Evaluation of a Pilot School-Based Physical Activity Clustered Randomised Controlled Trial—Active Schools: Skelmersdale

 ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
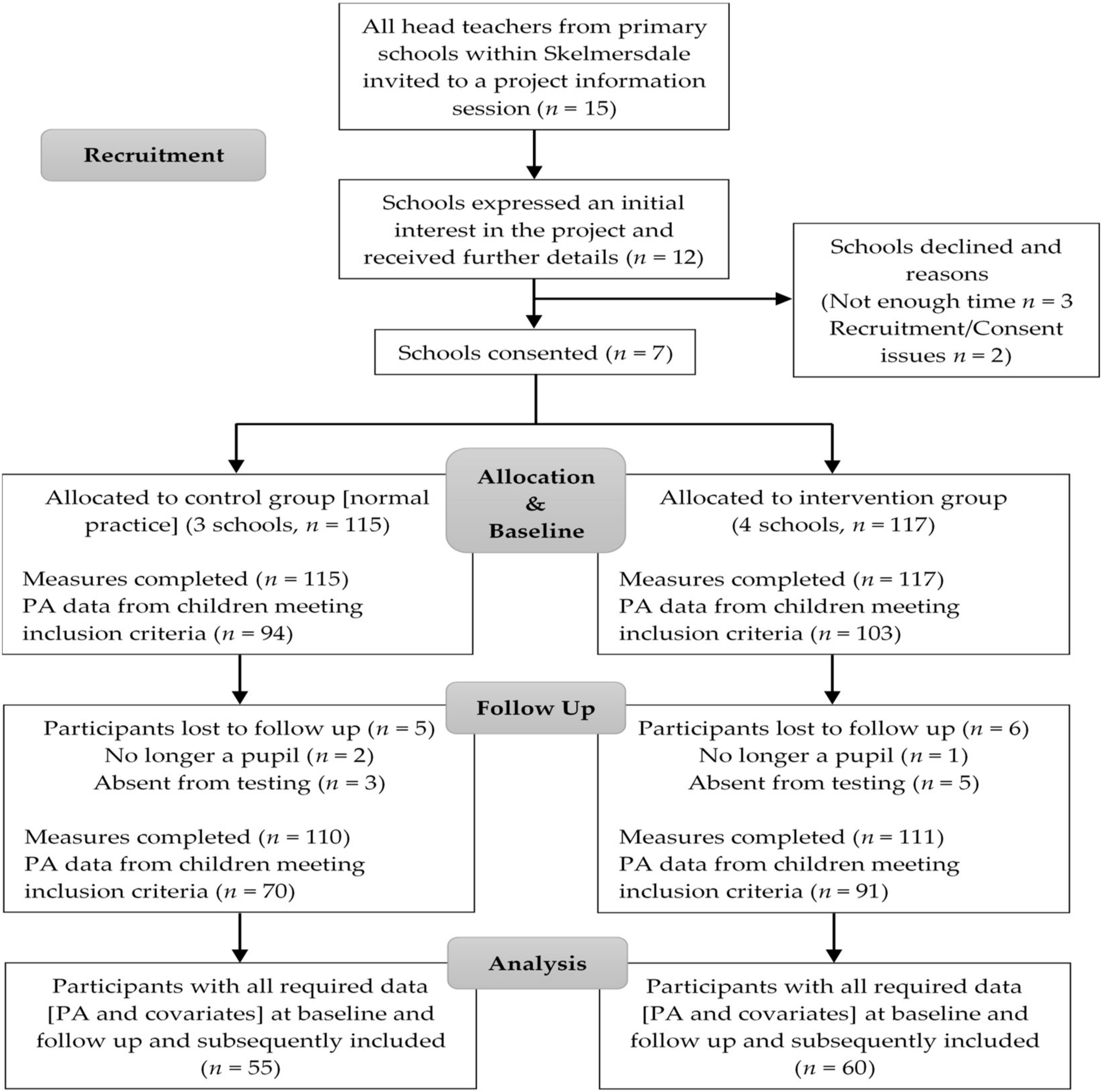
2.1. Participants
2.2. Study Design
2.3. Intervention
2.4. Measures
2.4.1. Physical Activity
2.4.2. Anthropometrics
2.4.3. Cardiorespiratory Fitness (CRF)
2.4.4. Psychological Constructs
2.4.5. Socioeconomic Status (SES)
2.5. Statistical Analysis
3. Results
3.1. Preliminary Results
3.2. Intervention Effects
3.3. Sub-Group Analyses
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Cooper, A.R.; Goodman, A.; Page, A.S.; Sherar, L.B.; Esliger, D.W.; van Sluijs, E.M.; Andersen, L.B.; Anderssen, S.; Cardon, G.; Davey, R.; et al. Objectively measured physical activity and sedentary time in youth: The International children’s accelerometry database (ICAD). Int. J. Behav. Nutr. Phys. Act. 2015, 12, 113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hallal, P.C.; Andersen, L.B.; Bull, F.C.; Guthold, R.; Haskell, W.; Ekelund, U. Global physical activity levels: Surveillance progress, pitfalls, and prospects. Lancet 2012, 380, 247–257. [Google Scholar] [CrossRef]
- Poitras, V.J.; Gray, C.E.; Borghese, M.M.; Carson, V.; Chaput, J.P.; Janssen, I.; Katzmarzyk, P.T.; Pate, R.R.; Connor Gorber, S.; Kho, M.E.; et al. Systematic review of the relationships between objectively measured physical activity and health indicators in school-aged children and youth. Appl. Physiol. Nutr. Metab. 2016, 41 (Suppl. 3), S197–S239. [Google Scholar] [CrossRef] [PubMed]
- Lubans, D.; Richards, J.; Hillman, C.; Faulkner, G.; Beauchamp, M.; Nilsson, M.; Kelly, P.; Smith, J.; Raine, L.; Biddle, S. Physical Activity for Cognitive and Mental Health in Youth: A Systematic Review of Mechanisms. Pediatrics 2016, 138, e20161642. [Google Scholar] [CrossRef] [PubMed]
- Reddon, H.; Meyre, D.; Cairney, J. Physical Activity and Global Self-worth in a Longitudinal Study of Children. Med. Sci. Sports Exerc. 2017, 49, 1606–1613. [Google Scholar] [CrossRef] [PubMed]
- Pearson, N.; Haycraft, E.; Johnston, J.P.; Atkin, A.J. Sedentary behaviour across the primary-secondary school transition: A systematic review. Prev. Med. 2017, 94, 40–47. [Google Scholar] [CrossRef] [PubMed]
- Carson, V.; Hunter, S.; Kuzik, N.; Gray, C.E.; Poitras, V.J.; Chaput, J.P.; Saunders, T.J.; Katzmarzyk, P.T.; Okely, A.D.; Connor Gorber, S. Systematic review of sedentary behaviour and health indicators in school-aged children and youth: An update. Appl. Physiol. Nutr. Metab. 2016, 41, S240–S265. [Google Scholar] [CrossRef] [PubMed]
- Hesketh, K.R.; Lakshman, R.; van Sluijs, E.M.F. Barriers and facilitators to young children’s physical activity and sedentary behaviour: A systematic review and synthesis of qualitative literature. Obes. Rev. 2017, 18, 987–1017. [Google Scholar] [CrossRef] [PubMed]
- Burns, R.D.; Fu, Y.; Podlog, L.W. School-based physical activity interventions and physical activity enjoyment: A meta-analysis. Prev. Med. 2017, 103, 84–90. [Google Scholar] [CrossRef] [PubMed]
- Childhood Obesity: A Plan for Action; HM Government: London, UK, 2016.
- Medicine, I.O. (Ed.) Educating the Student Body: Taking Physical Activity and Physical Education to School; The National Academies Press: Washington, DC, USA, 2013. [Google Scholar]
- Chief Medical Officer Department of Health. Start Active, Stay Active: A Report on Physical Activity from the Four Home Countries; Department of Health: London, UK, 2011.
- Tremblay, M.S.; Carson, V.; Chaput, J.P.; Connor Gorber, S.; Dinh, T.; Duggan, M.; Faulkner, G.; Gray, C.E.; Gruber, R.; Janson, K.; et al. Canadian 24-Hour Movement Guidelines for Children and Youth: An Integration of Physical Activity, Sedentary Behaviour, and Sleep. Appl. Physiol. Nutr. Metab. 2016, 41 (Suppl. 3), S311–S327. [Google Scholar] [CrossRef] [PubMed]
- Physical Activity Guidelines 2017; Health Council of the Netherlands: The Hague, The Netherlands, 2017.
- Erwin, H.; Beighle, A.; Carson, R.L.; Castelli, D.M. Comprehensive School-Based Physical Activity Promotion: A Review. Quest 2013, 65, 412–428. [Google Scholar] [CrossRef]
- Russ, L.B.; Webster, C.A.; Beets, M.W.; Phillips, D.S. Systematic Review and Meta-Analysis of Multi-Component Interventions Through Schools to Increase Physical Activity. J. Phys. Act. Health 2015, 12, 1436–1446. [Google Scholar] [CrossRef] [PubMed]
- Kenneth, R.M.; Daniel, B.; Allan, S.; Karen, G. An Ecological Perspective on Health Promotion Programs. Health Educ. Q. 1988, 15, 351–377. [Google Scholar]
- Naylor, P.-J.; Macdonald, H.M.; Reed, K.E.; McKay, H.A. Action Schools! BC: A Socioecological Approach to Modifying Chronic Disease Risk Factors in Elementary School Children. Prev. Chronic Dis. 2006, 3, A60. [Google Scholar] [PubMed]
- Naylor, P.-J.; Macdonald, H.M.; Zebedee, J.A.; Reed, K.E.; McKay, H.A. Lessons learned from Action Schools! BC—An ‘active school’ model to promote physical activity in elementary schools. J. Sci. Med. Sport 2006, 9, 413–423. [Google Scholar] [CrossRef] [PubMed]
- Kellou, N.; Sandalinas, F.; Copin, N.; Simon, C. Prevention of unhealthy weight in children by promoting physical activity using a socio-ecological approach: What can we learn from intervention studies? Diabetes Metab. 2014, 40, 258–271. [Google Scholar] [CrossRef] [PubMed]
- Murillo Pardo, B.; García Bengoechea, E.; Generelo Lanaspa, E.; Bush, P.L.; Zaragoza Casterad, J.; Julián Clemente, J.A.; García González, L. Promising school-based strategies and intervention guidelines to increase physical activity of adolescents. Health Educ. Res. 2013, 28, 523–538. [Google Scholar] [CrossRef] [PubMed]
- Van Sluijs, E.M.F.; McMinn, A.M.; Griffin, S.J. Effectiveness of interventions to promote physical activity in children and adolescents: Systematic review of controlled trials. BMJ 2007, 335, 703–707. [Google Scholar] [CrossRef] [PubMed]
- Owen, M.B.; Curry, W.B.; Kerner, C.; Newson, L.; Fairclough, S.J. The effectiveness of school-based physical activity interventions for adolescent girls: A systematic review and meta-analysis. Prev. Med. 2017, 105, 237–249. [Google Scholar] [CrossRef] [PubMed]
- Okely, A.D.; Lubans, D.R.; Morgan, P.J.; Cotton, W.; Peralta, L.; Miller, J.; Batterham, M.; Janssen, X. Promoting physical activity among adolescent girls: The Girls in Sport group randomized trial. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 81. [Google Scholar] [CrossRef] [PubMed]
- Van Kann, D.H.; Kremers, S.P.; de Vries, N.K.; de Vries, S.I.; Jansen, M.W. The effect of a school-centered multicomponent intervention on daily physical activity and sedentary behavior in primary school children: The Active Living study. Prev. Med. 2016, 89, 64–69. [Google Scholar] [CrossRef] [PubMed]
- Beets, M.W.; Okely, A.; Weaver, R.G.; Webster, C.; Lubans, D.; Brusseau, T.; Carson, R.; Cliff, D.P. The theory of expanded, extended, and enhanced opportunities for youth physical activity promotion. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 120. [Google Scholar] [CrossRef] [PubMed]
- Collins, S. Seven Wards: A Focus on Skelmersdale; Lancashire, C.C., Ed.; Lancashire County Council: Preston, UK, 2015.
- Hemming, K.; Girling, A.J.; Sitch, A.J.; Marsh, J.; Lilford, R.J. Sample size calculations for cluster randomised controlled trials with a fixed number of clusters. BMC Med. Res. Methodol. 2011, 11, 102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taylor, S.L.; Curry, W.B.; Knowles, Z.R.; Noonan, R.J.; McGrane, B.; Fairclough, S.J. Predictors of Segmented School Day Physical Activity and Sedentary Time in Children from a Northwest England Low-Income Community. Int. J. Environ. Res. Public Health 2017, 14, E534. [Google Scholar] [CrossRef] [PubMed]
- Campbell, M.K.; Piaggio, G.; Elbourne, D.R.; Altman, D.G. Consort 2010 statement: Extension to cluster randomised trials. BMJ 2012, 345, e5661. [Google Scholar] [CrossRef] [PubMed]
- Welk, G.J. The Youth Physical Activity Promotion Model: A Conceptual Bridge Between Theory and Practice. Quest 1999, 51, 5–23. [Google Scholar] [CrossRef]
- Watson, A.; Timperio, A.; Brown, H.; Hesketh, K.D. A primary school active break programme (ACTI-BREAK): Study protocol for a pilot cluster randomised controlled trial. Trials 2017, 18, 433. [Google Scholar] [CrossRef] [PubMed]
- Carlson, J.A.; Engelberg, J.K.; Cain, K.L.; Conway, T.L.; Mignano, A.M.; Bonilla, E.A.; Geremia, C.; Sallis, J.F. Implementing classroom physical activity breaks: Associations with student physical activity and classroom behavior. Prev. Med. 2015, 81, 67–72. [Google Scholar] [CrossRef] [PubMed]
- McKay, H.; MacLean, L.; Petit, M.; MacKelvie-O’Brien, K.; Janssen, P.; Beck, T.; Khan, K. “Bounce at the Bell”: A novel program of short bouts of exercise improves proximal femur bone mass in early pubertal children. Br. J. Sports Med. 2005, 39, 521–526. [Google Scholar] [CrossRef] [PubMed]
- Macdonald, H.M.; Kontulainen, S.A.; Khan, K.M.; McKay, H.A. Is a school-based physical activity intervention effective for increasing tibial bone strength in boys and girls? J. Bone Miner. Res. Off. J. Am. Soc. Bone Miner. Res. 2007, 22, 434–446. [Google Scholar] [CrossRef] [PubMed]
- Fairclough, S.J.; McGrane, B.; Sanders, G.; Taylor, S.; Owen, M.; Curry, W. A non-equivalent group pilot trial of a school-based physical activity and fitness intervention for 10–11 year old english children: Born to move. BMC Public Health 2016, 16, 861. [Google Scholar] [CrossRef] [PubMed]
- Sacheck, J.M.; Wright, C.; Amin, S.; Anzman-Frasca, S.; Chomitz, V.; Chui, K.; Nelson, M.; Economos, C. The Fueling Learning Through Exercise (FLEX) Study: Short-term Findings On Sedentary Time In Lower-income Schoolchildren778 May 31 445 PM–500 PM. Med. Sci. Sports Exerc. 2017, 49, 200–201. [Google Scholar] [CrossRef]
- Lubans, D.R.; Lonsdale, C.; Cohen, K.; Eather, N.; Beauchamp, M.R.; Morgan, P.J.; Sylvester, B.D.; Smith, J.J. Framework for the design and delivery of organized physical activity sessions for children and adolescents: Rationale and description of the ‘SAAFE’ teaching principles. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 24. [Google Scholar] [CrossRef] [PubMed]
- Brazendale, K.; Chandler, J.L.; Beets, M.W.; Weaver, R.G.; Beighle, A.; Huberty, J.L.; Moore, J.B. Maximizing children’s physical activity using the LET US Play principles. Prev. Med. 2015, 76, 14–19. [Google Scholar] [CrossRef] [PubMed]
- Lubans, D.R.; Morgan, P.J.; Weaver, K.; Callister, R.; Dewar, D.L.; Costigan, S.A.; Finn, T.L.; Smith, J.; Upton, L.; Plotnikoff, R.C. Rationale and study protocol for the supporting children’s outcomes using rewards, exercise and skills (SCORES) group randomized controlled trial: A physical activity and fundamental movement skills intervention for primary schools in low-income communities. BMC Public Health 2012, 12, 427. [Google Scholar]
- Sutherland, R.; Campbell, E.; Lubans, D.R.; Morgan, P.J.; Okely, A.D.; Nathan, N.; Wolfenden, L.; Wiese, J.; Gillham, K.; Hollis, J.; et al. ‘Physical Activity 4 Everyone’ school-based intervention to prevent decline in adolescent physical activity levels: 12 month (mid-intervention) report on a cluster randomised trial. Br. J. Sports Med. 2016, 50, 488–495. [Google Scholar] [CrossRef] [PubMed]
- Vander Ploeg, K.A.; Maximova, K.; McGavock, J.; Davis, W.; Veugelers, P. Do school-based physical activity interventions increase or reduce inequalities in health? Soc. Sci. Med. 2014, 112, 80–87. [Google Scholar] [CrossRef] [PubMed]
- Fairclough, S.J.; Hackett, A.F.; Davies, I.G.; Gobbi, R.; Mackintosh, K.A.; Warburton, G.L.; Stratton, G.; van Sluijs, E.M.F.; Boddy, L.M. Promoting healthy weight in primary school children through physical activity and nutrition education: A pragmatic evaluation of the CHANGE! randomised intervention study. BMC Public Health 2013, 13, 626. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kriemler, S.; Zahner, L.; Schindler, C.; Meyer, U.; Hartmann, T.; Hebestreit, H.; Brunner-La Rocca, H.P.; van Mechelen, W.; Puder, J.J. Effect of school based physical activity programme (KISS) on fitness and adiposity in primary schoolchildren: Cluster randomised controlled trial. BMJ 2010, 340, c785. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Hees, V.T.; Gorzelniak, L.; Dean Leon, E.C.; Eder, M.; Pias, M.; Taherian, S.; Ekelund, U.; Renstrom, F.; Franks, P.W.; Horsch, A.; et al. Separating movement and gravity components in an acceleration signal and implications for the assessment of human daily physical activity. PLoS ONE 2013, 8, e61691. [Google Scholar] [CrossRef] [PubMed]
- Van Hees, V.T.; Fang, Z.; Langford, J.; Assah, F.; Mohammad, A.; da Silva, I.C.M.; Trenell, M.I.; White, T.; Wareham, N.J.; Brage, S. Autocalibration of accelerometer data for free-living physical activity assessment using local gravity and temperature: An evaluation on four continents. J. Appl. Physiol. 2014, 117, 738–744. [Google Scholar] [CrossRef] [PubMed]
- Fairclough, S.J.; Noonan, R.; Rowlands, A.V.; Van Hees, V.; Knowles, Z.; Boddy, L.M. Wear Compliance and Activity in Children Wearing Wrist- and Hip-Mounted Accelerometers. Med. Sci. Sports Exerc. 2016, 48, 245–253. [Google Scholar] [CrossRef] [PubMed]
- Rowlands, A.V.; Cliff, D.P.; Fairclough, S.J.; Boddy, L.M.; Olds, T.S.; Parfitt, G.; Noonan, R.J.; Downs, S.J.; Knowles, Z.R.; Beets, M.W. Moving Forward with Backward Compatibility: Translating Wrist Accelerometer Data. Med. Sci. Sports Exerc. 2016, 48, 2142–2149. [Google Scholar] [CrossRef] [PubMed]
- Noonan, R.J.; Boddy, L.M.; Kim, Y.; Knowles, Z.R.; Fairclough, S.J. Comparison of children’s free-living physical activity derived from wrist and hip raw accelerations during the segmented week. J. Sports Sci. 2017, 35, 2067–2072. [Google Scholar] [CrossRef] [PubMed]
- Hildebrand, M.; van Hees, V.T.; Hansen, B.H.; Ekelund, U.L.F. Age Group Comparability of Raw Accelerometer Output from Wrist- and Hip-Worn Monitors. Med. Sci. Sports Exerc. 2014, 46, 1816–1824. [Google Scholar] [CrossRef] [PubMed]
- Hildebrand, M.; Hansen, B.H.; van Hees, V.T.; Ekelund, U. Evaluation of raw acceleration sedentary thresholds in children and adults. Scand. J. Med. Sci. Sports 2017, 27, 1814–1823. [Google Scholar] [CrossRef] [PubMed]
- Rich, C.; Geraci, M.; Griffiths, L.; Sera, F.; Dezateux, C.; Cortina-Borja, M. Quality Control Methods in Accelerometer Data Processing: Defining Minimum Wear Time. PLoS ONE 2013, 8, e67206. [Google Scholar] [CrossRef] [PubMed]
- Cole, T.J.; Freeman, J.V.; Preece, M.A. Body mass index reference curves for the UK, 1990. Arch. Dis. Child. 1995, 73, 25–29. [Google Scholar] [CrossRef] [PubMed]
- Cole, T.J.; Bellizzi, M.C.; Flegal, K.M.; Dietz, W.H. Establishing a standard definition for child overweight and obesity worldwide: International survey. BMJ 2000, 320, 1240. [Google Scholar] [CrossRef] [PubMed]
- Mehta, S.K. Waist circumference to height ratio in children and adolescents. Clin. Pediatr. 2015, 54, 652–658. [Google Scholar] [CrossRef] [PubMed]
- Moore, S.A.; McKay, H.A.; Macdonald, H.; Nettlefold, L.; Baxter-Jones, A.D.; Cameron, N.; Brasher, P.M. Enhancing a Somatic Maturity Prediction Model. Med. Sci. Sports Exerc. 2015, 47, 1755–1764. [Google Scholar] [CrossRef] [PubMed]
- Léger, L.A.; Mercier, D.; Gadoury, C.; Lambert, J. The multistage 20 metre shuttle run test for aerobic fitness. J. Sports Sci. 1988, 6, 93–101. [Google Scholar] [CrossRef] [PubMed]
- Boddy, L.M.; Fairclough, S.J.; Atkinson, G.; Stratton, G. Changes in cardiorespiratory fitness in 9- to 10.9-year-old children: SportsLinx 1998–2010. Med. Sci. Sports Exerc. 2012, 44, 481–486. [Google Scholar] [CrossRef] [PubMed]
- Motl, R.W.; Dishman, R.K.; Trost, S.G.; Saunders, R.P.; Dowda, M.; Felton, G.; Ward, D.S.; Pate, R.R. Factorial Validity and Invariance of Questionnaires Measuring Social-Cognitive Determinants of Physical Activity among Adolescent Girls. Prev. Med. 2000, 31, 584–594. [Google Scholar] [CrossRef] [PubMed]
- Motl, R.W.; Dishman, R.K.; Saunders, R.; Dowda, M.; Felton, G.; Pate, R.R. Measuring enjoyment of physical activity in adolescent girls. Am. J. Prev. Med. 2001, 21, 110–117. [Google Scholar] [CrossRef]
- The English Indicies of Deprivation 2015; Ministry of Housing, Communities & Local Government: Wetherby, UK, 2015.
- Rabesh, J.; Charlton, C.; Browne, W.J.; Healy, M.; Cameron, B. MLwiN Version 2.10.; Centre for Multilevel Modelling, University of Bristol: Bristol, UK, 2009. [Google Scholar]
- Twisk, J.W.R. Applied Multilevel Analysis; Cambridge University Press: Cambridge, UK, 2006. [Google Scholar]
- Zaqout, M.; Vyncke, K.; Moreno, L.A.; De Miguel-Etayo, P.; Lauria, F.; Molnar, D.; Lissner, L.; Hunsberger, M.; Veidebaum, T.; Tornaritis, M.; et al. Determinant factors of physical fitness in European children. Int. J. Public Health 2016, 61, 573–582. [Google Scholar] [CrossRef] [PubMed]
- Baquet, G.; Ridgers, N.D.; Blaes, A.; Aucouturier, J.; Van Praagh, E.; Berthoin, S. Objectively assessed recess physical activity in girls and boys from high and low socioeconomic backgrounds. BMC Public Health 2014, 14, 192. [Google Scholar] [CrossRef] [PubMed]
- Borraccino, A.; Lemma, P.; Iannotti, R.J.; Zambon, A.; Dalmasso, P.; Lazzeri, G.; Giacchi, M.; Cavallo, F. Socioeconomic effects on meeting physical activity guidelines: Comparisons among 32 countries. Med. Sci. Sports Exerc. 2009, 41, 749–756. [Google Scholar] [CrossRef] [PubMed]
- Richmond, R.C.; Davey Smith, G.; Ness, A.R.; den Hoed, M.; McMahon, G.; Timpson, N.J. Assessing Causality in the Association between Child Adiposity and Physical Activity Levels: A Mendelian Randomization Analysis. PLoS Med. 2014, 11, e1001618. [Google Scholar] [CrossRef] [PubMed]
- Santos, R.; Mota, J.; Okely, A.D.; Pratt, M.; Moreira, C.; Coelho-e-Silva, M.J.; Vale, S.; Sardinha, L.B. The independent associations of sedentary behaviour and physical activity on cardiorespiratory fitness. Br. J. Sports Med. 2014, 48, 1508–1512. [Google Scholar] [CrossRef] [PubMed]
- Grund, A.; Dilba, B.; Forberger, K.; Krause, H.; Siewers, M.; Rieckert, H.; Müller, M.J. Relationships between physical activity, physical fitness, muscle strength and nutritional state in 5- to 11-year-old children. Eur. J. Appl. Physiol. 2000, 82, 425–438. [Google Scholar] [CrossRef] [PubMed]
- Silva, G.; Andersen, L.B.; Aires, L.; Mota, J.; Oliveira, J.; Ribeiro, J.C. Associations between sports participation, levels of moderate to vigorous physical activity and cardiorespiratory fitness in childrenand adolescents. J. Sports Sci. 2013, 31, 1359–1367. [Google Scholar] [CrossRef] [PubMed]
- Mann, K.D.; Howe, L.D.; Basterfield, L.; Parkinson, K.N.; Pearce, M.S.; Reilly, J.K.; Adamson, A.J.; Reilly, J.J.; Janssen, X. Longitudinal study of the associations between change in sedentary behavior and change in adiposity during childhood and adolescence: Gateshead Millennium Study. Int. J. Obes. 2017, 41, 1042–1047. [Google Scholar] [CrossRef] [PubMed]
- Wilkie, H.J.; Standage, M.; Gillison, F.B.; Cumming, S.P.; Katzmarzyk, P.T. Correlates of intensity-specific physical activity in children aged 9–11 years: A multilevel analysis of UK data from the International Study of Childhood Obesity, Lifestyle and the Environment. BMJ Open 2018, 8, e018373. [Google Scholar] [CrossRef] [PubMed]
- Haapala, H.L.; Hirvensalo, M.H.; Kulmala, J.; Hakonen, H.; Kankaanpää, A.; Laine, K.; Laakso, L.; Tammelin, T.H. Changes in physical activity and sedentary time in the Finnish Schools on the Move program: A quasi-experimental study. Scand. J. Med. Sci. Sports 2017, 27, 1442–1453. [Google Scholar] [CrossRef] [PubMed]
- Carson, V.; Tremblay, M.S.; Chaput, J.P.; Chastin, S.F. Associations between sleep duration, sedentary time, physical activity, and health indicators among Canadian children and youth using compositional analyses. Appl. Physiol. Nutr. Metab. 2016, 41 (Suppl. 3), S294–S302. [Google Scholar] [CrossRef] [PubMed]
- Dumith, S.C.; Gigante, D.P.; Domingues, M.R.; Kohl, H.W. Physical activity change during adolescence: A systematic review and a pooled analysis. Int. J. Epidemiol. 2011, 40, 685–698. [Google Scholar] [CrossRef] [PubMed]
- Dumuid, D.; Stanford, T.E.; Pedišić, Ž.; Maher, C.; Lewis, L.K.; Martín-Fernández, J.-A.; Katzmarzyk, P.T.; Chaput, J.-P.; Fogelholm, M.; Standage, M.; et al. Adiposity and the isotemporal substitution of physical activity, sedentary time and sleep among school-aged children: A compositional data analysis approach. BMC Public Health 2018, 18, 311. [Google Scholar] [CrossRef] [PubMed]
- Fairclough, S.J.; Dumuid, D.; Taylor, S.; Curry, W.; McGrane, B.; Stratton, G.; Maher, C.; Olds, T. Fitness, fatness and the reallocation of time between children’s daily movement behaviours: An analysis of compositional data. Int. J. Behav. Nutr.Phys. Act. 2017, 14, 64. [Google Scholar] [CrossRef] [PubMed]
- Moore, G.F.; Audrey, S.; Barker, M.; Bond, L.; Bonell, C.; Hardeman, W. Process evaluation of complex interventions: Medical Research Council guidance. BMJ 2015, 350, h1258. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Naylor, P.J.; Nettlefold, L.; Race, D.; Hoy, C.; Ashe, M.C.; Wharf Higgins, J.; McKay, H.A. Implementation of school based physical activity interventions: A systematic review. Prev. Med. 2015, 72, 95–115. [Google Scholar] [CrossRef] [PubMed]
- Nathan, N.; Elton, B.; Babic, M.; McCarthy, N.; Sutherland, R.; Presseau, J.; Seward, K.; Hodder, R.; Booth, D.; Yoong, S.L.; et al. Barriers and facilitators to the implementation of physical activity policies in schools: A systematic review. Prev. Med. 2018, 107, 45–53. [Google Scholar] [CrossRef] [PubMed]
- Routen, A.C.; Johnston, J.P.; Glazebrook, C.; Sherar, L.B. Teacher perceptions on the delivery and implementation of movement integration strategies: The CLASS PAL (Physically Active Learning) Programme. Int. J. Educ. Res. 2018, 88, 48–59. [Google Scholar] [CrossRef]
- Dyrstad, S.M.; Kvalø, S.E.; Alstveit, M.; Skage, I. Physically active academic lessons: Acceptance, barriers and facilitators for implementation. BMC Public Health 2018, 18, 322. [Google Scholar] [CrossRef] [PubMed]
- Dobbins, M.; De Corby, K.; Robeson, P.; Husson, H.; Tirilis, D. School-based physical activity programs for promoting physical activity and fitness in children and adolescents aged 6–18. Cochrane Database Syst. Rev. 2009, 28, CD007651. [Google Scholar]
- Møller, N.C.; Tarp, J.; Kamelarczyk, E.F.; Brønd, J.C.; Klakk, H.; Wedderkopp, N. Do extra compulsory physical education lessons mean more physically active children—Findings from the childhood health, activity, and motor performance school study Denmark (The CHAMPS-study DK). Int. J. Behav. Nutr. Phys. Act. 2014, 11, 121. [Google Scholar] [CrossRef] [PubMed]
- Ridgers, N.D.; Timperio, A.; Cerin, E.; Salmon, J.O. Compensation of Physical Activity and Sedentary Time in Primary School Children. Med. Sci. Sports Exerc. 2014, 46, 1564–1569. [Google Scholar] [CrossRef] [PubMed]
- Kriemler, S.; Meyer, U.; Martin, E.; Sluijs, E.M.; Andersen, L.B.; Martin, B.W. Effect of school-based interventions on physical activity and fitness in children and adolescents: A review of reviews and systematic update. Br. J. Sports Med. 2011, 45, 923–930. [Google Scholar] [CrossRef] [PubMed]
- Naylor, P.J.; Macdonald, H.M.; Warburton, D.E.R.; Reed, K.E.; McKay, H.A. An active school model to promote physical activity in elementary schools: Action schools! BC. Br. J. Sports Med. 2008, 42, 338–343. [Google Scholar] [CrossRef] [PubMed]
- Noonan, R.J.; Boddy, L.M.; Fairclough, S.J.; Knowles, Z.R. Parental perceptions on childrens out-of-school physical activity and family-based physical activity. Early Child Dev. Care 2017, 187, 1909–1924. [Google Scholar] [CrossRef]
- Solomon-Moore, E.; Matthews, J.; Reid, T.; Toumpakari, Z.; Sebire, S.J.; Thompson, J.L.; Lawlor, D.A.; Jago, R. Examining the challenges posed to parents by the contemporary screen environments of children: A qualitative investigation. BMC Pediatr. 2018, 18, 129. [Google Scholar] [CrossRef] [PubMed]
- Craig, P.; Dieppe, P.; Macintyre, S.; Michie, S.; Nazareth, I.; Petticrew, M. Developing and evaluating complex interventions: The new Medical Research Council guidance. BMJ 2008, 337, a1655. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Freedson, P.; Bowles, H.R.; Troiano, R.; Haskell, W. Assessment of physical activity using wearable monitors: Recommendations for monitor calibration and use in the field. Med. Sci. Sports Exerc. 2012, 44 (Suppl. 1), S1–S4. [Google Scholar] [CrossRef] [PubMed]
- Peach, D.; Van Hoomissen, J.; Callender, H.L. Exploring the ActiLife((R)) filtration algorithm: Converting raw acceleration data to counts. Physiol. Meas. 2014, 35, 2359–2367. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Intervention Component | Content Description | Phase 2 Findings | Associated/Supportive Research | Conceptual Model/Theory | Duration | Frequency |
|---|---|---|---|---|---|---|
| Active Breaks | Twenty-three activity cards were created with pictures on the front demonstrating the activity and instructions on the back. All activities were designed for use within the restricted space of a classroom. Each activity card was designed to last for 30 s. (Delivery: class teacher) | Deemed feasible and acceptable. No changes needed. | Pilot primary school AB study with a similar 5-min implementation protocol [32]. ABs reported to improve PA during school [33]. | SE YPAPM TEO | 5 min. | x1/day. |
| Bounce at the bell | Teachers were provided with a suggested jump routine (star jumps, tuck jumps) to perform whenever the bell sounded in class (usually for morning break, lunch break and the end of the school day). The jumps were to be performed once the lesson had finished just before leaving the classroom. (Delivery: class teacher) | N/A | Used in a PA school-based intervention for increasing bone strength (no PA outcomes) [34]. Reported as a simple classroom-based exercise without the need for equipment or access to a gym, requiring only 3 min of the school day [35]. | SE YPAPM TEO | 1–2 min. | x3/day. |
| Born To Move videos | Videos provided by Les Mills (free access videos available on http://www.lesmillsondemand.com), included instructor led high-intensity motor skills set to contemporary music, designed to improve health-related and skill-related fitness. Videos required hall/gym space with a projector screen connected to an internet enabled device. (Delivery: class teacher) | Daily implementation reduced due to hall/gym accessibility barrier. | Evaluation of BTM pilot programme concluded that live 30-min BTM lessons delivered by a trained instructor engaged children in significantly more MPA than during regular PE [36]. | SE YPAPM TEO | 10 min. | x2/week. |
| Daily Mile or 100 Mile Club | Schools planned an outdoor route around school grounds. If the route was smaller than a mile, the number of laps required to achieve the mile was calculated. For the 100 MC, each child received a recording sheet to record miles accumulated. For the DM option, no tracking of distance ran was required. (Delivery: class teacher) | N/A | Short-term follow up results of a study implementing 100 MC in lower-income schoolchildren indicated significant positive effect on ST [37]. The DM is cited by the UK government as an option for schools to deliver PA [10]. | SE YPAPM TEO | 15 min. | x1/day (DM). x3/week (100 MC). |
| Playground activity challenge cards | There were 5 games in total which all included 5 different activity cards. Activities were easy-to-perform exercises designed for children to follow independently without the need for any equipment (apart from a ball in one of the games) or the need for teachers to set up or assist with games. They were placed around the playground in visible places (tied to gates/faces, stuck to classroom windows). (Delivery: child independent/playground staff) | Challenges/games designed for children to follow independently due to teacher barriers cited. | SE YPAPM TEO | 5 min per game. | Every recess break. | |
| PE teacher training | The school sport coach or PE teacher in each intervention school were sent access to an online training session (immediately after intervention allocation, the week prior to the intervention period). The focus of the online content was how to increase high intensity PA and reduce time spent standing still during PE. Access to follow-up support via email was provided. (Delivery: PE teacher) | Supportive, Active (high levels of PA, minimal transition time), Autonomous (opportunity for student choice), Fair, Enjoyable (SAAFE) framework used to guide staff for the planning and delivery of their PE lessons [38]. LET US Play principles also highlighted to staff [39]. Including removing lines, eliminating elimination, reducing team sizes and rethinking space, equipment and rules. | SE YPAPM TEO | N/A | Every PE lesson. | |
| Newsletters | Information relating to PA and its importance for health and wellbeing were sent to schools. Schools were asked to insert messages into their school newsletter which was sent home to all parents (most commonly online via an email or through the school website). | N/A | Use in previous school-based PA interventions as a means for engaging parents [40,41,42]. | SE YPAPM | Weekly/2 weeks (school dependent). | |
| Activity homework | Children received a homework pack which included a letter to parents and 10 different PA challenges. A separate pack of the individual challenges on small pieces of paper were also provided for children to take home if their original pack had been lost at home. Children received a weekly diary to complete whenever they had done PA at home. A blank class chart was provided to populate with names and update every week with school rewards for those who completed the most PA at home. | N/A | Use in previous school-based PA interventions [43,44]. | SE YPAPM TEO | Encouraged to be x1/day. |
| Baseline | Follow Up | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Measure | Sex | n | Control | n | Intervention | n | Control | n | Intervention |
| Stature (cm) | Boy | 54 | 137.5 (7.2) | 60 | 136.9 (5.1) | 52 | 138.6 (7.2) | 56 | 137.7 (4.9) |
| Girl | 60 | 136.7 (6.7) | 58 | 137.8 (6.0) | 58 | 137.5 (6.5) | 54 | 139.0 (6.2) | |
| All | 114 | 137.1 (6.9) | 118 | 137.3 (5.5) | 110 | 138.0 (6.8) | 110 | 138.3 (5.6) | |
| Body mass (kg) | Boy | 54 | 34.9 (8.8) | 59 | 33.7 (6.3) | 52 | 35.9 (8.8) | 55 | 34.0 (6.3) |
| Girl | 60 | 35.2 (8.5) | 58 | 37.1 (8.1) | 56 | 35.7 (9.1) | 54 | 38.0 (8.5) | |
| All | 114 | 35.1 (8.6) | 117 | 35.4 (7.4) | 108 | 35.8 (8.9) | 109 | 36.0 (7.7) | |
| BMI (kg·m2) | Boy | 54 | 18.3 (3.2) | 59 | 17.9 (2.6) | 52 | 18.5 (3.2) | 55 | 17.8 (2.6) |
| Girl | 60 | 18.7 (3.5) | 58 | 19.5 (3.6) | 56 | 18.7 (3.7) | 54 | 19.6 (3.6) | |
| All | 114 | 18.5 (3.3) | 117 | 18.6 (3.2) | 108 | 18.6 (3.5) | 109 | 18.7 (3.3) | |
| BMI z-score | Boy | 53 | 0.7 (1.2) | 56 | 0.5 (1.1) | 51 | 0.7 (1.1) | 53 | 0.5 (1.0) |
| Girl | 60 | 0.7 (1.3) | 57 | 0.9 (1.2) | 56 | 0.5 (1.2) | 53 | 0.9 (1.2) | |
| All | 113 | 0.7 (1.2) | 113 | 0.7 (1.2) | 107 | 0.6 (1.2) | 106 | 0.7 (1.2) | |
| Overweight/Obese (%) | Boy | 53 | 22.6 | 56 | 21.4 | 51 | 25.5 | 53 | 18.9 |
| Girl | 60 | 35.0 | 57 | 43.9 | 56 | 35.7 | 53 | 47.1 | |
| All | 113 | 29.2 | 113 | 32.7 | 107 | 30.8 | 106 | 33.0 | |
| Waist circumference (cm) | Boy | 54 | 63.7 (9.5) | 59 | 63.5 (7.8) | 52 | 66.7 (9.1) | 55 | 63.8 (6.7) |
| Girl | 60 | 63.7 (9.4) | 58 | 65.9 (8.8) | 56 | 65.1 (10.1) | 54 | 66.1 (8.5) | |
| All | 114 | 63.7 (9.4) | 117 | 64.7 (8.3) | 108 | 65.9 (9.6) | 109 | 64.9 (7.7) | |
| Maturity offset (y) | Boy | 51 | −3.2 (0.3) | 57 | −3.3 (0.2) | 51 | −3.0 (0.4) | 54 | −3.0 (0.3) |
| Girl | 60 | −2.2 (0.4) | 57 | −2.1 (0.3) | 57 | −1.8 (0.5) | 53 | −1.8 (0.5) | |
| All | 111 | −2.7 (0.7) | 114 | −2.7 (0.6) | 108 | −2.3 (0.7) | 107 | −2.4 (0.7) | |
| CRF (Number of shuttles) | Boy | 52 | 36.7 (18.3) | 59 | 33.1 (15.2) | 50 | 34.1 (18.9) | 57 | 36.2 (17.6) |
| Girl | 58 | 28.2 (13.3) | 55 | 25.1 (11.4) | 57 | 25.3 (12.5) | 54 | 25.2 (11.6) | |
| All | 110 | 32.3 (16.3) | 114 | 29.2 (14.0) | 107 | 29.4 (16.3) | 111 | 30.9 (15.9) | |
| IMD Rank | Boy | 51 | 5618.8 (5324.0) | 59 | 6379.4 (7995.8) | N/A | N/A | ||
| Girl | 58 | 5811.1 (6396.3) | 56 | 8322.6 (8497.7) | N/A | N/A | |||
| All | 109 | 5721.1 (5892.7) | 115 | 7325.7 (8265.5) | N/A | N/A | |||
| Crude Model a | Adjusted Model b | |||||
|---|---|---|---|---|---|---|
| Outcome Measure | β or OR | 95% CI | p | β or OR | 95% CI | p |
| School day ST | 10.1 c | −17.8 to −2.4 | 0.01 | −9.0 c | −17.7 to −0.2 | 0.04 |
| School day LPA | 4.2 c | −1.1 to 9.4 | 0.1 | 3.5 c | −1.9 to 8.9 | 0.2 |
| School day total PA | 7.1 c | −1.1 to 15.2 | 0.1 | 5.4 c | −2.0 to 12.8 | 0.2 |
| School day MVPA | 1.9 c | 1.8 to 2.1 | 0.5 | 1.5 c | −4.0 to 7.0 | 0.6 |
| 30 min MVPA/school day | 2.73 d | 0.36 to 2.20 | 0.03 | 2.79 d | 0.49 to 2.71 | 0.07 |
| Whole day ST | −0.2 c | −23.4 to 22.9 | 1.0 | −2.7 c | −25.1 to 19.7 | 0.8 |
| Whole weekday LPA | −2.7 c | −14.2 to 8.8 | 0.9 | −8.8 c | −20.3 to 2.7 | 0.1 |
| Whole weekday total PA | −2.5 c | −19.7 to 14.7 | 0.8 | −12.3 c | −30.2 to 5.7 | 0.2 |
| Whole weekday MVPA | −0.9 c | −10.5 to 8.7 | 0.7 | −4.1 c | −13.9 to 5.7 | 0.4 |
| CRF | 4.9 c | 0.8 to 8.9 | 0.02 | 3.7 c | −0.1 to 7.6 | 0.06 |
| BMI z-score | 0.0 c | −0.2 to 0.2 | 0.8 | 0.0 c | −0.2 to 0.2 | 1.0 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Taylor, S.L.; Noonan, R.J.; Knowles, Z.R.; Owen, M.B.; McGrane, B.; Curry, W.B.; Fairclough, S.J. Evaluation of a Pilot School-Based Physical Activity Clustered Randomised Controlled Trial—Active Schools: Skelmersdale. Int. J. Environ. Res. Public Health 2018, 15, 1011. https://doi.org/10.3390/ijerph15051011
Taylor SL, Noonan RJ, Knowles ZR, Owen MB, McGrane B, Curry WB, Fairclough SJ. Evaluation of a Pilot School-Based Physical Activity Clustered Randomised Controlled Trial—Active Schools: Skelmersdale. International Journal of Environmental Research and Public Health. 2018; 15(5):1011. https://doi.org/10.3390/ijerph15051011
Chicago/Turabian StyleTaylor, Sarah L., Robert J. Noonan, Zoe R. Knowles, Michael B. Owen, Bronagh McGrane, Whitney B. Curry, and Stuart J. Fairclough. 2018. "Evaluation of a Pilot School-Based Physical Activity Clustered Randomised Controlled Trial—Active Schools: Skelmersdale" International Journal of Environmental Research and Public Health 15, no. 5: 1011. https://doi.org/10.3390/ijerph15051011
APA StyleTaylor, S. L., Noonan, R. J., Knowles, Z. R., Owen, M. B., McGrane, B., Curry, W. B., & Fairclough, S. J. (2018). Evaluation of a Pilot School-Based Physical Activity Clustered Randomised Controlled Trial—Active Schools: Skelmersdale. International Journal of Environmental Research and Public Health, 15(5), 1011. https://doi.org/10.3390/ijerph15051011