Influence of Active Exposure to Tobacco Smoke on Nitric Oxide Status of Pregnant Women

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Blood Sampling and Biochemical Analysis
2.3. Statistical Analysis
3. Results
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Polakowska, M.; Kaleta, D.; Piotrowski, W.; Topór-Mądry, R.; Puch-Walczak, A.; Niklas, A.; Bielecki, W.; Kozakiewicz, K.; Pająk, A.; Tykarski, A.; et al. Tobacco smoking in Poland in the years from 2003 to 2014. Multi-centre National Population Health Examination Survey (WOBASZ). Pol. Arch. Inter. Med. 2017, 127, 91–99. [Google Scholar] [CrossRef]
- Laskowska-Klita, T.; Chełchowska, M.; Ołtarzewski, M.; Gajewska, J.; Ambroszkiewicz, J. The effect of tobacco smoking during pregnancy on birth mass on the basis of population study—Preliminary results. Prz. Lek. 2010, 67, 830–834. [Google Scholar] [PubMed]
- Polanska, K.; Krol, A.; Kaluzny, P.; Ligocka, D.; Mikolajewska, K.; Shaheen, S.; Walton, R.; Hanke, W. Estimation of cut-off points for active and passive smoking during pregnancy-polish mother and child cohort (REPRO_PL). Int. J. Environ. Res. Public Health 2016, 13, 1216. [Google Scholar] [CrossRef] [PubMed]
- Król, M.; Florek, E.; Piekoszewski, W.; Bokiniec, R.; Kornacka, M.K. The impact of intrauterine tobacco exposure on the cerebral mass of the neonate based on the measurement of head circumference. Brain Behav. 2012, 2, 243–248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kharkova, O.A.; Grjibovski, A.M.; Krettek, A.; Nieboer, E.; Odland, J.O. Effect of smoking behawior before and during pregnancy on selected birth outcomes among singleton full-term pregnancy: A Murmansk County Birth Registry Study. Int. J. Environ. Res. Public Health 2017, 14, 867. [Google Scholar] [CrossRef] [PubMed]
- Pereira, P.P.; Da Mata, F.A.; Figueiredo, A.C.; de Andrade, K.R.; Pereira, M.G. Maternal active smoking during pregnancy and low birth weight in the Americas: A systematic review and meta-analysis. Nicotine Tob. Res. 2017, 19, 497–505. [Google Scholar] [CrossRef] [PubMed]
- Dietz, P.M.; England, L.J.; Shapiro-Mendoza, C.K.; Tong, V.T.; Farr, S.L.; Callaghan, W.M. Infant morbidity and mortality attributable to prenatal smoking in the U.S. Am. J. Prev. Med. 2010, 39, 45–52. [Google Scholar] [CrossRef]
- Wisborg, K.; Kesmodel, U.; Henriksen, T.B.; Olsen, S.F.; Secher, N.J. Exposure to tobacco smoke in utero and the risk of stillbirth and death in the first year of life. Am. J. Epidemiol. 2001, 154, 322–327. [Google Scholar] [CrossRef]
- Leite, M.; Albieri, V.; Kjaer, S.K.; Jensen, A. Maternal smoking in pregnancy and risk for congenital malformations: results of a Danish register-based cohort study. Acta Obstet. Gynecol. Scand. 2014, 93, 825–834. [Google Scholar] [CrossRef]
- Mennella, J.A.; Yourshaw, L.M.; Morgan, L.K. Breastfeeding and smoking: short-term effects on infant feeding and sleep. Pediatrics 2007, 120, 497–502. [Google Scholar] [CrossRef]
- Talati, A.; Wickramaratne, P.J.; Wesselhoeft, R.; Weissman, M.M. Prenatal tobacco exposure, birthweight, and offspring psychopathology. Psychiatry Res. 2017, 252, 346–352. [Google Scholar] [CrossRef] [PubMed]
- Polanska, K.; Krol, A.; Merecz-Kot, D.; Ligocka, D.; Mikolajewska, K.; Mirabella, F.; Chiarotti, F.; Calamandrei, G.; Hanke, W. Environmental Tobacco Smoke Exposure during Pregnancy and Child Neurodevelopment. Int. J. Environ. Res. Public Health 2017, 14, 796. [Google Scholar] [CrossRef] [PubMed]
- Albers, L.; Sobotzki, C.; Kuß, O.; Ajslev, T.; Batista, R.; Bettiol, H.; Brabin, B.; Buka, S.L.; Cardoso, V.C.; Clifton, V.L. Maternal smoking during pregnancy and offspring overweight: is there a dose-response relationship? An individual patient data meta-analysis. Int. J. Obes. (Lond). 2018, 42, 1249–1264. [Google Scholar] [CrossRef] [PubMed]
- Burke, H.; Leonardi-Bee, J.; Hashim, A.; Pine-Abata, H.; Chen, Y.; Cook, D.G.; Britton, J.R.; McKeever, T.M. Prenatal and passive smoke exposure and incidence of asthma and wheeze: systematic review and meta-analysis. Pediatrics 2012, 129, 735–744. [Google Scholar] [CrossRef] [PubMed]
- Brion, M.J.; Leary, S.D.; Lawlor, D.A.; Smith, G.D.; Ness, A.R. Modifiable maternal exposures and offspring blood pressure: a review of epidemiological studies of maternal age, diet, and smoking. Pediatr. Res. 2008, 63, 593–598. [Google Scholar] [CrossRef]
- Bao, W.; Michels, K.B.; Tobias, D.K.; Li, S.; Chavarro, J.E.; Gaskins, A.J.; Vaag, A.A.; Hu, F.B.; Zhang, C. Parental smoking during pregnancy and the risk of gestational diabetes in the daughter. Int. J. Epidemiol. 2016, 45, 160–169. [Google Scholar] [CrossRef] [Green Version]
- England, M.C.; Benjamin, A.; Abenhaim, H.A. Increased risk of preterm premature rupture of membranes at early gestational ages among maternal cigarette smokers. Am. J. Perinatol. 2013, 30, 821–826. [Google Scholar] [CrossRef]
- Shobeiri, F.; Jenabi, E. Smoking and placenta previa: a meta-analysis. J. Matern. Fetal. Neonatal. Med. 2017, 30, 2985–2990. [Google Scholar] [CrossRef]
- Nio-Kobayashi, J.; Abidin, H.B.; Brown, J.K.; Iwanaga, T.; Horne, A.W.; Duncan, W.C. Cigarette smoking alters sialylation in the Fallopian tube of women, with implications for the pathogenesis of ectopic pregnancy. Mol. Reprod. Dev. 2016, 83, 1083–1091. [Google Scholar] [CrossRef] [Green Version]
- Pineles, B.L.; Park, E.; Samet, J.M. Systematic review and meta-analysis of miscarriage and maternal exposure to tobacco smoke during pregnancy. Am. J. Epidemiol. 2014, 179, 807–823. [Google Scholar] [CrossRef]
- Ko, T.J.; Tsai, L.Y.; Chu, L.C.; Yeh, S.J.; Leung, C.; Chen, C.Y.; Chou, H.C.; Tsao, P.N.; Chen, P.C.; Hsieh, W.S. Parental smoking during pregnancy and its association with low birth weight, small for gestational age, and preterm birth offspring: a birth cohort study. Pediatr. Neonatol. 2014, 55, 20–27. [Google Scholar] [CrossRef] [PubMed]
- Ion, R.; Bernal, A.L. Smoking and Preterm Birth. Reprod. Sci. 2015, 22, 918–926. [Google Scholar] [CrossRef] [PubMed]
- Blatt, K.; Moore, E.; Chen, A.; Van Hook, J.; DeFranco, E.A. Association of reported trimester-specific smoking cessation with fetal growth restriction. Obstet. Gynecol. 2015, 125, 1452–1459. [Google Scholar] [CrossRef] [PubMed]
- Abraham, M.; Alramadhan, S.; Iniguez, C.; Duijts, L.; Jaddoe, V.W.; Den Dekker, H.T.; Crozier, S.; Godfrey, K.M.; Hindmarsh, P.; Vik, T. A systematic review of maternal smoking during pregnancy and fetal measurements with meta-analysis. PLoS ONE 2017, 12, e0170946. [Google Scholar] [CrossRef] [PubMed]
- Ardalic, D.; Stefanovic, A.; Kotur-Stevuljevic, J.; Vujović, A.; Spasić, S.; Spasojević-Kaliomanvska, V.; Jelić-Ivanović, Z.; Mandić-Marković, V.; Miković, Z.; Cerović, N. The influence of maternal smoking habits before pregnancy and antioxidative supplementation during pregnancy on oxidative stress status in non-complicated pregnancy. Adv. Clin. Exp. Med. 2014, 23, 575. [Google Scholar] [CrossRef] [PubMed]
- Al-Gubory, K.H.; Fowler, P.A.; Garrel, C. The roles of cellular reactive oxygen species, oxidative stress and antioxidants in pregnancy outcomes. Int. J. Biochem. Cell Biol. 2010, 42, 1634–1650. [Google Scholar] [CrossRef] [PubMed]
- Gromadzińska, J.; Polanska, K.; Kozlowska, L.; Mikolajewska, K.; Stelmach, I.; Jerzynska, J.; Stelmach, W.; Grzesiak, M.; Hanke, W.; Wasowicz, W. Vitamins A and E during pregnancy and allergy symptoms in an early childhood-lack of association with tobacco smoke exposure. Int. J. Environ. Res. Public Health 2018, 15, 1245. [Google Scholar] [CrossRef]
- Bizoń, A.; Milnerowicz, H. The effect of passive and active exposure to tobacco smoke on lipid profile parameters and the activity of certain membrane enzymes in the blood of women in the first trimester of pregnancy. Environ. Toxicol. Pharmacol. 2017, 53, 74–80. [Google Scholar] [CrossRef]
- Chełchowska, M.; Ambroszkiewicz, J.; Gajewska, J.; Laskowska-Klita, T.; Leibschang, J. The effect of tobacco smoking during pregnancy on plasma oxidant and antioxidant status in mother and newborn. Eur. J. Obstet. Gynecol. Reprod. Biol. 2011, 155, 132–136. [Google Scholar] [CrossRef]
- Orhon, F.S.; Ulukol, B.; Kahya, D.; Cengiz, B.; Baskan, S.; Tezcan, S. The influence of maternal smoking on maternal and newborn oxidant and antioxidant status. Eur. J. Pediatr. 2009, 168, 975–981. [Google Scholar] [CrossRef]
- Valavanidis, A.; Vlachogianni, T.; Fiotakis, K. Tobacco smoke: Involvement of reactive oxygen species and stable free radicals in mechanisms of oxidative damage, carcinogenesis and synergistic effects with other respirable particles. Int. J. Environ. Res. Public Health 2009, 6, 445–462. [Google Scholar] [CrossRef] [PubMed]
- Abdelghany, T.M.; Ismail, R.S.; Mansoor, F.A.; Zweier, J.R.; Lowe, F.; Zweier, J.L. Cigarette smoke constituents cause endothelial nitric oxide synthase dysfunction and uncoupling due to depletion of tetrahydrobiopterin with degradation of GTP cyclohydrolase. Nitric Oxide 2018, 76, 113–121. [Google Scholar] [CrossRef] [PubMed]
- Andersen, M.R.; Walker, L.R.; Stender, S. Reduced endothelial nitric oxide synthase activity and concentration in fetal umbilical veins from maternal cigarette smokers. Am. J. Obstet. Gynecol. 2004, 191, 346–351. [Google Scholar] [CrossRef] [PubMed]
- Khorram, O.; Han, G.; Magee, T. Cigarette smoke inhibits endometrial epithelial cell proliferation through a nitric oxide-mediated pathway. Fertil. Steril. 2010, 93, 257–263. [Google Scholar] [CrossRef] [PubMed]
- Mordwinkin, N.M.; Ouzounian, J.G.; Yedigarova, L.; Montoro, M.N.; Louie, S.G.; Rodgers, K.E. Alteration of endothelial function markers in women with gestational diabetes and their fetuses. J. Matern. Fetal Neonatal Med. 2013, 26, 507–512. [Google Scholar] [CrossRef] [PubMed]
- Shaamash, A.H.; Elsnosy, E.D.; Makhlouf, A.M.; Zakhari, M.M.; Ibrahim, O.A.; EL-dien, H.M. Maternal and fetal serum nitric oxide (NO) concentrations in normal pregnancy, pre-eclampsia and eclampsia. Int. J. Gynecol. Obstet. 2000, 68, 207–214. [Google Scholar] [CrossRef]
- Hodžić, J.; Izetbegović, S.; Muračević, B.; Iriškić, R.; Jović, H.Š. Nitric oxide biosynthesis during normal pregnancy and pregnancy complicated by preeclampsia. Med. Glas. (Zenica) 2017, 14, 211. [Google Scholar] [CrossRef]
- Andersen, M.R.; Simonsen, U.; Uldbjerg, N.; Aalkjaer, C.; Stender, S. Smoking cessation early in pregnancy and birth weight, length, head circumference, and endothelial nitric oxide synthase activity in umbilical and chorionic vessels. Circulation 2009, 119, 857–864. [Google Scholar] [CrossRef]
- Ozerol, E.; Ozerol, I.; Gokdeniz, R.; Temel, I.; Akyol, O. Effect of smoking on serum concentrations of total homocysteine, folate, vitamin B12, and nitric oxide in pregnancy: A preliminary study. Fetal Diagn. Ther. 2004, 19, 145–148. [Google Scholar] [CrossRef]
- Chełchowska, M.; Maciejewski, T.; Ambroszkiewicz, J.; Gajewska, J.; Łecka, R.; Laskowska-Klita, T.; Ołtarzewski, M. The effect of tobacco smoking on nitric oxide serum concentration in pregnant women and umbilical cord blood. Prz. Lek. 2009, 66, 648–651. [Google Scholar]
- Jarvis, M.J.; Tunstall-Pedoe, H.; Feyerabend, C.; Vesey, C.; Saloojee, Y. Comparison of tests used to distinguish smokers from non-smokers. Am. J. Public Health 1987, 77, 1435–1438. [Google Scholar] [CrossRef] [PubMed]
- Tatzber, F.; Griebenow, S.; Wonisch, W.; Winkler, R. Dual method for the determination of peroxidase activity and total peroxides-iodide leads to a significant increase of peroxidase activity in human sera. Anal. Biochem. 2003, 316, 147–153. [Google Scholar] [CrossRef]
- Ozler, A.; Ucmak, D.; Evsen, M.S.; Kaplan, I.; Elbey, B.; Arica, M.; Kaya, M. Immune mechanisms and the role of oxidative stress in intrahepatic cholestasis of pregnancy. Cent. Eur. J. Immunol. 2014, 39, 198–202. [Google Scholar] [CrossRef] [PubMed]
- Maciejczyk, M.; Szulimowska, J.; Skutnik, A.; Taranta-Janusz, K.; Wasilewska, A.; Wiśniewska, N.; Zalewska, A. Salivary Biomarkers of Oxidative Stress in Children with Chronic Kidney Disease. J. Clin. Med. 2018, 7, 209. [Google Scholar] [CrossRef] [PubMed]
- Barua, R.S.; Ambrose, J.A.; Srivastava, S.; DeVoe, M.C.; Eales-Reynolds, L.J. Reactive oxygen species are involved in smoking-induced dysfunction of nitric oxide biosynthesis and upregulation of endothelial nitric oxide synthase: An in vitro demonstration in human coronary artery endothelial cells. Circulation 2003, 107, 2342–2347. [Google Scholar] [CrossRef] [PubMed]
- Milnerowicz-Nabzdyk, E.; Bizoń, A. Effect of cigarette smoking on vascular flows in pregnancies complicated by intrauterine growth restriction. Reprod. Toxicol. 2014, 50, 27–35. [Google Scholar] [CrossRef] [PubMed]
- Zdravkovic, T.; Genbacev, O.; McMaster, M.T.; Fisher, S.J. The adverse effects of maternal smoking on the human placenta: A review. Placenta 2005, 26A, 81–90. [Google Scholar] [CrossRef] [PubMed]
- Node, K.; Kitakaze, M.; Yashikawa, H.; Kosaka, H.; Hori, M. Reversible reduction in plasma concentration of nitric oxide induced by cigarette smoking in young adults. Am. J. Cardiol. 1997, 79, 1538–1541. [Google Scholar] [CrossRef]
- Stępnik, M. Molecular aspects of toxic effects of nitric oxide. Med. Pr. 2001, 52, 375–381. [Google Scholar]
- Shi, Z.; Chen, Y.; Pei, Y.; Liu, C.; Cao, J.; Chen, P. The role of cyclooxygenase-2 in the protection against apoptosis in vascular endothelial cells induced by cigarette smoking. J. Thorac. Dis. 2017, 9, 30. [Google Scholar] [CrossRef]
- Loke, W.M.; Sing, K.L.; Lee, C.Y.; Chong, W.L.; Chew, S.E.; Huang, H.; Looi, W.F.; Quek, A.M.; Lim, E.C.; Seet, R.C. Cyclooxygenase-1 mediated platelet reactivity in young male smokers. Clin. Appl. Thromb. Hemost. 2014, 20, 371–377. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Cremades, D.; Bueno-Betí, C.; García-Giménez, J.L.; Ibañez-Cabellos, J.S.; Hermenegildo, C.; Pallardó, F.V.; Novella, S. Extracellular histones disarrange vasoactive mediators release through a COX-NOS interaction in human endothelial cells. J. Cell. Mol. Med. 2017, 21, 1584–1592. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Attard, R.; Dingli, P.; Doggen, C.J.M.; Cassar, K.; Farrugia, R.; Wettinger, S.B. The impact of passive and active smoking on inflammation, lipid profile and the risk of myocardial infarction. Open Heart 2017, 4, e000620. [Google Scholar] [CrossRef] [PubMed]
- Laskowska, M.; Laskowska, K.; Oleszczuk, J. Maternal serum levels of endothelial nitric oxide synthase and ADMA, endogenous eNOS inhibitor in pregnancies complicated by severe preeclampsia. Pregnancy Hypertens. 2012, 2, 312. [Google Scholar] [CrossRef] [PubMed]
- Ulm, M.R.; Plockinger, B.; Pirich, C.; Gryglewski, R.J.; Sinzinger, H.F. Umbilical arteries of babies born to cigarette smokers generate less prostacyclin and contain less arginine and citruline compared with those of babies born to control subjects. Am. J. Obstet. Gynecol. 1995, 172, 1485–1487. [Google Scholar] [CrossRef]
- Dobrzycka, B.; Kinalski, M.; Piechocka, D.; Terlikowski, S.J. The role of estrogens in angiogenesis in the female reproductive system. Endokrynol. Pol. 2009, 60, 210–214. [Google Scholar] [PubMed]
- Szkup, M.; Jurczak, A.; Karakiewicz, B.; Kotwas, A.; Kopeć, J.; Grochans, E. Influence of cigarette smoking on hormone and lipid metabolism in women in late reproductive stage. Clin. Interv. Aging 2018, 13, 109. [Google Scholar] [CrossRef]
- Marom-Haham, L.; Shulman, A. Cigarette smoking and hormones. Curr. Opin. Obstet. Gynecol. 2016, 28, 230–235. [Google Scholar] [CrossRef]
- Novella, S.; Laguna-Fernández, A.; Lázaro-Franco, M.; Sobrino, A.; Bueno-Betí, C.; Tarín, J.J.; Monsalve, E.; Sanchís, J.; Hermenegildo, C. Estradiol, acting through estrogen receptor alpha, restores dimethylarginine dimethylaminohydrolase activity and nitric oxide production in oxLDL-treated human arterial endothelial cells. Mol. Cell. Endocrinol. 2013, 365, 11–16. [Google Scholar] [CrossRef] [Green Version]
- Vidal-Gómez, X.; Novella, S.; Pérez-Monzó, I.; Garabito, M.; Dantas, A.P.; Segarra, G.; Hermenegildo, C.; Medina, P. Decreased bioavailability of nitric oxide in aorta from ovariectomized senescent mice. Role of cyclooxygenase. Exp. Gerontol. 2016, 76, 1–8. [Google Scholar] [CrossRef]
- Chalon, S.; Moreno, H.; Benowitz, N.L.; Hoffmann, B.B.; Blaschke, T.F. Nicotine impairs endothelium-dependent dilatation in human veins in vivo. Clin. Pharmacol. Ther. 2000, 67, 391–397. [Google Scholar] [CrossRef] [PubMed]
- Ostergaard, L.; Stankevicius, E.; Andersen, M.R.; Eskildsen-Helmond, Y.; Ledet, T.; Mulvany, M.J.; Simonsen, U. Diminished NO release in chronic hypoxic endothelial cells. Am. J. Physiol. Heart Circ. Physiol. 2007, 293, H2894–H2903. [Google Scholar] [CrossRef] [PubMed]
- Tsuchiya, M.; Asada, A.; Kasahara, E.; Sato, E.F.; Shindo, M.; Inoue, M. Smoking a single cigarette rapidly reduces combined concentrations of nitrate and nitrite and concentrations of antioxidants in plasma. Circulation 2002, 105, 1155–1157. [Google Scholar] [CrossRef] [PubMed]
- Chahal, N.; McLain, A.C.; Ghassabian, A.; Michels, K.A.; Bell, E.M.; Lawrence, D.A.; Yeung, E.H. Maternal smoking and newborn cytokine and immunoglobulin levels. Nicotine Tob. Res. 2017, 19, 789–796. [Google Scholar] [CrossRef]
- Billert, H. Tobacco use disorder and nitric oxide metabolism—Pathomechanisms of the perioperative cardiovascular and respiratory complications in the perioperative period. Prz. Lek. 2011, 68, 1017–1020. [Google Scholar]
- Nene, S.; Gelabert, H.; Moore, W.; Quinones-Baldrich, W.; Santibanez-Gallerani, A.; Ignarro, L. Cigarette smoking increases endothelial-derived vasorelaxation in the rat carotid artery in a dose-dependent manner. J. Surg. Res. 1997, 71, 101–106. [Google Scholar] [CrossRef] [PubMed]
- Chambers, D.C.; Tunnicliffe, W.S.; Ayres, J.G. Acute inhalation of cigarette smoke increases lower respiratory tract nitric oxide concentrations. Thorax 1998, 53, 677–679. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghasemi, A.; Zahedi Asl, S.; Mehrabi, Y.; Saadat, N.; Azizi, F. Serum nitric oxide metabolite levels in a general healthy population: Relation to sex and age. Life Sci. 2008, 83, 326–331. [Google Scholar] [CrossRef]
- Marshall, T. What is a case-control study? Int. J. Epidemiol. 2004, 33, 612–613. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Newborn | References |
|---|---|
| Low birth weight | [6] |
| Stillbirth | [7,8] |
| Congenital malformation | [9] |
| Increased risk of sudden infant death syndrome (SIDS) | [10] |
| Behavior disorders | [11] |
| Neurodevelopmental disorders | [12] |
| Increased risk of overweight and obesity | [13] |
| Increased risk of respiratory allergy | [14] |
| Higher blood pressure | [15] |
| Increased risk of gestational diabetes | [16] |
| Pregnant women | |
| Preterm premature rupture of membranes | [17] |
| Placenta previa | [18] |
| Ectopic pregnancy | [19] |
| Spontaneous miscarriage | [20] |
| Preterm birth | [21,22] |
| Fetal growth restriction | [23] |
| Fetal size | [24] |
| Biochemical Parameter | Smoking | Non-Smoking | p Value |
|---|---|---|---|
| NO (µmol/L) a | 68.8 ± 15.4 | 92.1 ± 16.9 | ≤0.001 |
| eNOS (pg/mL) a | 60.4 ± 21.6 | 76.9 ± 25.5 | 0.003 |
| iNOS (pg/mL) a | 101.5 ± 21.0 | 92.3 ± 19.3 | 0.020 |
| TAC (mmol/L) a | 1.265 ± 0.441 | 1.877 ± 0.483 | ≤0.001 |
| TOC (mmol/L) a | 0.417 ± 0.210 | 0.267 ± 0.157 | ≤0.001 |
| OSI b | 42.3 (14.8–61.8) | 13.6 (7.2–20.1) | ≤0.001 |
| Biochemical Parameter | B | 95%CI | β | p-Value | R2 |
|---|---|---|---|---|---|
| All women | |||||
| eNOS | 0.431 | 0.297/0.565 | 0.543 | ≤0.001 | 0.295 |
| iNOS | −0.244 | −0.434/−0.053 | −0.249 | 0.013 | 0.062 |
| Smokers | |||||
| eNOS | 0.353 | 0.155/0.552 | 0.494 | 0.001 | 0.244 |
| iNOS | −0.152 | −0.382/0.078 | −0.207 | 0.189 | 0.043 |
| Non-smokers | |||||
| eNOS | 0.294 | 0.133/0.456 | 0.441 | 0.001 | 0.195 |
| iNOS | −0.099 | −0.335/0.138 | −0.112 | 0.407 | 0.013 |
| Smoking | Non-Smoking | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| NO | eNOS | iNOS | NO | eNOS | iNOS | |||||||
| β | p-Value | β | p-Value | β | p-Value | β | p-Value | β | p-Value | β | p-Value | |
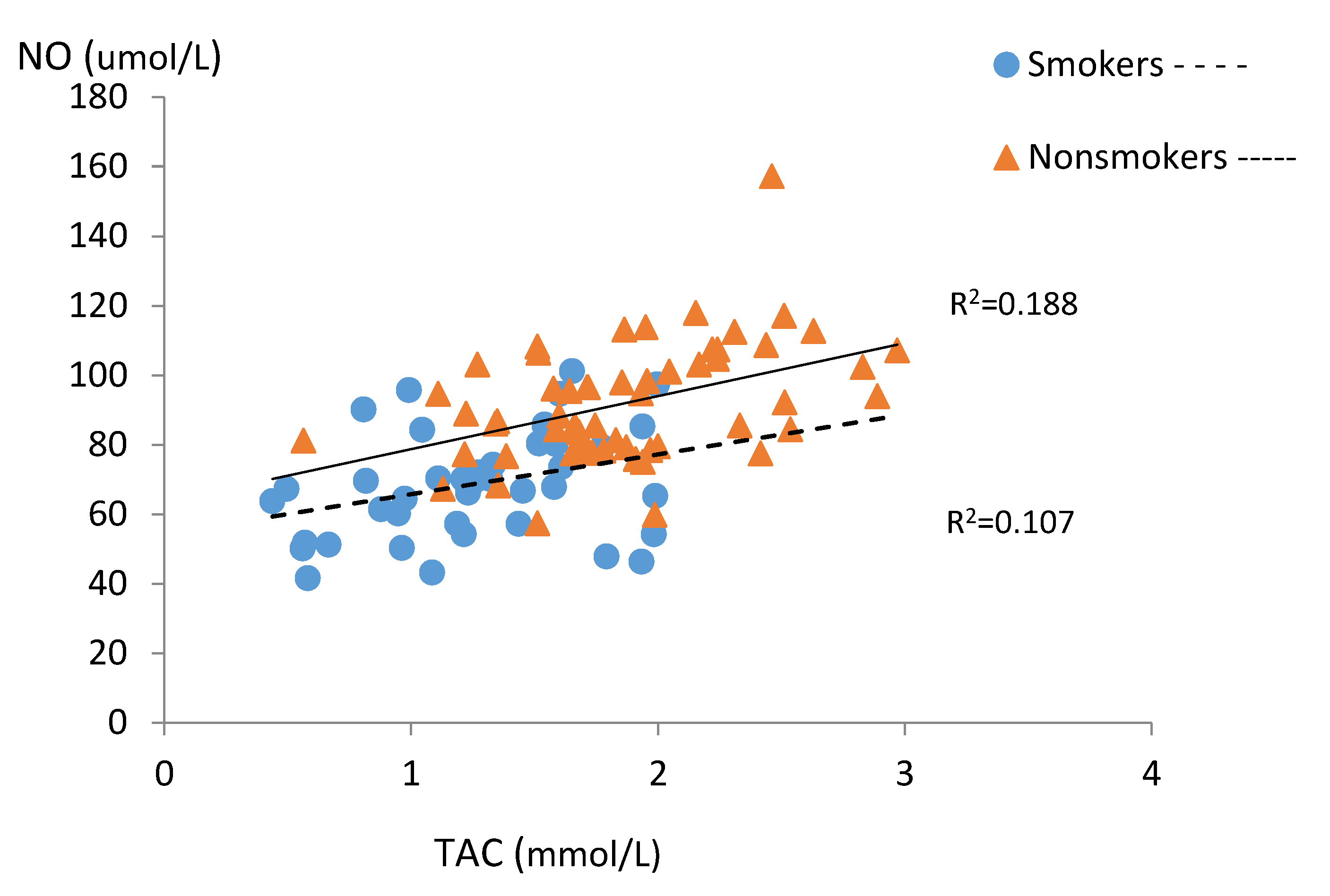
| TAC | 0.327 | 0.033 | 0.056 | 0.994 | −0.197 | 0.211 | 0.435 | 0.001 | 0.361 | 0.006 | 0.055 | 0.684 |
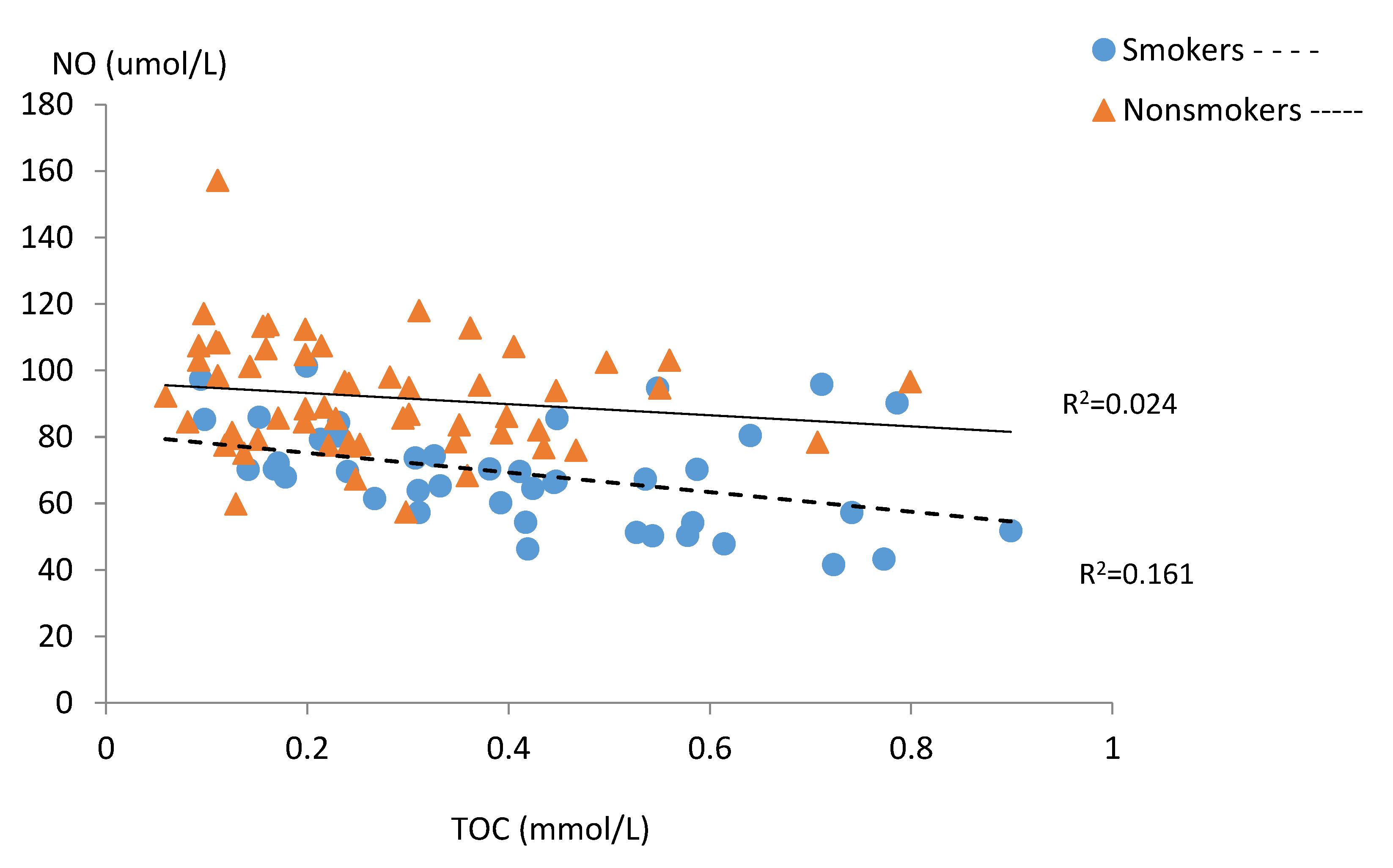
| TOC | −0.401 | 0.008 | −0.395 | 0.010 | 0.472 | 0.002 | −0.155 | 0.250 | −0.190 | 0.158 | 0.239 | 0.074 |
| OSI | −0.301 | 0.053 | −0.237 | 0.131 | 0.410 | 0.007 | −0.243 | 0.069 | −0.210 | 0.117 | 0.119 | 0.377 |
| Biochemical Parameter | B | 95%CI | β | p-Value |
|---|---|---|---|---|
| All women eNOS | 0.268 | 0.141/0.395 | 0.338 | ≤0.001 |
| iNOS | −0.075 | −0.228/0.079 | −0.076 | 0.338 |
| TAC | 6.421 | −0.400/13.242 | 0.178 | 0.065 |
| TOC | −5.359 | −23.922/13.204 | −0.052 | 0.568 |
| Smoking status (no = 1, yes = 0) | −12.299 | −19.340/−5.257 | −0.306 | 0.001 |
| R2 (%) | 54.1 | |||
| Smokers | ||||
| eNOS | 0.275 | 0.045/0.505 | 0.383 | 0.021 |
| iNOS | −0.076 | −0.313/0.161 | −0.103 | 0.519 |
| TAC | 3.006 | −8.338/14.350 | 0.086 | 0.593 |
| TOC | −3.746 | −33.082/25.590 | −0.051 | 0.797 |
| Cotynine | −0.152 | −0.295/−0.009 | −0.323 | 0.037 |
| R2 (%) | 45.2 | |||
| Non-smokers | ||||
| eNOS | 0.194 | 0.020/0.368 | 0.291 | 0.030 |
| iNOS | −0.100 | −0.323/0.123 | −0.113 | 0.373 |
| TAC | 12.282 | 2.506/22.057 | 0.350 | 0.015 |
| TOC | 5.434 | −23.474/34.342 | −0.164 | 0.417 |
| R2 (%) | 32.7 | |||
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chełchowska, M.; Ambroszkiewicz, J.; Gajewska, J.; Mazur, J.; Lewandowski, L.; Reśko-Zachara, M.; Maciejewski, T.M. Influence of Active Exposure to Tobacco Smoke on Nitric Oxide Status of Pregnant Women. Int. J. Environ. Res. Public Health 2018, 15, 2719. https://doi.org/10.3390/ijerph15122719
Chełchowska M, Ambroszkiewicz J, Gajewska J, Mazur J, Lewandowski L, Reśko-Zachara M, Maciejewski TM. Influence of Active Exposure to Tobacco Smoke on Nitric Oxide Status of Pregnant Women. International Journal of Environmental Research and Public Health. 2018; 15(12):2719. https://doi.org/10.3390/ijerph15122719
Chicago/Turabian StyleChełchowska, Magdalena, Jadwiga Ambroszkiewicz, Joanna Gajewska, Joanna Mazur, Leszek Lewandowski, Marzanna Reśko-Zachara, and Tomasz M. Maciejewski. 2018. "Influence of Active Exposure to Tobacco Smoke on Nitric Oxide Status of Pregnant Women" International Journal of Environmental Research and Public Health 15, no. 12: 2719. https://doi.org/10.3390/ijerph15122719