I Can Stand Learning: A Controlled Pilot Intervention Study on the Effects of Increased Standing Time on Cognitive Function in Primary School Children


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Instruments and Procedure
2.2.1. Standing Desk and Floor Mat
2.2.2. Objective Measurement of Activity
2.2.3. Subjective Measurement of Activity: Self-Reporting
Subjective Measurement of Activity: External Observation
2.2.4. Digit Span Task
2.2.5. Eriksen Flanker Task
2.2.6. Body Composition
2.3. Data Analysis
3. Results
3.1. Objectively Measured Sitting, Standing, and Walking Time during Lessons and Breaks
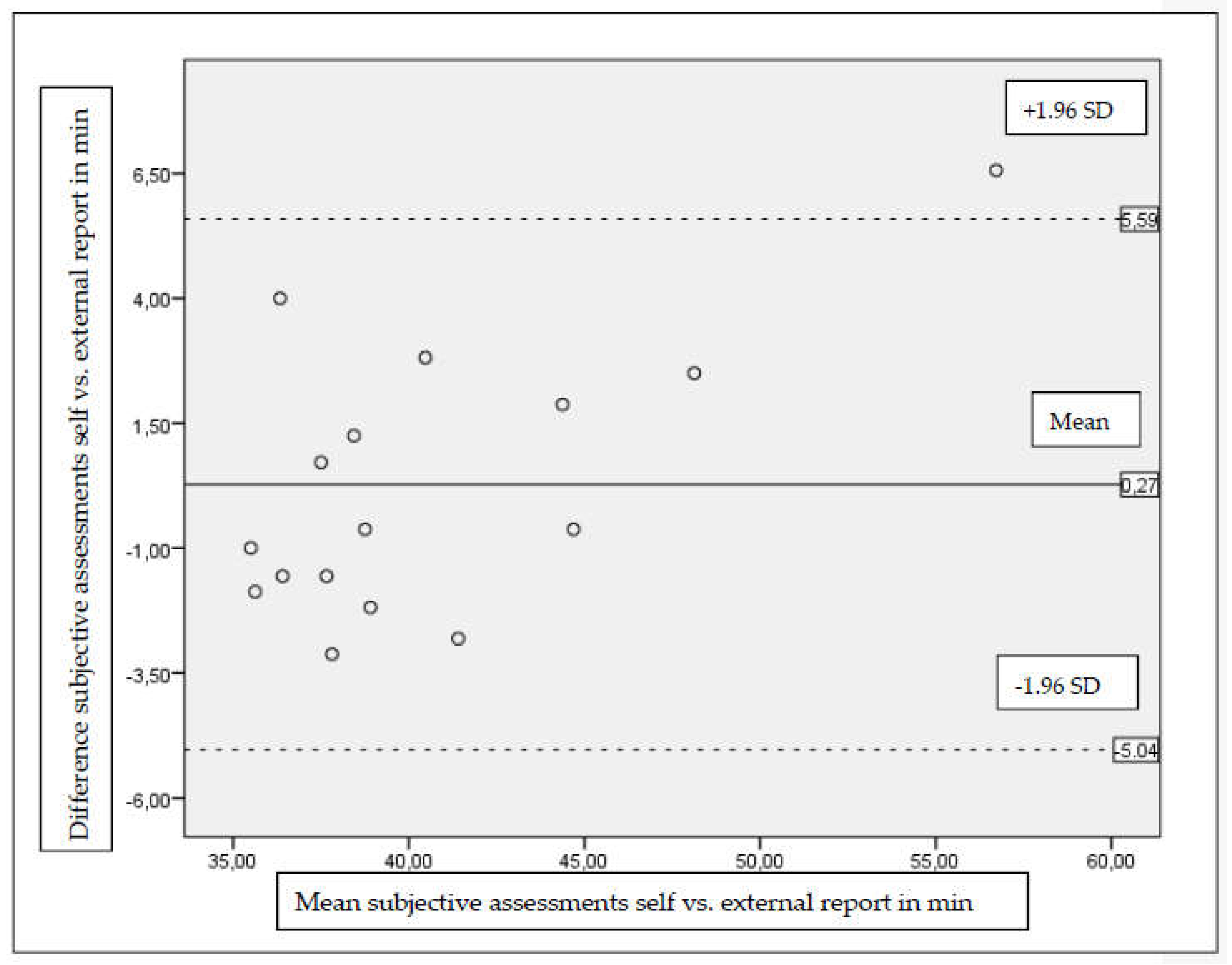
3.2. Association between Self-Reported Desk Standing Time
3.3. Digit Span Task
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Weiler, R.; Stamatakis, E.; Blair, S.N. Physical inactivity is associated with earlier mortality-the evidence is incontrovertible. Br. J. Gen. Pract. 2011, 61, 719–720. [Google Scholar] [CrossRef] [PubMed]
- Blair, S.N. Physical inactivity: The biggest public health problem of the 21st century. Br. J. Sports Med. 2009, 43, 1–2. [Google Scholar] [PubMed]
- World Health Organization (WHO). Global Recommendations on Physical Activity for Health; WHO: Geneva, Switzerland, 2010. [Google Scholar]
- Pate, R.R.; O’Neill, J.R.; Brown, W.H.; McIver, K.L.; Howie, E.K.; Dowda, M. Top 10 research questions related to physical activity in preschool children. Res. Q. Exerc. Sport 2013, 84, 448–455. [Google Scholar] [CrossRef] [PubMed]
- Tucker, P. The physical activity levels of preschool-aged children: A systematic review. Early Child. Res. Q. 2008, 23, 547–558. [Google Scholar] [CrossRef]
- Riddoch, C.; Edwards, D.; Page, A.; Froberg, K.; Anderssen, S.; Wedderkopp, N.; Brage, S.; Cooper, A.; Sardinha, L.; Harro, M.; et al. The European Youth Heart Study—Cardiovascular Disease Risk Factors in Children: Rationale, Aims, Study Design, and Validation of Methods. J. Phys. Act. Health 2005, 2, 115–129. [Google Scholar] [CrossRef]
- Hallal, P.C.; Martins, R.C.; Ramirez, A. The Lancet Physical Activity Observatory: Promoting physical activity worldwide. Lancet 2014, 384, 471–472. [Google Scholar] [CrossRef]
- Bernstein, M.S.; Morabia, A.; Sloutskis, D. Definition and prevalence of sedentarism in an urban population. Am. J. Public Health 1999, 89, 862–867. [Google Scholar] [CrossRef] [PubMed]
- Chau, J.Y.; Grunseit, A.C.; Chey, T.; Stamatakis, E.; Brown, W.J.; Matthews, C.E.; Bauman, A.E.; van der Ploeg, H.P. Daily sitting time and all-cause mortality: A meta-analysis. PLoS ONE 2013, 8, e80000. [Google Scholar] [CrossRef] [PubMed]
- Van Uffelen, J.G.; Wong, J.; Chau, J.Y.; van der Ploeg, H.P.; Riphagen, I.; Gilson, N.D.; Burton, N.W.; Healy, G.N.; Thorp, A.A.; Clark, B.K.; et al. Occupational sitting and health risks: A systematic review. Am. J. Prev. Med. 2010, 39, 379–388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rey-Lopez, J.P.; Vicente-Rodriguez, G.; Biosca, M.; Moreno, L.A. Sedentary behaviour and obesity development in children and adolescents. Nutr. Metab. Cardiovasc. Dis. 2008, 18, 242–251. [Google Scholar] [CrossRef] [PubMed]
- Tremblay, M.S.; LeBlanc, A.G.; Kho, M.E.; Saunders, T.J.; Larouche, R.; Colley, R.C.; Goldfield, G.; Connor Gorber, S. Systematic review of sedentary behaviour and health indicators in school-aged children and youth. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 98. [Google Scholar] [CrossRef] [PubMed]
- Ridgers, N.D.; Salmon, J.; Ridley, K.; O’Connell, E.; Arundell, L.; Timperio, A. Agreement between activPAL and ActiGraph for assessing children’s sedentary time. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 15. [Google Scholar] [CrossRef] [PubMed]
- Abbott, R.A.; Straker, L.M.; Mathiassen, S.E. Patterning of children’s sedentary time at and away from school. Obesity (Silver Spring) 2013, 21, E131–E133. [Google Scholar] [CrossRef] [PubMed]
- Hinckson, E.A.; Aminian, S.; Ikeda, E.; Stewart, T.; Oliver, M.; Duncan, S.; Schofield, G. Acceptability of standing workstations in elementary schools: A pilot study. Prev. Med. 2013, 56, 82–85. [Google Scholar] [CrossRef] [PubMed]
- Clemes, S.A.; Barber, S.E.; Bingham, D.D.; Ridgers, N.D.; Fletcher, E.; Pearson, N.; Salmon, J.; Dunstan, D.W. Reducing children’s classroom sitting time using sit-to-stand desks: Findings from pilot studies in UK and Australian primary schools. J. Public Health 2015, 38, 526–533. [Google Scholar] [CrossRef] [PubMed]
- Salmon, J.; Arundell, L.; Hume, C.; Brown, H.; Hesketh, K.; Dunstan, D.W.; Daly, R.M.; Pearson, N.; Cerin, E.; Moodie, M. A cluster-randomized controlled trial to reduce sedentary behavior and promote physical activity and health of 8–9 year olds: The Transform-Us! study. BMC Public Health 2011, 11, 759. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lanningham-Foster, L.; Foster, R.C.; McCrady, S.K.; Manohar, C.U.; Jensen, T.B.; Mitre, N.G.; Hill, J.O.; Levine, J.A. Changing the school environment to increase physical activity in children. Obesity (Silver Spring) 2008, 16, 1849–1853. [Google Scholar] [CrossRef] [PubMed]
- Benden, M.E.; Zhao, H.; Jeffrey, C.E.; Wendel, M.L.; Blake, J.J. The evaluation of the impact of a stand-biased desk on energy expenditure and physical activity for elementary school students. Int. J. Environ. Res. Public Health 2014, 11, 9361–9375. [Google Scholar] [CrossRef] [PubMed]
- Benden, M.E.; Blake, J.J.; Wendel, M.L.; Huber, J.C. The impact of stand-biased desks in classrooms on calorie expenditure in children. Am. J. Public Health. 2011, 101, 1433–1436. [Google Scholar] [CrossRef] [PubMed]
- Torbeyns, T.; Bailey, S.; Bos, I.; Meeusen, R. Active workstations to fight sedentary behaviour. Sports Med. 2014, 44, 1261–1273. [Google Scholar] [CrossRef] [PubMed]
- Mura, G.; Vellante, M.; Nardi, A.E.; Machado, S.; Carta, M.G. Effects of School-Based Physical Activity Interventions on Cognition and Academic Achievement: A Systematic Review. CNS Neurol. Disord. Drug Target. 2015, 14, 1194–1208. [Google Scholar] [CrossRef]
- Skotte, J.; Korshoj, M.; Kristiansen, J.; Hanisch, C.; Holtermann, A. Detection of physical activity types using triaxial accelerometers. J. Phys. Act. Health 2014, 11, 76–84. [Google Scholar] [CrossRef] [PubMed]
- Steeves, J.A.; Bowles, H.R.; McClain, J.J.; Dodd, K.W.; Brychta, R.J.; Wang, J.; Chen, K.Y. Ability of thigh-worn ActiGraph and activPAL monitors to classify posture and motion. Med. Sci. Sports Exerc. 2015, 47, 952–959. [Google Scholar] [CrossRef] [PubMed]
- Choi, L.; Liu, Z.; Matthews, C.E.; Buchowski, M.S. Validation of accelerometer wear and nonwear time classification algorithm. Med. Sci. Sports Exerc. 2011, 43, 357–364. [Google Scholar] [CrossRef] [PubMed]
- Alloway, T.P.; Gathercole, S.E.; Kirkwood, H.; Elliott, J. Evaluating the validity of the Automated Working Memory Assessment. Educ. Psychol. 2008, 28, 725–734. [Google Scholar] [CrossRef]
- Eriksen, B.A.; Eriksen, C.W. Effects of noise letters upon the identification of a target letter in a nonsearch task. Percept. Psychophys. 1974, 16, 143–149. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Erlbaum: Hillsdale, Australia, 1988. [Google Scholar]
- Fleiss, J.L. The Design and Analysis of Clinical Experiments; Wiley: New York, NY, USA, 1986. [Google Scholar]
- Ridgers, N.D.; Timperio, A.; Crawford, D.; Salmon, J. Five-year changes in school recess and lunchtime and the contribution to children’s daily physical activity. Br. J. Sports Med. 2012, 46, 741–746. [Google Scholar] [CrossRef] [PubMed]
- Nettlefold, L.; McKay, H.A.; Warburton, D.E.; McGuire, K.A.; Bredin, S.S.; Naylor, P.J. The challenge of low physical activity during the school day: At recess, lunch and in physical education. Br. J. Sports Med. 2011, 45, 813–819. [Google Scholar] [CrossRef] [PubMed]
- Minges, K.E.; Chao, A.M.; Irwin, M.L.; Owen, N.; Park, C.; Whittemore, R.; Salmon, J. Classroom Standing Desks and Sedentary Behavior: A Systematic Review. Pediatrics 2016, 137, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Donath, L.; Faude, O.; Schefer, Y.; Roth, R.; Zahner, L. Repetitive daily point of choice prompts and occupational sit-stand transfers, concentration and neuromuscular performance in office workers: An RCT. Int. J. Environ. Res. Public Health 2015, 12, 4340–4353. [Google Scholar] [CrossRef] [PubMed]
- Lang, J.J.; McNeil, J.; Tremblay, M.S.; Saunders, T.J. Sit less, stand more: A randomized point-of-decision prompt intervention to reduce sedentary time. Prev. Med. 2015, 73, 67–69. [Google Scholar] [CrossRef] [PubMed]
- Swartz, A.M.; Rote, A.E.; Welch, W.A.; Maeda, H.; Hart, T.L.; Ik Cho, Y.; Strath, S.J. Prompts to disrupt sitting time and increase physical activity at work, 2011–2012. Prev. Chronic. Dis. 2014, 11, E73. [Google Scholar] [CrossRef] [PubMed]
- De Ruiter, W.K.; Cairney, J.; Leatherdale, S.T.; Faulkner, G.E. A longitudinal examination of the interrelationship of multiple health behaviors. Am. J. Prev. Med. 2014, 47, 283–289. [Google Scholar] [CrossRef] [PubMed]
- Jeffrey, B.A.; Hannan, M.T.; Quinn, E.K.; Zimmerman, S.; Barton, B.A.; Rubin, C.T.; Kiel, D.P. Self-reported adherence with the use of a device in a clinical trial as validated by electronic monitors: The VIBES study. BMC Med. Res. Methodol. 2012, 12, 171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prince, S.A.; Adamo, K.B.; Hamel, M.E.; Hardt, J.; Connor, G.S.; Tremblay, M. A comparison of direct versus self-report measures for assessing physical activity in adults: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2008, 5, 56. [Google Scholar] [CrossRef] [PubMed]
- Fransson, E.; Knutsson, A.; Westerholm, P.; Alfredsson, L. Indications of recall bias found in a retrospective study of physical activity and myocardial infarction. J. Clin. Epidemiol. 2008, 61, 840–847. [Google Scholar] [CrossRef] [PubMed]
- Adams, S.A.; Matthews, C.E.; Ebbeling, C.B.; Moore, C.G.; Cunningham, J.E.; Fulton, J.; Hebert, J.R. The effect of social desirability and social approval on self-reports of physical activity. Am. J. Epidemiol. 2005, 161, 389–398. [Google Scholar] [CrossRef] [PubMed]
- Ainsworth, B.E.; Caspersen, C.J.; Matthews, C.E.; Masse, L.C.; Baranowski, T.; Zhu, W. Recommendations to improve the accuracy of estimates of physical activity derived from self report. J. Phys. Act. Health 2012, 9, S76–S84. [Google Scholar] [CrossRef] [PubMed]
- Mehta, R.K.; Shortz, A.E.; Benden, M.E. Standing Up for Learning: A Pilot Investigation on the Neurocognitive Benefits of Stand-Biased School Desks. Int. J. Environ. Res. Public Health 2016, 13, 59. [Google Scholar] [CrossRef] [PubMed]
- Koepp, G.A.; Manohar, C.U.; McCrady-Spitzer, S.K.; Ben-Ner, A.; Hamann, D.J.; Runge, C.F.; Levine, J.A. Treadmill desks: A 1-year prospective trial. Obesity (Silver Spring) 2013, 21, 705–711. [Google Scholar] [CrossRef] [PubMed]
- Ridgers, N.D.; Timperio, A.; Crawford, D.; Salmon, J. What factors are associated with adolescents’ school break time physical activity and sedentary time? PLoS ONE 2013, 8, e56838. [Google Scholar] [CrossRef] [PubMed]
- Wick, K.; Faude, O.; Schwager, S.; Zahner, L.; Donath, L. Deviation between self-reported and measured occupational physical activity levels in office employees: Effects of age and body composition. Int. Arch. Occup. Environ. Health 2016, 89, 575–582. [Google Scholar] [CrossRef] [PubMed]
- Kurth, B.M.; Ellert, U. Estimated and measured BMI and self-perceived body image of adolescents in Germany: Part 1—general implications for correcting prevalence estimations of overweight and obesity. Obes. Facts 2010, 3, 181–190. [Google Scholar] [CrossRef] [PubMed]
- Peterson, N.E.; Sirard, J.R.; Kulbok, P.A.; DeBoer, M.D.; Erickson, J.M. Validation of Accelerometer Thresholds and Inclinometry for Measurement of Sedentary Behavior in Young Adult University Students. Res. Nurs. Health 2015, 38, 492–499. [Google Scholar] [CrossRef] [PubMed]
- Sellers, C.; Dall, P.; Grant, M.; Stansfield, B. Validity and reliability of the activPAL3 for measuring posture and stepping in adults and young people. Gait Posture 2016, 43, 42–47. [Google Scholar] [CrossRef] [PubMed]
- Owen, K.B.; Smith, J.; Lubans, D.R.; Ng, J.Y.; Lonsdale, C. Self-determined motivation and physical activity in children and adolescents: A systematic review and meta-analysis. Prev. Med. 2014, 67, 270–279. [Google Scholar] [CrossRef] [PubMed]
- Graf, C.; Beneke, R.; Bloch, W.; Bucksch, J.; Dordel, S.; Eiser, S.; Ferrari, N.; Koch, B.; Krug, S.; Lawrenz, W.; et al. Recommendations for promoting physical activity for children and adolescents in Germany. A consensus statement. Obes. Facts 2014, 7, 178–190. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Mean Scores (SD) | IG (n = 19) | CG (n = 19) |
|---|---|---|
| age, years | 10.8 (0.6) | 10.8 (0.8) |
| weight, kg | 39.3 (9.1) | 40.8 (12.1) |
| height, cm | 147.1 (7.8) | 147.2 (8.2) |
| body mass index, kg/m2 | 18.0 (2.8) | 18.6 (4.3) |
| sex, n (%) | ||
| male | 9 (47.4) | 13 (68.4) |
| female | 10 (52.6) | 6 (31.6) |
| Physical Activity | Group | Mean Time in % (SD) | Mean Time in Min (SD) | Mean Difference (95% CI) | t-Value (df) | p-Value | Effect Size d |
|---|---|---|---|---|---|---|---|
| Sitting time lesson | IG | 68.2 (5.7) | 172.1 (19.7) | 12.7 (1.6; 23.9) | 2.32 (36) | 0.03 * | 0.75 |
| CG | 73.7 (5.4) | 184.9 (13.7) | |||||
| Standing time lesson | IG | 23.9 (5.6) | 60.5 (15.1) | −13.4 (−22.3; −4.5) | −3.06 (36) | 0.004 ** | 0.99 |
| CG | 18.8 (4.7) | 47.1 (11.6) | |||||
| Walking time lesson | IG | 7.9 (2.5) | 19.9 (6.3) | −1.0 (−4.6; 2.6) | −0.57 (36) | 0.57 | 0.18 |
| CG | 7.5 (1.7) | 18.9 (4.4) | |||||
| Sitting time break | IG | 32.3 (10.7) | 7.5 (2.5) | −1.0 (−2.4; 0.4) | −1.48 (36) | 0.15 | 0.47 |
| CG | 34.3 (8.2) | 6.5 (1.6) | |||||
| Standing time break | IG | 37.3 (12.2) | 8.8 (3.1) | −2.5 (−4.0; −0.9) | −3.15 (36) | 0.003 ** | 1.04 |
| CG | 33.4 (7.6) | 6.3 (1.4) | |||||
| Walking time break | IG | 30.4 (13.8) | 7.0 (3.0) | −0.9 (−2.7; 0.8) | −1.05 (36) | 0.30 | 0.34 |
| CG | 32.3 (11.7) | 6.1 (2.2) |
| Cognitive Function | Group | Mean (SD) Pre | Mean (SD) Post | Mean Difference (95% CI) | Effect Size d | p-Value Time | p-Value Group | p-Value Time × Group |
|---|---|---|---|---|---|---|---|---|
| Forward digit span (Mean) | ||||||||
| Number of correct trials | IG | 4.8 (1.5) | 5.5 (1.4) | −0.7 (−1.6; 0.3) | 0.48 | 0.07 | 0.59 | 0.50 |
| CG | 4.8 (1.3) | 5.2 (1.7) | −0.3 (−1.0; 0.3) | 0.26 | ||||
| Maximum sequence length | IG | 4.8 (0.8) | 5.2 (0.7) | −0.4 (−0.9; 0.1) | 0.48 | 0.29 | 0.58 | 0.16 |
| CG | 5.0 (0.7) | 4.9 (0.7) | 0.1 (−0.3; 0.4) | 0.09 | ||||
| Backward digit span (Mean) | ||||||||
| Number of correct trials | IG | 5.0 (1.2) | 5.7 (1.8) | −0.7 (−1.4; 0.0) | 0.46 | 0.07 | 0.56 | 0.74 |
| CG | 4.8 (1.7) | 5.3 (1.9) | −0.5 (−1.6; 0.6) | 0.26 | ||||
| Maximum sequence length | IG | 4.1 (0.8) | 4.4 (1.0) | −0.4 (−0.8; 0.1) | 0.41 | 0.16 | 0.28 | 0.57 |
| CG | 3.9 (0.9) | 4.1 (1.0) | −0.2 (−0.8; 0.5) | 0.17 | ||||
| Eriksen flanker reaction time (ms) | ||||||||
| Congruous | IG | 476 (99) | 451 (119) | 25 (−18; 69) | 0.23 | 0.04 * | 0.92 | 0.95 |
| CG | 474 (89) | 447 (82) | 27 (−3; 57) | 0.32 | ||||
| Incongruous | IG | 546 (127) | 518 (120) | 28 (−27; 83) | 0.23 | 0.07 | 0.85 | 0.95 |
| CG | 541 (99) | 510 (88) | 30 (−7; 67) | 0.32 | ||||
| Eriksen flanker accuracy (%, range 0–1) | ||||||||
| Congruous | IG | 0.87 (0.17) | 0.92 (0.16) | −0.05 (−0.10; 0.01) | 0.29 | 0.01 * | 0.52 | 0.93 |
| CG | 0.90 (0.14) | 0.95 (0.06) | −0.05 (−0.09; 0.00) | 0.42 | ||||
| Incongruous | IG | 0.74 (0.15) | 0.79 (0.17) | −0.05 (−0.11; 0.00) | 0.32 | 0.06 | 0.82 | 0.75 |
| CG | 0.76 (0.19) | 0.80 (0.15) | −0.04 (−0.12; 0.04) | 0.22 | ||||
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wick, K.; Faude, O.; Manes, S.; Zahner, L.; Donath, L. I Can Stand Learning: A Controlled Pilot Intervention Study on the Effects of Increased Standing Time on Cognitive Function in Primary School Children. Int. J. Environ. Res. Public Health 2018, 15, 356. https://doi.org/10.3390/ijerph15020356
Wick K, Faude O, Manes S, Zahner L, Donath L. I Can Stand Learning: A Controlled Pilot Intervention Study on the Effects of Increased Standing Time on Cognitive Function in Primary School Children. International Journal of Environmental Research and Public Health. 2018; 15(2):356. https://doi.org/10.3390/ijerph15020356
Chicago/Turabian StyleWick, Katharina, Oliver Faude, Susanne Manes, Lukas Zahner, and Lars Donath. 2018. "I Can Stand Learning: A Controlled Pilot Intervention Study on the Effects of Increased Standing Time on Cognitive Function in Primary School Children" International Journal of Environmental Research and Public Health 15, no. 2: 356. https://doi.org/10.3390/ijerph15020356
APA StyleWick, K., Faude, O., Manes, S., Zahner, L., & Donath, L. (2018). I Can Stand Learning: A Controlled Pilot Intervention Study on the Effects of Increased Standing Time on Cognitive Function in Primary School Children. International Journal of Environmental Research and Public Health, 15(2), 356. https://doi.org/10.3390/ijerph15020356