Employee Perceptions of Workplace Health Promotion Programs: Comparison of a Tailored, Semi-Tailored, and Standardized Approach

Abstract
:1. Introduction
- (1)
- A fully tailored one-on-one health consultation with a registered dietitian and exercise physiologist;
- (2)
- A semi-tailored SMS health messages program with tailoring based on employees’ reported readiness to change exercise and eating behaviors; and
- (3)
- A standardized group health workshop presentation delivered by a registered dietitian and exercise physiologist.
2. Materials and Methods
2.1. Participants
2.1.1. Tailored Individual Consultation
2.1.2. Semi-Tailored SMS Health Message Program
2.1.3. Standardized Group Workshop
2.2. Design
2.3. Procedure
2.3.1. Ethics Approval
2.3.2. Recruitment
2.3.3. Tailored Individual Consultation
2.3.4. Semi-Tailored SMS Health Message Program
2.3.5. Standardized Health Workshop
2.3.6. Program Evaluation
2.4. Measures
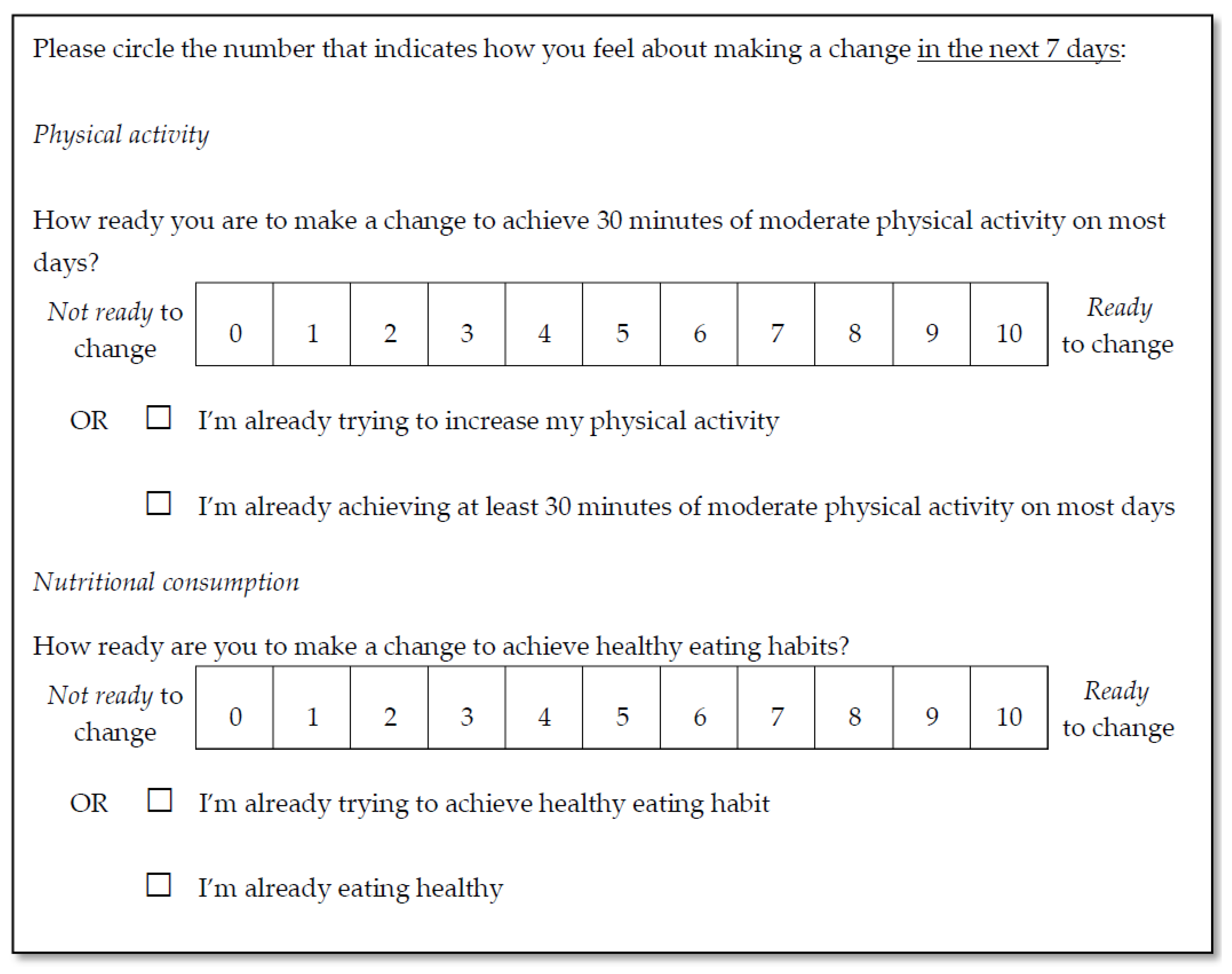
2.4.1. Readiness to Change
2.4.2. Overall Program Rating
2.4.3. Affect and Utility
3. Results
3.1. Overall Rating
3.2. Affect and Utility
3.2.1. Scale Reliability
3.2.2. Affect
3.2.3. Utility
4. Discussion
4.1. Overall Rating
4.2. Affect
4.3. Utility
4.4. Clinical Implications
4.5. Limitations
4.6. Future Research
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Arena, R.; Guazzi, M.; Briggs, P.D.; Cahalin, L.P.; Myers, J.; Kaminsky, L.A.; Forman, D.E.; Cipriano, G.; Borghi-Silva, A.; Babu, A.S. Promoting health and wellness in the workplace: A unique opportunity to establish primary and extended secondary cardiovascular risk reduction programs. Mayo Clin. Proc. 2013, 88, 605–617. [Google Scholar] [CrossRef] [PubMed]
- Ng, M.K.; Yousuf, B.; Bigelow, P.L.; Van Eerd, D. Effectiveness of health promotion programmes for truck drivers: A systematic review. Health Educ. J. 2015, 74, 270–286. [Google Scholar] [CrossRef]
- Pescud, M.; Waterworth, P.; Shilton, T.; Teal, R.; Slevin, T.; Ledger, M.; Lester, L.; Rosenberg, M. A healthier workplace? Implementation of fruit boxes in the workplace. Health Educ. J. 2016, 75, 843–854. [Google Scholar] [CrossRef]
- Hutchinson, A.D.; Wilson, C. Improving nutrition and physical activity in the workplace: A meta-analysis of intervention studies. Health Promot. Int. 2012, 27, 238–249. [Google Scholar] [CrossRef] [PubMed]
- ODonnell, M.P.; Bishop, C.; Kaplan, K. Benchmarking best practices in workplace health promotion. Am. J. Health Promot. 1997, 1, 1–8. [Google Scholar]
- Rodrigues, A.L.; Ball, J.; Ski, C.; Stewart, S.; Carrington, M.J. A systematic review and meta-analysis of primary prevention programmes to improve cardio-metabolic risk in non-urban communities. Prev. Med. 2016, 87, 22–34. [Google Scholar] [CrossRef] [PubMed]
- Nöhammer, E.; Schusterschitz, C.; Stummer, H. Employee perceived effects of workplace health promotion. Int. J. Workplace Health Manag. 2013, 6, 38–53. [Google Scholar] [CrossRef]
- Conn, V.S.; Hafdahl, A.R.; Cooper, P.S.; Brown, L.M.; Lusk, S.L. Meta-analysis of workplace physical activity interventions. Am. J. Prev. Med. 2009, 37, 330–339. [Google Scholar] [CrossRef] [PubMed]
- Kilpatrick, M.; Blizzard, L.; Sanderson, K.; Teale, B.; Nelson, M.; Chappell, K.; Venn, A. Investigating employee-reported benefits of participation in a comprehensive Australian workplace health promotion program. J. Occup. Environ. Med. 2016, 58, 505–513. [Google Scholar] [CrossRef] [PubMed]
- Anderson, L.M.; Quinn, T.A.; Glanz, K.; Ramirez, G.; Kahwati, L.C.; Johnson, D.B.; Buchanan, L.R.; Archer, W.R.; Chattopadhyay, S.; Kalra, G.P.; et al. The effectiveness of worksite nutrition and physical activity interventions for controlling employee overweight and obesity: A systematic review. Am. J. Prev. Med. 2009, 37, 340–357. [Google Scholar] [CrossRef] [PubMed]
- Mhurchu, C.N.; Aston, L.M.; Jebb, S.A. Effects of worksite health promotion interventions on employee diets: A systematic review. BMC Public Health 2010, 10, 62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goetzel, R.Z.; Ozminkowski, R.J.; Bowen, J.; Tabrizi, M.J. Employer integration of health promotion and health protection programs. Int. J. Workplace Health Manag. 2008, 1, 109–122. [Google Scholar] [CrossRef]
- Lenneman, J.; Schwartz, S.; Giuseffi, D.L.; Wang, C. Productivity and health: An application of three perspectives to measuring productivity. J. Occup. Environ. Med. 2011, 53, 55–61. [Google Scholar] [CrossRef] [PubMed]
- Hymel, P.A.; Loeppke, R.R.; Baase, C.M.; Burton, W.N.; Hartenbaum, N.P.; Hudson, T.W.; McLellan, R.K.; Mueller, K.L.; Roberts, M.A.; Yarborough, C.M. Workplace health protection and promotion: A new pathway for a healthier—and safer—workforce. J. Occup. Environ. Med. 2011, 53, 695–702. [Google Scholar] [CrossRef] [PubMed]
- Rongen, A.; Robroek, S.J.W.; Van Lenthe, F.J.; Burdorf, A. Workplace health promotion: A meta-analysis of effectiveness. Am. J. Prev. Med. 2013, 44, 406. [Google Scholar] [CrossRef] [PubMed]
- Noar, S.M.; Chabot, M.; Zimmerman, R.S. Applying health behavior theory to multiple behavior change: Considerations and approaches. Prev. Med. 2008, 46, 275–280. [Google Scholar] [CrossRef] [PubMed]
- Kristén, L.; Ivarsson, A.; Parker, J.; Ziegert, K. Future challenges for intervention research in health and lifestyle research—A systematic meta-literature review. Int. J. Qual. Stud. Health Well-Being 2015, 10, 27326. [Google Scholar] [CrossRef] [PubMed]
- Harden, A.; Peersman, G.; Oliver, S.; Mauthner, M.; Oakley, A. A systematic review of the effectiveness of health promotion interventions in the workplace. Occup. Med. 1999, 49, 540–548. [Google Scholar] [CrossRef]
- Brug, J.; Oenema, A.; Ferreira, I. Theory, evidence and intervention mapping to improve behavior nutrition and physical activity interventions. Int. J. Behav. Nutr. Phys. Act. 2005, 2, 2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crutzen, R.; Cyr, D.; de Vries, N.K. Bringing loyalty to e-health: Theory validation using three internet-delivered interventions. J. Med. Internet Res. 2011, 13. [Google Scholar] [CrossRef] [PubMed]
- Michie, S.; Fixsen, D.; Grimshaw, J.M.; Eccles, M.P. Specifying and reporting complex behaviour change interventions: The need for a scientific method. Implement Sci. 2009, 4, 40. [Google Scholar] [CrossRef] [PubMed]
- Webb, T.L.; Joseph, J.; Yardley, L.; Michie, S. Using the internet to promote health behavior change: A systematic review and meta-analysis of the impact of theoretical basis, use of behavior change techniques, and mode of delivery on efficacy. J. Med. Internet Res. 2010, 12. [Google Scholar] [CrossRef] [PubMed]
- Radcliff, T.A.; Bobroff, L.B.; Lutes, L.D.; Durning, P.E.; Daniels, M.J.; Limacher, M.C.; Janicke, D.M.; Martin, A.D.; Perri, M.G. Comparing costs of telephone vs face-to-face extended-care programs for the management of obesity in rural settings. J. Acad. Nutr. Diet. 2012, 112, 1363–1373. [Google Scholar] [CrossRef] [PubMed]
- Noar, S.M.; Benac, C.N.; Harris, M.S. Does tailoring matter? Meta-analytic review of tailored print health behavior change interventions. Psychol. Bull. 2007, 133, 673. [Google Scholar] [CrossRef] [PubMed]
- Fjeldsoe, B.S.; Marshall, A.L.; Miller, Y.D. Behavior change interventions delivered by mobile telephone short-message service. Am. J. Prev. Med. 2009, 36, 165–173. [Google Scholar] [CrossRef] [PubMed]
- Crutzen, R. On the use of internet-delivered interventions in worksite health promotion. In Well-Being; Springer: London, UK, 2011; pp. 174–182. [Google Scholar]
- Attfield, S.; Kazai, G.; Lalmas, M.; Piwowarski, B. Towards a Science of User Engagement (Position Paper). In Proceedings of the WSDM Workshop on User Modelling for Web Applications, Hong Kong, China, 9–12 February 2011; pp. 9–12. [Google Scholar]
- McCleary, K.; Goetzel, R.Z.; Roemer, E.C.; Berko, J.; Kent, K.; De La Torre, H. Employer and employee opinions about workplace health promotion (wellness) programs: Results of the 2015 Harris poll Nielsen survey. J. Occup. Environ. Med. 2017, 59, 256–263. [Google Scholar] [CrossRef] [PubMed]
- Goetzel, R.Z.; Shechter, D.; Ozminkowski, R.J.; Marmet, P.F.; Tabrizi, M.J.; Roemer, E.C. Promising practices in employer health and productivity management efforts: Findings from a benchmarking study. J. Occup. Environ. Med. 2007, 49, 111–130. [Google Scholar] [CrossRef] [PubMed]
- Crutzen, R.; Ruiter, R.A.; de Vries, N.K. Can interest and enjoyment help to increase use of internet-delivered interventions? Psychol. Health 2014, 29, 1227–1244. [Google Scholar] [CrossRef] [PubMed]
- Bandura, A. Health promotion by social cognitive means. Health Educ. Behav. 2004, 31, 143–164. [Google Scholar] [CrossRef] [PubMed]
- Michie, S.; van Stralen, M.M.; West, R. The behaviour change wheel: A new method for characterising and designing behaviour change interventions. Implement Sci. 2011, 6, 42. [Google Scholar] [CrossRef] [PubMed]
- Mache, S.; Jensen, S.; Linnig, S.; Jahn, R.; Steudtner, M.; Ochsmann, E.; Preuß, G. Do overweight workers profit by workplace health promotion, more than their normal-weight peers? Evaluation of a worksite intervention. J. Occup. Med. Toxicol. 2015, 10, 28. [Google Scholar] [CrossRef] [PubMed]
- De Greef, M.; Van den Broek, K. Making the Case for Workplace Health Promotion: Analysis of the effects of WHP; European Network for Workplace Health Promotion: Essen, Germany, 2004. [Google Scholar]
- Grossmeier, J.; Terry, P.E.; Cipriotti, A.; Burtaine, J.E. Best practices in evaluating worksite health promotion programs. Am. J. Health Promot. 2010, 24, TAHP-1–TAHP-11. [Google Scholar] [CrossRef]
- Wilson, M.G.; Holman, P.B.; Hammock, A. A comprehensive review of the effects of worksite health promotion on health-related outcomes. Am. J. Health Promot. 1996, 10, 429–435. [Google Scholar] [CrossRef] [PubMed]
- Lacey, S.J.; Street, T. The bottom line: Linking psychological health risks with productivity costs for Australian miners. Int. J. Psychol. 2016, 51, 762. [Google Scholar]
- Middlestadt, S.E.; Sheats, J.L.; Geshnizjani, A.; Sullivan, M.R.; Arvin, C.S. Factors associated with participation in work-site wellness programs: Implications for increasing willingness among rural service employees. Health Educ. Behav. 2011, 38, 502–509. [Google Scholar] [CrossRef] [PubMed]
- Davis, F.D. Perceived usefulness, perceived ease of use, and user acceptance of information technology. Manag. Inf. Syst. Q. 1989, 13, 319–340. [Google Scholar] [CrossRef]
- Ainley, M.; Hidi, S.; Berndorff, D. Interest, learning, and the psychological processes that mediate their relationship. J. Educ. Psychol. 2002, 94, 545. [Google Scholar] [CrossRef]
- Crutzen, R.; de Nooijer, J.; Brouwer, W.; Oenema, A.; Brug, J.; de Vries, N.K. A conceptual framework for understanding and improving adolescents’ exposure to internet-delivered interventions. Health Promot. Int. 2009, 24, 277–284. [Google Scholar] [CrossRef] [PubMed]
- Australian Government Department of Health and Ageing. Nutrition and Physical Activity Guidelines. Available online: http://www.health.gov.au/internet/main/publishing.nsf/Content/Nutrition+and+Physical+Activity-1 (accessed on 12 March 2018).
- Shinitzky, H.E.; Kub, J. The art of motivating behavior change: The use of motivational interviewing to promote health. Public Health Nurs. 2001, 18, 178–185. [Google Scholar] [CrossRef] [PubMed]
- Miller, W.R.; Rollnick, S. Motivational Interviewing: Helping People Change; Guilford Press: New York, NY, USA, 2012. [Google Scholar]
- Street, T.D.; Lacey, S.J. Empowering, progressing and sustaining employee health behaviours via SMS: An applied study design. In Proceedings of the 28th International Congress of Applied Psychology, Paris, France, 8–13 July 2014. [Google Scholar]
- Walthouwer, M.J.L.; Oenema, A.; Soetens, K.; Lechner, L.; De Vries, H. Systematic development of a text-driven and a video-driven web-based computer-tailored obesity prevention intervention. BMC Public Health 2013, 13, 978. [Google Scholar] [CrossRef] [PubMed]
- IBM Corporation. IBM SPSS Statistics for Windows, version 21.0 (Computer Software); IBM Corporation: Armonk, NY, USA, 2012. [Google Scholar]
- Street, T.D.; Lacey, S.J.; Grambower, J.A. Employees prefer information more than free food. Int. J. Workplace Health Manag. 2017, 10, 332–342. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Program | x | SD | 95% CI |
|---|---|---|---|
| Tailored individual consultations | 9.42 | 0.83 | [9.02, 9.82] |
| Semi-tailored SMS health messages program | 6.37 | 2.07 | [6.04, 6.69] |
| Standardized group workshop | 8.93 | 1.10 | [8.74, 9.13] |
| Program | Item/Theme | n | Example Response |
|---|---|---|---|
| Tailored individual consultations | |||
| What did you like most about the service? | 19 | ||
| Authority | 3 | “The doctor knew his stuff” | |
| Content | 6 | “Information was relevant” | |
| Delivery | 2 | “Healthy people advising” | |
| Other | 1 | “Everything!” | |
| Tailoring | 6 | “Personalized, helpful, informative” | |
| Self-awareness | 1 | “Cam was able to identify possible health risks in my life I wasn’t aware of that I have been wanting to change” | |
| What did you like least about the service? | 5 | ||
| Content | 1 | “Green tea, hate the stuff!” | |
| Self-awareness | 4 | “Having to look at how I have let myself down” | |
| Do you have any suggestions to improve the service? | 6 | ||
| Content | 1 | “Worthwhile information for an aging workforce” | |
| Delivery | 5 | “Please provide regularly” | |
| Semi-tailored SMS health messages program | |||
| What did you like most about the service? | 96 | ||
| Authority | 2 | “Factual” | |
| Content | 58 | “Thought provoking topics” | |
| Delivery | 16 | “I liked the regular health reminder” | |
| Other | 4 | “It was a discussion point with work colleagues” | |
| Self-awareness | 13 | “Simple reminders to stop and think about my own health” | |
| Tailoring | 2 | “The messages reinforced that I am making good decisions” | |
| What did you like least about the service? | 27 | ||
| Content | 7 | “The advice was very general and ‘common sense’. I didn’t benefit from the information given” | |
| Delivery | 6 | “Our irregular starting times meant that I was getting SMS messages while sleeping” | |
| Other | 6 | “It probably works for some, but not for me” | |
| Self-awareness | 1 | “I need to make more of a commitment” | |
| Tailoring | 7 | “I felt as though the messages assumed I was unhealthy” | |
| Do you have any suggestions to improve the service? | 58 | ||
| Authority | 4 | “More of the factual messages” | |
| Content | 24 | “Links to health resources would be good e.g., recipes” | |
| Delivery | 14 | “Reduce the number of messages to 1 or 2 a week” | |
| Other | 2 | “Ditch it, it has no relevance to me and provided no practical benefits” | |
| Tailoring | 14 | “Make it more personalized e.g., get each person to provide their goals and custom messages to that” | |
| Standardized group workshop | |||
| What did you like most about the service? | 95 | ||
| Authority | 6 | “Strongly evidence based” | |
| Content | 42 | “Explanation of brain function and fitness” | |
| Delivery | 42 | “Presenter was engaging, motivating, well-spoken and had great examples” | |
| Other | 4 | “I feel a bit more motivated” | |
| Self-awareness | 1 | “Raised my awareness” | |
| What did you like least about the service? | 34 | ||
| Content | 5 | “Didn’t address how people are confused by the multiplicity of often conflicting health messages” | |
| Delivery | 29 | “Not enough time to discuss, needed an hour” | |
| Do you have any suggestions to improve the service? | 37 | ||
| Content | 14 | “More healthy eating suggestions/plans” | |
| Delivery | 23 | “Regular check in and on-going sessions” | |
| Tailored Individual Consultations | Semi-Tailored SMS Health Messages Program | Standardized Group Workshop | |||||||
|---|---|---|---|---|---|---|---|---|---|
| x | SD | 95% CI | x | SD | 95% CI | x | SD | 95% CI | |
| Affect | |||||||||
| The service was interesting | 4.78 | 0.43 | [4.57, 4.99] | 3.58 | 1.16 | [3.38, 3.78] | 4.64 | 0.54 | [4.54, 4.73] |
| The service was motivating | 4.72 | 0.56 | [4.44, 5.01] | 3.58 | 1.00 | [3.40, 3.76] | 4.55 | 0.59 | [4.45, 4.64] |
| The service was enjoyable | 4.67 | 0.69 | [4.33, 5.01] | 3.44 | 1.12 | [3.25, 3.64] | 4.61 | 0.53 | [4.52, 4.70] |
| The service was personal | 4.67 | 0.49 | [4.43, 4.91] | 3.46 | 0.88 | [3.30, 3.62] | 3.75 | 0.83 | [3.61, 3.89] |
| I felt supported | 4.78 | 0.43 | [4.57, 4.99] | 3.47 | 0.94 | [3.30, 3.63] | 3.92 | 0.78 | [3.79, 4.05] |
| I trust the information provided | 4.78 | 0.43 | [4.57, 4.99] | 3.56 | 1.26 | [3.34, 3.79] | 4.52 | 0.56 | [4.42, 4.61] |
| I would use the service again | 4.72 | 0.58 | [4.44, 5.01] | 3.71 | 1.20 | [3.49, 3.92] | 4.34 | 0.65 | [4.23, 4.44] |
| I would recommend the service to others wanting to improve their health | 4.78 | 0.43 | [4.57, 4.99] | 3.64 | 1.16 | [3.44, 3.85] | 4.44 | 0.63 | [4.33, 4.54] |
| Overall affect | 4.74 | 0.43 | [4.52, 4.95] | 3.54 | 0.88 | [3.39, 3.70] | 4.35 | 0.48 | [4.26, 4.43] |
| Utility | |||||||||
| The information in the service was useful | 4.67 | 0.49 | [4.43, 4.91] | 3.55 | 1.14 | [3.35, 3.75] | 4.57 | 0.53 | [4.48, 4.66] |
| The service increased my confidence in my ability to choose healthy behaviors | 4.67 | 0.49 | [4.43, 4.91] | 3.47 | 0.89 | [3.31, 3.63] | 4.12 | 0.72 | [4.00, 4.25] |
| The service increased my awareness of health risks related to my behaviors | 4.44 | 0.78 | [4.05, 4.83] | 3.60 | 1.13 | [3.40, 3.80] | 4.26 | 0.73 | [4.14, 4.39] |
| The service increased my knowledge of how to achieve a healthy lifestyle | 4.56 | 0.62 | [4.25, 4.86] | 3.63 | 1.08 | [3.44, 3.82] | 4.28 | 0.69 | [4.17, 4.40] |
| The service provided relevant health information | 4.72 | 0.46 | [4.49, 4.95] | 3.54 | 1.21 | [3.33, 3.75] | 4.54 | 0.65 | [4.43, 4.65] |
| I was able to easily use the service to receive health information | 4.56 | 0.51 | [4.30, 4.81] | 3.62 | 1.35 | [3.38, 3.86] | 4.50 | 0.58 | [4.41, 4.60] |
| I could set my own health goals | 4.67 | 0.49 | [4.43, 4.91] | 3.49 | 0.94 | [3.33, 3.66] | 4.28 | 0.63 | [4.18, 4.39] |
| I will act upon the information provided | 4.67 | 0.49 | [4.43, 4.91] | 3.51 | 1.01 | [3.33, 3.69] | 4.31 | 0.60 | [4.21, 4.41] |
| Overall utility | 4.62 | 0.47 | [4.39, 4.85] | 3.55 | 0.89 | [3.40, 3.71] | 4.40 | 0.49 | [4.28, 4.44] |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Street, T.D.; Lacey, S.J. Employee Perceptions of Workplace Health Promotion Programs: Comparison of a Tailored, Semi-Tailored, and Standardized Approach. Int. J. Environ. Res. Public Health 2018, 15, 881. https://doi.org/10.3390/ijerph15050881
Street TD, Lacey SJ. Employee Perceptions of Workplace Health Promotion Programs: Comparison of a Tailored, Semi-Tailored, and Standardized Approach. International Journal of Environmental Research and Public Health. 2018; 15(5):881. https://doi.org/10.3390/ijerph15050881
Chicago/Turabian StyleStreet, Tamara D., and Sarah J. Lacey. 2018. "Employee Perceptions of Workplace Health Promotion Programs: Comparison of a Tailored, Semi-Tailored, and Standardized Approach" International Journal of Environmental Research and Public Health 15, no. 5: 881. https://doi.org/10.3390/ijerph15050881