Moderators of School-Based Physical Activity Interventions on Cardiorespiratory Endurance in Primary School-Aged Children: A Meta-Regression


Abstract
:1. Introduction
2. Materials and Methods
2.1. Literature Search Strategy
2.2. Eligibility Criteria
2.3. Type of Participants
2.4. Types of Physical Activity Interventions
2.5. Outcome Measures
2.6. Calculation of Standardized Mean Differences
2.7. Data Processing
2.8. Statistical Analysis
3. Results
3.1. Sample Characteristics
3.2. Intervention Characteristics
3.3. Assessments
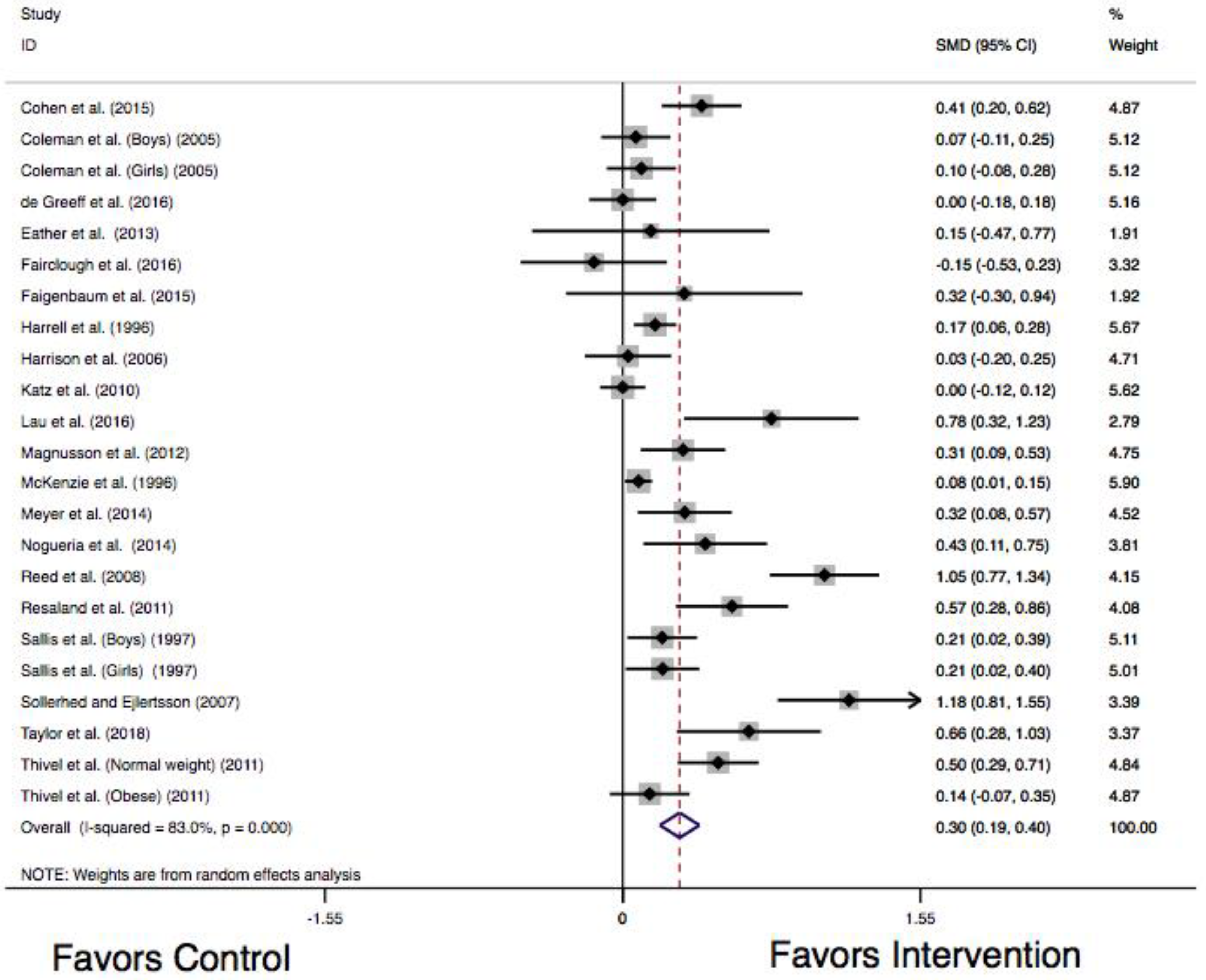
3.4. Meta-Analysis
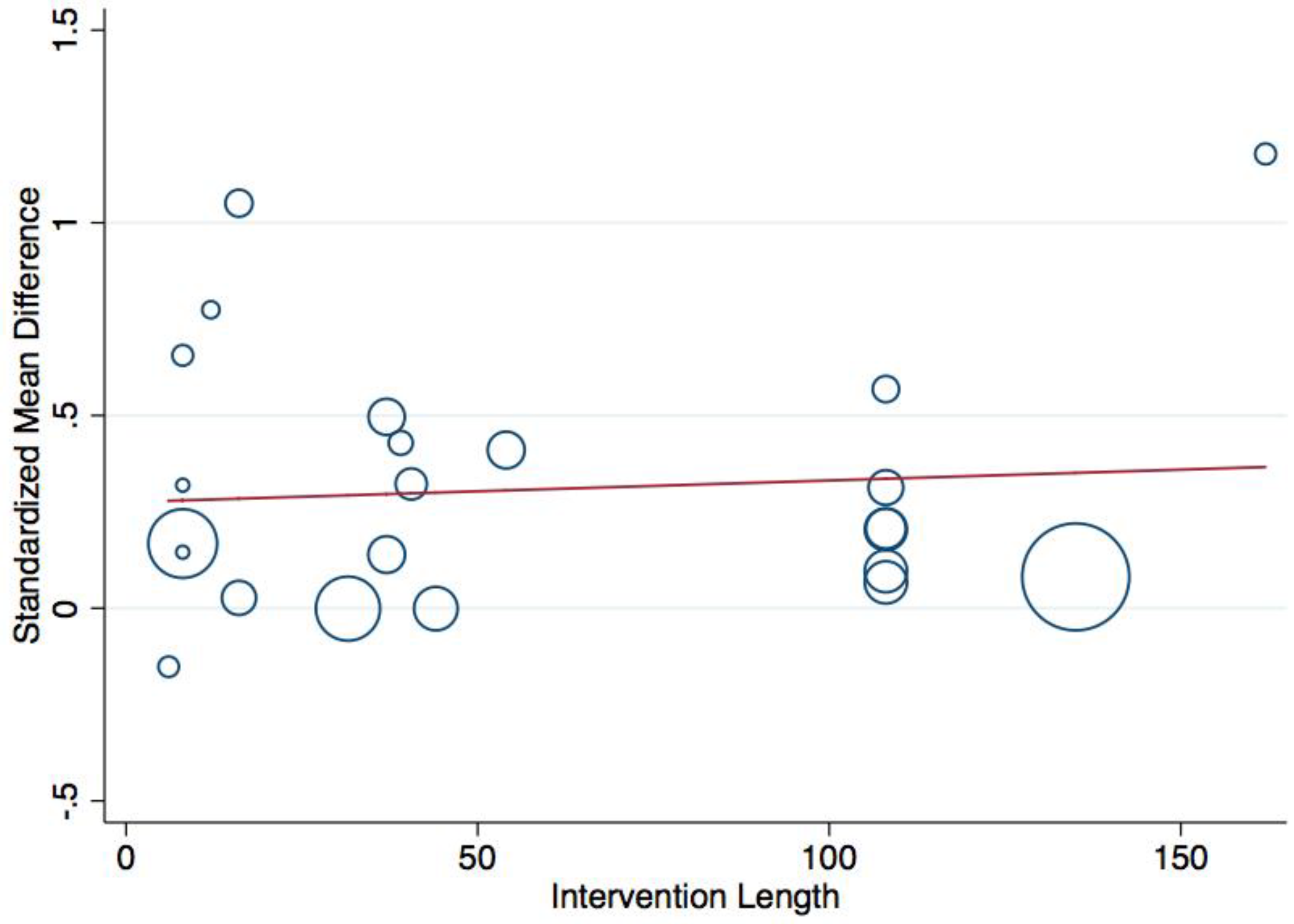
3.5. Meta-Regression
3.6. Sensitivity Analysis
3.7. Trim and Fill
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Ekelund, U.; Luan, J.; Sherar, L.B.; Esliger, D.W.; Griew, P.; Cooper, A.; for the International Children’s Accelerometry Database. Moderate to vigorous physical activity and sedentary time and cardio-metabolic risk factors in children and adolescents. JAMA 2012, 307, 704–712. [Google Scholar] [CrossRef] [PubMed]
- Hillman, C.H.; Erickson, K.I.; Kramer, A.F. Be smart, exercise your heart: Exercise effects on brain and cognition. Nat. Rev. Neurosci. 2008, 9, 58–65. [Google Scholar] [CrossRef] [PubMed]
- Biddle, S.J.; Asare, M. Physical activity and mental health in children and adolescents: A review of reviews. Br. J. Sports Med. 2011, 45, 886–895. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Katzmarzyk, P.T.; Denstel, K.N.; Beals, K.; Bolling, C.; Wright, C.; Crouter, S.E.; McKenzie, T.L.; Pate, R.R.; Saelens, B.E.; Staiano, A.E.; et al. Results from the United States of America’s 2016 report card on physical activity for children and youth. J. Phys. Act. Health 2016, 13, S307–S313. [Google Scholar] [CrossRef] [PubMed]
- Cooper, A.R.; Goodman, A.; Page, A.S.; Sherar, L.B.; Esliger, D.W.; Sluijs, E.M.; Andersen, L.B.; Anderssen, S.; Cardon, G.; Davey, R.; et al. Objectively measured physical activity and sedentary time in youth: The International children’s accelerometry database (ICAD). Int. J. Behav. Nutr. Phys. Act. 2015. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Strategies to Prevent Obesity and Other Chronic Diseases: The CDC Guide to Strategies to Increase Physical Activity in the Community. Available online: https://www.cdc.gov/obesity/downloads/PA_2011_WEB.pdf (accessed on 14 August 2018).
- Pate, R.R.; Davis, M.G.; Robinson, T.N.; Stone, E.J.; McKenzie, T.L.; Young, J.C. Promoting physical activity in children and youth: A leadership role for schools: A scientific statement from the American Heart Association Council on Nutrition, Physical Activity, and Metabolism (Physical Activity Committee) in collaboration with the Councils on Cardiovascular Disease in the Young and Cardiovascular Nursing. Circulation 2006, 114, 1214–1224. [Google Scholar] [PubMed]
- Beets, M.W.; Okely, A.; Weaver, R.G.; Webster, C.; Lubans, D.; Brusseau, T.; Carsom, R.; Cliff, D.P. The theory of expanded, extended, and enhanced opportunities for youth physical activity promotion. Int. J. Behav. Nutr. Phys. Act. 2016. [Google Scholar] [CrossRef] [PubMed]
- Mears, R.; Jago, R. Effectiveness of after-school interventions at increasing moderate-to-vigorous physical activity levels in 5- to 18-year olds: A systematic review and meta-analysis. Br. J. Sports Med. 2016. [Google Scholar] [CrossRef] [PubMed]
- Watson, A.; Timperio, A.; Brown, H.; Best, K.; Hesketh, K.D. Effect of classroom-based physical activity interventions on academic and physical activity outcomes: A systematic review and meta-analysis. Int. J. Behav. Nutr. Phys. Act. 2017. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. School health guidelines to promote healthy eating and physical activity. MMWR 2011, 60, 28–33. [Google Scholar]
- Carson, R.L.; Castelli, D.M.; Beighle, A.; Erwin, H. School-based physical activity promotion: A conceptual framework for research and practice. Child. Obes. 2014, 10, 100–106. [Google Scholar] [CrossRef] [PubMed]
- Vander Ploeg, K.A.; McGavock, J.; Maximova, K.; Veugelers, P.J. School-based health promotion and physical activity during and after school hours. Pediatrics 2014, 133, e371–e378. [Google Scholar] [CrossRef] [PubMed]
- Mahar, M.T.; Murphy, S.K.; Rowe, D.A.; Golden, J.; Shields, A.T.; Raedeke, T.D. Effects of a classroom-based program on physical activity and on-task behavior. Med. Sci. Sports Exerc. 2006, 38, 2086–2094. [Google Scholar] [CrossRef] [PubMed]
- Brusseau, T.A.; Hannon, J.C.; Burns, R. The effect of a Comprehensive School Physical Activity Program on physical activity and health-related fitness in children from low-income families. J. Phys. Act. Health 2016, 13, 888–894. [Google Scholar] [CrossRef] [PubMed]
- Naylor, P.J.; Nettlefold, L.; Race, D.; Hoy, C.; Ashe, M.C.; Higgins, J.W.; McKay, H.A. Implementation of school based physical activity interventions: A systematic review. Prev. Med. 2015, 72, 95–115. [Google Scholar] [CrossRef] [PubMed]
- Owen, M.B.; Curry, W.B.; Kerner, C.; Newson, L.; Fairclough, S.J. The effectiveness of school-based physical activity interventions for adolescent girls: A systematic review and meta-analysis. Prev. Med. 2007, 105, 237–249. [Google Scholar] [CrossRef] [PubMed]
- Saint-Maurice, P.F.; Welk, G.; Ihmels, M.A.; Krapfl, J.R. Validation of the SOPLAY direct observation tool with an accelerometry-based physical activity monitor. J. Phys. Act. Health 2011, 8, 1108–1116. [Google Scholar] [CrossRef] [PubMed]
- Cain, K.L.; Sallis, J.F.; Conway, T.L.; Van Dyck, D.; Calhoon, L. Using accelerometers in youth physical activity studies: A review of methods. J. Phys. Act. Health 2013, 10, 437–450. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Beets, M.W.; Pate, R.R.; Blair, S.N. The effect of reintegrating Actigraph accelerometer counts in preschool children: Comparison using different epoch lengths. J. Sci. Med. Sport 2013, 16, 129–134. [Google Scholar] [CrossRef] [PubMed]
- Brusseau, T.A.; Kulinna, P.H.; Tudor-Locke, C.; van der Mars, H.; Darst, P. Children’s step counts on weekend, physical education, and non physical education days. J. Hum. Kinet. 2011, 27, 125–135. [Google Scholar] [CrossRef]
- Remmers, T.; Thijs, C.; Timperio, A.; Salmon, J.O.; Veitch, J.; Kremers, S.P.J.; Ridgers, N.D. Daily weather and children’s physical activity patterns. Med. Sci. Sports Exerc. 2017, 49, 922–929. [Google Scholar] [CrossRef] [PubMed]
- Chan, C.B.; Ryan, D.A. Assessing the effects of weather conditions on physical activity participation using objective measures. Int. J. Environ. Res. Public Health 2009, 6, 2639–2654. [Google Scholar] [CrossRef] [PubMed]
- Borde, R.; Smith, J.J.; Sutherland, R.; Nathan, N.; Lubans, D.R. Methodological considerations and impact of school-based interventions on objectively measured physical activity in adolescents: A systematic review and meta-analysis. Obes. Rev. 2017, 18, 476–490. [Google Scholar] [CrossRef] [PubMed]
- Russ, L.B.; Webster, C.A.; Beets, M.W.; Phillips, D.S. Systematic review and meta-analysis of multi-component interventions through schools to increase physical activity. J. Phys. Act. Health 2015, 12, 1436–1446. [Google Scholar] [CrossRef] [PubMed]
- Welk, G.J.; Laurson, K.R.; Eisenmann, J.C.; Cureton, K.J. Development of youth aerobic capacity standards using receiver operating characteristic curves. Am. J. Prev. Med. 2011, 41, S111–S116. [Google Scholar] [CrossRef] [PubMed]
- Sasayama, K.; Ochi, E.; Adachi, M. Importance of Both Fatness and Aerobic Fitness on Metabolic Syndrome Risk in Japanese Children. PLoS ONE 2015. [Google Scholar] [CrossRef] [PubMed]
- Eisenmann, J.C.; Laurson, K.R.; Welk, G.J. Aerobic fitness percentiles for US adolescents. Am. J. Prev. Med. 2011, 41, S106–S110. [Google Scholar] [CrossRef] [PubMed]
- Eisenmann, J.C.; Katzmarzyk, P.T.; Perusse, L.; Tremblay, A.; Despres, J.P.; Bouchard, C. Aerobic fitness, body mass index, and CVD risk factors among adolescents: The Québec family study. Int. J. Obes. 2005, 29, 1077–1083. [Google Scholar] [CrossRef] [PubMed]
- Burns, R.D.; Brusseau, T.A.; Fang, Y.; Fu, Y.; Hannon, J.C. Waist-to-Height ratio, aerobic fitness, and cardio-metabolic risk in Hispanic children from low-income U.S. schools. Pediatr. Exerc. Sci. 2016, 28, 388–396. [Google Scholar] [CrossRef] [PubMed]
- An, R. Diet quality and physical activity in relation to childhood obesity. Int. J. Adolesc. Med. Health 2017. [Google Scholar] [CrossRef] [PubMed]
- Janssen, I.; Katzmarzyk, P.T.; Boyce, W.F.; Vereecken, C.; Mulvihill, C.; Roberts, C.; Currie, C.; Pickett, W.; The Health Behaviour in School-Aged Children Obesity Working Group. Comparison of overweight and obesity prevalence in school-aged youth from 34 countries and their relationships with physical activity and dietary patterns. Obes. Rev. 2005, 6, 123–132. [Google Scholar] [CrossRef] [PubMed]
- Morrow, J.R.; Freedson, P.S. Relationship between habitual physical activity and aerobic fitness in adolescents. Pediatr. Exerc. Sci. 1994, 6, 315–329. [Google Scholar] [CrossRef]
- Mahar, M.T.; Welk, G.J.; Rowe, D.A. Estimation of aerobic fitness from PACER performance with and without body mass index. Meas. Phys. Educ. Exerc. Sci. 2018. [Google Scholar] [CrossRef]
- Burns, R.D.; Hannon, J.C.; Brusseau, T.A.; Eisenman, P.A.; Shultz, B.B.; Saint-Maurice, P.F.; Welk, G.J.; Mahar, M.T. Development of an aerobic capacity prediction model from one-mile run/walk performance in adolescents aged 13–16 years. J. Sports Sci. 2016, 34, 18–26. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cohen, K.E.; Morgan, P.J.; Plontikoff, R.C.; Callister, R.; Lubans, D.R. Physical activity and skills intervention: SCORES cluster randomized controlled trial. Med. Sci. Sports Exerc. 2014, 47, 765–774. [Google Scholar] [CrossRef] [PubMed]
- Coleman, K.J.; Tiller, C.L.; Sanchez, J.; Heath, E.M.; Sy, O.; Milliken, G.; Dzewaltowski, D.A. Prevention of the epidemic increase in child risk of overweight in low-income schools: The El Paso coordinated approach to child health. Arch. Pediatr. Adolesc. Med. 2005, 159, 217–224. [Google Scholar] [CrossRef] [PubMed]
- De Greef, J.W.; Hartman, E.; Mullender-Wijnsma, M.J.; Bosker, R.J.; Doolaard, S.; Visscher, C. Long-term effects of physically active academic lessons on physical fitness and functions in primary school children. Health Educ. Res. 2016, 31, 185–194. [Google Scholar] [CrossRef] [PubMed]
- Eather, N.; Morgan, P.J.; Lubans, D.R. Feasibility and preliminary efficacy of the Fit4Fun intervention for improving physical fitness in a sample of primary school children: A pilot study. Phys. Educ. Sport Pedagog. 2013, 18, 389–411. [Google Scholar] [CrossRef]
- Fairclough, S.J.; McGrane, B.; Sanders, G.; Taylor, S.; Owen, M.; Curry, W. A non-equivalent group pilot trial of a school-based physical activity and fitness intervention for 10–11 year old English children: Born to move. BMC Public Health 2016, 16, 861. [Google Scholar] [CrossRef] [PubMed]
- Faigenbaum, A.D.; Bush, J.A.; McLoone, R.P.; Kreckel, M.C.; Farrell, A.; Ratamess, N.A.; Kang, J. Benefits of strength and skill-based training during primary school physical education. J. Strength Cond. Res. 2015, 29, 1255–1262. [Google Scholar] [CrossRef] [PubMed]
- Harrell, J.S.; McMurray, R.G.; Bangdiwala, S.I.; Frauman, A.C.; Gansky, S.A.; Bradley, C.B. Effects of a school-based intervention to reduce cardiovascular disease risk factors in elementary school children: The Cardiovascular Health in Children (CHIC) study. J. Pediatr. 1996, 128, 797–805. [Google Scholar] [CrossRef]
- Harrison, M.; Burns, C.F.; McGuinness, M.; Heslin, J.; Murphy, N.M. Influence of a health education intervention on physical activity and screen time in primary school children: ‘Switch Off—Get Active’. J. Sci. Med. Sport 2006, 9, 388–394. [Google Scholar] [CrossRef] [PubMed]
- Katz, D.L.; Cushman, D.; Reynolds, J.; Njike, V.; Treu, J.A.; Katz, C.; Walker, J.; Smith, E. Putting physical activity where it fits in the school day: Preliminary results of the ABC (Activity Bursts in the Classroom) for fitness program. Prev. Chronic Dis. 2010, 7, A82. [Google Scholar] [PubMed]
- Lau, P.W.; Wang, J.J.; Maddison, R. A randomized-controlled trial of school-based active videogame intervention on Chinese children’s aerobic fitness, physical activity level, and psychological correlates. Games Health J. 2016, 5, 405–412. [Google Scholar] [CrossRef] [PubMed]
- Magnusson, R.T.; Hrafnkelsson, H.; Sigurgeirsson, I.; Johannsson, E.; Sveinsson, T. Limited effects of a 2-year school-based physical activity intervention on body composition and cardiorespiratory fitness in 7-year-old children. Health Educ. Res. 2012, 27, 484–494. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McKenzie, T.L.; Nader, P.R.; Strikmiller, P.K.; Yang, M.; Stone, E.J.; Perry, C.L.; Taylor, W.C.; Epping, J.N.; Feldman, H.A.; Luepker, R.V.; et al. School physical education: Effect of the Child and Adolescent Trial for Cardiovascular Health. Prev. Med. 1996, 25, 423–431. [Google Scholar] [CrossRef] [PubMed]
- Meyer, U.; Schindler, C.; Zachner, L.; Ernst, D.; Hebestreit, H.; van Mechelen, W.; Brunner-La, R.H.P.; Probst-Hensch, N.; Puder, J.J.; Kriemler, S. Long-Term Effect of a school-based physical activity program (KISS) on fitness and adiposity in children: A cluster-randomized controlled trial. PLoS ONE 2014, 9, e87929. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nogueira, R.C.; Weeks, B.K.; Beck, B.R. An in-school exercise intervention to enhance bone and reduce fat in girls: The CAPO Kids trial. Bone 2014, 68, 92–99. [Google Scholar] [CrossRef] [PubMed]
- Reed, K.E.; Warburton, D.E.R.; Macdonald, H.M.; Naylor, P.J.; McKay, H.A. Action Schools! BC: A school-based physical activity intervention designed to decrease cardiovascular disease risk factors in children. Prev. Med. 2008, 46, 525–531. [Google Scholar] [CrossRef] [PubMed]
- Resaland, G.K.; Andersen, L.B.; Mamen, A.; Anderssen, S.A. Effects of a 2-year school-based daily physical activity intervention on cardiorespiratory fitness: The Sogndal school-intervention study. Scand. J. Med. Sci. Sports 2011, 21, 302–309. [Google Scholar] [CrossRef] [PubMed]
- Sallis, J.F.; McKenzie, T.L.; Alcaraz, J.E.; Kolody, B.; Faucette, N.; Hovell, M.F. Effects of a 2-year physical education program (SPARK) on physical activity and fitness in elementary school students. Am. J. Public Health 1997, 87, 1328–1334. [Google Scholar] [CrossRef] [PubMed]
- Sollerhed, A.C.; Ejlertsson, G. Physical benefits of expanded physical education in primary school: Findings from a 3-year intervention study in Sweden. Scand. J. Med. Sci. Sports 2008, 18, 102–107. [Google Scholar] [CrossRef] [PubMed]
- Taylor, S.L.; Noonan, R.J.; Knowles, Z.R.; Owen, M.B.; McGrane, B.; Curry, W.B.; Fairclough, S.J. Evaluation of a pilot school-based physical activity clustered randomised controlled trial—Active Schools: Skelmersdale. Int. J. Environ. Res. Public Health 2018, 15, 1011. [Google Scholar] [CrossRef] [PubMed]
- Thivel, D.; Isacco, L.; Lazaar, N.; Aucouturier, J.; Ratel, S.; Dore, E.; Meyer, M.; Duche, P. Effect of a 6-month school-based physical activity program on body composition and physical fitness in lean and obese school children. Eur. J. Pediatr. 2011, 170, 1435–1443. [Google Scholar] [CrossRef] [PubMed]
- van Sluijs, E.M.; McMinn, A.M.; Griffin, S.J. Effectiveness of interventions to promote physical activity in children and adolescents: Systematic review of controlled trials. Br. J. Sports Med. 2008, 42, 653–657. [Google Scholar] [CrossRef] [PubMed]
- Burns, R.D.; Fu, Y.; Podlog, L.W. School-based physical activity interventions and physical activity enjoyment: A meta-analysis. Prev. Med. 2017, 103, 84–90. [Google Scholar] [CrossRef] [PubMed]
- McEwan, D.; Harden, S.M.; Zumbo, B.D.; Sylvester, B.D.; Kaulius, M.; Ruissen, G.R.; Dowd, A.J.; Beauchamp, M.R. The effectiveness of multi-component goal setting interventions for changing physical activity behaviour: A systematic review and meta-analysis. Health Psychol. Rev. 2016, 10, 67–88. [Google Scholar] [CrossRef] [PubMed]
- Shilts, M.K.; Horowitz, M.; Townsend, M.S. Goal setting as a strategy for dietary and physical activity behavior change: A review of the literature. Am. J. Health Promot. 2004, 19, 81–93. [Google Scholar] [CrossRef] [PubMed]
- Lytle, L.; Achterberg, C. Changing the diet of America’s children: What works and why? J. Nutr. Educ. 1995, 27, 250–260. [Google Scholar] [CrossRef]
- Burns, R.D.; Brusseau, T.A.; Fu, Y. Influence of goal setting on physical activity and cardio-respiratory endurance in low-income children enrolled in CSPAP schools. Am. J. Health Educ. 2017, 48, 32–40. [Google Scholar] [CrossRef]
- Boreham, C.; Riddoch, C. The physical activity, fitness, and health of children. J. Sports Sci. 2001, 19, 915–919. [Google Scholar] [CrossRef] [PubMed]
- Trudeau, F.; Shephard, R.J. Physical education, school physical activity, school sports and academic performance. Int. J. Behav. Nutr. Phys. Act. 2008. [Google Scholar] [CrossRef] [PubMed]
- Boddy, L.M.; Murphy, M.H.; Cunningham, C.; Breslin, G.; Foweather, L.; Gobbi, R.; Graves, L.E.; Hopkins, N.D.; Auth, M.K.; Stratton, G. Physical activity, cardiorespiratory fitness, and clustered cardio-metabolic risk in 10- to 12-year-old school children: The REACH Y6 study. Am. J. Hum. Biol. 2014, 26, 446–451. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Conn, V.S.; Hafdahl, A.R.; Mehr, D.R. Interventions to increase physical activity among healthy adult: Meta-analysis of outcomes. Am. J. Public Health 2011, 101, 751–758. [Google Scholar] [CrossRef] [PubMed]
- Tannehill, D.; Van der Mars, H.; McPhail, A. Comprehensive school physical activity programs. In Building Effective Physical Education Programs; Jones & Bartlett Learning: Burlington, VT, USA, 2014; pp. 27–54. [Google Scholar]
- Comprehensive School Physical Activity Programs: A Guide for Schools; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2013; p. 12.
- Carson, R.L.; Castelli, D.M.; Pulling Kuhn, A.C.; Moore, J.B.; Beets, M.W.; Beighle, A.; Aija, R.; Calvert, H.G.; Glowacki, E.M. Impact of trained champions of comprehensive school physical activity programs on school physical activity offerings, youth physical activity and sedentary behaviors. Prev. Med. 2014, 69, S12–S19. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, N.; Tomkinson, G.; Ekelund, U. Aerobic fitness and its relationship to sport, exercise training and habitual physical activity during youth. Brit. J. Sports Med. 2011, 45, 849–858. [Google Scholar] [CrossRef] [PubMed]
- Minatto, G.; Barbosa Filho, V.C.; Berria, J.; Petroski, E.L. School-based interventions to improve cardiorespiratory fitness in adolescents: Systematic review with meta-analysis. Sports Med. 2016, 46, 1273–1292. [Google Scholar] [CrossRef] [PubMed]
- Crimarco, A.; Mayfield, C.; Mitchell, N.; Beets, M.W.; Yin, Z.; Moore, J.B. Determinants of attendance at a physical activity focused afterschool program in elementary school children. Int. J. Exerc. Sci. 2018, 11, 137–151. [Google Scholar] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Study Location | Sample Size | Sample Characteristics | Intervention Length | Intervention Characteristics | Cardiorespiratory Endurance Assessment |
|---|---|---|---|---|---|---|
| Cohen et al. (2015) [38] | Australia | n = 208 (control) n = 162 (intervention) | Low-income children | 12 months | RCT; multicomponent; physical activity and fundamental motor skill focus | 20-m multistage fitness test |
| Coleman et al. (2005) † [39] | United States | n = 473 (control) n = 423 (intervention) | Low-income children | 24 months | Non-RCT; multicomponent; enhanced physical education and cafeteria nutrition, parent education | Nine-minute timed run |
| De Greeff et al. (2016) [40] | The Netherlands | n = 250 (control) n = 249 (intervention) | Primary school-aged children | 24 months | RCT; single component; physically active academic lessons | 20-m multistage fitness test |
| Eather et al. (2013) [41] | Australia | n = 16 (control) n = 27 (intervention) | Primary school-aged children | Eight weeks | RCT; multicomponent; physical education, recess, home fitness program | 20-m multistage fitness test |
| Fairclough et al. (2016) [42] | United Kingdom | n = 48 (control) n = 59 (intervention) | Primary school-aged children | Six weeks | Non-RCT; single component; structured class-based physical activity and fitness program | Andersen Test (10 min 10-m intermittent shuttle run) |
| Faigenbaum et al. (2015) [43] | United States | n = 21 (control) n = 20 (intervention) | Fourth grade children | Eight weeks | RCT; single component; integrative strength skill and fitness program during physical education | 20-m PACER |
| Harrell et al. (1996) [44] | United States | n = 686 (control) n = 588 (intervention) | Rural and urban third and fourth graders | Eight weeks | RCT; multicomponent; exercise program, nutrition and smoking education classes | Eurofit submaximal cycle ergometry test |
| Harrison et al. (2006) [45] | Ireland | n = 130 (control) n = 182 (intervention) | Low-income primary school-aged children | 16 weeks | Non-RCT; single component; health education curriculum | 20-m multistage fitness test |
| Katz et al. (2010) [46] | United States | n = 503 (control) n = 603 (intervention) | Elementary school-aged children | Eight months | Non-RCT; single component; academic classroom activity breaks | 20-m PACER |
| Lau et al. (2016) [47] | China | n = 40 (control) n = 40 (intervention) | Primary school-aged children | 12 weeks | RCT; single component; active video game intervention | 20-m PACER |
| Magnusson et al. (2012) [48] | Iceland | n = 151 (control) n = 170 (intervention) | Elementary school-aged children | 24 months | RCT; multicomponent; increasing physical activity, promotion of active commuting, outdoor teaching, healthy dietary promotion | Maximal progressive cycle ergometer test |
| McKenzie et al. (1996) [49] | United States | n = 1294 (control) n = 1920 (intervention) | Elementary school-aged children | 30 months | RCT; multicomponent; health-related physical education, teacher training, on-site consultation | Nine-minute distance run |
| Meyer et al. (2014) [50] | Switzerland | n = 100 (control) n = 181 (intervention) | Elementary school-aged children | Nine months | RCT; multicomponent; additional physical education classes, academic classroom activity breaks, physical activity homework | 20-m multistage fitness test |
| Nogueira et al. (2014) [51] | Australia | n = 75 (control) n = 76 (intervention) | Primary school-aged girls | Nine months | Non-RCT; single component, addition of 10-min exercise sessions three times per week | 20-m multistage fitness test |
| Reed et al. (2008) [52] | Canada | n = 81 (control) n = 156 (intervention) | Elementary school-aged children | 16 weeks | RCT; multicomponent; school environment, scheduled physical education, extra-curricular, school spirit, family and community, classroom physical activity | 20-m multistage fitness test |
| Resaland et al. (2011) [53] | Norway | n = 86 (control) n = 102 (intervention) | Primary school-aged children | 24 months | Non-RCT; single component; additional 60 min of physical activity during school hours | Maximal progressive treadmill test |
| Sallis et al. (1997) † [54] | United States | n = 360 (control) n = 595 (intervention) | Elementary school-aged children | 24 months | RCT; multicomponent; health-related physical education, self-management | One-mile run test |
| Sollerhed and Ejlertsson (2007) [55] | Sweden | n = 74 (control) n = 58 (intervention) | Rural primary school aged children | 36 months | Non-RCT; single component; expanded physical education lessons | Six-minute running test |
| Taylor et al. (2018) [56] | United Kingdom | n = 55 (control) n = 60 (intervention) | Primary school-aged children | Eight weeks | RCT pilot; multicomponent; active breaks, videos, running clubs, playground challenges, teacher training, newsletters and activity homework | 20-m multistage fitness test |
| Thivel et al. (2011) † [57] | France | n = 228 (control) n = 229 (intervention) | Primary school-aged children | Six months | RCT; single component; additional two hours of exercise per week | 20-m multistage fitness test |
| B-Coefficient | 95% Confidence Interval | p-Value | |
|---|---|---|---|
| Multi-Component | −0.09 | −0.40–0.23 | 0.560 |
| Length (weeks) | 0.001 | −0.002–0.004 | 0.427 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Burns, R.D.; Brusseau, T.A.; Fu, Y. Moderators of School-Based Physical Activity Interventions on Cardiorespiratory Endurance in Primary School-Aged Children: A Meta-Regression. Int. J. Environ. Res. Public Health 2018, 15, 1764. https://doi.org/10.3390/ijerph15081764
Burns RD, Brusseau TA, Fu Y. Moderators of School-Based Physical Activity Interventions on Cardiorespiratory Endurance in Primary School-Aged Children: A Meta-Regression. International Journal of Environmental Research and Public Health. 2018; 15(8):1764. https://doi.org/10.3390/ijerph15081764
Chicago/Turabian StyleBurns, Ryan D., Timothy A. Brusseau, and You Fu. 2018. "Moderators of School-Based Physical Activity Interventions on Cardiorespiratory Endurance in Primary School-Aged Children: A Meta-Regression" International Journal of Environmental Research and Public Health 15, no. 8: 1764. https://doi.org/10.3390/ijerph15081764