Heat-Related Health Impacts under Scenarios of Climate and Population Change

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Population Projections
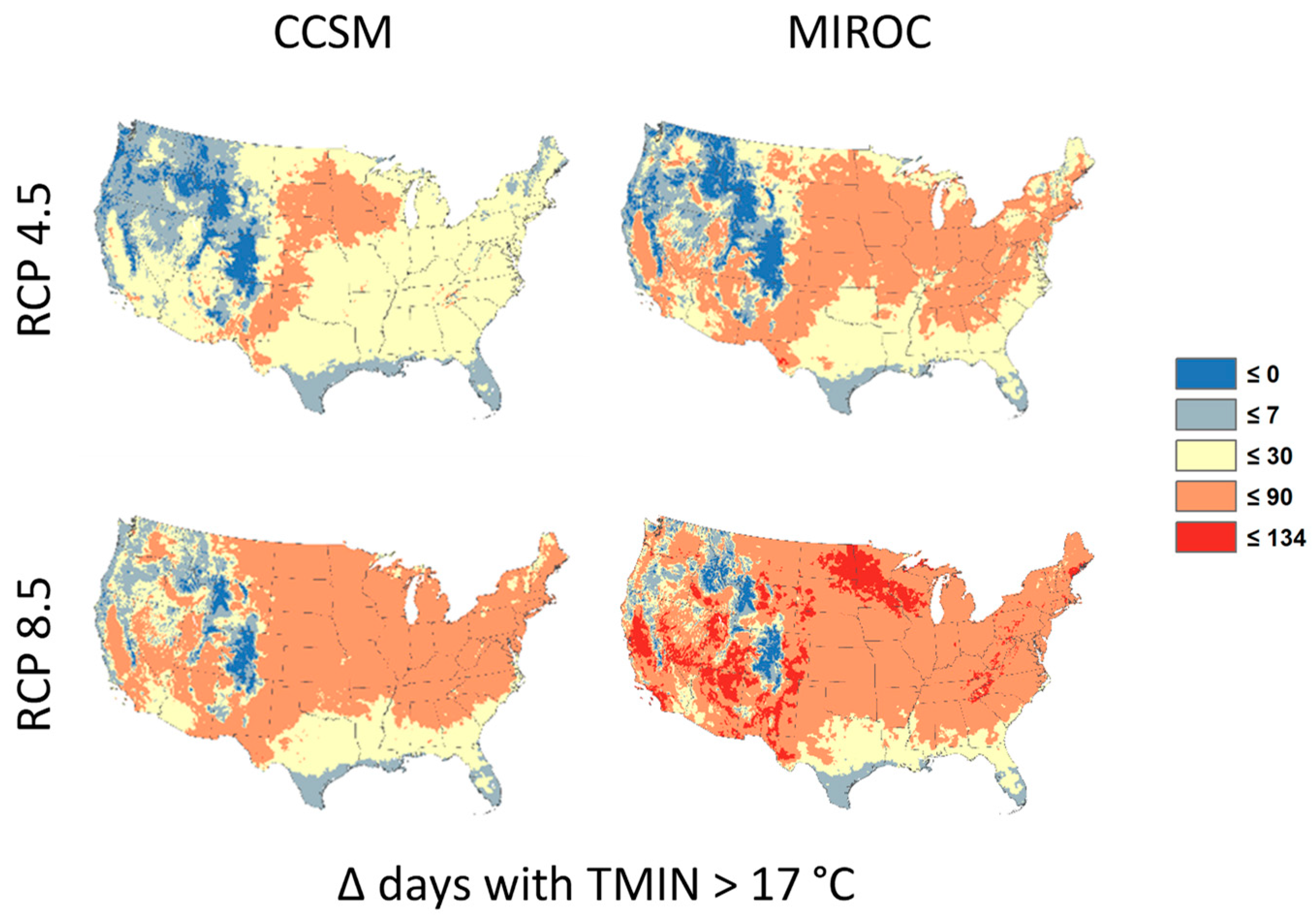
2.2. Climate Change Projections
2.3. Quantifying Heat-Related Mortality
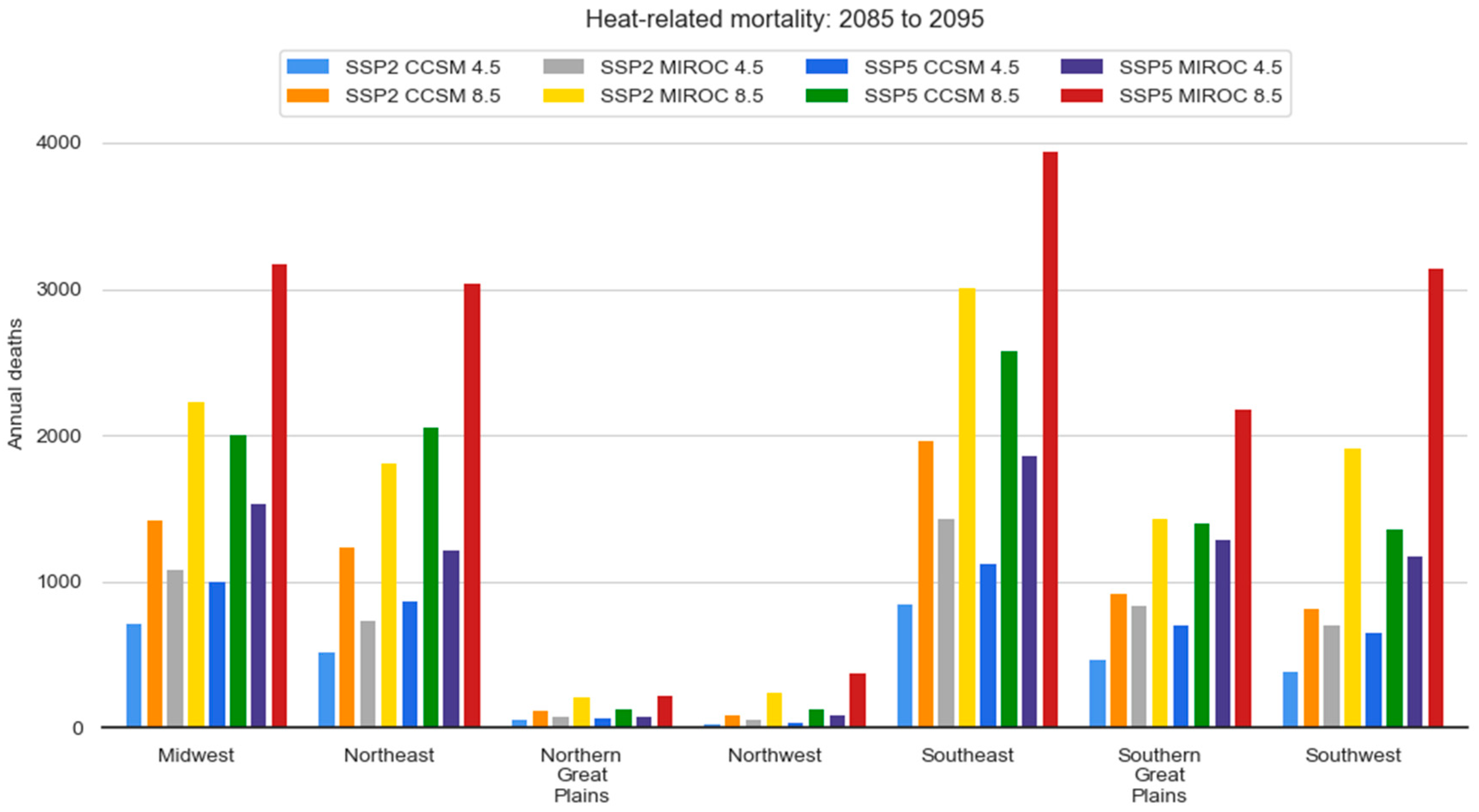
3. Results
Regional Results
4. Discussion
- the spread in projections of future climate across different climate models;
- the spread in projections of future climate across different greenhouse gas scenarios;
- consideration of changes in population and demographics (and the spread across different projections of changes in these factors);
- adequate resolution of finer-scale UHI effects on top of regional climate change;
- the choice of specific mortality model used, and the way in which the mortality model was calibrated with observed data;
- if adaptation (autonomous or planned) was considered, and the specific adaptations considered.
- choice of climate model;
- choice of future greenhouse gas trajectory;
- and future changes in population size and geographic distribution.
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Centers for Disease Control and Prevention. Heat-Related Mortality—Chicago, July 1995. Morb. Mortal. Wkly. Rep. 1995, 44, 577–579. [Google Scholar]
- Semenza, J.C.; Rubin, C.H.; Falter, K.H.; Selanikio, J.D.; Flanders, W.D.; Howe, H.L.; Wilhelm, J.L. Heat-related deaths during the July 1995 heat wave in Chicago. N. Engl. J. Med. 1996, 335, 84–90. [Google Scholar] [CrossRef] [PubMed]
- Semenza, J.C.; McCullough, J.E.; Flanders, W.D.; McGeehin, M.A.; Lumpkin, J.R. Excess hospital admissions during the July 1995 heat wave in Chicago. Am. J. Prev. Med. 1999, 16, 269–277. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Heat-related deaths—Philadelphia and United States, 1993–1994. Morb. Mortal. Wkly. Rep. 1994, 43, 453–455. [Google Scholar]
- Knowlton, K.; Rotkin-Ellman, M.; King, G.; Margolis, H.G.; Smith, D.; Solomon, G.; Trent, R.; English, P. The 2006 California Heat Wave: Impacts on Hospitalizations and Emergency Department Visits. Environ. Health Perspect. 2009, 117, 61–67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ostro, B.D.; Roth, L.A.; Green, R.S.; Basu, R. Estimating the mortality effect of the July 2006 California heat wave. Environ. Res. 2009, 109, 614–619. [Google Scholar] [CrossRef] [PubMed]
- Kilbourne, E.M. Heat waves and hot environments. In The Public Health Consequences of Disasters; Noji, K., Ed.; Oxford University Press: New York, NY, USA, 1997; pp. 245–269. [Google Scholar]
- Basu, R.; Pearson, D.; Malig, B.; Broadwin, R.; Green, R. The effect of high ambient temperature on emergency room visits. Epidemiology 2012, 23, 813–820. [Google Scholar] [CrossRef] [PubMed]
- Choudhary, E.; Vaidyanathan, A. Heat stress illness hospitalizations—Environmental public health tracking program, 20 states, 2001–2010. MMWR Surveill. Summ. 2014, 63, 1–10. [Google Scholar] [PubMed]
- Fechter-Leggett, E.D.; Vaidyanathan, A.; Choudhary, E. Heat Stress Illness Emergency Department Visits in National Environmental Public Health Tracking States, 2005–2010. J. Community Health 2016, 41, 51–69. [Google Scholar] [CrossRef] [PubMed]
- Hess, J.J.; Saha, S.; Luber, G. Summertime acute heat illness in U.S. emergency departments from 2006 through 2010: Analysis of a nationally representative sample. Environ. Health Perspect. 2014, 122, 1209–1215. [Google Scholar] [CrossRef] [PubMed]
- Saha, S.; Brock, J.W.; Vaidyanathan, A.; Easterling, D.R.; Luber, G. Spatial variation in hyperthermia emergency department visits among those with employer-based insurance in the United States—A case-crossover analysis. Environ. Health 2015, 14, 20. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Gu, S.; Bi, P.; Yang, J.; Liu, Q. Heat waves and morbidity: Current knowledge and further directions—A comprehensive literature review. Int. J. Environ. Res. Public Health 2015, 12, 5256–5283. [Google Scholar] [CrossRef] [PubMed]
- Gronlund, C.J.; Zanobetti, A.; Schwartz, J.D.; Wellenius, G.A.; O’Neill, M.S. Heat, heat waves, and hospital admissions among the elderly in the United States, 1992–2006. Environ. Health Perspect. 2014, 122, 1187–1192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sheridan, S.C.; Lin, S. Assessing variability in the impacts of heat on health outcomes in New York City over time, season, and heat-wave duration. EcoHealth 2014, 11, 512–515. [Google Scholar] [CrossRef] [PubMed]
- Curriero, F.C.; Heiner, K.S.; Samet, J.M.; Zeger, S.L.; Strug, L.; Patz, J.A. Temperature and mortality in 11 cities of the eastern United States. Am. J. Epidemiol. 2002, 155, 80–87. [Google Scholar] [CrossRef] [PubMed]
- Braga, A.; Zanobetti, A.; Schwartz, J. The effect of weather on respiratory and cardiovascular deaths in 12 U.S. cities. Environ. Health Perspect. 2002, 110, 859–863. [Google Scholar] [CrossRef] [PubMed]
- Basu, R.; Samet, J.M. Relation between elevated ambient temperature and mortality: A review of epidemiologic evidence. Epidemiol. Rev. 2002, 24, 190–202. [Google Scholar] [CrossRef] [PubMed]
- Basu, R. High ambient temperature and mortality: A review of epidemiological studies from 2001 to 2008. Environ. Health 2009, 8, 40. [Google Scholar] [CrossRef] [PubMed]
- Medina-Ramon, M.; Schwartz, J. Temperature, temperature extremes, and mortality: A study of acclimatization and effect modification in 50 United States cities. Occup. Environ. Med. 2007, 64, 827–833. [Google Scholar] [CrossRef] [PubMed]
- Zanobetti, A.; Schwartz, J. Temperature and mortality in nine US cities. Epidemiology 2008, 19, 563–570. [Google Scholar] [CrossRef] [PubMed]
- Anderson, B.G.; Bell, M.L. Weather-related mortality: How heat, cold, and heat waves affect mortality in the United States. Epidemiology 2009, 20, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Anderson, B.G.; Bell, M.L. Heat waves in the United States: Mortality risk during heat waves and effect modification by heat wave characteristics in 43 U.S. communities. Environ. Health Perspect. 2011, 119, 210–218. [Google Scholar] [CrossRef] [PubMed]
- U.S. Global Change Research Program. Climate Science Special Report: Fourth National Climate Assessment; Wuebbles, D., Fahey, D., Hibbard, K., Dokken, D., Stewart, B., Maycock, T., Eds.; U.S. Global Change Research Program: Washington, DC, USA, 2017; Volume 1, 470p.
- Intergovernmental Panel on Climate Change. Climate Change 2014: Impacts, Adaptation, and Vulnerability. Part A: Global and Sectoral Aspects; Field, C., Barros, V., Dokken, D., Mach, K., Mastrandrea, M., Bilir, T., Chatterjee, M., Ebi, K., Estrada, Y., Genova, R., et al., Eds.; Cambridge University Press: Cambridge, UK; New York, NY, USA, 2014; pp. 1–32. [Google Scholar]
- Sarofim, M.C.; Saha, S.; Hawkins, M.D.; Mills, D.M.; Hess, J.; Horton, R. Temperature-related death and illness. In The Impacts of Climate Change on Human Health in the United States: A Scientific Assessment; Crimmins, A., Balbus, J., Gamble, J., Beard, C., Bell, J., Dodgen, D., Eisen, R., Fann, N., Hawkins, M., Herring, S., et al., Eds.; U.S. Global Change Research Program: Washington, DC, USA, 2016; pp. 43–68. [Google Scholar]
- Sanderson, M.; Arbuthnott, K.; Kovats, S.; Hajat, S.; Falloon, P. The use of climate information to estimate future mortality from high ambient temperature: A systematic literature review. PLoS ONE 2017, 12, 1–34. [Google Scholar] [CrossRef] [PubMed]
- Mills, D.; Schwartz, J.; Lee, M.; Sarofim, M.; Jones, R.; Lawson, M. Climate change impacts on extreme temperature mortality in select metropolitan areas in the United States. Clim. Chang. 2015, 131, 83–95. [Google Scholar] [CrossRef]
- Gosling, S.N.; McGregor, G.R.; Lowe, J.A. The benefits of quantifying climate model uncertainty in climate change impacts assessment: An example with heat-related mortality change estimates. Clim. Chang. 2012, 112, 217–231. [Google Scholar] [CrossRef]
- Knowlton, K.; Lynn, B.; Goldberg, R.A.; Rosenzweig, C.; Hogrefe, C.; Rosenthal, J.K.; Kinney, P.L. Projecting heat-related mortality impacts under a changing climate in the New York City region. Am. J. Public Health 2007, 97, 2028–2034. [Google Scholar] [CrossRef] [PubMed]
- Voorhees, A.S.; Fann, N.; Fulcher, C.; Dolwick, P.; Hubbell, B.; Bierwagen, B.; Morefield, P. Climate change-related temperature impacts on warm season heat mortality: A proof-of-concept methodology using BenMAP. Environ. Sci. Technol. 2011, 45, 1450–1457. [Google Scholar] [CrossRef] [PubMed]
- Flynn, A.; McGreevy, C.; Mulkerrin, E.C. Why do older patients die in a heatwave? Q. J. Med. 2005, 98, 227–229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McGeehin, M.A.; Mirabelli, M. The potential impacts of climate variability and change on temperature-related morbidity and mortality in the United States. Environ. Health Perspect. 2001, 109, 185–189. [Google Scholar] [PubMed]
- Klinenberg, E. Review of heat wave: Social autopsy of disaster in Chicago. N. Engl. J. Med. 2003, 348, 666–667. [Google Scholar] [CrossRef] [PubMed]
- Luber, G.; McGeehin, M. Climate change and extreme heat events. Am. J. Prev. Med. 2008, 35, 429–435. [Google Scholar] [CrossRef] [PubMed]
- Naughton, M.P.; Henderson, A.; Mirabelli, M.C.; Kasier, R.; Wilhelm, J.L.; Kieszak, S.M.; Rubin, C.H.; McGeehin, M.A. Heat-related mortality during a 1999 heat wave in Chicago. Am. J. Prev. Med. 2002, 22, 221–227. [Google Scholar] [CrossRef]
- Environmental Benefits Mapping and Analysis Program–Community Edition (BenMAP–CE). Available online: https://www.epa.gov/benmap (accessed on 26 September 2018).
- Taylor, K.E.; Stouffer, R.J.; Meehl, G.A. An overview of CMIP5 the experiment design. Bull. Am. Meteorol. Soc. 2012, 93, 485–498. [Google Scholar] [CrossRef]
- Moss, R.H.; Edmonds, J.A.; Hibbard, K.A.; Manning, M.R.; Rose, S.K.; Van Vuuren, D.P.; Carter, T.R.; Emori, S.; Kainuma, M.; Kram, T.; et al. The next generation of scenarios for climate change research and assessment. Nature 2010, 463, 747–756. [Google Scholar] [CrossRef] [PubMed]
- Locating and Selecting Scenarios Online (LASSO). Available online: https://lasso.epa.gov (accessed on 2 July 2018).
- U.S. Environmental Protection Agency. Updates to the Demographic and Spatial Allocation Models to Produce Integrated Climate and Land Use Scenarios (ICLUS) Version 2; EPA/600/R-16/366F; National Center for Environmental Assessment: Washington, DC, USA, 2017.
- O’Neill, B.C.; Kriegler, E.; Ebi, K.L.; Kemp-Benedict, E.; Riahi, K.; Rothman, D.S.; van Ruijven, B.J.; van Vuuren, D.P.; Birkmann, J.; Kok, K.; et al. The roads ahead: Narratives for shared socioeconomic pathways describing world futures in the 21st century. Glob. Environ. Chang. 2017, 42, 169–180. [Google Scholar] [CrossRef]
- Weaver, C.P.; Moss, R.H.; Ebi, K.L.; Gleick, P.H.; Stern, P.C.; Tebaldi, C.; Wilson, R.S.; Arvai, J.L. Reframing climate change assessments around risk: Recommendations for the US National Climate Assessment. Environ. Res. Lett. 2017, 12, 080201. [Google Scholar] [CrossRef]
- King, D.; Schrag, D.; Zhou, D.; Ye, Q.; Ghosh, A. Climate Change: A Risk Assessment; Hynard, J., Rodger, T., Eds. Available online: http://www.csap.cam.ac.uk/media/uploads/files/1/climate-change--a-risk-assessment-v11.pdf (accessed on 20 September 2018).
- Kunreuther, H.; Heal, G.; Allen, J.; Edenhofer, O.; Field, C.B.; Yohe, G. Risk management and climate change. Nat. Clim. Chang. 2013, 3, 447–450. [Google Scholar] [CrossRef] [Green Version]
- National Academies of Sciences, Engineering, and Medicine. Characterizing Risk in Climate Change Assessments: Summary of a Workshop for the U.S. Global Change Research Program; The National Academies Press: Washington, DC, USA, 2016. [Google Scholar]
- Kirchhoff, C.J.; Lemos, M.C.; Dessai, S. Actionable knowledge for environmental decision making: Broadening the usability of climate science. Ann. Rev. Environ. Resour. 2013, 38, 393–414. [Google Scholar] [CrossRef]
- U.S. Environmental Protection Agency. Climate Change in the United States: Benefits of Global Action; U.S. Environmental Protection Agency: Washington, DC, USA, 2015.
- O’Neill, B.C.; Done, J.M.; Gettelman, A.; Lawrence, P.; Lehner, F.; Lamarque, J.F.; Lin, L.; Monaghan, A.J.; Oleson, K.; Ren, X.; et al. The benefits of reduced anthropogenic Climate ChangE (BRACE): A synthesis. Clim. Change. 2018, 146, 287–301. [Google Scholar] [CrossRef]
- Post, E.S.; Grambsch, A.; Weaver, C.; Morefield, P.; Huang, J.; Leung, L.Y.; Nolte, C.G.; Adams, P.; Liang, X.Z.; Zhu, J.H.; et al. Variation in estimated ozone-related health impacts of climate change due to modeling choices and assumptions. Environ. Health Perspect. 2012, 120, 1559–1564. [Google Scholar] [CrossRef] [PubMed]
- Wittgenstein Centre Data Explorer. Available online: http://dataexplorer.wittgensteincentre.org/shiny/wic/ (accessed on 26 September 2018).
- Scenarios for the National Climate Assessment. Available online: https://scenarios.globalchange.gov (accessed on 26 September 2018).
- U.S. Population Migration Data. Available online: https://www.irs.gov/statistics/soi-tax-stats-migration-data (accessed on 20 September 2018).
- Cartographic Boundary Shapefiles—Metropolitan and Micropolitan Statistical Areas and Related Statistical Areas. Available online: https://www.census.gov/geo/maps-data/data/cbf/cbf_msa.html (accessed on 26 September 2018).
- Plane, D.A.; Henrie, C.J.; Perry, M.J. Migration up and down the urban hierarchy and across the life course. Proc. Natl. Acad. Sci. USA 2005, 102, 15313–15318. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manson, G.; Groop, R. U.S. intercounty migration in the 1990s: People and income move down the urban hierarchy. Prof. Geogr. 2000, 52, 493–504. [Google Scholar] [CrossRef]
- Cannon, A. Selecting GCM scenarios that span the range of changes in a multimodel ensemble: Application to CMIP5 climate extremes indices. J. Clim. 2015, 28, 1260–1267. [Google Scholar] [CrossRef]
- Salathé, E.P.; Mote, P.W.; Wiley, M.W. Review of scenario selection and downscaling methods for the assessment of climate change impacts on hydrology in the United States pacific northwest. Int. J. Climatol. 2007, 27, 1611–1621. [Google Scholar] [CrossRef] [Green Version]
- Stainforth, D.A.; Downing, T.E.; Washington, R.; Lopez, A.; New, M. Issues in the interpretation of climate model ensembles to inform decisions. Philos. Trans. A Math Phys. Eng. Sci. 2007, 365, 2163–2177. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pierce, D.W.; Cayan, D.R.; Thrasher, B.L. Statistical downscaling using localized constructed analogs (LOCA). J. Hydrometeorol. 2014, 15, 2558–2585. [Google Scholar] [CrossRef]
- Downscaled CMIP3 and CMIP5 Climate and Hydrology Projections. Available online: https://gdo-dcp.ucllnl.org/downscaled_cmip_projections/dcpInterface.html (accessed on 9 September 2018).
- CDC WONDER. Available online: https://wonder.cdc.gov (accessed on 27 September 2018).
- Johnson, T.; Butcher, J.; Deb, D.; Faizullabhoy, M.; Hummel, P.; Kittle, J.; McGinnis, S.; Mearns, L.O.; Nover, D.; Parker, A.; et al. Modeling streamflow and water quality sensitivity to climate change and urban development in 20 U.S. watersheds. J. Am. Water Resour. Assoc. 2015, 51, 1321–1341. [Google Scholar] [CrossRef]
- Nover, D.M.; Witt, J.W.; Butcher, J.B.; Johnson, T.E.; Weaver, C.P. The effects of downscaling method on the variability of simulated watershed response to climate change in five U.S. basins. Earth Interact. 2016, 20, 1–27. [Google Scholar] [CrossRef] [PubMed]
- Oke, T.R. The energetic basis of the urban heat island. Q. J. R. Meteorol. Soc. 1982, 108, 1–24. [Google Scholar] [CrossRef]
- Georgescu, M.; Morefield, P.E.; Bierwagen, B.G.; Weaver, C.P. Urban adaptation can roll back warming of emerging megapolitan regions. Proc. Natl. Acad. Sci. USA 2014, 111, 2909–2914. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kalkstein, L.S. Health and climate change: Direct impacts in cities. Lancet 1993, 342, 1397–1399. [Google Scholar] [CrossRef]
- Kalkstein, L.S.; Greene, S.; Mills, D.M.; Samenow, J. An evaluation of the progress in reducing heat-related mortality in major U.S. cities. Nat. Hazards 2015, 56, 113–129. [Google Scholar] [CrossRef]
- Arbuthnott, K.A.; Hajat, S.; Heaviside, C.; Vardoulakis, S. Changes in population susceptibility to heat and cold over time: Assessing adaptation to climate change. Environ. Health 2016, 15, 73–93. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, J.D.; Lee, M.; Kinney, P.L.; Yang, S.; Mills, D.; Sarofim, M.C.; Jones, R.; Streeter, R.; St. Juliana, A.; Peers, J.; et al. Projections of temperature-attributable premature deaths in 209 U.S. cities using a cluster-based Poisson approach. Environ. Health 2015, 14, 85. [Google Scholar] [CrossRef] [PubMed]
- Hondula, D.M.; Balling, R.C.; Vanos, J.K.; Georgescu, M. Rising temperatures, human health, and the role of adaptation. Curr. Clim. Chang. Rep. 2015, 1, 144–154. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Version/Component | BenMAP v4 | BenMAP-CE |
|---|---|---|
| Language | Delphi | C# |
| Source code | Proprietary | https://github.com/BenMAPCE/BenMAP-CE |
| Algorithm used to quantify health impacts | Health impact function | Health impact function |
| Database of demographic, health and economic data | Firebird SQL | Firebird SQL |
| Geographic information system | Tatuk (proprietary) | DotSpatial (open source) |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Morefield, P.E.; Fann, N.; Grambsch, A.; Raich, W.; Weaver, C.P. Heat-Related Health Impacts under Scenarios of Climate and Population Change. Int. J. Environ. Res. Public Health 2018, 15, 2438. https://doi.org/10.3390/ijerph15112438
Morefield PE, Fann N, Grambsch A, Raich W, Weaver CP. Heat-Related Health Impacts under Scenarios of Climate and Population Change. International Journal of Environmental Research and Public Health. 2018; 15(11):2438. https://doi.org/10.3390/ijerph15112438
Chicago/Turabian StyleMorefield, Philip E., Neal Fann, Anne Grambsch, William Raich, and Christopher P. Weaver. 2018. "Heat-Related Health Impacts under Scenarios of Climate and Population Change" International Journal of Environmental Research and Public Health 15, no. 11: 2438. https://doi.org/10.3390/ijerph15112438