Furthering the Evidence of the Effectiveness of Employment Strategies for People with Mental Disorders in Europe: A Systematic Review

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Selection Criteria
- (a)
- were published between January 2011 and April 2016;
- (b)
- were published in English;
- (c)
- were intervention studies—namely, randomized trials, nonrandomized controlled trials, noncontrolled pre-post intervention studies;
- (d)
- were observational studies—namely, cohort studies, case–control studies, cross-sectional studies, descriptive longitudinal studies;
- (e)
- were qualitative studies or mixed-methods studies (for present study only);
- (f)
- were carried out in the 28 countries of the European Union, in Norway, Lichtenstein, Iceland, or Switzerland, or in non-European countries with western lifestyle: Canada, United States of America, Australia;
- (g)
- reported on effectiveness regarding at least one of the following work outcomes:
- (1)
- employment status (employed/unemployed);
- (2)
- return to work;
- (3)
- absenteeism (sick leave);
- (4)
- maintaining a job;
- (5)
- obtaining a job;
- (h)
- investigated variables potentially affecting effectiveness (e.g., views and experiences of involved persons with a given strategy).
- (a)
- PwCDs in general (i.e., specific conditions are not further specified in the studies or results for different conditions are reported together) and persons with disabilities in general;
- (b)
- the following disease groups: mental disorders, musculoskeletal disorders, and cancer, neurological, metabolic, respiratory, and cardiovascular diseases;
- (c)
- the following specific diseases: depression, back and neck pain, migraine, diabetes mellitus, chronic obstructive pulmonary disease, and ischemic heart disease.
- (a)
- included participants with mainly other chronic diseases than the ones defined above;
- (b)
- included participants aged <16 or >65 years;
- (c)
- were case report/case series, psychometric studies, letters, comments, editorials, overviews without empirical primary or secondary data, reviews (systematic and nonsystematic reviews, health technology assessments) and meta-analyses, protocols, studies reporting exclusively on design or baseline data;
- (d)
- considered no effectiveness outcomes—for example, studies reporting only on costs resulting from the implementation of strategies—nor variables potentially affecting effectiveness;
- (e)
- did not focus on a concrete strategy or group of strategies, for example, studies focusing on factors facilitating return to work after sick leave in general;
- (f)
- were published in languages other than English;
- (g)
- were published before 2011;
- (h)
- had no abstract available.
2.2. Study Selection and Data Extraction
2.3. Study Quality Assessment
- −
- Yes. Yes was selected if estimates for relevant work outcomes had an adequate p-value, usually <0.05, or if the confidence interval for the estimate excluded the no-effect value (e.g., the value 1 was not included in the confidence interval of reported odds ratio);
- −
- Unclear. Unclear was selected if the precision of the effect estimate was not reported, or if results were inconsistent or difficult to interpret (e.g., statistically nonsignificant but large estimates in subgroup analyses);
- −
- No. No was selected if data did not support the presence of an effect of the intervention on relevant work outcomes.
3. Results
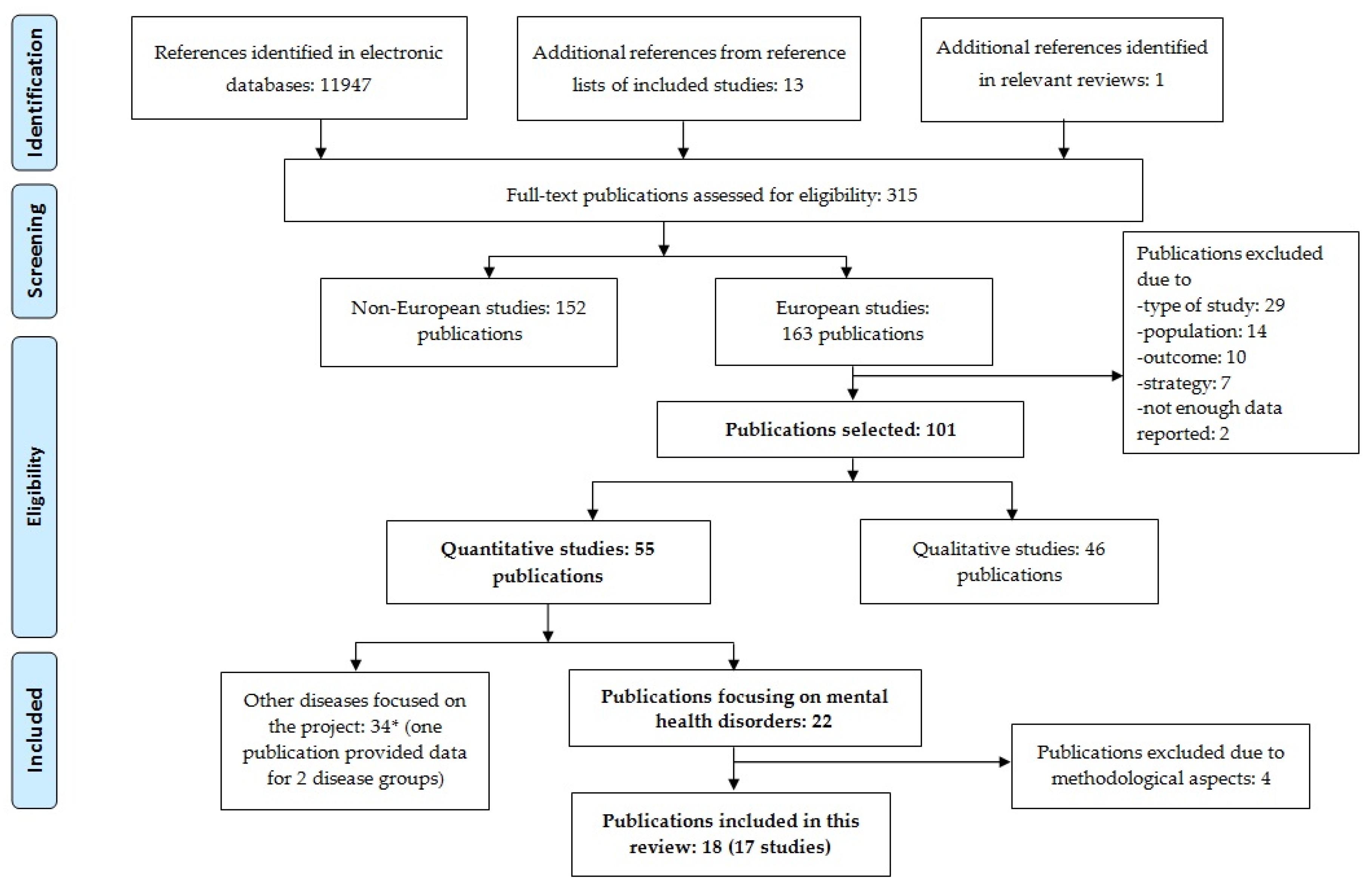
3.1. Literature Search
3.2. Study Characteristics
3.3. Intervention Analyses
3.3.1. Job Access Programs
3.3.2. RTW Programs
3.3.3. Mixed Programs (Job Access and RTW)
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Vigo, D.; Thornicroft, G.; Atun, R. Estimating the true global burden of mental illness. Lancet Psychiatry 2016, 3, 171–178. [Google Scholar] [CrossRef]
- Murray, C.J.L.; Vos, T.; Lozano, R.; Naghavi, M.; Flaxman, A.D.; Michaud, C.; Ezzati, M.; Shibuya, K.; Salomon, J.A.; Abdalla, S.; et al. Disability-adjusted life years (DALYs) for 291 diseases and injuries in 21 regions, 1990–2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2197–2223. [Google Scholar] [CrossRef]
- Mathers, C.; Stevens, G.; Ho, J.; Fat, D.M.; Mahanani, W.R.; Andreev, K.; Bassani, D.; Black, B.; Boerma, T.; Boucher, P.; et al. WHO Methods and Data Sources for Global Burden of Disease Estimates 2000–2011; WHO, Department of Health Statistics and Information Systems: Geneva, Switzerland, 2013. [Google Scholar]
- World Health Organization (WHO). The European Mental Health Action Plan 2013–2020; WHO: Copenhagen, Denmark, 2015. [Google Scholar]
- Burns, J.K. Poverty, inequality and a political economy of mental health. Epidemiol. Psychiatr. Sci. 2015, 24, 107–113. [Google Scholar] [CrossRef] [PubMed]
- Hert, M.; Correll, C.U.; Bobes, J.; Cetkovich-Bakmas, M.; Cohen, D.; Asai, I.; Detraux, J.; Gautam, S.; Möller, H.-J.; Ndetei, D.M.; et al. Physical illness in patients with severe mental disorders. I. Prevalence, impact of medications and disparities in health care. World Psychiatry 2011, 10, 52–77. [Google Scholar] [CrossRef]
- Scott, D.; Happell, B. The high prevalence of poor physical health and unhealthy lifestyle behaviours in individuals with severe mental illness. Issues Ment. Health Nurs. 2011, 32, 589–597. [Google Scholar] [CrossRef] [PubMed]
- Vreeland, B. Bridging the gap between mental and physical health: A multidisciplinary approach. J. Clin. Psychiatry 2007, 68, 26–33. [Google Scholar] [CrossRef] [PubMed]
- Sobocki, P.; Jönsson, B.; Angst, J.; Rehnberg, C. Cost of depression in Europe. J. Ment. Health Policy Econ. 2006, 9, 87–98. [Google Scholar] [PubMed]
- Dupré, D. Work-Related Health Problems in the EU 1998–1999; Eurostat: Luxembourg, 2001. [Google Scholar]
- Alonso, J.; Angermeyer, M.C.; Bernert, S.; Bruffaerts, R.; Brugha, T.S.; Bryson, H.; Girolamo, G.; Graaf, R.; Demyttenaere, K.; Gasquet, I.; et al. Prevalence of mental disorders in Europe: Results from the European study of the epidemiology of mental disorders (ESEMeD) project. Acta Psychiatr. Scand. 2004, 109, 21–27. [Google Scholar] [CrossRef] [PubMed]
- Haro, J.M.; Ayuso-Mateos, J.L.; Bitter, I.; Demotes-Mainard, J.; Leboyer, M.; Lewis, S.W.; Linszen, D.; Maj, M.; Mcdaid, D.; Meyer-Lindenberg, A.; et al. ROAMER: Roadmap for mental health research in Europe. Int. J. Methods Psychiatr. Res. 2014, 23, 1–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Corral, A.; Duran, J.; Isusi, I. Employment Opportunities for People with Chronic Diseases; European Foundation for the Improvement of Living and Working Conditions (Eurofound): Dublin, Ireland, 2014. [Google Scholar]
- Eurostat. Employment of Disabled People. Statistical Analysis of the 2011 Labour Force Survey Ad Hoc Module; Publications Office of the European Union: Luxembourg, 2015. [Google Scholar]
- Stewart, W.F.; Ricci, J.A.; Chee, E.; Hahn, S.R.; Morganstein, D. Cost of lost productive work time among US workers with depression. JAMA 2003, 289, 3135–3144. [Google Scholar] [CrossRef] [PubMed]
- Corrigan, P.W.; Watson, A.C. Understanding the impact of stigma on people with mental illness. World Psychiatry 2002, 1, 16–20. [Google Scholar] [PubMed]
- Alonso, J.; Buron, A.; Rojas-Farreras, S.; de Graaf, R.; Haro, J.M.; de Girolamo, G.; Bruffaerts, R.; Kovess, V.; Matschinger, H.; et al. Perceived stigma among individuals with common mental disorders. J. Affect. Disord. 2009, 118, 180–186. [Google Scholar] [CrossRef] [PubMed]
- Vandekinderen, C.; Roets, G.; Vandenbroeck, M.; Vanderplasschen, W.; Van Hove, G. One size fits all? The social construction of dis-employ-abled women. Disabil. Soc. 2012, 27, 703–716. [Google Scholar] [CrossRef]
- Lewis, R.; Dobbs, L.; Biddle, P. “If this wasn’t here I probably wouldn’t be’: Disabled workers’ views of employment support. Disabil. Soc. 2013, 28, 1089–1103. [Google Scholar] [CrossRef]
- Lerner, D.; Adler, D.A.; Rogers, W.H.; Chang, H.; Lapitsky, L.; McLaughlin, T.; Reed, J. Work performance of employees with depression: The impact of work stressors. Am. J. Health Promot. 2010, 24, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Scheid, T.L. Stigma as a barrier to employment: Mental disability and the Americans with disabilities act. Int. J. Law Psychiatry 2005, 28, 670–690. [Google Scholar] [CrossRef] [PubMed]
- Lerner, D.; Adler, D.A.; Chang, H.; Berndt, E.R.; Irish, J.T.; Lapitsky, L.; Hood, M.Y.; Reed, J.; Rogers, W.H. The clinical and occupational correlates of work productivity loss among employed patients with depression. J. Occup. Environ. Med. 2004, 46, S46–S55. [Google Scholar] [CrossRef] [PubMed]
- Henderson, M.; Harvey, S.B.; Overland, S.; Mykletun, A.; Hotopf, M. Work and common psychiatric disorders. J. R. Soc. Med. 2011, 104, 198–207. [Google Scholar] [CrossRef] [PubMed]
- Spurgeon, P. New Directions in Managing Employee Absence: An Evidence-Based Approach; Chartered Institute of Personnel and Development: London, UK, 2007. [Google Scholar]
- Department for Work and Pensions. Pathways to Work: Helping People into Employment the Government’s Response and Action Plan; The Stationery Office: London, UK, 2003.
- Black, C.; Frost, D. Health at Work—An Independent Review of Sickness Absence; The Stationery Office: London, UK, 2011. [Google Scholar]
- Waddell, G.; Burton, A.K. Is Work Good for Your Health And Well-Being? The Stationery Office: London, UK, 2006. [Google Scholar]
- Council on Accreditation. Vocational Rehabilitation Services; Council on Accreditation: New York NY, USA, 2018. [Google Scholar]
- Mcdonald, R. APSE Ethical Guidelines for Professionals in Supported Employment; APSE: Rockville, MD, USA, 1998. [Google Scholar]
- Catty, J.; Lissouba, P.; White, S.; Becker, T.; Drake, R.E.; Fioritti, A.; Knapp, M.; Lauber, C.; Rössler, W.; Tomov, T.; et al. EQOLISE group predictors of employment for people with severe mental illness: Results of an international six-centre randomised controlled trial. Br. J. Psychiatry 2008, 192, 224–231. [Google Scholar] [CrossRef] [PubMed]
- Bond, G.R.; Drake, R.E.; Becker, D.R. An update on randomized controlled trials of evidence-based supported employment. Psychiatr. Rehabil. J. 2008, 31, 280–290. [Google Scholar] [CrossRef] [PubMed]
- Germundsson, P.; Gustafsson, J.; Lind, M.; Danermark, B. Disability and supported employment: Impact on employment, income, and allowances. Int. J. Rehabil. Res. 2012, 35, 263–269. [Google Scholar] [CrossRef] [PubMed]
- Grove, B. International employment schemes for people with mental health problems. Br. J. Psych. Int. 2015, 12, 97–99. [Google Scholar] [CrossRef]
- Marshall, M.; Crowther, R.; Almaraz-Serrano, A.; Creed, F.; Sledge, W.; Kluiter, H.; Roberts, C.; Hill, E.; Wiersma, D.; Bond, G.R.; et al. Systematic reviews of the effectiveness of day care for people with severe mental disorders: (1) acute day hospital versus admission; (2) vocational rehabilitation; (3) day hospital versus outpatient care. Health Technol. Assess. 2001, 5, 1–75. [Google Scholar] [CrossRef] [PubMed]
- Perkins, D.V.; Raines, J.A.; Tschopp, M.K.; Warner, T.C. Gainful Employment Reduces Stigma toward People Recovering from Schizophrenia. Community Ment. Health J. 2009, 45, 158–162. [Google Scholar] [CrossRef] [PubMed]
- Funk, M. Mental Health and Work: Impact, Issues and Good Practices; WHO: Geneva, Switzerland, 2000. [Google Scholar]
- Khalifa, N.; Talbot, E.; Schneider, J.; Walker, D.M.; Bates, P.; Bird, Y.; Davies, D.; Brookes, C.; Hall, J.; Völlm, B. Individual placement and support (IPS) for patients with offending histories: The IPSOH feasibility cluster randomised trial protocol. BMJ Open 2016, 6, e012710. [Google Scholar] [CrossRef] [PubMed]
- Bond, G.R.; Drake, R.E.; Becker, D.R. Generalizability of the Individual Placement and Support (IPS) model of supported employment outside the US. World Psychiatry 2012, 11, 32–39. [Google Scholar] [CrossRef] [PubMed]
- Kinoshita, Y.; Furukawa, T.A.; Kinoshita, K.; Honyashiki, M.; Omori, I.M.; Marshall, M.; Bond, G.R.; Huxley, P.; Amano, N.; Kingdon, D. Supported employment for adults with severe mental illness. Cochrane Database Syst. Rev. 2013, CD008297. [Google Scholar] [CrossRef] [PubMed]
- Crowther, R.; Marshall, M.; Bond, G.R.; Huxley, P. Vocational rehabilitation for people with severe mental illness. Cochrane Database Syst. Rev. 2001, CD003080. [Google Scholar] [CrossRef] [PubMed]
- Modini, M.; Tan, L.; Brinchmann, B.; Wang, M.-J.; Killackey, E.; Glozier, N.; Mykletun, A.; Harvey, S.B. Supported employment for people with severe mental illness: Systematic review and meta-analysis of the international evidence. Br. J. Psychiatry 2016, 209, 14–22. [Google Scholar] [CrossRef] [PubMed]
- European Commission. Horizon 2020 Work Programme 2018-2020. 19 General Annexes. Decision C(2017)7124 of 27 October 2017; European Comission: Brussels, Belgium; Luxembourg, 2017. [Google Scholar]
- Scaratti, C.; Leonardi, M.; Silvaggi, F.; Ávila, C.; Muñoz-Murillo, A.; Stavroussi, P.; Roka, O.; Burger, H.; Fheodoroff, K.; Tobiasz-Adamczyk, B.; et al. Mapping european welfare models: State of the art of strategies for professional integration and reintegration of persons with chronic diseases. Int. J. Environ. Res. Public Health 2018, 15, 781. [Google Scholar] [CrossRef] [PubMed]
- Sabariego, C.; Coenen, M.; Ito, E.; Fheodoroff, K.; Scaratti, C.; Leonardi, M.; Vlachou, A.; Stavroussi, P.; Brecelj, V.; Kovačič, D.; et al. Effectiveness of integration and re-integration into work strategies for persons with chronic conditions: A systematic review of European strategies. Int. J. Environ. Res. Public Health 2018, 15, 552. [Google Scholar] [CrossRef]
- Esteban, E.; Coenen, M.; Ito, E.; Gruber, S.; Scaratti, C.; Leonardi, M.; Roka, O.; Vasilou, E.; Muñoz-Murillo, A.; Ávila, C.C.; et al. Views and experiences of persons with chronic diseases about strategies that aim to integrate and re-integrate them into work: A systematic review of qualitative studies. Int. J. Environ. Res. Public Health 2018. under review. [Google Scholar]
- Higgins, J.P.T.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions|Cochrane Training; Higgins, J.P.T., Green, S., Eds.; John Wiley and Sons: New York, NY, USA, 2011. [Google Scholar]
- Clayton, S.; Bambra, C.; Gosling, R.; Povall, S.; Misso, K.; Whitehead, M. Assembling the evidence jigsaw: Insights from a systematic review of UK studies of individual-focused return to work initiatives for disabled and long-term ill people. BMC Public Health 2011, 11, 170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alderson, P.; Tan, T. The use of Cochrane Reviews in NICE clinical guidelines. In Cochrane Database of Systematic Reviews; Tovey, D., Ed.; John Wiley and Sons, Ltd.: Chichester, UK, 2011. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. PRISMA group preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Van Veggel, R.; Waghorn, G.; Dias, S. Implementing evidence-based supported employment in Sussex for people with severe mental illness. Br. J. Occup. Ther. 2015, 78, 286–294. [Google Scholar] [CrossRef]
- Andrén, D. Does part-time sick leave help individuals with mental disorders recover lost work capacity? J. Occup. Rehabil. 2014, 24, 344–360. [Google Scholar] [CrossRef] [PubMed]
- Kröger, C.; Bode, K.; Wunsch, E.-M.; Kliem, S.; Grocholewski, A.; Finger, F. Work-related treatment for major depressive disorder and incapacity to work: Preliminary findings of a controlled, matched study. J. Occup. Health Psychol. 2015, 20, 248–258. [Google Scholar] [CrossRef] [PubMed]
- Lagerveld, S.E.; Blonk, R.W.B.; Brenninkmeijer, V.; Wijngaards-de Meij, L.; Schaufeli, W.B. Work-focused treatment of common mental disorders and return to work: A comparative outcome study. J. Occup. Health Psychol. 2012, 17, 220–234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martin, M.H.T.; Nielsen, M.B.D.; Madsen, I.E.H.; Petersen, S.M.A.; Lange, T.; Rugulies, R. Effectiveness of a coordinated and tailored return-to-work intervention for sickness absence beneficiaries with mental health problems. J. Occup. Rehabil. 2013, 23, 621–630. [Google Scholar] [CrossRef] [PubMed]
- Arends, I.; van der Klink, J.J.L.; van Rhenen, W.; de Boer, M.R.; Bültmann, U. Prevention of recurrent sickness absence in workers with common mental disorders: Results of a cluster-randomised controlled trial. Occup. Environ. Med. 2014, 71, 21–29. [Google Scholar] [CrossRef] [PubMed]
- Bejerholm, U.; Areberg, C.; Hofgren, C.; Sandlund, M.; Rinaldi, M. Individual placement and support in Sweden—A randomized controlled trial. Nord. J. Psychiatry 2015, 69, 57–66. [Google Scholar] [CrossRef] [PubMed]
- Hees, H.L.; de Vries, G.; Koeter, M.W.J.; Schene, A.H. Adjuvant occupational therapy improves long-term depression recovery and return-to-work in good health in sick-listed employees with major depression: Results of a randomised controlled trial. Occup. Environ. Med. 2013, 70, 252–260. [Google Scholar] [CrossRef] [PubMed]
- Heslin, M.; Howard, L.; Leese, M.; McCrone, P.; Rice, C.; Jarrett, M.; Spokes, T.; Huxley, P.; Thornicroft, G. Randomized controlled trial of supported employment in England: 2 year follow-up of the supported work and needs (SWAN) study. World Psychiatry 2011, 10, 132–137. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, H.; Jäckel, D.; Glauser, S.; Kupper, Z. A randomised controlled trial of the efficacy of supported employment. Acta Psychiatr. Scand. 2012, 125, 157–167. [Google Scholar] [CrossRef] [PubMed]
- Michon, H.; van Busschbach, J.T.; Stant, A.D.; van Vugt, M.D.; van Weeghel, J.; Kroon, H. Effectiveness of individual placement and support for people with severe mental illness in the Netherlands: A 30-month randomized controlled trial. Psychiatr. Rehabil. J. 2014, 37, 129–136. [Google Scholar] [CrossRef] [PubMed]
- Noordik, E.; van der Klink, J.J.; Geskus, R.B.; de Boer, M.R.; van Dijk, F.J.; Nieuwenhuijsen, K. Effectiveness of an exposure-based return-to-work program for workers on sick leave due to common mental disorders: A cluster-randomized controlled trial. Scand. J. Work. Environ. Health 2013, 39, 144–154. [Google Scholar] [CrossRef] [PubMed]
- Reme, S.E.; Grasdal, A.L.; Løvvik, C.; Lie, S.A.; Øverland, S. Work-focused cognitive-behavioural therapy and individual job support to increase work participation in common mental disorders: A randomised controlled multicentre trial. Occup. Environ. Med. 2015, 72, 745–752. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vlasveld, M.C.; van der Feltz-Cornelis, C.M.; Adèr, H.J.; Anema, J.R.; Hoedeman, R.; van Mechelen, W.; Beekman, A.T.F. Collaborative care for sick-listed workers with major depressive disorder: A randomised controlled trial from the Netherlands depression initiative aimed at return to work and depressive symptoms. Occup. Environ. Med. 2013, 70, 223–230. [Google Scholar] [CrossRef] [PubMed]
- Volker, D.; Zijlstra-Vlasveld, M.C.; Anema, J.R.; Beekman, A.T.; Brouwers, E.P.; Emons, W.H.; van Lomwel, A.G.C.; van der Feltz-Cornelis, C.M. Effectiveness of a blended web-based intervention on return to work for sick-listed employees with common mental disorders: Results of a cluster randomized controlled trial. J. Med. Internet Res. 2015, 17, e116. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, H.; Jäckel, D.; Glauser, S.; Mueser, K.T.; Kupper, Z. Long-term effectiveness of supported employment: 5-year follow-up of a randomized controlled trial. Am. J. Psychiatry 2014, 171, 1183–1190. [Google Scholar] [CrossRef] [PubMed]
- Høgelund, J.; Holm, A.; Eplov, L.F. The effect of part-time sick leave for employees with mental disorders. J. Ment. Health Policy Econ. 2012, 15, 157–170. [Google Scholar] [PubMed]
- Bond, G.R.; Drake, R.E. Making the case for IPS supported employment. Adm. Policy Ment. Health Ment. Health Serv. Res. 2014, 41, 69–73. [Google Scholar] [CrossRef] [PubMed]
- Swanson, S.J.; Courtney, C.T.; Meyer, R.H.; Reeder, S.A. Strategies for integrated employment and mental health services. Psychiatr. Rehabil. J. 2014, 37, 86–89. [Google Scholar] [CrossRef] [PubMed]
- Corbière, M.; Shen, J. A Systematic review of psychological return-to-work interventions for people with mental health problems and/or physical injuries. Can. J. Community Ment. Health 2006, 25, 261–288. [Google Scholar] [CrossRef]
- Steffick, D.E.; Fortney, J.C.; Smith, J.L.; Pyne, J.M. Worksite disease management programs for depression. Dis. Manag. Health Outcomes 2006, 14, 13–26. [Google Scholar] [CrossRef]
- Keller, M.B.; Lavori, P.W.; Friedman, B.; Nielsen, E.; Endicott, J.; McDonald-Scott, P.; Andreasen, N.C. The longitudinal interval follow-up evaluation. Arch. Gen. Psychiatry 1987, 44, 540–548. [Google Scholar] [CrossRef] [PubMed]
- Checkoway, H.; Pearce, N.; Kriebel, D. Selecting appropriate study designs to address specific research questions in occupational epidemiology. Occup. Environ. Med. 2007, 64, 633–638. [Google Scholar] [CrossRef] [PubMed]
- Nieuwenhuijsen, K.; Bültmann, U.; Neumeyer-Gromen, A.; Verhoeven, A.C.; Verbeek, J.H.; Feltz-Cornelis, C.M. Interventions to improve occupational health in depressed people. In Cochrane Database of Systematic Reviews; Nieuwenhuijsen, K., Ed.; John Wiley & Sons, Ltd.: Chichester, UK, 2008; p. CD006237. [Google Scholar]
- Secker, J.; Grove, B.; Seebohm, P. Challenging barriers to employment, training and education for mental health service users: The service user’s perspective. J. Ment. Health 2001, 10, 395–404. [Google Scholar] [CrossRef]
- Boardman, J.; Rinaldi, M. Difficulties in implementing supported employment for people with severe mental health problems. Br. J. Psychiatry 2013, 203, 247–249. [Google Scholar] [CrossRef] [PubMed]
- Kim, T.J.; von dem Knesebeck, O. Is an insecure job better for health than having no job at all? A systematic review of studies investigating the health-related risks of both job insecurity and unemployment. BMC Public Health 2015, 15, 985. [Google Scholar] [CrossRef] [PubMed]
- Ory, G.; Murphy, C.; Athanasou, J.A.; Murphy, G.C. The eVect of unemployment on mental health. J. Occup. Organ. Psychol. 1999, 72, 83–99. [Google Scholar]
- Linn, M.W.; Sandifer, R.; Stein, S. Effects of unemployment on mental and physical health. Am. J. Public Health 1985, 75, 502–506. [Google Scholar] [CrossRef] [PubMed]
- Shaw, W.; Hong, Q.; Pransky, G.; Loisel, P. A literature review describing the role of return-to-work coordinators in trial programs and interventions designed to prevent workplace disability. J. Occup. Rehabil. 2008, 18, 2–15. [Google Scholar] [CrossRef] [PubMed]
- Perkins, R.; Rinaldi, M. Unemployment rates among patients with long-term mental health problems. Psychiatr. Bull. 2002, 26, 295–298. [Google Scholar]
- Latimer, E.A.; Bush, P.W.; Becker, D.R.; Drake, R.E.; Bond, G.R. The cost of high-fidelity supported employment programs for people with severe mental illness. Psychiatr. Serv. 2004, 55, 401–406. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Authors, Year & Country | Name of Strategy | Type of Intervention Strategy | Employment Status Before Treatment | Sample (N, Mean Age, % Women) | Study Design | Study Period (Months) | Number of Follow-Up |
|---|---|---|---|---|---|---|---|
| Germundsson, P.; Gustafsson, J.; Lind, M.; Danermark, B. (2012) Sweden [32] | Vocational rehabilitation, according to the supported employment approach | Job access | Unemployed, not further described | N = 225 (46%) | Cohort | not clearly specified | 2 |
| Hogelund, J.; Holm, A.; Eplov, L. F. (2012) The Netherlands [66] | Part-time Sick Leave for Employees with Mental Disorders | RTW | Employed and on long-term sick leave | N = 226 (61%) | Cohort | 18 | 0 |
| van Veggel, R.; Waghorn, G. and Dias, S. (2015) UK [50] | Individual Placement and Support | Job access | Unemployed and seeking a job | N = 446 (39.6 years old, 44.7%) | Cohort | 12 | 1 |
| Andren, D. (2014) Sweden [51] | Part-time sick leave | RTW | Employed (open labor market) and on sick leave | Intervention groups (group 1: N = 548, 78%; group 2: N = 367, 73%; group 3: N = 172, 74%) Comparison groups (group 1: N = 79, 68%; group 2: N = 181, 66%; group 3: N = 155, 69%). | Cohort | Up to 12 | 12 |
| Kroger, C.; Bode, K.; Wunsch, E. M.; Kliem, S.; Grocholewski, A.; Finger, F. (2014) Germany [52] | Psychotherapy intervention | RTW Sickness absence | Employed and on sick leave | Intervention group: N = 13 (38%). Comparison group: N = 13 (54%). | CT | 12 | 1 |
| Lagerveld, S. E.; Blonk, R. W.; Brenninkmeijer, V.; Wijngaards-de Meij, L.; Schaufeli, W. B. (2012) The Netherlands [53] | Work-Focused Treatment of Common Mental Disorders and Return to Work | RTW | Employed (open labor market) and on sick leave | N = 168 (40.7 years old, 60%) Intervention group: N = 89 (40.2 years old) Comparison group: N = 79 (41.3 years old) | CT | 12 | 5 |
| Martin, M. H.; Nielsen, M. B.; Madsen, I. E.; Petersen, S. M.; Lange, T.; Rugulies, R. (2013) Denmark [54] | Multidisciplinary, coordinated and tailored RTW intervention | RTW | Mix—employed and unemployed, sick-listed for 4–12 weeks | N = 76 (42 years old, 82%) | CT | 3 | 1 |
| Arends, I.; van der Klink, J. J.; van Rhenen, W.; de Boer, M. R.; Bultmann, U. (2014) The Netherlands [55] | Stimulating Healthy participation And Relapse Prevention (SHARP)-at work intervention | RTW Sickness absence | Employed (open labor market) who had sickness absence in the past | N = 158 (42.3 years old, 58.8%) Intervention group: N = 80. Comparison group: N = 78 | RCT | 12 | 3 |
| Bejerholm, U.; Areberg, C.; Hofgren, C.; Sandlund, M.; Rinaldi, M. (2015) Sweden [56] | Individual Placement and Support | Job access | Unemployed and have a desire to work in the near future. | N = 120. Intervention group: N = 60 (53% females). Comparison group: N = 60 (35%) | RCT | 18 | 2 |
| Hees, H. L.; de Vries, G.; Koeter, M. W.; Schene, A. H. (2013) The Netherlands [57] | Occupational therapy, adjuvant to treatment as usual | RTW | Employed and on sick leave | N = 117 (42.6 years old) Intervention group: N = 39(47%) Comparison group: N = 78 (59%). | RCT | 18 | 3 |
| Heslin, M.; Howard, L.; Leese, M.; McCrone, P.; Rice, C.; Jarrett, M.; Spokes, T.; Huxley, P.; Thornicroft, G. (2011) UK [58] | Individual placement and support | Job access | Unemployed | N = 188 (not further described) | RCT | 24 | 2 |
| Hoffmann, Holger; Jäckel, Dorothea; Glauser, Sybille; Mueser, Kim T.; Kupper, Zeno (2012) Switzerland [59] | Supported employment | Job access | Not currently employed in the open market | Intervention group: N = 46 (33.5 years old), Comparison group: N = 54 (34.1 years old) | RCT | 24 | 2 |
| Hoffmann, H.; Jackel, D.; Glauser, S.; Kupper, Z. (2014) Switzerland [65] | Job Coach Project (Supported employment program) | Job access | Not currently employed in the open market | Intervention group: N = 46, Comparison group: N = 54 (33.5 years old, 35%) | RCT | 60 | 2 |
| Michon, H.; van Busschbach, J. T.; Stant, A. D.; van Vugt, M. D.; van Weeghel, J.; Kroon, H. (2014) The Netherlands [60] | Individual Placement and Support | Job access | Unemployed and seeking a job | Intervention group: N = 71 (34.1 years old, 27%) Comparison group: N = 80 (25%) | RCT | 30 | 3 |
| Noordik, E.; van der Klink, JJ.; Geskus, RB.; de Boer, MR.; van Dijk, FJ.; H. and Nieuwenhuijsen, K. (2013) The Netherlands [61] | Exposure-based return-to-work program for workers on sick leave due to common mental disorder | RTW | Employed (open labor market) and on sick leave | N = 160 (70.9%) Intervention group: N = 75 (44.9 years old) Comparison group: N = 85 (45.9 years old) | RCT | 12 | 1 |
| Reme, S. E.; Grasdal, A. L.; Lovvik, C.; Lie, S. A.; Overland, S. (2015) Norway [62] | AWaC (At Work and Coping) | Job status: RTW & Job access | Mix—people on and at risk of sick leave, and people on long-term benefits | Total sample: N = 1193 (40.4 years old). Intervention group: N = 437 (69.4%). Comparison group: N = 365 (65%) | RCT | 12 | 1 |
| Vlasveld, M. C.; van der Feltz-Cornelis, C. M.; Ader, H. J.; Anema, J. R.; Hoedeman, R.; van Mechelen, W.; Beekman, A. T. (2013) The Netherlands [63] | Collaborative care | RTW | Employed (open labor market) and on sick leave | Intervention group: N = 65 (41.9 years old) Comparison group: N = 51 (43.4 years old) | RCT | 12 | 4 |
| Volker, D., Zijlstra-Vlasveld, M. C., Anema, J. R., Beekman, A. T., Brouwers, E. P., Emons, W. H., van Lomwel, A. G. and van der Feltz-Cornelis, C. M. (2015) The Netherlands [64] | E-health module embedded in Collaborative Occupational health care | RTW | Employed (open labor market) and on sick leave | Intervention group: N = 131 (45.5 years old) Comparison group: N = 89 (45.5 years old) | RCT | 12 | 4 |
| Reference | Employment Outcomes | Results | Quality Assessment |
|---|---|---|---|
| Germundsson, P.; et al. (2012) [32] | Obtaining a job: (1) level of employment; (2) disposable income; (3) sum of allowances. | The authors reported that supported employment participants were hired faster, earned a higher disposable income, and lower individual allowances. Significance was not reported. | + |
| Hogelund, J.; et al. (2012) [66] | Time to full RTW: (1) time until first return to regular working hours. | This study suggested that PTSL did not reduce duration until full RTW for employees with mental disorders. Without controlling unobserved characteristics, they found a strong and significant effect of PTSL for these employees with mental disorders. However, this effect disappeared after the correction for unobserved characteristics. | + |
| van Veggel, R.; et al. (2015) [50] | Competitive employment: (1) getting a job in competitive employment; (2) individuals accumulating 13 weeks or more employment; (3) individuals accumulating 26 weeks or more employment; (4) days to first job; (5) mean hours worked per week in employment. | The authors found that more IPS participants initiated competitive employment than pre-IPS participants (24.9% vs. 14.3%). Significance not reported. | + |
| Andren, D. (2014) [51] | Time to return to work: (1) fully recovering lost work capacity and (2) duration of sick leave. | This study suggests positive and significant effects of PTSL after 60 days of FTSL for persons with mental disorders. | + |
| Kroger, C.; et al. (2014) [52] | Sickness absence: (1) days of incapacity to work. | This study underlined that more W-CBT participants were working at the follow-up and the treatment effect size for W-CBT was significantly higher than the control group effect. | + |
| Lagerveld, S. E.; et al. (2012) [53] | RTW: (1) full RTW; (2) duration of full RTW; (3) duration of partial RTW; Process of RTW: (4) number of steps until full RTW; (5) RTW relapses. | The authors of the study found significant effects on duration until full RTW in the W-CBT group: full RTW occurred 65 days earlier and partial RTW occurred 12 days earlier. W-CBT experienced relapse more often, but the difference was not significant. | ++ |
| Martin, M. H.; et al. (2013) [54] | RTW: (1) time to RTW and (2) labor market status (self-supported, receiving sickness benefits, unemployment, disability, other). | This study found that the intervention significantly delayed time to RTW (HR = 0.50; 95% CI 0.34–0.75) in comparison with conventional case management. | + |
| Arends, I.; et al. (2014) [55] | Sickness absence: (1) recurrent sickness absence episodes; (2) time until recurrent sick absence. | This study underlined that the SHARP intervention was significantly effective in increasing the time until relapse and reducing sickness absence episodes, compared to care as usual. | + |
| Bejerholm, U.; et al. (2015) [56] | Competitive employment: (1) getting a job; (2) number of hours worked; (3) weeks worked; (4) job tenure; (5) income; and (6) time to first employment. | The authors found that IPS was significantly more effective than TVR in job access at 18-month follow-up (46% vs. 11%; difference 36%, 95% CI 18–54), as well as the number of working hours and weeks, longer job tenure periods, and income. | ++ |
| Hees, H. L.; et al. (2013) [57] | RTW: (1) time until partial RTW; (2) full RTW (3) absenteeism; (4) RTW with good health. | This study found that TAU+OT significantly accelerated work achievement and increased the probability of RTW in good health (GH). However, the addition of OT to TAU did not hasten recovery from depression. | ++ |
| Heslin, M.; et al. (2011) [58] | Job access: (1) competitive employment at 12 months; (2) competitive employment at 24 months | The authors of this IPS study reported that the intervention program was significantly more effective in obtaining a competitive job at 24 months follow-up than TAU (22% vs. 11%, p = 0.041). Previous work in the last 5 years also predicted job achievement and time to work attainment. | ++ |
| Hoffmann, H.; et al. (2012) [59] | Job access: (1) competitive employment rate; (2) length of employment at least 50% in competitive work (CW); (3) total weeks in CW; (4) annual weeks CW; (5) job tenure in longest CW held; (6) mean hours worked per year in CW; (7) cumulative duration of CW; (8) yearly income from CW; and (9) hourly competitive job wage in last 3 years. | This study showed that SE program was significantly more effective than TVR programs in assisting persons with severe mental illness to obtain and maintain competitive employment (65% compared with 33%). | ++ |
| Hoffmann, H.; et al. (2014) (Follow up study of Hoffmann et al., 2012) [65] | Job access: (1) competitive employment rate; (2) length of employment at least 50% in competitive work (CW); (3) total weeks in CW; (4) annual weeks CW; (5) job tenure in longest CW held; (6) mean hours worked per year in CW; (7) cumulative duration of CW; (8) yearly income from CW; and (9) hourly competitive job wage in last 3 years. | The authors found that SE intervention (IPS), at 5-year follow-up, was significantly more effective than TVR for competitive employment rate, length of employment, total weeks in CW, annual weeks CW, job tenure in longest CW, mean hours worked. | ++ |
| Michon, H.; et al. (2014) [60] | Rates of competitive employment: (1) gaining a competitive job; (2) days in competitive employment; (3) hours in competitive employment; (4) days to first job. | This study found that significantly more participants obtained competitive jobs before 18 and 30 months in the IPS group than the participants in the TVR group. | ++ |
| Noordik, E.; et al. (2013) [61] | RTW: (1) time to full RTW; (2) time to partial RTW; and (3) number of sick leave relapses. | The authors of this study reported that workers receiving the RTW-E intervention (209 days; 95% CI 62–256) had a significantly extended time to full RTW compared to workers receiving CAU (153 days; 95% CI 128–178). | + |
| Reme, S. E.; et al. (2015) [62] | Maintain or increase active work-life: (1) maintained work participation or new employment; (2) full or partial RTW. | This study showed that the intervention group had increased or maintained their work participation at follow-up compared to the control group (44.2% vs. 37.2%, p = 0.015). The effectiveness at 18 months remained significant. However, RTW results were inconsistent. | ++ |
| Vlasveld, M. C.; et al. (2013) [63] | RTW: (1) Duration until lasting, full RTW; (2) total number of sickness absence days | The results of this study suggested that the intervention was not significantly effective for the work-related outcomes. Collaborative care participants had a shorter time to response, with a difference of 2.8 months. | + |
| Volker, D.; et al. (2015) [64] | RTW: (1) time to first RTW; (2) time to full RTW; (3) number of days of sickness absence in the first-year follow-up. | The authors of the study determined inconclusive results. There was a significant RTW duration reduction until first RTW only. Time to full RTW and number of sickness absence days had no significant effects. | + |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Muñoz-Murillo, A.; Esteban, E.; Ávila, C.C.; Fheodoroff, K.; Haro, J.M.; Leonardi, M.; Olaya, B. Furthering the Evidence of the Effectiveness of Employment Strategies for People with Mental Disorders in Europe: A Systematic Review. Int. J. Environ. Res. Public Health 2018, 15, 838. https://doi.org/10.3390/ijerph15050838
Muñoz-Murillo A, Esteban E, Ávila CC, Fheodoroff K, Haro JM, Leonardi M, Olaya B. Furthering the Evidence of the Effectiveness of Employment Strategies for People with Mental Disorders in Europe: A Systematic Review. International Journal of Environmental Research and Public Health. 2018; 15(5):838. https://doi.org/10.3390/ijerph15050838
Chicago/Turabian StyleMuñoz-Murillo, Amalia, Eva Esteban, Carolina C. Ávila, Klemens Fheodoroff, Josep Maria Haro, Matilde Leonardi, and Beatriz Olaya. 2018. "Furthering the Evidence of the Effectiveness of Employment Strategies for People with Mental Disorders in Europe: A Systematic Review" International Journal of Environmental Research and Public Health 15, no. 5: 838. https://doi.org/10.3390/ijerph15050838