gho/data/node.wrapper.nutrition-2016?lang=en (accessed on 2 February 2016).
- Costa-Font, J.; Gil, J. Intergenerational and socioeconomic gradients of child obesity. Soc. Sci. Med. 2013, 93, 29–37. [Google Scholar] [CrossRef] [PubMed]
- Zilanawala, A.; Davis-Kean, P.; Nazroo, J.; Sacker, A.; Simonton, S.; Kelly, Y. Race/ethnic disparities in early childhood BMI, obesity and overweight in the United Kingdom and United States. Int. J. Obes. (Lond.) 2015, 39, 520–529. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, D.J.; Sawaya, A.L.; Verreschi, I.; Tucker, K.L.; Roberts, S.B. Why are nutritionally stunted children at increased risk of obesity? Studies of metabolic rate and fat oxidation in shantytown children from São Paulo, Brazil. Am. J. Clin. Nutr. 2000, 72, 702–707. [Google Scholar] [PubMed]
- Bates, K.; Gjonça, A.; Leone, T. Double burden or double counting of child malnutrition? The methodological and theoretical implications of stuntingoverweight in low and middle income countries. J. Epidemiol. Commun. Health 2017, 71, 779–785. [Google Scholar] [CrossRef] [PubMed]
- Han, J.C.; Lawlor, D.A.; Kimm, S.Y.S. Childhood Obesity—2010: Progress and challenges. Lancet. Child. Obes. 2010, 375, 1737–1748. [Google Scholar]
- Niehues, J.R.; Gonzales, A.I.; Lemos, R.R.; Bezerra, P.P.; Haas, P. Prevalence of overweight and obesity in children and adolescents from the age range of 2 to 19 years old in Brazil. Int. J. Pediatr. 2014. [Google Scholar] [CrossRef] [PubMed]
- Jaime, P.C.; Stopa, S.R.; Oliveira, T.P.; Vieira, M.L.; Szwarcwald, C.L.; Malta, D.C. Prevalência e distribuição sociodemográfica de marcadores de alimentação saudável, Pesquisa Nacional de Saúde, Brasil 2013. Epidemiol. Serv. Saúde 2015, 24, 267–276. [Google Scholar] [CrossRef]
- Bortolini, G.A.; Vitolo, M.R.; Gubert, M.B.; Santos, L.M. Social inequalities influence the quality and diversity of diet in Brazilian children 6 to 36 months of age. Cad. Saude Publica 2015, 31, 2413–2424. [Google Scholar] [CrossRef] [PubMed]
- Victora, C.G.; Bahl, R.; Barros, A.J.; França, G.V.; Horton, S.; Krasevec, J.; Murch, S.; Sankar, M.J.; Walker, N.; Rollins, N.C.; et al. Breastfeeding in the 21st century: Epidemiology, mechanisms, and lifelong effect. Lancet 2016, 387, 475–490. [Google Scholar] [CrossRef]
- Christian, P.; Mullany, L.C.; Hurley, K.M.; Katz, J.; Black, R.E. Nutrition and maternal, neonatal, and child health. Semin. Perinatol. 2015, 39, 361–372. [Google Scholar] [CrossRef] [PubMed]
- Venancio, S.I.; Saldiva, S.R.D.M.; Monteiro, C.A. Secular trends in breastfeeding in Brazil. Rev. Saúde Publ. 2013, 47, 1205–1208. [Google Scholar] [CrossRef]
- Stenhammar, C.; Wells, M.; Ahman, A.; Wettergren, B.; Edlund, B.; Sarkadi, A. “Children are exposed to temptation all the time”—Parents’ lifestyle-related discussions in focus groups. Acta Paediatr. 2012, 101, 208–215. [Google Scholar] [CrossRef] [PubMed]
- Mazarello Paes, V.; Ong, K.K.; Lakshman, R. Factors influencing obesogenic dietary intake in young children (0–6 years): Systematic review of qualitative evidence. BMJ Open 2015. [Google Scholar] [CrossRef] [PubMed]
- Dórea, J.G. Cassava cyanogens and fish mercury are high but safely consumed in the diet of native Amazonians. Ecotoxicol. Environ. Saf. 2004, 57, 248–256. [Google Scholar] [CrossRef] [PubMed]
- Food and Agriculture Organization of the United Nations (FAO). The State of World Fisheries and Aquaculture 2016: Contributing to Food Security and Nutrition for All; FAO: Rome, Italy, 2016. [Google Scholar]
- Oliveira, R.C.; Dórea, J.G.; Bernardi, J.V.; Bastos, W.R.; Almeida, R.; Manzatto, A.G. Fish consumption by traditional subsistence villagers of the Rio Madeira (Amazon): Impact on hair mercury. Ann. Hum. Biol. 2010, 37, 629–642. [Google Scholar] [CrossRef] [PubMed]
- Dórea, J.G.; Marques, R.C. Mercury levels and human health in the Amazon Basin. Ann. Hum. Biol. 2016, 43, 349–359. [Google Scholar] [CrossRef] [PubMed]
- Leventakou, V.; Roumeliotaki, T.; Martinez, D.; Barros, H.; Brantsaeter, A.L.; Casas, M.; Charles, M.A.; Cordier, S.; Eggesbø, M.; van Eijsden, M.; Forastiere, F.; et al. Fish intake during pregnancy, fetal growth, and gestational length in 19 European birth cohort studies. Am. J. Clin. Nutr. 2014, 99, 506–516. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stratakis, N.; Roumeliotaki, T.; Oken, E.; Barros, H.; Basterrechea, M.; Charles, M.A.; Eggesbø, M.; Forastiere, F.; Gaillard, R.; Gehring, U.; Govarts, E.; et al. Fish intake in pregnancy and child growth: A pooled analysis of 15 European and US birth cohorts. JAMA Pediatr. 2016, 170, 381–390. [Google Scholar] [CrossRef] [PubMed]
- Grün, F.; Blumberg, B. Endocrine disrupters as obesogens. Mol. Cell. Endocrinol. 2009, 304, 19–29. [Google Scholar] [CrossRef] [PubMed]
- Marques, R.C.; Bernardi, J.V.; Dórea, J.G.; Brandão, K.G.; Bueno, L.; Leão, R.S.; Malm, O. Fish consumption during pregnancy, mercury transfer, and birth weight along the Madeira River Basin in Amazonia. Int. J. Environ. Res. Public. Health 2013, 10, 2150–2163. [Google Scholar] [CrossRef] [PubMed]
- Marques, R.C.; Dórea, J.G.; Bernardi, J.V.E.; Bastos, W.R.; Malm, O. Maternal fish consumption in the nutrition transition of the Amazon Basin: Growth of exclusively breastfed infants during the first 5 years. Ann. Hum. Biol. 2008, 35, 363–377. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cunha, M.P.L.; Marques, R.C.; Dórea, J.G. Child Nutritional Status in the Changing Socioeconomic Region of the Northern Amazon, Brazil. Int. J. Environ. Res. Public Health 2018, 15, 15. https://doi.org/10.3390/ijerph15010015
Cunha MPL, Marques RC, Dórea JG. Child Nutritional Status in the Changing Socioeconomic Region of the Northern Amazon, Brazil. International Journal of Environmental Research and Public Health. 2018; 15(1):15. https://doi.org/10.3390/ijerph15010015
Chicago/Turabian StyleCunha, Mônica P. L., Rejane C. Marques, and José G. Dórea. 2018. "Child Nutritional Status in the Changing Socioeconomic Region of the Northern Amazon, Brazil" International Journal of Environmental Research and Public Health 15, no. 1: 15. https://doi.org/10.3390/ijerph15010015