Full Atrioventricular Block Secondary to Acute Poisoning Mercury: A Case Report


{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Background
2. Ethics, Approval and Consent to Participate
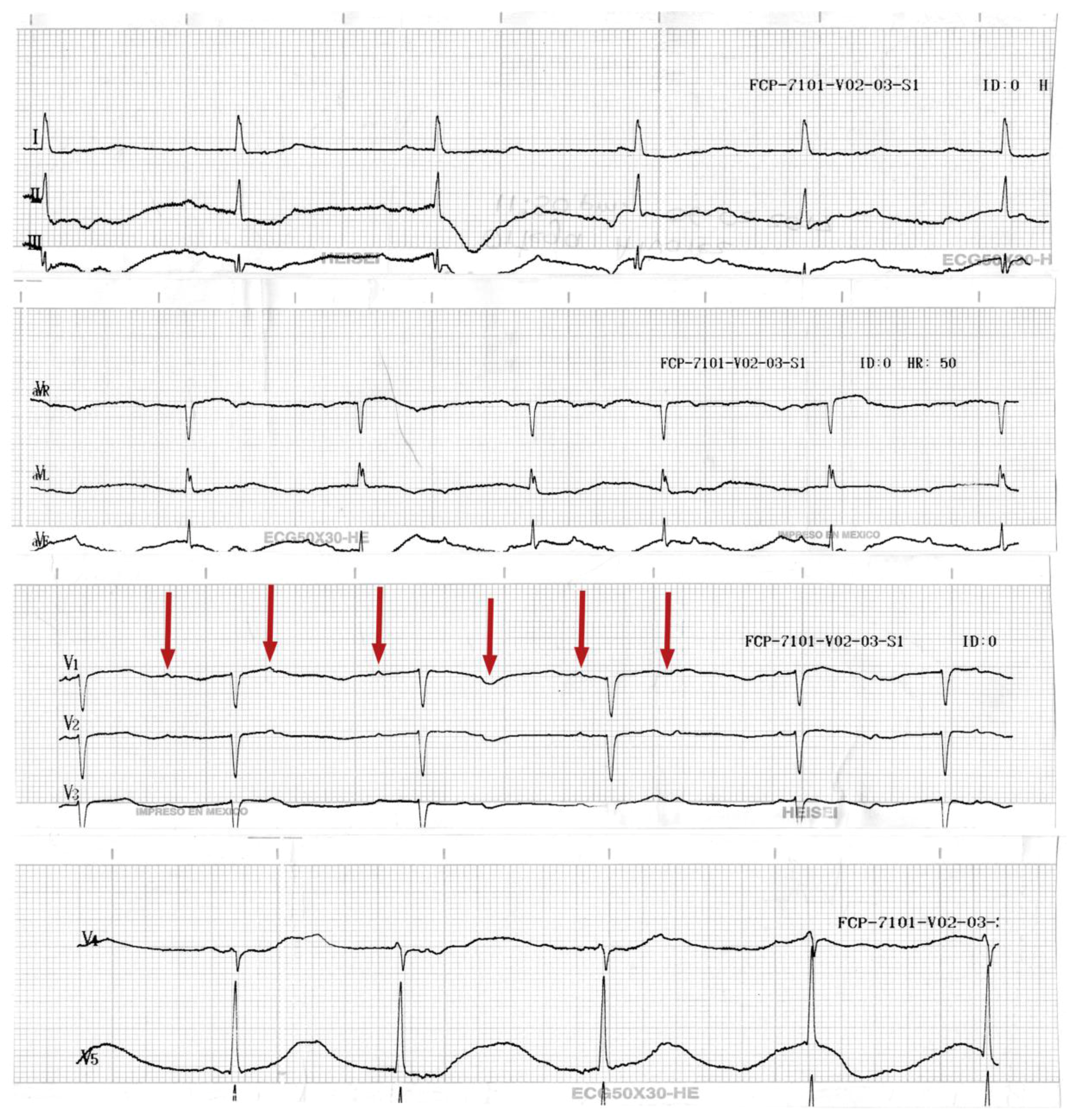
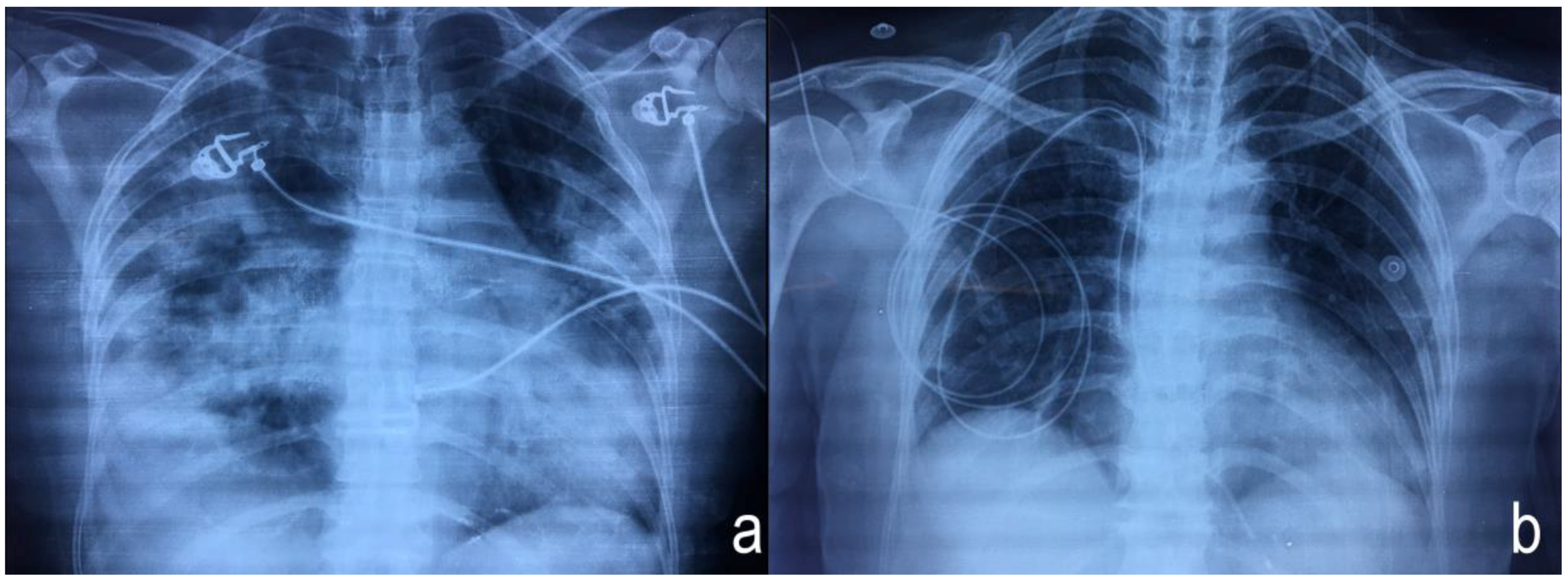
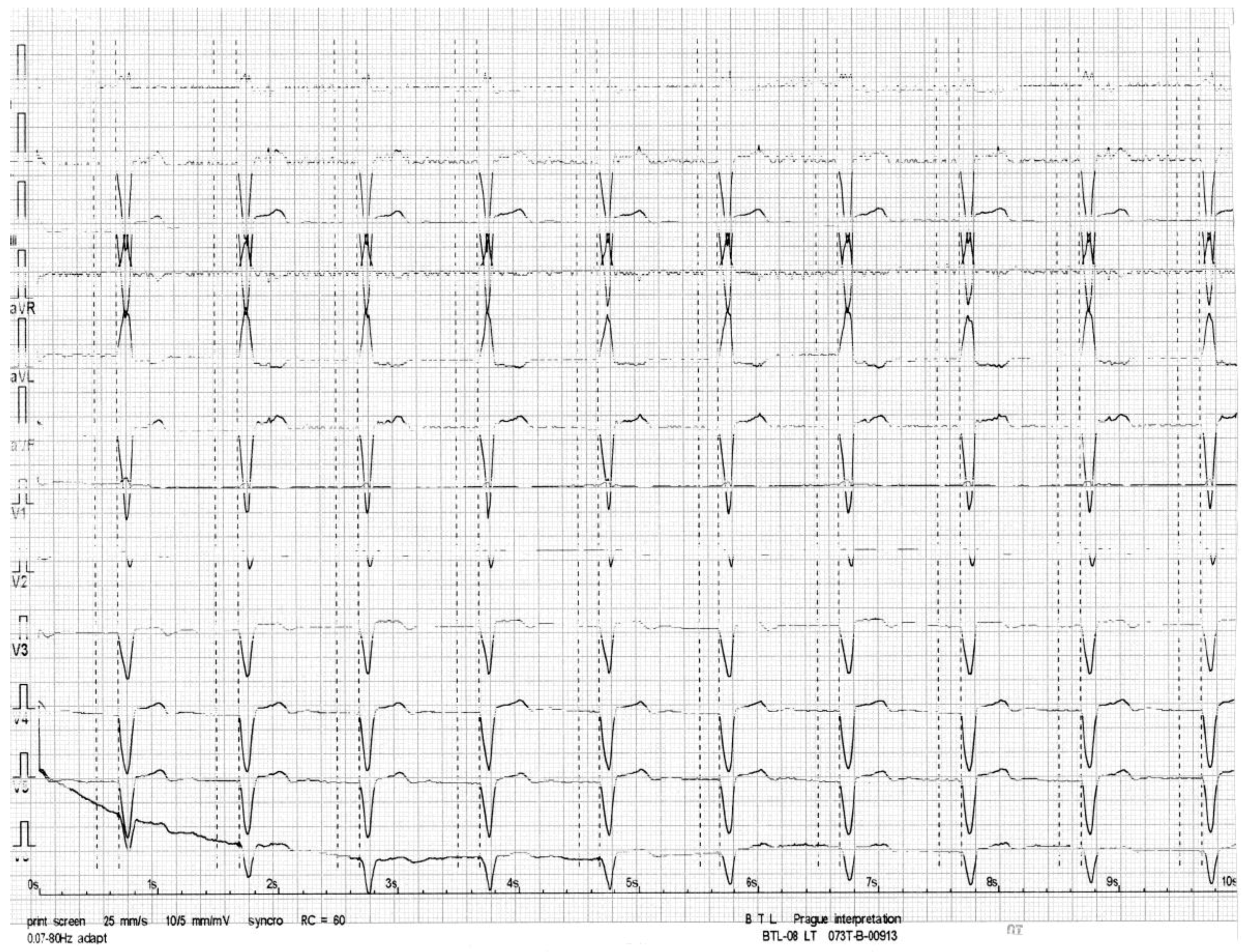
3. Case Presentation
4. Discussion and Literature Revision
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Bernhoft, R.A. Mercury toxicity and treatment: A review of the literature. J. Environ. Public Health 2012, 2012, 460508. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Exposure to Mercury: A Major Public Health Concern, Preventing Disease through Healthy Environment; World Health Organization: Geneva, Switzerland, 2008. [Google Scholar]
- United Nations Industrial Development Organization. Global Mercury Project: Global Impacts of Mercury Supply and Demand in Small-Scale Gold Mining; Report to the United Nations Environment Programme Governing Council, Nairobi, Kenya; United Nations Industrial Development Organization: Vienna, Austria, 2007. [Google Scholar]
- World Health Organization. Technical Paper #1: Environmental and Occupational Health Hazards Associated with Artisanal and Small-Scale Gold Mining; WHO Library Cataloguing-in-Publication Data: Geneva, Switzerland, 2016. [Google Scholar]
- Concise International Chemical Assessment. Elemental Mercury and Inorganic Mercury Compounds: Human Health Aspects; Risher, J.F., Ed.; WHO Library: Geneva, Switzerland, 2003. [Google Scholar]
- Clarkson, T.W.; Magos, L. The toxicology of mercury and its chemical compounds. Crit. Rev. Toxicol. 2006, 36, 609–662. [Google Scholar] [CrossRef] [PubMed]
- Jepson, W.; Richardson, M.; Rowlinson, J. The solubility of mercury in gases at moderate pressures. Trans. Faraday Soc. 1957, 53, 1586–1591. [Google Scholar] [CrossRef]
- Liu, J.; Shi, J.Z.; Yu, L.M.; Goyer, R.A.; Waalkes, M.P. Mercury in traditional medicines: Is cinnabar toxicologically similar to common mercurials? Exp. Biol. Med. 2008, 233, 810–817. [Google Scholar] [CrossRef] [PubMed]
- Genchi, G.; Sinicropi, M.S.; Carocci, A.; Lauria, G.; Catalano, A. Mercury exposure and heart diseases. Int. J. Environ. Res. Public Health 2017, 14, 74. [Google Scholar] [CrossRef] [PubMed]
- Wildemann, T.M.; Weber, L.P.; Siciliano, S.D. Combined exposure to lead, inorganic mercury and methylmercury shows deviation from additivity for cardiovascular toxicity in rats. J. Appl. Toxicol. 2015, 35, 918–926. [Google Scholar] [CrossRef] [PubMed]
- United States Environmental Protection Agency. America’s Children and the Environment (ACE); Biomonitoring: Mercury—Report Contents; United States Environmental Protection Agency: Washington, DC, USA, 2017.
- United Nations Environment. Minamata Convention on Mercury. Available online: http://www.mercuryconvention.org/Convention/tabid/3426/language/en-US/Default.aspx (accessed on 7 February 2018).
- International Labour Organization. Social and Labour Issues in Small-Scale Mines; Report Tmssm/1999; International Labour Organization: Geneva, Switzerland, 1999. [Google Scholar]
- Liang, C.; Li, Z.; Xia, X.; Wang, Q.; Tao, R.; Tao, Y.; Xiang, H.; Tong, S.; Tao, F. Determine multiple elements simultaneously in the sera of umbilical cord blood samples-a very simple method. Biol. Trace Elem. Res. 2017, 177, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Ferrero, M.E. Rationale for the successful management of edta chelation therapy in human burden by toxic metals. Biomed. Res. Int. 2016, 2016, 8274504. [Google Scholar] [CrossRef] [PubMed]
- Delafiori, J.; Ring, G.; Furey, A. Clinical applications of HPLC-ICP-MS element speciation: A review. Talanta 2016, 153, 306–331. [Google Scholar] [CrossRef] [PubMed]
- Dias, D.; Bessa, J.; Guimaraes, S.; Soares, M.E.; Bastos Mde, L.; Teixeira, H.M. Inorganic mercury intoxication: A case report. Forensic Sci. Int. 2016, 259, e20–e24. [Google Scholar] [CrossRef] [PubMed]
- Rafati-Rahimzadeh, M.; Kazemi, S.; Moghadamnia, A.A. Current approaches of the management of mercury poisoning: Need of the hour. Daru 2014, 22, 46. [Google Scholar] [CrossRef] [PubMed]
- Wiggers, G.A.; Furieri, L.B.; Briones, A.M.; Avendano, M.S.; Pecanha, F.M.; Vassallo, D.V.; Salaices, M.; Alonso, M.J. Cerebrovascular endothelial dysfunction induced by mercury exposure at low concentrations. Neurotoxicology 2016, 53, 282–289. [Google Scholar] [CrossRef] [PubMed]
- Karimi, R.; Vacchi-Suzzi, C.; Meliker, J.R. Mercury exposure and a shift toward oxidative stress in avid seafood consumers. Environ. Res. 2016, 146, 100–107. [Google Scholar] [CrossRef] [PubMed]
- Lim, K.M.; Kim, S.; Noh, J.Y.; Kim, K.; Jang, W.H.; Bae, O.N.; Chung, S.M.; Chung, J.H. Low-level mercury can enhance procoagulant activity of erythrocytes: A new contributing factor for mercury-related thrombotic disease. Environ. Health Perspect. 2010, 118, 928–935. [Google Scholar] [CrossRef] [PubMed]
- Frustaci, A.; Magnavita, N.; Chimenti, C.; Caldarulo, M.; Sabbioni, E.; Pietra, R.; Cellini, C.; Possati, G.F.; Maseri, A. Marked elevation of myocardial trace elements in idiopathic dilated cardiomyopathy compared with secondary cardiac dysfunction. J. Am. Coll. Cardiol. 1999, 33, 1578–1583. [Google Scholar] [CrossRef]
- Houston, M.C. Role of mercury toxicity in hypertension, cardiovascular disease, and stroke. J. Clin. Hypertens. 2011, 13, 621–627. [Google Scholar] [CrossRef] [PubMed]
- Solenkova, N.V.; Newman, J.D.; Berger, J.S.; Thurston, G.; Hochman, J.S.; Lamas, G.A. Metal pollutants and cardiovascular disease: Mechanisms and consequences of exposure. Am. Heart J. 2014, 168, 812–822. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Xu, C.; Fu, Z.; Shu, Y.; Zhang, J.; Lu, C.; Mo, X. Associations between total mercury and methyl mercury exposure and cardiovascular risk factors in us adolescents. Environ. Sci. Pollut. Res. Int. 2018, 25, 6265–6272. [Google Scholar] [CrossRef] [PubMed]
- Okin, P.M.; Devereux, R.B.; Howard, B.V.; Fabsitz, R.R.; Lee, E.T.; Welty, T.K. Assessment of QT interval and QT dispersion for prediction of all-cause and cardiovascular mortality in American Indians: The strong heart study. Circulation 2000, 101, 61–66. [Google Scholar] [CrossRef] [PubMed]
- Zulqarnain, M.A.; Qureshi, W.T.; O’Neal, W.T.; Shah, A.J.; Soliman, E.Z. Risk of mortality associated with QT and JT intervals at different levels of QRS duration (from the third national health and nutrition examination survey). Am. J. Cardiol. 2015, 116, 74–78. [Google Scholar] [CrossRef] [PubMed]
- Mozaffarian, D.; Shi, P.; Morris, J.S.; Spiegelman, D.; Grandjean, P.; Siscovick, D.S.; Willett, W.C.; Rimm, E.B. Mercury exposure and risk of cardiovascular disease in two U.S. Cohorts. N. Engl. J. Med. 2011, 364, 1116–1125. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, S.W. The role of chelation in the treatment of other metal poisonings. J. Med. Toxicol. 2013, 9, 355–369. [Google Scholar] [CrossRef] [PubMed]
- Sharma, B.; Singh, S.; Siddiqi, N.J. Biomedical implications of heavy metals induced imbalances in redox systems. Biomed. Res. Int. 2014, 2014, 640754. [Google Scholar] [CrossRef] [PubMed]
- Quan, H.; Ghali, W.A.; Verhoef, M.J.; Norris, C.M.; Galbraith, P.D.; Knudtson, M.L. Use of chelation therapy after coronary angiography. Am. J. Med. 2001, 111, 686–691. [Google Scholar] [CrossRef]
- Miller, K.L.; Liebowitz, R.S.; Newby, L.K. Complementary and alternative medicine in cardiovascular disease: A review of biologically based approaches. Am. Heart J. 2004, 147, 401–411. [Google Scholar] [CrossRef] [PubMed]
- Flora, S.J.; Pachauri, V. Chelation in metal intoxication. Int. J. Environ. Res. Public Health 2010, 7, 2745–2788. [Google Scholar] [CrossRef] [PubMed]



© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Peregrina-Chávez, A.G.; Ramírez-Galindo, M.D.R.; Chávez-Martínez, R.; Delahanty-Delgado, C.A.; Vazquez-Alaniz, F. Full Atrioventricular Block Secondary to Acute Poisoning Mercury: A Case Report. Int. J. Environ. Res. Public Health 2018, 15, 657. https://doi.org/10.3390/ijerph15040657
Peregrina-Chávez AG, Ramírez-Galindo MDR, Chávez-Martínez R, Delahanty-Delgado CA, Vazquez-Alaniz F. Full Atrioventricular Block Secondary to Acute Poisoning Mercury: A Case Report. International Journal of Environmental Research and Public Health. 2018; 15(4):657. https://doi.org/10.3390/ijerph15040657
Chicago/Turabian StylePeregrina-Chávez, Amelia Geraldine, María Del Rayo Ramírez-Galindo, Rolando Chávez-Martínez, Cesar Anuar Delahanty-Delgado, and Fernando Vazquez-Alaniz. 2018. "Full Atrioventricular Block Secondary to Acute Poisoning Mercury: A Case Report" International Journal of Environmental Research and Public Health 15, no. 4: 657. https://doi.org/10.3390/ijerph15040657