A Socio-Technical Exploration for Reducing & Mitigating the Risk of Retained Foreign Objects

Abstract
:1. Introduction
- Patients: Symptoms experienced by patients vary depending on the nature of the RFO (inert or not), the duration it has been left in situ and the location in which it has been left. Symptoms identified in a recent national, 10-year review of closed claims pertaining to RFO in maternity and gynaecology services (performed by [4] at the State Claims Agency) included pain (acute and chronic), foul smelling discharge, difficulty walking, vaginal bleeding and general malaise. Complications included weight gain, hirsutism, pelvic inflammatory disease, infertility and the need for further surgery. Medium- and long-term associations were identified and diagnosed by both patient and consultant physician respectively on over one-third of patients with RFO in gynaecology services in this review. Problems included depression (requiring psychotherapy and pharmacotherapy), mild adjustment disorder and anxiety regarding further surgery and return to work. RFOs and their sequelae often culminate in a loss of trust in the medical profession.
- Financial costs: There is a varied cost implication depending on location and the impact it has on the individual affected. In a study conducted by [5], the variance in cost of a RFO ranged from between $51 to $3,988,829 with an average cost for legal practice payments of $86,247 alone.
- Reputational damage at both the individual clinician level and at the institutional level. Stawicki et al. identifies that RFOs are in the main a result of team- or systems-based errors as opposed to an individual human error [6]. However, as a result of the ‘blame’ culture that exists within the healthcare industry this perception leads to a tendency of providers to attempt to conceal the error or shift blame away from them [7].
- Absence of policies and procedures
- Failure to comply with existing policies and procedures
- Problems with hierarchy and intimidation
- Failure in communication with physicians
- Failure of staff to communicate relevant patient information
- Inadequate or incomplete education of staff
1.1. Objectives
- Analyse and understand the problem of RFOs in surgical and maternity settings in Ireland
- Develop hospital-specific RFO management processes and implementation roadmaps
- Provide RFO management toolkits
- Ensure impact in healthcare and academia
1.2. New methods for Human Factors Socio-Technical Modelling
- It is impossible to generalise from one case analysis to other potential situations.
- When one uses FRAM or STAMP to analyse a particular case in order to project how it might pan out in the future, it is necessary to put values on key variables in order to draw inferences about how they might perform and influence other variables in the future [27]. In the absence of a theory, this becomes rather subjective and can easily lead to wrong predictions. This is a serious problem that is not commonly recognised by the advocates of these models [27].
- A process map details the sequence involved in transforming input to output. This supports a high-level ‘decision point map’ which can both represent the status of the relevant dependencies, and show how the dependencies of intersecting processes can be represented (e.g., map the key steps in the delivery process and highlight the current barriers/blockers).
- An information map denotes the flow of information and the sharing of knowledge. It is designed to highlight cycles of transformation and validation of knowledge and information (e.g., what type of patient information is required in what format, etc.).
- A social relations/team map describes the network of connections between people involved in the process. This highlights the reciprocal relations amongst sub-groups which provide social structure to sustain activity (e.g., capturing the lived experiences and challenges of different healthcare staff) [27].
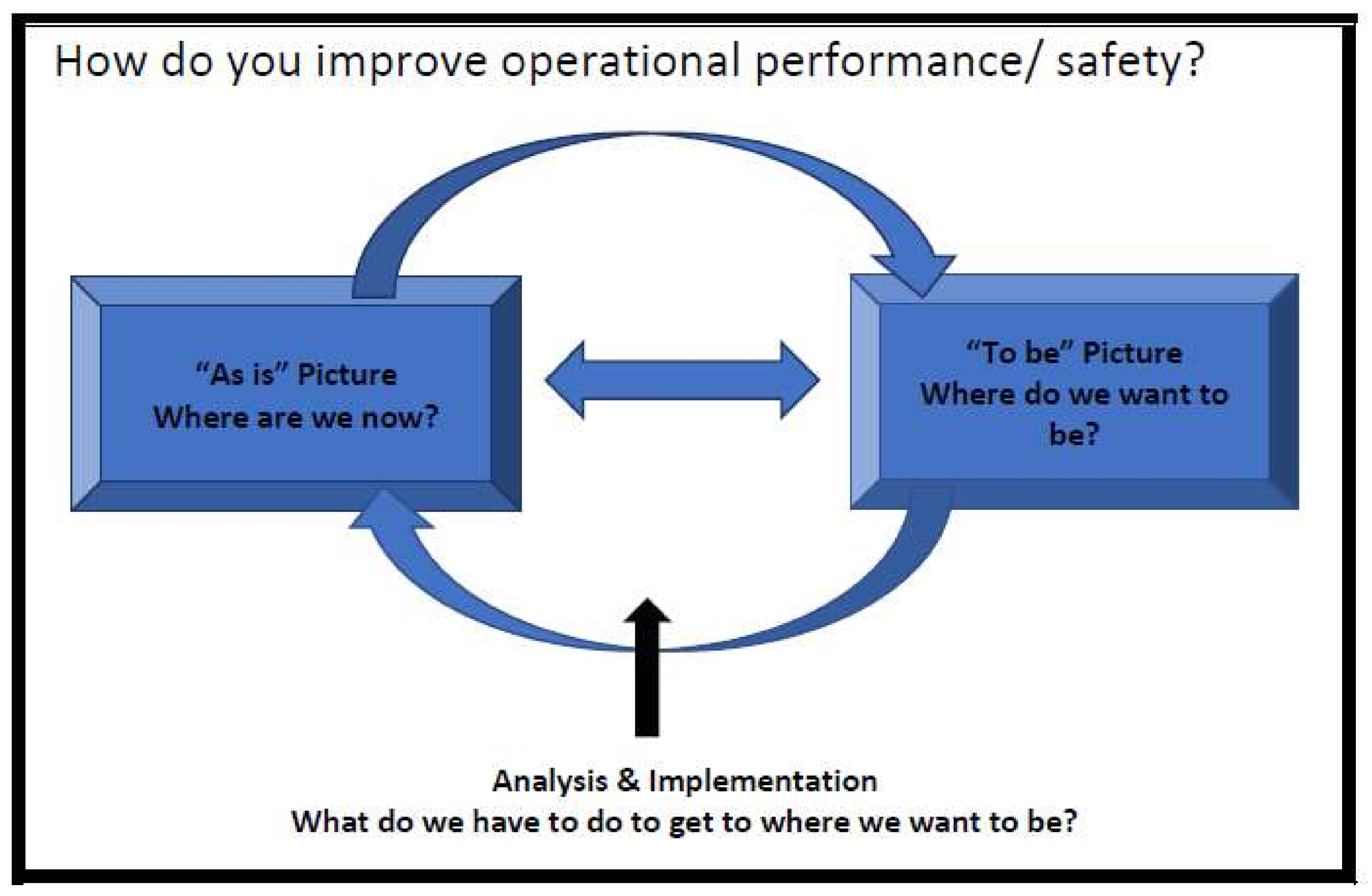
1.3. Context of the Research
2. Materials and Methods
- “The process of developing and evaluating a complex intervention has several phases, although they may not follow a linear sequence”. The research in the project covers the development and pilot phases.
- “Complex interventions may work best if tailored to local circumstances rather than being completely standardised”. This research will define complex interventions but also builds a customisation and implementation process.
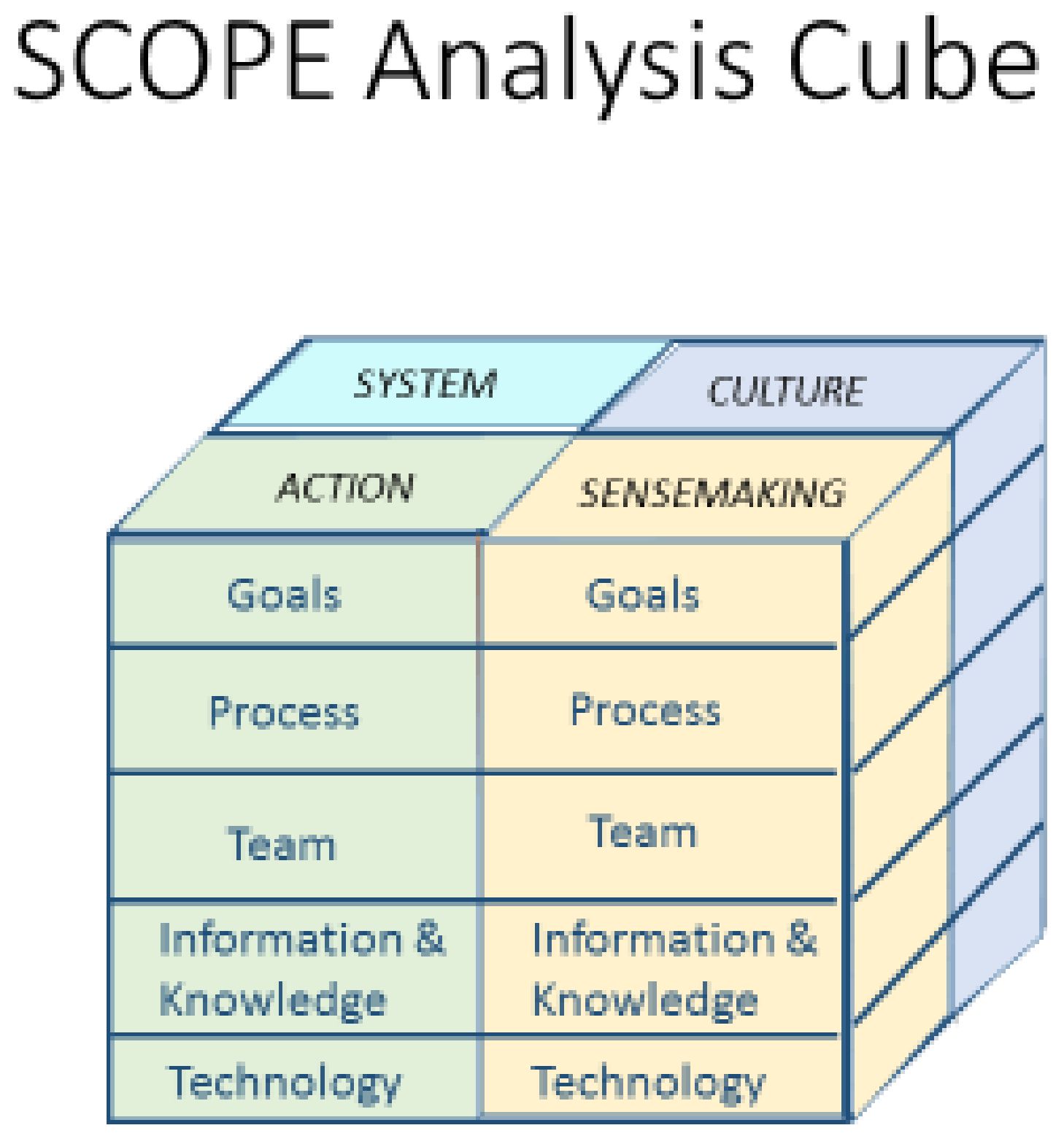
- Phase 1: Adapting SCOPE Analysis Cube to the specific research objectives topic
- Phase 2: Developing process maps & STS analysis
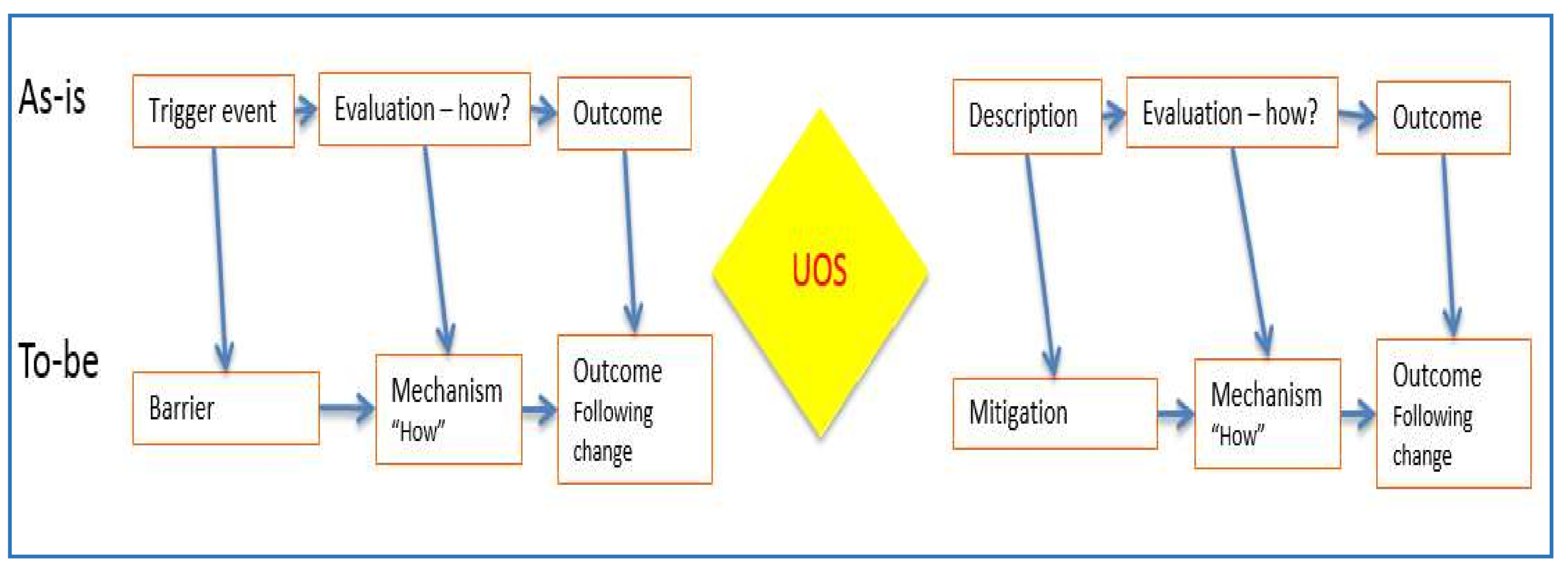
- Phase 3: Examining the Risk in Proposed Change Interventions (Bow Tie Analysis)
- Phase 4: Selecting Interventions & Implementation Road Map
2.1. Phase 1: Adapting SCOPE Analysis Cube to the Specific Research Objectives Topic
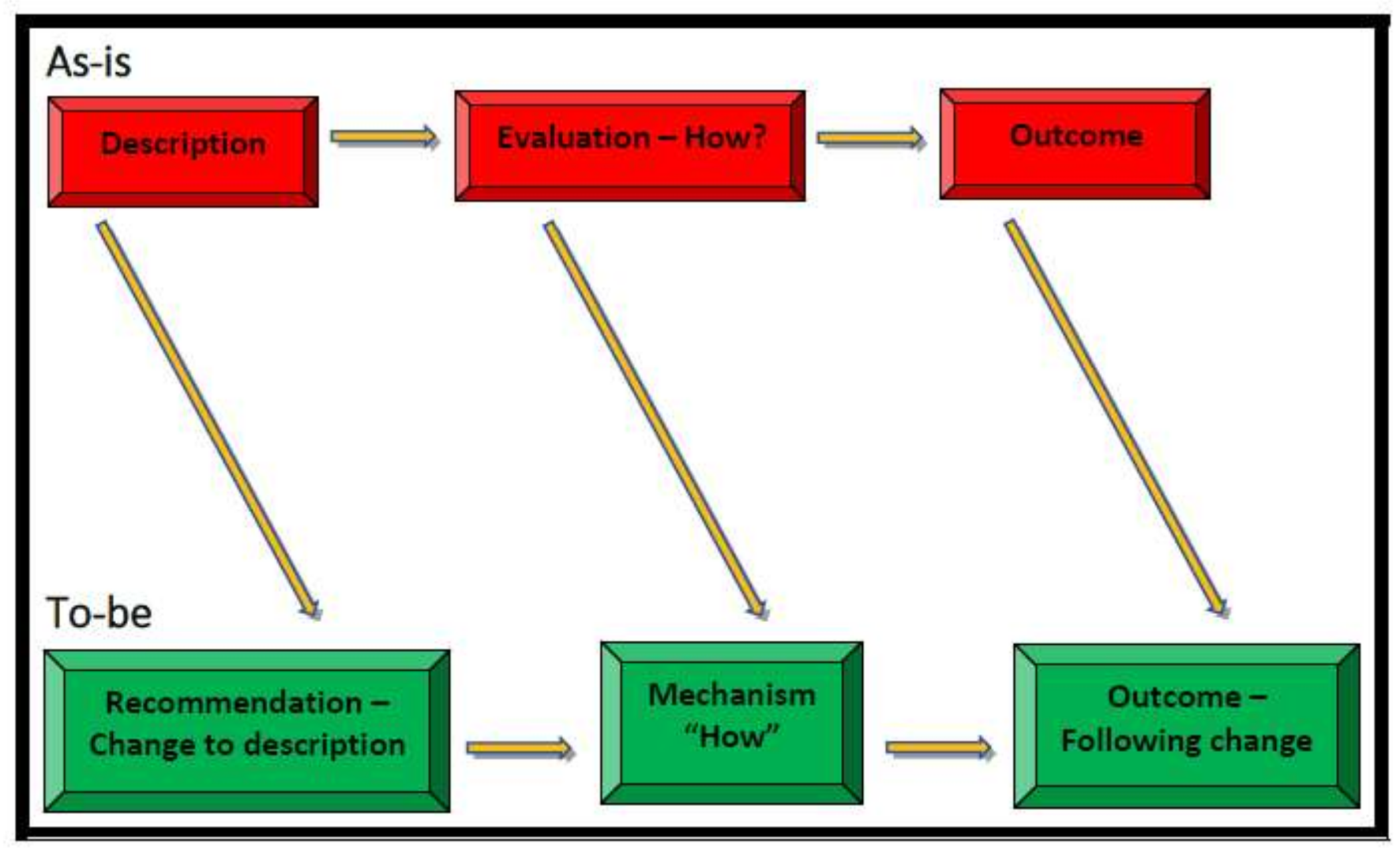
2.2. Phase 2: Developing Process Maps and STS Analysis
- Surgery: (Aim: 20 participants)
- Maternity: (Aim: 20 participants)
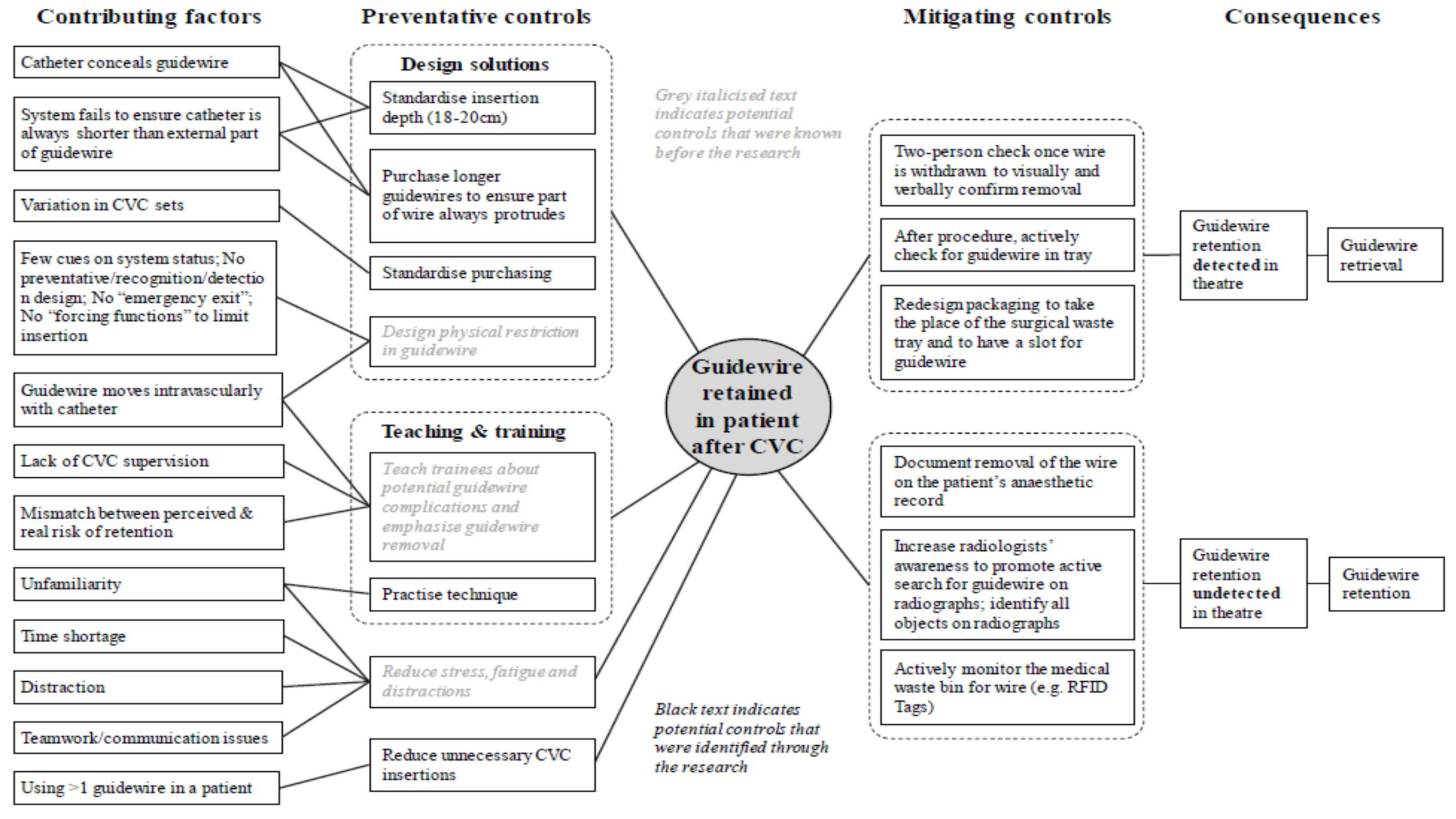
2.3. Phase 3: Examining the Risk in Proposed Change Interventions (Bow Tie Analysis)
2.4. Phase 4: Select Interventions and Implementation Road Map
3. Discussion
- RFO as an issue, traverses multiple specialties from surgery, maternity, gynaecology to medicine. Identifying a successful model of implementation of human factors risk management in healthcare which traverses multiple disciplines and multiple specialties would be a significant progressive step. Additionally, it would fully support the Health Service Executive’s (HSE) Integrated Care aims through the Five Integrated Care Programmes of which maternity is one. Poor communication, hierarchical structures and the absence of a culture of “speaking up” are identified barriers to preventing change and improving care.
- Process and outcome measures will be identified to support ongoing evaluation of RFO defined as a “serious reportable event” (SRE) by the HSE [38]. RFO is classified as an event which should never happen and considered “unacceptable and eminently preventable” by the National Health Service (NHS) [39].
- This research project may lead to reduced physical and psychological harm to patients and reduce risk of mortality. While deaths from RFO have not been recorded in the Irish Health Service in recent times, the frequency of RFO incidents makes them a significant risk in this regard. Cases of septicemia related to RFO have been identified which required urgent admission to hospital, intravenous antibiotics and surgical removal of RFO. Additionally, reduction in RFO will reduce the risk of “second victim” (which may include symptoms of anxiety, stress, loss of confidence, insomnia, depression and sometimes suicide) in clinicians involved in a RFO incident.
- Improved public confidence and trust in the national healthcare system may stem from this research work through prevention of incidents of RFO. The latter have the ability to attract significant negative media attention and, together with other SREs, are used as an international comparator for healthcare systems. Claims have a reputational cost to the Irish Healthcare System at an international, national, institutional and individual healthcare professional level.
4. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Stawicki, S.P.; Moffatt-Bruce, S.D.; Ahmed, H.M.; Anderson, H.L.; Balija, T.M.; Bernescu, I.; Chan, L.; Chowayou, L.; Cipolla, J.; Coyle, S.M.; et al. Retained surgical items: A problem yet to be solved. J. Am. Coll. Surg. 2013, 216, 15–22. [Google Scholar] [CrossRef] [PubMed]
- Smith, Y.; Burke, L. Swab and Instrument Count Practice: Ways to Enhance Patient Safety. Br. J. Nurs. 2014, 23, 590–593. [Google Scholar] [CrossRef] [PubMed]
- Rupp, C.C.; Kagarise, M.J.; Nelson, S.M.; Deal, A.M.; Phillips, S.; Chadwick, J.; Petty, T.; Meyer, A.A.; Kim, H.J. Effectiveness of a radiofrequency detection system as an adjunct to manual counting protocols for tracking surgical sponges: A prospective trial of 2285 patients. J. Am. Coll. Surg. 2012, 215, 524–533. [Google Scholar] [CrossRef] [PubMed]
- Slattery, D. Clinical Incidents and Claims Report in Maternity and Gynaecology Services: A Five Year Review: 2010–2014. 2015. Available online: http://stateclaims.ie/wp-content/uploads/2015/10/SCAClinicalIncidentsClaimsReportOct2015FINAL.pdf (accessed on 10 December 2017).
- Mehtsun, W.T.; Ibrahim, A.M.; Diener-West, M.; Pronovost, P.J.; Makary, M.A. Surgical never events in the United States. Surgery 2013, 153, 465–472. [Google Scholar] [CrossRef] [PubMed]
- Stawicki, S.P.; Cook, C.H.; Anderson, H.L., III; Chowayou, L.; Cipolla, J.; Ahmed, H.M.; Coyle, S.M.; Gracias, V.H.; Evans, D.C.; Marchigiani, R.; et al. Natural history of retained surgical items supports the need for team training, early recognition, and prompt retrieval. Am. J. Surg. 2014, 208, 65–72. [Google Scholar] [CrossRef] [PubMed]
- Hignett, S.; Lang, A.; Pickup, L.; Ives, C.; Fray, M.; McKeown, C.; Tapley, S.; Woodward, M.; Bowie, P. More holes than cheese. What prevents the delivery of effective, high quality and safe health care in England? Ergonomics 2016, in press. [Google Scholar] [CrossRef] [PubMed]
- Fencl, J.L. Guideline Implementation: Prevention of retained surgical items. Assoc. Perioper. Regist. Nurses 2016, 104, 37–48. [Google Scholar] [CrossRef] [PubMed]
- State Claims Agency. National Clinical Incidents, Claims and Costs Report: Lessons Learned, A Five Year Review: 2010–2014. 2017. Available online: http://stateclaims.ie/wp-content/uploads/2017/05/State-Claims-Agency-National-Clinical-Incidents-Claims-and-Costs-Report.pdf (accessed on 10 December 2017).
- Lincourt, A.E.; Harrell, A.; Cristiano, J.; Sechrist, C.; Kercher, K.; Heniford, B.T. Retained foreign bodies after surgery. J. Surg. Res. 2007, 138, 170–174. [Google Scholar] [CrossRef] [PubMed]
- Lutgendorf, M.A.; Schindler, L.L.; Hill, J.B.; Magann, E.F.; O’Boyle, J.D. Implementation of a protocol to reduce occurrence of retained sponges after vaginal delivery. Mil. Med. 2011, 176, 702–704. [Google Scholar] [CrossRef] [PubMed]
- Minnesota Department of Health. Retained Foreign Objects. In Adverse Health Events in Minnesota: Fifth Annual Public Report; Minnesota Department of Health: St Paul, MN, USA, 2009. [Google Scholar]
- Joint Commission Sentinel Event Alert. Preventing Unintended Retained Foreign Objects. 2013, pp. 1–5. Available online: http://www.jointcommission.org/assets/1/6/SEA_51_URFOs_10_17_13_FINAL.pdf (accessed on 19 December 2017).
- Association of Peri-Operative Registered Nurses. Guideline for Prevention of Retained Surgical Items. In Guidelines for Perioperative Practice; AORN Inc.: Denver, CO, USA, 2017; pp. 375–421. [Google Scholar]
- Steelman, V.M.; Cullen, J.J. Designing a safer process to prevent retained surgical sponges: A healthcare failure mode and effect analysis. AORN J. 2011, 94, 132–141. [Google Scholar] [CrossRef] [PubMed]
- Egorova, N.N.; Moskowitz, A.; Gelijns, A.; Weinberg, A.; Curty, J.; Rabin-Fastman, B.; Kaplan, H.; Cooper, M.; Fowler, D.; Emond, J.C.; et al. Managing the prevention of retained surgical instruments: what is the value of counting? Ann. Surg. 2008, 247, 13–18. [Google Scholar] [CrossRef] [PubMed]
- Bardes, J.M.; Inaba, K. The use of radiofrequency detection to mitigate the risk of retained surgical sponges. Adv. Surg. 2017, 51, 219–227. [Google Scholar] [CrossRef] [PubMed]
- Cima, R.R.; Kollengode, A.; Garnatz, J.; Storsveen, A.; Weisbrod, C.; Deschamps, C. Incidence and Characteristics of potential and actual retained foreign objects in surgical patients. Am. Coll. Surg. 2008, 207, 80–87. [Google Scholar] [CrossRef] [PubMed]
- Steelman, V.M. Sensitivity of detection of radiofrequency surgical sponges: A prospective, cross-over study. Am. J. Surg. 2011, 201, 233–237. [Google Scholar] [CrossRef] [PubMed]
- Inaba, K.; Okoye, O.; Aksoy, H.; Skiada, D.; Ault, G.; Sener, S.; Demetriades, D. The role of radio frequency detection system embedded surgical sponges in preventing retained surgical sponges: A prospective evaluation in patients undergoing emergency surgery. Ann. Surg. 2016, 264, 599–604. [Google Scholar] [CrossRef] [PubMed]
- Gillespie, B.M.; Marshall, A. Implementation of safety checklists in surgery: A realist synthesis of evidence. Implement. Sci. 2015, 137, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Moffatt-Bruce, S.D.; Cook, C.H.; Steinberg, S.M.; Stawicki, S.P. Risk factors for retained surgical items: A meta-analysis and proposed risk stratification system. J. Surg. Res. 2014, 190, 429–436. [Google Scholar] [CrossRef] [PubMed]
- Carayon, P.; Hancock, P.; Leveson, N.; Noy, Y.; Sznelwar, L.; van Hootegem, G. Advancing a Sociotechnical Systems Approach to Workplace Safety: Developing the Conceptual Framework. Ergonomics 2015, 58, 548–564. [Google Scholar] [CrossRef] [PubMed]
- Robertson, M.; Hettinger, L.; Waterson, P.; Noya, I.Y.; Dainoff, M.; Leveson, N.G.; Carayon, P.; Courtney, K. Sociotechnical approaches to workplace safety: Research needs and opportunities. Ergonomics 2015, 58, 650–658. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hollnagel, E. FRAM Functional Resonance Analysis Method; Ashgate: Farnham, UK, 2012. [Google Scholar]
- Leveson, N. Engineering a Safer World; MIT Press: Cambridge, MA, USA, 2012. [Google Scholar]
- Mc Donald, N. The Evaluation of Change. J. Cognit. Technol. Work 2015, 17, 193–206. [Google Scholar] [CrossRef]
- Managing System Change in Aviation (MASCA). EU FP7 2010–2013. MASCA. Available online: https://cordis.europa.eu/project/rcn/97673_en.html (accessed on 6 April 2018).
- Proactive Safety Performance for Operations (PROSPERO). EU FP7 2012–2015. PROSPERO: York, UK. Available online: https://cordis.europa.eu/project/rcn/105505_en.html (accessed on 6 April 2018).
- Advanced Cockpit for the Reduction of Stress and Workload (ACROSS). EU FP7 2013–2016. Available online: https://cordis.europa.eu/project/rcn/106358_en.html (accessed on 6 April 2018).
- McDonald, N.; Morrison, R.; Kay, A.; Ryan, M.; Zon, R.; Brouwer, O.; Fereira, A. Validation of Human Factors Components; ACROSS.4-3, Internal Report to the European Commission; Trinity College: Dublin, Ireland, April 2016. [Google Scholar]
- Corrigan, S.; Martensson, L.; Kay, A.; Okwir, S.; Ulfvengren, P. Implementing Collaborative Decision Making in European Airports: Challenges & Recommendations. J. Cognit. Technol. Work 2015, 17, 1435–5558. [Google Scholar]
- UK Medical Research Council’s. Developing and Evaluating Complex Interventions: New Guidance. 2006. Available online: www.mrc.ac.uk/complexinterventionsguidance (accessed on 27 December 2017).
- McDonald, N. Case Study Methodology; Internal Working Paper; Centre for Innovative Human Systems, Trinity College: Dublin, Ireland, 2017. [Google Scholar]
- McDonald, N. What Sort of a Theoretical Model is Required? Internal Working Paper; TCD, CIHS: Hong Kong, China, 2015. [Google Scholar]
- Aviation Risk Management Solutions Working Group (ARMS). The ARMS Methodology for Operational Risk Assessment in Aviation Organisations. Arms Working Group (2007–2010). 2010. Available online: http://www.skybrary.aero/bookshelf/books/1141.pdf (accessed on 20 March 2016).
- Ward, J.R.; Chatzimichailidou, M.M.; Horberry, T.; Teng, Y.-C.; Clarkson, P.J. Guidewire Retention after Central Venous Catheterisation: Prevention and Mitigation using Bow-Tie Analysis. In Proceedings of the Contemporary Ergonomics and Human Factors, Daventry, UK, 19–21 April 2016; pp. 95–99. [Google Scholar]
- Health Service Executive. Serious Reportable Events (SREs). HSE Implementation Guidance Document; Health Service Executive: Dublin, Ireland, 2015; pp. 1–17.
- NHS England Patient Safety Domain. Never Event List 2015/2016. 27 March 2015. Available online: https://www.england.nhs.uk/wp-content/uploads/2015/03/never-evnts-list-15-16.pdf (accessed on 20 March 2016).
- Sittig, D.F.; Singh, H. A New Socio-technical Model for Studying Health Information Technology in Complex Adaptive Healthcare Systems. Qual. Saf. Health Care 2010, 19 (Suppl. 3), 68–74. [Google Scholar] [CrossRef] [PubMed]
- Kamal, N.; Kelly Barnard, D.; Christenson, J.M.; Innes, G.D.; Aikman, P. Addressing Emergency Department Overcrowding through a Systems Approach Using Big Data Research. J. Health Med. Inform. 2014, 5, 148. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Goals | Best Care for Each Patient—Best Outcomes & Experiences, Reduction in Adverse Outcomes |
|---|---|
| Process | What tools, equipment, resources (including time and people), are available? What tasks are relevant? What are the critical points for the process? What are the relevant dependencies? |
| Team | Team relations, accountability, how do people collaborate? Is there a time, place mechanism for them to talk? |
| Information & Knowledge | Data transformation, knowledge cycle. Do people get the right information at the right time? |
| Technology | Technology functions/automation. How does software (& hardware) support the operational process? How do they support the people? |
| Goals | Reduction in Adverse Outcomes |
|---|---|
| Process | All relevant tasks (ward, theatre, admin) mapped (including variability, uncertainty, hazards) |
| Team | Co-ordination. Are everyone’s responsibilities clear? Do they know what they should be doing (with whom? And when?)? |
| Information & Knowledge | Operational data Information is captured AND shared between the right people at the right time |
| Technology | Automation Centralisation, standardisation of technology where appropriate. |
| Goals | Shared Understanding of Roles and Responsibilities for All Operations (Medical, Surgical, Admin, etc.) |
|---|---|
| Process | Staff understand the operational process AND what that means in terms of workload, potential risks, hazards, error. |
| Team | Collaboration—Does everyone have an opportunity to contribute? Team structure & support (awareness of social network) Trust—Is there transparency in the process? Everyone’s roles and responsibilities? |
| Information & Knowledge | Are staff able to anticipate what is happening/should happen? Is there good (individual and collective) situation awareness? What decision support is available for staff to use (independently and as a group)? |
| Technology | Does the software and interface support the flow of information as it should for individuals, teams, management? |
| Goals | Best Care for Patient Best Care for STAFF Shared Vision for Above Valued by Staff |
|---|---|
| Process | What norms of behaviour & everyday practice? What are the relevant organisational routines? |
| Team | How is/are the organisation(s) divided? Are there professional/personal subcultures? Would it be useful to provide an analysis of this? |
| Information & Knowledge | Good common operational picture, shared situational awareness and understanding. Flow of information supports this. |
| Technology | Technology (state-of-the-art) is trusted by staff, used by staff and designed/reviewed by staff (sense of ownership) |
| Hospital Information/Documentation | |
|---|---|
| 1. | Prevention of Retained Surgical Items Policy |
| 2. | Swabs, Sharps & Instrument Count Policy |
| 4. | Count sheet (in-chart documentation used for every procedure) |
| 5. | Post-operative note (in-chart Surgeon’s operative sheet) |
| 6. | C.S.S.D./H.S.S.D. (Central Sterile Services Department/Hospital Sterile Services Department) Instrument Policy (sterile instrument service) |
| 7. | Reporting Protocol/Policy |
| 8. | Incident Report Form/Risk Management Form |
| 9. | Surgical Safety Checklist Policy/Documentation |
| 10. | Policy availability—Hard copy or Intranet |
| 11. | Monitoring process for read policies |
| 12. | New staff orientation information on Foreign Object Retention |
| Profession | Role | Number |
|---|---|---|
| Surgeon | Consultant | 2 |
| Registrar | 2 | |
| Senior House Officer | 1 | |
| Nurse | Scrub | 3 |
| Circulating | 3 (total = 6) | |
| Anaesthetist | Consultant | 1 |
| Registrar | 1 | |
| Senior House Officer | 1 | |
| Clinical Nurse Manager (CNM) | CNM 3 | 1 |
| CNM 2 | 1 | |
| CNM 1 | (total = 2/3) | |
| Clinical Facilitator | Policy involvement | 1 |
| Clinical Risk Manager | Risk manager | 1 |
| Stores Manager | Equipment/stock orders | 1 |
| Cleaners Sterile Services | Theatre cleaner | 1 |
| Equipment sterilisation | 1 |
| Profession | Role | Number |
|---|---|---|
| Obstetrician | Consultant | 2 |
| Registrar | 2 | |
| Midwife/Nurse | Scrub/Circulating (theatre) | 2 |
| Midwife | 6 | |
| Anaesthetist | Consultant | 1 |
| Registrar | 1 | |
| Senior House Officer | 1 | |
| Clinical Midwife/Nurse Manager (CMM/CNM) | CMM/CNM 3 | 1 |
| CMM 2 | 1 | |
| CMM 1 | 1 | |
| Clinical Facilitator | Policy involvement | 1 |
| Clinical Risk Manager | Risk manager | 1 |
| Stores Manager | Equipment/stock orders | 1 |
| Cleaners Sterile Services | Theatre cleaner | 1 |
| Equipment sterilisation | 1 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Corrigan, S.; Kay, A.; O’Byrne, K.; Slattery, D.; Sheehan, S.; McDonald, N.; Smyth, D.; Mealy, K.; Cromie, S. A Socio-Technical Exploration for Reducing & Mitigating the Risk of Retained Foreign Objects. Int. J. Environ. Res. Public Health 2018, 15, 714. https://doi.org/10.3390/ijerph15040714
Corrigan S, Kay A, O’Byrne K, Slattery D, Sheehan S, McDonald N, Smyth D, Mealy K, Cromie S. A Socio-Technical Exploration for Reducing & Mitigating the Risk of Retained Foreign Objects. International Journal of Environmental Research and Public Health. 2018; 15(4):714. https://doi.org/10.3390/ijerph15040714
Chicago/Turabian StyleCorrigan, Siobhán, Alison Kay, Katie O’Byrne, Dubhfeasa Slattery, Sharon Sheehan, Nick McDonald, David Smyth, Ken Mealy, and Sam Cromie. 2018. "A Socio-Technical Exploration for Reducing & Mitigating the Risk of Retained Foreign Objects" International Journal of Environmental Research and Public Health 15, no. 4: 714. https://doi.org/10.3390/ijerph15040714