Mental Health Recovery of Evacuees and Residents from the Fukushima Daiichi Nuclear Power Plant Accident after Seven Years—Contribution of Social Network and a Desirable Lifestyle

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Survey Variables
2.2.1. Disaster-Related Experiences
2.2.2. Economic Status
2.2.3. Subjective Health Status and Lifestyle
2.2.4. Social Network
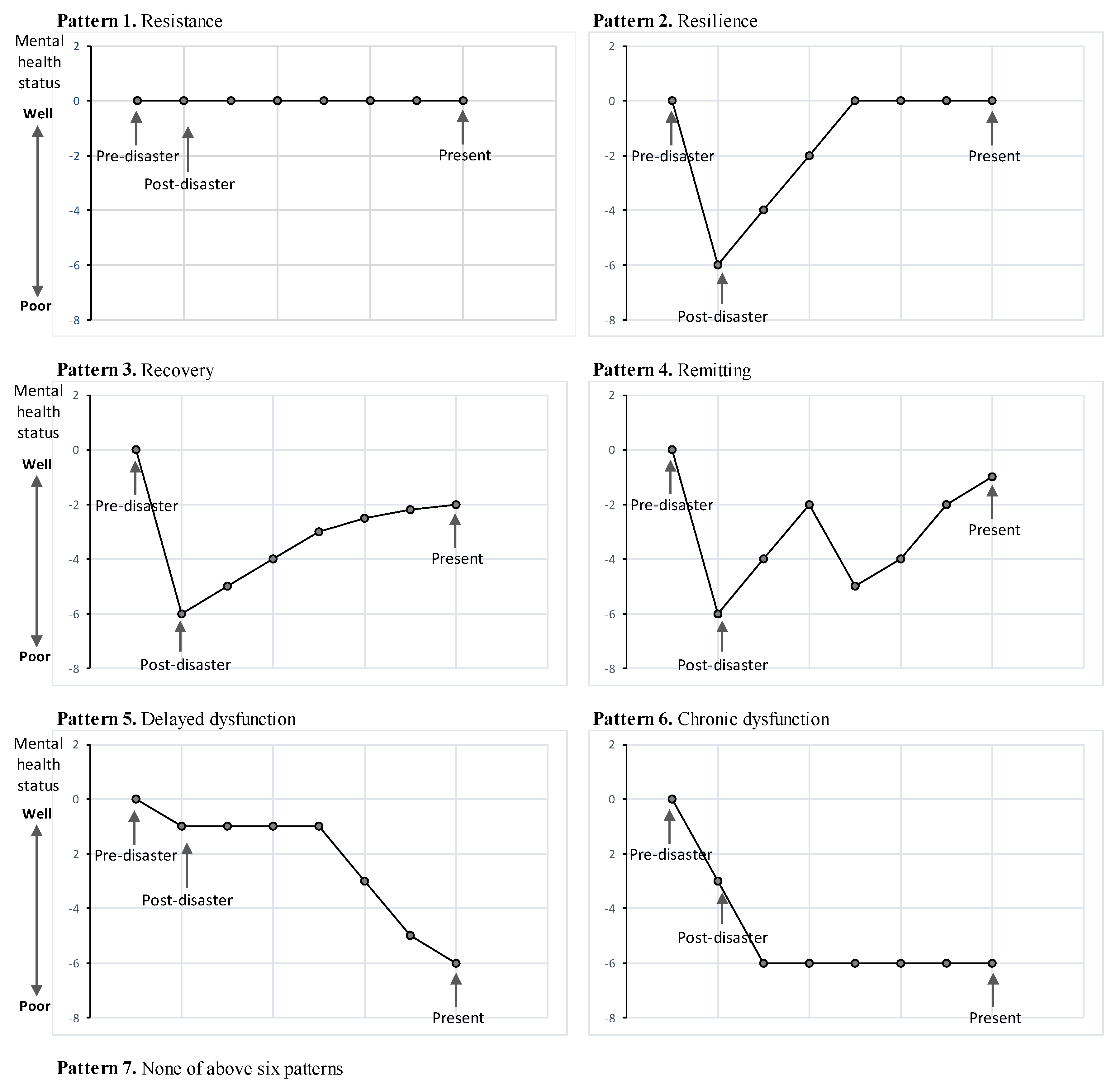
2.2.5. Mental Health Recovery Patterns
2.3. Statistical Analysis
3. Results
3.1. Participants
3.2. Respondent Characteristics
3.3. Disaster-Related Experiences and Current Economic Status
3.4. Current Health Status, Lifestyle, and Social Network
3.5. Association between Mental Health Recovery and Disaster-Related Experience, Current Economic Status and Health Status, and Lifestyle and Social Network
4. Discussion
4.1. The Mental Health Recovery Patterns and Their Basic Characteristics
4.2. Association between Mental Health Recovery and Disaster-Related Experiences, Current Economic and Health Status, and Lifestyle and Social Network
4.3. Limitations and Strengths
5. Conclusions
Supplementary Materials
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Fukushima Prefectural Government, Japan. Fukushima Revitalization Station. 2016. Available online: http://www.pref.fukushima.lg.jp/site/portal-english/ (accessed on 9 June 2018).
- Yabe, H.; Suzuki, Y.; Mashiko, H.; Nakayama, Y.; Hisata, M.; Niwa, S.; Yasumura, S.; Yamashita, S.; Kamiya, K.; Abe, M.; et al. Psychological distress after the Great East Japan Earthquake and Fukushima Daiichi Nuclear Power Plant accident: Results of a mental health and lifestyle survey through the Fukushima Health Management Survey in FY2011 and FY2012. Fukushima J. Med. Sci. 2014, 60, 57–67. [Google Scholar] [CrossRef] [PubMed]
- Shigemura, J.; Tanigawa, T.; Nishi, D.; Matsuoka, Y.; Nomura, S.; Yoshino, A. Associations between disaster exposures, peritraumatic distress, and posttraumatic stress responses in Fukushima nuclear plant workers following the 2011 nuclear accident: The Fukushima NEWS Project study. PLoS ONE 2014, 9, e87516. [Google Scholar] [CrossRef] [PubMed]
- Oe, M.; Fujii, S.; Maeda, M.; Nagai, M.; Harigane, M.; Miura, I.; Yabe, H.; Ohira, T.; Takahashi, H.; Suzuki, Y.; et al. Three-year trend survey of psychological distress, post-traumatic stress, and problem drinking among residents in the evacuation zone after the Fukushima Daiichi Nuclear Power Plant accident (The Fukushima Health Management Survey). Psychiatry Clin. Neurosci. 2016, 70, 245–252. [Google Scholar] [CrossRef] [PubMed]
- Goodwin, R.; Takahashi, M.; Sun, S.; Ben-Ezra, M. Psychological distress among tsunami refugees from the Great East Japan earthquake. BJPsych. Open 2015, 1, 92–97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suzuki, Y.; Yabe, H.; Yasumura, S.; Ohira, T.; Niwa, S.; Ohtsuru, A.; Mashiko, H.; Maeda, M.; Abe, M.; Mental Health Group of the Fukushima Health Management Survey. Psychological distress and the perception of radiation risks: The Fukushima health management survey. Bull. World Health Organ. 2015, 93, 598–605. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, Y.; Takebayashi, Y.; Yasumura, S.; Murakami, M.; Harigane, M.; Yabe, H.; Ohira, T.; Ohtsuru, A.; Nakajima, S.; Maeda, M. Changes in Risk Perception of the Health Effects of Radiation and Mental Health Status: The Fukushima Health Management Survey. Int. J. Environ. Res. Public Health 2018, 15, E1219. [Google Scholar] [CrossRef] [PubMed]
- Ohto, H.; Maeda, M.; Yabe, H.; Yasumura, S.; Bromet, E.E. Suicide rates in the aftermath of the 2011 earthquake in Japan. Lancet 2015, 385, 1727. [Google Scholar] [CrossRef]
- Orui, M.; Suzuki, Y.; Maeda, M.; Yasumura, S. Suicide Rates in Evacuation Areas after the Fukushima Daiichi Nuclear Disaster. Crisis 2018, 39, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Bromet, E.J. Emotional consequences of nuclear power plant disasters. Health Phys. 2014, 106, 206–210. [Google Scholar] [CrossRef] [PubMed]
- Maeda, M.; Oe, M. Mental Health Consequences and Social Issues After the Fukushima Disaster. Asia Pac. J. Public Health 2017, 29, 36S–46S. [Google Scholar] [CrossRef] [PubMed]
- Ohto, H.; Yasumura, S.; Maeda, M.; Kainuma, H.; Fujimori, K.; Nollet, K.E. From Devastation to Recovery and Revival in the Aftermath of Fukushima’s Nuclear Power Plants Accident. Asia Pac. J. Public Health 2017, 29, 10S–17S. [Google Scholar] [CrossRef] [PubMed]
- Fukunaga, H.; Kumakawa, H. Mental Health Crisis in Northeast Fukushima after the 2011 Earthquake, Tsunami and Nuclear Disaster. Tohoku J. Exp. Med. 2015, 237, 41–43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yamashita, S. Radiation Medical Science Center for the Fukushima Health Management Survey. Comprehensive Health Risk Management after the Fukushima Nuclear Power Plant Accident. Clin. Oncol. 2016, 28, 255–262. [Google Scholar] [CrossRef] [PubMed]
- Hino, Y.; Murakami, M.; Midorikawa, S.; Ohtsuru, A.; Suzuki, S.; Tsuboi, K.; Ohira, T. Explanatory Meetings on Thyroid Examination for the “Fukushima Health Management Survey” after the Great East Japan Earthquake: Reduction of Anxiety and Improvement of Comprehension. Tohoku J. Exp. Med. 2016, 239, 333–343. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murakami, M.; Sato, A.; Matsui, S.; Goto, A.; Kumagai, A.; Tsubokura, M.; Orita, M.; Takamura, N.; Kuroda, Y.; Ochi, S. Communicating with Residents about Risks Following the Fukushima Nuclear Accident. Asia Pac. J. Public Health 2017, 29, 74S–89S. [Google Scholar] [CrossRef] [PubMed]
- Imamura, K.; Sekiya, Y.; Asai, Y.; Umeda, M.; Horikoshi, N.; Yasumura, S.; Yabe, H.; Akiyama, T.; Kawakami, N. The effect of a behavioral activation program on improving mental and physical health complaints associated with radiation stress among mothers in Fukushima: A randomized controlled trial. BMC Public Health 2016, 16, 1144. [Google Scholar] [CrossRef] [PubMed]
- Murakami, M.; Nakatani, J.; Oki, T. Evaluation of Risk Perception and Risk-Comparison Information Regarding Dietary Radionuclides after the 2011 Fukushima Nuclear Power Plant Accident. PLoS ONE 2016, 11, e0165594. [Google Scholar] [CrossRef] [PubMed]
- Takebayashi, Y.; Lyamzina, Y.; Suzuki, Y.; Murakami, M. Risk Perception and Anxiety Regarding Radiation after the 2011 Fukushima Nuclear Power Plant Accident: A Systematic Qualitative Review. Int. J. Environ. Res. Public Health 2017, 14, E1306. [Google Scholar] [CrossRef] [PubMed]
- Fukushima Medical University Fukushima Health Management Survey. Radiation Medical Science Center for the Fukushima Health Management Survey. 2016. Available online: http://www.pref.fukushima.lg.jp/site/portal/kenkocyosa-kentoiinkai.html (accessed on 9 June 2018). (In Japanese).
- Ueda, Y.; Yabe, H.; Maeda, M.; Ohira, T.; Fujii, S.; Niwa, S. Drinking Behavior and Mental Illness among Evacuees in Fukushima Following the Great East Japan Earthquake: The Fukushima Health Management Survey. Alcohol. Clin. Exp. Res. 2016, 40, 623–630. [Google Scholar] [CrossRef] [PubMed]
- Gallo, W.T.; Bradley, E.H.; Siegel, M.; Kasl, S.V. The impact of involuntary job loss on subsequent alcohol consumption by older workers: Findings from the health and retirement survey. J. Gerontol. 2001, 56, S3–S9. [Google Scholar] [CrossRef]
- Yokoyama, Y.; Otsuka, K.; Kawakami, N.; Kobayashi, S.; Ogawa, A.; Tanno, K. Mental health and related factors after the Great East Japan earthquake and tsunami. PLoS ONE 2014, 9, e102497. [Google Scholar] [CrossRef] [PubMed]
- Itani, O.; Kaneita, Y.; Munezawa, T.; Mishima, K.; Jike, M.; Nakagome, S.; Tokiya, M.; Ohida, T. Nationwide epidemiological study of insomnia in Japan. Sleep Med. 2016, 25, 130–138. [Google Scholar] [CrossRef] [PubMed]
- Takeda, F.; Noguchi, H.; Monma, T.; Tamiya, N. How possibly do leisure and social activities impact mental health of middle-aged adults in Japan?: An evidence from a National Longitudinal Survey. PLoS ONE 2015, 10, e0139777. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adams, R.E.; Boscarino, J.A.; Galea, S. Alcohol use, mental health status and psychological well-being 2 years after the World Trade Center attacks in New York City. Am. J. Drug Alcohol Abuse 2006, 32, 203–224. [Google Scholar] [CrossRef] [PubMed]
- Nordløkken, A.; Pape, H.; Wentzel-Larsen, T.; Heir, T. Changes in alcohol consumption after a natural disaster: A study of Norwegian survivors after the 2004 Southeast Asia tsunami. BMC Public Health 2013, 13, 58. [Google Scholar] [CrossRef] [PubMed]
- Hayashi, K.; Kawachi, I.; Ohira, T.; Kondo, K.; Shirai, K.; Kondo, N. Laughter and subjective health among community-dwelling older people in Japan: Cross-sectional analysis of the Japan gerontological evaluation study cohort data. J. Nerv. Ment. Dis. 2015, 203, 934–942. [Google Scholar] [CrossRef] [PubMed]
- Itagaki, S.; Harigane, M.; Maeda, M.; Yasumura, S.; Suzuki, Y.; Mashiko, H.; Nagai, M.; Ohira, T.; Yabe, H. Mental Health Group of the Fukushima Health Management Survey. Exercise habits are important for the mental health of children in fukushima after the Fukushima Daiichi Disaster. Asia Pac. J. Public Health 2017, 29, 171S–181S. [Google Scholar] [CrossRef] [PubMed]
- Tsuchiya, N.; Nakaya, N.; Nakamura, T.; Narita, A.; Kogure, M.; Aida, J.; Tsuji, I.; Hozawa, A.; Tomita, H. Impact of social capital on psychological distress and interaction with house destruction and displacement after the Great East Japan Earthquake of 2011. Psychiatry Clin. Neurosci. 2017, 71, 52–60. [Google Scholar] [CrossRef] [PubMed]
- Norris, F.H.; Tracy, M.; Galea, S. Looking for resilience: Understanding the longitudinal trajectories of responses to stress. Soc. Sci. Med. 2009, 68, 2190–2198. [Google Scholar] [CrossRef] [PubMed]
- Kessler, R.C.; Barker, P.R.; Colpe, L.J.; Epstein, J.F.; Gfroerer, J.C.; Hiripi, E. Screening for serious mental illness in the general population. Arch. Gen. Psychiatry 2003, 60, 184–189. [Google Scholar] [CrossRef] [PubMed]
- Furukawa, T.; Kawakami, N.; Saitoh, M.; Ono, Y.; Nakane, Y.; Nakamura, Y. The performance of the Japanese version of the K6 and K10 in the World Mental Health Survey Japan. Int. J. Methods Psychiatry Res. 2008, 17, 152–158. [Google Scholar] [CrossRef] [PubMed]
- Tsuboya, T.; Aida, J.; Hikichi, H.; Subramanian, S.V.; Kondo, K.; Osaka, K.; Kawachi, I. Predictors of depressive symptoms following the Great East Japan earthquake: A prospective study. Soc. Sci. Med. 2016, 161, 47–54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nagai, M.; Ohira, T.; Zhang, W.; Nakano, H.; Maeda, M.; Yasumura, S.; Abe, M. Lifestyle-related factors that explain disaster-induced changes in socioeconomic status and poor subjective health: A cross-sectional study from the Fukushima health management survey. BMC Public Health 2017, 17, 340. [Google Scholar] [CrossRef] [PubMed]
- Wind, T.R.; Komproe, I.H. The mechanisms that associate community social capital with post-disaster mental health: A multilevel model. Soc. Sci. Med. 2012, 75, 1715–1720. [Google Scholar] [CrossRef] [PubMed]
- Kawachi, I.; Berkma, L. Social Ties and Mental Health. J. Urban. Health 2001, 78, 458–467. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McKenzie, K.; Whitley, R.; Weich, S. Social capital and mental health. Br. J. Psychiatry 2002, 181, 280–283. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Orui, M.; Suzuki, Y.; Goto, A.; Yasumura, S. Factors Associated with Maintaining the Mental Health of Employees after the Fukushima Nuclear Disaster: Findings from Companies Located in the Evacuation Area. Int. J. Environ. Res. Public Health. 2017, 15, E53. [Google Scholar] [CrossRef] [PubMed]
- Tomata, Y.; Sato, N.; Kogure, M.; Suto, S.; Imai, Y.; Aoki, H.; Sugiyama, K.; Suzuki, R.; Sugawara, Y.; Watanabe, T.; et al. Health effects of interventions to promote physical activity in survivors of the 2011 Great East Japan Earthquake. A longitudinal study. Nihon Koshu Eisei Zasshi 2015, 62, 66–72. (In Japanese) [Google Scholar] [PubMed]
- Tsuji, T.; Sasaki, Y.; Matsuyama, Y.; Sato, Y.; Aida, J.; Kondo, K.; Kawachi, I. Reducing depressive symptoms after the Great East Japan Earthquake in older survivors through group exercise participation and regular walking: A prospective observational study. BMJ Open 2017, 7, e013706. [Google Scholar] [CrossRef] [PubMed]
- Uchida, T.; Matsumoto, K.; Takahashi, Y.; Koshimichi, R.; Sakuma, A.; Katsura, M.; Sato, H.; Ueda, I.; Matsuoka, H. Activity to prevent mental diseases after the Great East Japan Earthquake. Seishin Shinkeigaku Zasshi 2014, 116, 203–208. (In Japanese) [Google Scholar] [PubMed]
- Fukasawa, M.; Kawakami, N.; Umeda, M.; Miyamoto, K.; Akiyama, T.; Horikoshi, N.; Yasumura, S.; Yabe, H.; Bromet, E.J. Environmental radiation level, radiation anxiety and psychological distress in non-evacuee residents in Fukushima five years after the Great East Japan Earthquake: Multilevel analyses. SSM Popul. Health 2017, 3, 740–748. [Google Scholar] [CrossRef] [PubMed]
- Bartley, M. Unemployement and ill health: Understanding the relationship. J. Epidemiol. Community Health 1994, 48, 333–337. [Google Scholar] [CrossRef] [PubMed]
- Iwasaki, Y.; Mannell, R.C. Hierarchical dimensions of leisure stress coping. Leis. Sci. 2000, 22, 163–181. [Google Scholar]
- Iwasaki, Y.; Schneider, I.E. Leisure, stress and coping: An evolving area of inquiry. Leis. Sci. 2003, 25, 107–113. [Google Scholar] [CrossRef]
- Sugimoto, T.; Umeda, M.; Shinozaki, T.; Naruse, T.; Miyamoto, Y. Sources of perceived social support associated with reduced psychological distress at 1 year after the Great East Japan Earthquake: Nationwide cross-sectional survey in 2012. Psychiatry Clin. Neurosci. 2015, 69, 580–586. [Google Scholar] [CrossRef] [PubMed]
- Koyama, S.; Aida, J.; Kawachi, I.; Kondo, N.; Subramanian, S.V.; Ito, K.; Kobashi, G.; Masuno, K.; Kondo, K.; Osaka, K. Social support improves mental health among the victims relocated to temporary housing following the Great East Japan Earthquake and Tsunami. Tohoku J. Exp. Med. 2014, 234, 241–247. [Google Scholar] [CrossRef] [PubMed]
- Takagi, D.; Kondo, K.; Kawachi, I. Social participation and mental health: Moderating effects of gender, social role and rurality. BMC Public Health. 2013, 13, 701. [Google Scholar] [CrossRef] [PubMed]
- SEEDS Asia. Support for the Great East Japan Earthquake. 2013. Available online: http://www.seedsasia.org/eng/the-great-east-japan-earthquake/the-great-east-japan-earthquak-01-summary/43 (accessed on 9 June 2018).
- AAR Japan. The Great East Japan Earthquake: Two Years on from the Earthquake Disaster—An Activity Report of the Progress to Date 2011/03–2013/03. 2014. Available online: http://www.aarjapan.gr.jp/activity/japan/#tohoku (accessed on 9 June 2018).
- Japan International Volunteer Center. Kesennuma, Miyagi-Pref. (Great East Japan Earthquake). 2016. Available online: https://www.ngo-jvc.net/en/ourprojects/kesennuma-miyagi-pref-great-east-japan-earthquake/ (accessed on 9 June 2018).
- International Federation of Rd Cross and Red Crescent Societies. Care Continues for the Elderly Survivors of the Great East Japan and Earthquake. 2016. Available online: www.ifrc.org/en/news-and-media/news-stories/asia-pacific/japan/care-continues-for-the-elderly-survivors-of-the-great-east-japan-and-earthquake-72003/ (accessed on 9 June 2018).
- Plaisier, I.; Beekman, A.T.; de Bruijn, J.G.; de Graaf, R.; Ten Have, M.; Smit, J.H.; van Dyck, R.; Penninx, B.W. The effect of social roles on mental health: A matter of quantity or quality? J. Affect. Disord. 2008, 111, 261–270. [Google Scholar] [CrossRef] [PubMed]
- Orui, M.; Harada, S.; Hayashi, M.; Disaster Mental Health Team of the Sendai City Mental Health and Welfare Center. Practical Report on Long-term Disaster Mental Health Services Following the Great East Japan Earthquake: Psychological and Social Background of Evacuees in Sendai City in the Mid- to Long-term Post-disaster Period. Disaster Med. Public Health Prep. 2017, 4, 439–450. [Google Scholar] [CrossRef] [PubMed]
- Horikoshi, N.; Iwasa, H.; Yasumura, S.; Maeda, M. The characteristics of non-respondents and respondents of a mental health survey among evacuees in a disaster: The Fukushima Health Management Survey. Fukushima J. Med. Sci. 2017, 63, 152–159. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Basic Characteristics | Total | Pattern 1 | Pattern 2 | Pattern 3 | Pattern 4 | Pattern 5 | Pattern 6 | None of These Patterns | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Resistance | Resilience | Recovery | Remitting | Delayed Dysfunction | Chronic Dysfunction | |||||||||||
| (n = 410) | (n = 42) | (n = 100) | (n = 127) | (n = 47) | (n = 19) | (n = 40) | (n = 35) | |||||||||
| n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | |||||||||
| Age (as of February 2018) | ||||||||||||||||
| Less than 40 years old | 56 | (100.0) | 9 | (16.1) | 9 | (16.1) | 15 | (26.8) | 12 | (21.4) | 6 | (10.7) | 1 | (1.8) | 4 | (7.1) |
| 40–64 years old | 190 | (100.0) | 19 | (10.0) | 50 | (26.3) | 58 | (30.5) | 22 | (11.6) | 7 | (3.7) | 17 | (8.9) | 17 | (8.9) |
| 65 years old and more | 164 | (100.0) | 14 | (8.5) | 41 | (25.0) | 54 | (32.9) | 13 | (7.9) | 6 | (3.7) | 22 | (13.4) | 14 | (8.5) |
| Gender | ||||||||||||||||
| Male | 178 | (100.0) | 27 | (15.2) | 42 | (23.6) | 51 | (28.7) | 14 | (7.9) | 9 | (5.1) | 18 | (10.1) | 17 | (9.6) |
| Female | 232 | (100.0) | 15 | (6.5) | 58 | (25.0) | 76 | (32.8) | 33 | (14.2) | 10 | (4.3) | 22 | (9.5) | 18 | (7.8) |
| Education | ||||||||||||||||
| Junior/Senior high school | 300 | (100.0) | 23 | (7.7) | 67 | (22.3) | 100 | (33.3) | 35 | (11.7) | 14 | (4.7) | 33 | (11.0) | 28 | (9.3) |
| Vocational college, University | 108 | (100.0) | 19 | (17.6) | 33 | (30.6) | 26 | (24.1) | 11 | (10.2) | 5 | (4.6) | 7 | (6.5) | 7 | (6.5) |
| Occupational category | ||||||||||||||||
| Employed, Owner | 154 | (100.0) | 24 | (15.6) | 44 | (28.6) | 42 | (27.3) | 19 | (12.3) | 4 | (2.6) | 11 | (7.1) | 10 | (6.5) |
| Part-time | 49 | (100.0) | 1 | (2.0) | 13 | (26.5) | 16 | (32.7) | 8 | (16.3) | 2 | (4.1) | 3 | (6.1) | 6 | (12.2) |
| Homemaker | 77 | (100.0) | 8 | (10.4) | 19 | (24.7) | 26 | (33.8) | 12 | (15.6) | 1 | (1.3) | 6 | (7.8) | 5 | (6.5) |
| Unemployed | 122 | (100.0) | 9 | (7.4) | 20 | (16.4) | 41 | (33.6) | 7 | (5.7) | 11 | (9.0) | 20 | (16.4) | 14 | (11.5) |
| Living area as of 11 March 2011 | ||||||||||||||||
| Evacuation area | 177 | (100.0) | 8 | (4.5) | 30 | (16.9) | 72 | (40.7) | 26 | (14.7) | 8 | (4.5) | 24 | (13.6) | 9 | (5.1) |
| Non-evacuation area | 233 | (100.0) | 34 | (14.6) | 70 | (30.0) | 55 | (23.6) | 21 | (9.0) | 11 | (4.7) | 16 | (6.9) | 26 | (11.2) |
| Living with family member | ||||||||||||||||
| Living with family | 362 | (100.0) | 40 | (11.0) | 93 | (25.7) | 111 | (30.7) | 39 | (10.8) | 14 | (3.9) | 35 | (9.7) | 30 | (8.3) |
| Single life | 38 | (100.0) | 1 | (2.6) | 7 | (18.4) | 14 | (36.8) | 7 | (18.4) | 3 | (7.9) | 3 | (7.9) | 3 | (7.9) |
| Current psychological distress (K6: Kessler 6) | ||||||||||||||||
| K6 score ≥ 13 | 50 | (100.0) | 5 | (12.8) | 4 | (4.0) | 3 | (2.5) | 6 | (13.6) | 7 | (36.8) | 20 | (54.1) | 5 | (14.7) |
| K6 score (mean, SD) | 6.0 | (5.3) | 5.2 | (5.7) | 3.1 | (3.9) | 5.5 | (3.7) | 6.8 | (4.4) | 11.8 | (5.1) | 12.3 | (5.4) | 6.4 | (6.38) |
| Basic Characteristics | Total | Recovered | Non-Recovered | p-Value (χ2/t) | |||
|---|---|---|---|---|---|---|---|
| (n = 333) | (n = 274) | (n = 59) | |||||
| n (%) | n (%) | n (%) | |||||
| Age (as of February 2018) | |||||||
| Less than 40 years old | 43 | (100.0) | 36 | (83.7) | 7 | (16.3) | |
| 40–64 years old | 154 | (100.0) | 130 | (84.4) | 24 | (15.6) | 0.52 (χ2 = 1.31) |
| 65 years old and more | 136 | (100.0) | 108 | (79.4) | 28 | (20.6) | |
| Gender | |||||||
| Male | 134 | (100.0) | 107 | (79.9) | 27 | (20.1) | 0.34 (χ2 = 0.91) |
| Female | 199 | (100.0) | 167 | (83.9) | 32 | (16.1) | |
| Education | |||||||
| Junior/Senior high school | 249 | (100.0) | 202 | (81.1) | 47 | (18.9) | 0.38 (χ2 = 0.76) |
| Vocational college, University | 82 | (100.0) | 70 | (85.4) | 12 | (14.6) | |
| Occupational category | |||||||
| Employed, Owner | 120 | (100.0) | 105 | (87.5) | 15 | (12.5) | |
| Part-time | 42 | (100.0) | 37 | (88.1) | 5 | (11.9) | |
| Homemaker | 64 | (100.0) | 57 | (89.1) | 7 | (10.9) | <0.01 (χ2 = 19.5) |
| Unemployed | 99 | (100.0) | 68 | (68.7) | 31 | (31.3) | |
| Living area as of 11 March 2011 | |||||||
| Evacuation area | 160 | (100.0) | 128 | (80.0) | 32 | (20.0) | 0.29 (χ2 = 1.10) |
| Non-evacuation area | 173 | (100.0) | 146 | (84.4) | 27 | (15.6) | |
| Living with family member | 0.90 (χ2 = 0.02) | ||||||
| Living with family | 292 | (100.0) | 243 | (83.2) | 49 | (16.8) | |
| Single life | 34 | (100.0) | 28 | (82.4) | 6 | (17.6) | |
| Current psychological distress (K6: Kessler6) | |||||||
| K6 score ≥ 13 | 40 | (100.0) | 13 | (32.5) | 27 | (67.5) | <0.01 (χ2 = 79.2) |
| K6 score ≤ 12 | 280 | (100.0) | 251 | (89.6) | 29 | (10.4) | |
| K6 score (mean, SD) | 6.0 | (5.3) | 4.8 | (4.1) | 12.1 | (5.2) | <0.01 (t = 9.81) |
| Disaster-Related Experience and Current Economic Status | Total | Recovered | Non-Recovered | p-Value (χ2) | |||
|---|---|---|---|---|---|---|---|
| (n = 333) | (n = 274) | (n = 59) | |||||
| n (%) | n (%) | n (%) | |||||
| Evacuation | |||||||
| Experienced | 176 | (100.0) | 144 | (81.8) | 32 | (18.2) | 0.82 (χ2 = 0.06) |
| Never | 157 | (100.0) | 130 | (82.8) | 27 | (17.2) | |
| Separation from family members | |||||||
| Experienced | 103 | (100.0) | 82 | (79.6) | 21 | (20.4) | 0.39 (χ2 = 0.73) |
| Never | 230 | (100.0) | 192 | (83.5) | 38 | (16.5) | |
| House damage (severe/partial collapse) | |||||||
| Experienced | 117 | (100.0) | 93 | (79.5) | 24 | (20.5) | 0.33 (χ2 = 0.97) |
| Never | 216 | (100.0) | 181 | (83.8) | 35 | (16.2) | |
| Loss of family, relatives or friends | |||||||
| Experienced | 59 | (100.0) | 41 | (69.5) | 18 | (30.5) | 0.01 (χ2 = 8.05) |
| Never | 274 | (100.0) | 233 | (85.0) | 41 | (15.0) | |
| Disaster-related loss of employment | <0.01 (χ2 = 17.9) | ||||||
| Experienced | 81 | (100.0) | 54 | (66.7) | 27 | (33.3) | |
| Never | 252 | (100.0) | 220 | (87.3) | 32 | (12.7) | |
| Economic status (Afford to live in current economic status) | |||||||
| Difficult | 110 | (100.0) | 76 | (69.1) | 34 | (30.9) | <0.01 (χ2 = 20.4) |
| Enough/Average | 221 | (100.0) | 197 | (89.1) | 24 | (10.9) | |
| Current Health Status, Lifestyle and Social Status | Total | Recovered | Non-Recovered | p-Value (χ2) | |||
|---|---|---|---|---|---|---|---|
| (n = 333) | (n = 274) | (n = 59) | |||||
| n (%) | n (%) | n (%) | |||||
| General subjective health status | |||||||
| Very well/Well/Unremarkable | 249 | (100.0) | 228 | (91.6) | 21 | (8.4) | <0.01 (χ2 = 61.6) |
| Poor/Very poor | 81 | (100.0) | 43 | (53.1) | 38 | (46.9) | |
| Sleep condition | |||||||
| Satisfied with sleep condition | 149 | (100.0) | 137 | (91.9) | 12 | (8.1) | <0.01 (χ2 = 17.3) |
| Dissatisfied | 184 | (100.0) | 137 | (74.5) | 47 | (25.5) | |
| Changes in physical activities | |||||||
| Increase/No change | 203 | (100.0) | 182 | (89.7) | 21 | (10.3) | <0.01 (χ2 = 19.7) |
| Decrease | 125 | (100.0) | 88 | (70.4) | 37 | (29.6) | |
| Changes in alcohol consumption | |||||||
| Increase | 42 | (100.0) | 33 | (78.6) | 9 | (21.4) | |
| No change | 111 | (100.0) | 95 | (85.6) | 16 | (14.4) | 0.22 (χ2 = 4.47) |
| Decrease | 42 | (100.0) | 31 | (73.8) | 11 | (26.2) | |
| Non-drinker | 109 | (100.0) | 94 | (86.2) | 15 | (13.8) | |
| Frequency of laughing | |||||||
| Almost everyday | 80 | (100.0) | 76 | (95.0) | 4 | (5.0) | <0.01 (χ2 = 11.7) |
| Less that 1–5 times/week | 253 | (100.0) | 198 | (78.3) | 55 | (21.7) | |
| Social network status | |||||||
| Social interaction with friends from pre-disaster | |||||||
| Agree | 190 | (100.0) | 173 | (91.1) | 17 | (8.9) | <0.01 (χ2 = 16.1) |
| Disagree/Neither or not | 132 | (100.0) | 94 | (71.2) | 38 | (28.8) | |
| Place to communicate about the disaster | |||||||
| Agree | 119 | (100.0) | 104 | (87.4) | 15 | (12.6) | 0.06 (χ2 = 3.59) |
| Disagree/Neither or not | 205 | (100.0) | 162 | (79.0) | 43 | (21.0) | |
| Social roles through daily activities | |||||||
| Agree | 138 | (100.0) | 129 | (93.5) | 9 | (6.5) | <0.01 (χ2 = 21.4) |
| Disagree/Neither or not | 189 | (100.0) | 139 | (73.5) | 50 | (26.5) | |
| Relative Factors with Mental Health Recovery | Model 1 (n = 331) | Model 2 (n = 310) | ||||||
|---|---|---|---|---|---|---|---|---|
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | |||||
| Basic characteristics | ||||||||
| Age | 1.02 | (0.99–1.04) | 0.15 | 1.00 | (0.98–1.03) | 0.78 | ||
| Gender | Male | 0.72 | (0.39–1.35) | 0.31 | 0.72 | (0.33–1.57) | 0.41 | |
| Female (Ref.) | 1.00 | 1.00 | ||||||
| Living area as of 11 March 2011 | Evacuation | 0.97 | (0.82–1.16) | 0.77 | 0.97 | (0.78–1.22) | 0.82 | |
| non-evacuation (Ref.) | 1.00 | 1.00 | ||||||
| Disaster-related experience | ||||||||
| Loss of family, relatives or friends | Experienced | 0.84 | (0.70–1.02) | 0.08 | 0.89 | (0.71–1.13) | 0.34 | |
| Never (Ref.) | 1.00 | 1.00 | ||||||
| Disaster-related loss of employment | Experienced | 0.75 | (0.63–0.89) | <0.01 | 0.80 | (0.65–0.99) | 0.04 | |
| Never (Ref.) | 1.00 | 1.00 | ||||||
| Economic status | ||||||||
| Afford to live in current economic status | Difficult | 0.70 | (0.59–0.82) | <0.01 | 0.80 | (0.65–0.98) | 0.03 | |
| Enough/Average (Ref.) | 1.00 | 1.00 | ||||||
| Current health status and lifestyle | ||||||||
| General subjective health status | Well/Unremarkable | 1.47 | (1.20–1.80) | <0.01 | ||||
| Poor/Very poor (Ref.) | 1.00 | |||||||
| Sleep condition | Satisfied with sleep | 1.09 | (0.86–1.37) | 0.49 | ||||
| Dissatisfied (Ref.) | 1.00 | |||||||
| Changes in physical activities | Increase/No change | 1.23 | (1.01–1.50) | 0.04 | ||||
| Decrease (Ref.) | 1.00 | |||||||
| Frequency of laughing | Almost everyday | 1.19 | (0.85–1.67) | 0.30 | ||||
| Less that 1–5 times/week (Ref.) | 1.00 | |||||||
| Social network status | ||||||||
| Social interaction with friends | Agree | 1.25 | (1.00–1.55) | 0.05 | ||||
| Disagree/Neither or not (Ref.) | 1.00 | |||||||
| Place to communicate about the disaster | Agree | 0.81 | (0.63–1.03) | 0.08 | ||||
| Disagree/Neither or not (Ref.) | 1.00 | |||||||
| Social roles through daily activities | Agree | 1.44 | (1.14–1.82) | <0.01 | ||||
| Disagree/Neither or not (Ref.) | 1.00 | |||||||
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Orui, M.; Nakajima, S.; Takebayashi, Y.; Ito, A.; Momoi, M.; Maeda, M.; Yasumura, S.; Ohto, H. Mental Health Recovery of Evacuees and Residents from the Fukushima Daiichi Nuclear Power Plant Accident after Seven Years—Contribution of Social Network and a Desirable Lifestyle. Int. J. Environ. Res. Public Health 2018, 15, 2381. https://doi.org/10.3390/ijerph15112381
Orui M, Nakajima S, Takebayashi Y, Ito A, Momoi M, Maeda M, Yasumura S, Ohto H. Mental Health Recovery of Evacuees and Residents from the Fukushima Daiichi Nuclear Power Plant Accident after Seven Years—Contribution of Social Network and a Desirable Lifestyle. International Journal of Environmental Research and Public Health. 2018; 15(11):2381. https://doi.org/10.3390/ijerph15112381
Chicago/Turabian StyleOrui, Masatsugu, Satomi Nakajima, Yui Takebayashi, Akiko Ito, Maho Momoi, Masaharu Maeda, Seiji Yasumura, and Hitoshi Ohto. 2018. "Mental Health Recovery of Evacuees and Residents from the Fukushima Daiichi Nuclear Power Plant Accident after Seven Years—Contribution of Social Network and a Desirable Lifestyle" International Journal of Environmental Research and Public Health 15, no. 11: 2381. https://doi.org/10.3390/ijerph15112381