The Effects of a Health Promotion Program Using Urban Forests and Nursing Student Mentors on the Perceived and Psychological Health of Elementary School Children in Vulnerable Populations



Abstract
:1. Introduction
Purpose of Study and Hypotheses
2. Materials and Methods
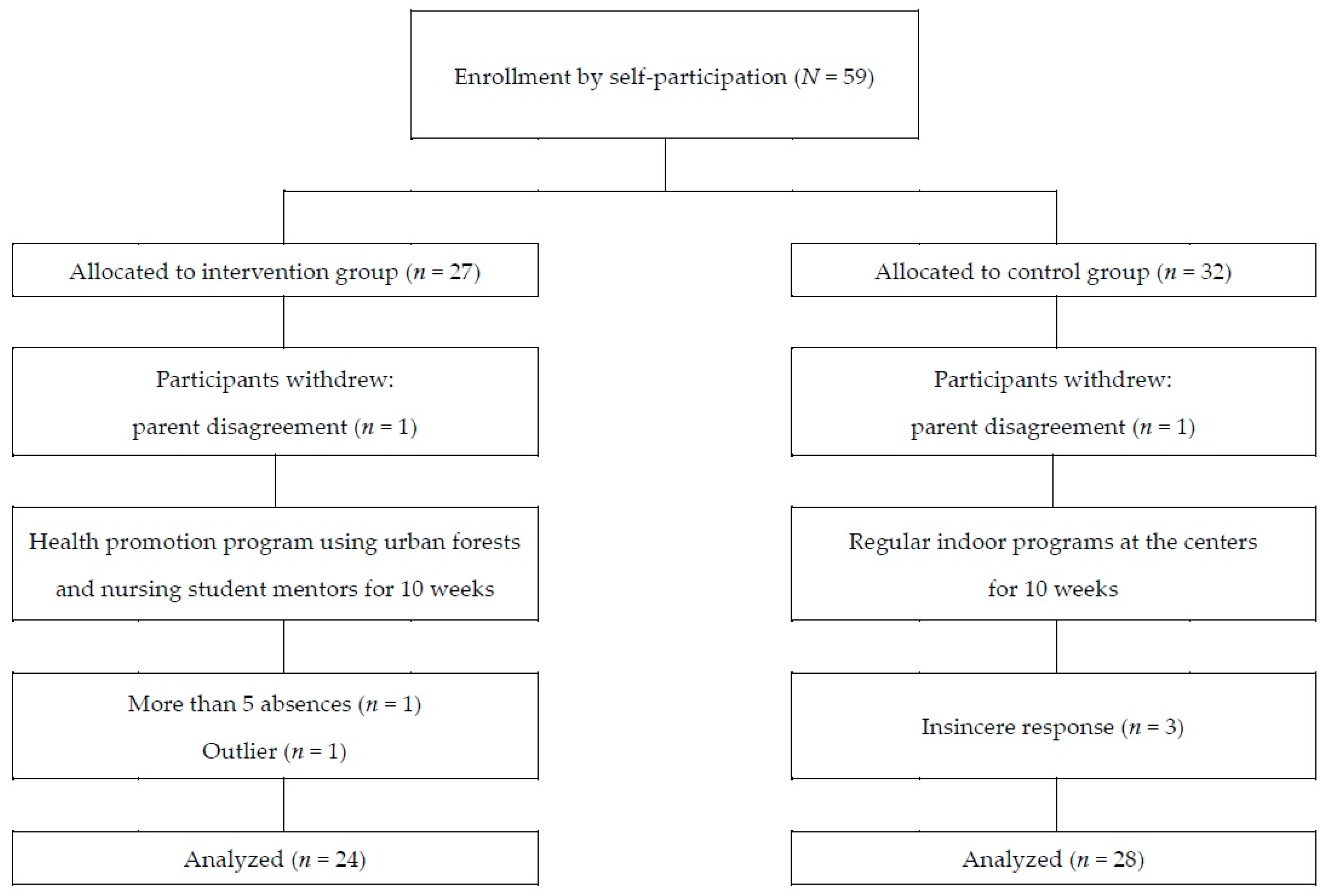
2.1. Study Design and Participants
2.2. Intervention
2.3. Measurements
2.4. Statistics
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Choi, I.; Mo, S.; Lee, S. A Study on Mental Health Improvement Policy for Children and Adolescents II; National Youth Policy Institute: Seoul, Korea, 2012. [Google Scholar]
- Carson, V.; Hunter, S.; Kuzik, N.; Gray, C.E.; Poitras, V.J.; Chaput, J.-P.; Saunders, T.J.; Katzmarzyk, P.T.; Okely, A.D.; Connor Gorber, S.; et al. Systematic review of sedentary behaviour and health indicators in school-aged children and youth: An update. Appl. Physiol. Nutr. Metab. 2016, 41, S240–S265. [Google Scholar] [CrossRef] [PubMed]
- Son, J.W.; Ha, S.Y. Examining the influence of school forests on attitudes towards forest and aggression for elementary school students. J. Korean Inst. For. Recreat. 2013, 17, 49–57. [Google Scholar]
- Kaplan, R.; Kaplan, S. The Experience of Nature: A Psychological Perspective; Cambridge University Press: New York, NY, USA, 1989. [Google Scholar]
- Corraliza, J.A.; Collado, S.; Bethelmy, L. Nature as a moderator of stress in urban children. Procedia-Soc. Behav. Sci. 2012, 38, 253–263. [Google Scholar] [CrossRef]
- Korpela, K.; Kyttä, M.; Hartig, T. Restorative experience, self-regulation, and children’s place preferences. J. Environ. Psychol. 2002, 22, 387–398. [Google Scholar] [CrossRef]
- Song, C.; Ikei, H.; Miyazaki, Y. Physiological effects of nature therapy: A review of the research in Japan. Int. J. Environ. Res. Public Health 2016, 13, 781. [Google Scholar] [CrossRef] [PubMed]
- The National Law Information Center Forestry Culture and Recreation Act. Available online: http://www.law.go.kr/main.html (accessed on 20 March 2017).
- Howard, J. Integrating Outdoor Experience with Curricular Learning. Available online: https://www.wcmt.org.uk/sites/default/files/report-documents/Howard%20J%20Repor%202015%20Final.pdf (accessed on 10 March 2017).
- Muñoz, S.-A. Children in the Outdoors; Sustainable Development Research Centre: London, UK, 2009. [Google Scholar]
- McCormick, R. Does access to green space impact the mental well-being of children: A systematic review. J. Pediatr. Nurs. 2017, 37, 3–7. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.A.; Joung, D.; Yeom, D.G.; Kim, G.; Park, B.J. The effects of forest activities on attitudes toward forest, stress, self-esteem and mental health of children in community child centers. J. Korean Inst. For Recreat. 2015, 19, 51–58. [Google Scholar]
- Kim, J.Y.; Shin, C.S.; Yeoun, P.S.; Yi, J.Y.; Kim, M.R.; Kim, J.K.; Yoo, Y.H. Forest healing program impact on the mental health recovery of elementary school students. J. Korean Inst. For. Recreat. 2013, 17, 69–81. [Google Scholar] [CrossRef]
- Choi, J.-H.; Kim, K.-E. Eating attitude of children using community child center: A structural equation modeling approach. Adv. Sci. Technol. Lett. 2014, 47, 351–356. [Google Scholar]
- Song, M.K.; Bang, K.-S. A systematic review of forest therapy programs for elementary school students. Child Health Nurs. Res. 2017, 23, 300–311. [Google Scholar] [CrossRef]
- Kang, K.; Kim, S. Health problems and related factors of socially vulnerable school-age children in Seoul. J. Korean Soc. School Health 2017, 30, 181–193. [Google Scholar]
- Taelman, J.; Vandeput, S.; Spaepen, A.; Van Huffel, S. Influence of Mental Stress on Heart Rate and Heart Rate Variability. In Proceedings of the 4th European Conference of the International Federation for Medical and Biological Engineering (IFMBE), Antwerp, Belgium, 23–27 November 2008; pp. 1366–1369. [Google Scholar]
- Rosenberg, M. Society and the Adolescent Self-Image; Princeton University Press: Princeton, NJ, USA, 2015. [Google Scholar]
- Han, E.; Yoo, A.-J. Children’s and adolescents’ depression, attributional style and academic achievement. J. Korean Home Econ. Assoc. 1994, 32, 147–157. [Google Scholar]
- Kim, Y.-J. Effects of Solution-Focused Brief Group Counseling Program on the Isolated Elementary School Children’s Peer Relationship and Self-Esteem. Master’s Thesis, Korea National University of Education, Cheongju, Korea, 2005. [Google Scholar]
- Bahn, G.-H.; Shin, M.-S.; Cho, S.C.; Hong, K.-E. A preliminary study for the development of the assessment scale for ADHD in adolescents: Reliability and validity for cass(s). Korean J. Child Adolesc. Psychiatry 2001, 12, 218–224. [Google Scholar]
- Field, A. Discovering Statistics Using IBM SPSS Statistics, 4rd ed.; Sage: Los Angeles, CA, USA, 2013. [Google Scholar]
- Gignac, G.E.; Szodorai, E.T. Effect size guidelines for individual differences researchers. Personal. Individ. Differ. 2016, 102, 74–78. [Google Scholar] [CrossRef]
- Wolf, T.J.; Spiers, M.J.; Doherty, M.; Leary, E.V. The effect of self-management education following mild stroke: An exploratory randomized controlled trial. Top. Stroke Rehabil. 2017, 24, 345–352. [Google Scholar] [CrossRef] [PubMed]
- Reed, K.; Wood, C.; Barton, J.; Pretty, J.N.; Cohen, D.; Sandercock, G.R. A repeated measures experiment of green exercise to improve self-esteem in UK school children. PLoS ONE 2013, 8, e69176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barton, J.; Pretty, J. What is the best dose of nature and green exercise for improving mental health? A multi-study analysis. Environ. Sci. Technol. 2010, 44, 3947–3955. [Google Scholar] [CrossRef] [PubMed]
- Choi, S.-J.; Koh, Y.-S. Effect of combined program of horticultural therapy and forest therapy on self-esteem, social competence, and life respect of low-income family children at community children’s center. J. School Soc. Work 2014, 29, 671–699. [Google Scholar]
- Cho, Y.M.; Shin, W.S.; Yeoun, P.S. The influence of forest experience program length on sociality and psychology stability of children from low income families. J. Korean Inst. For. Recreat. 2011, 15, 97–103. [Google Scholar]
- Kim, M.H. A study on the positive effects of forest activities for children from economically underprivileged households on their emotional state, life satisfaction, and ego-resilience. Korean J. Child Stud. 2014, 35, 223–247. [Google Scholar] [CrossRef]
- Wood, C.; Gladwell, V.; Barton, J. A repeated measures experiment of school playing environment to increase physical activity and enhance self-esteem in UK school children. PLoS ONE 2014, 9, e108701. [Google Scholar] [CrossRef] [PubMed]
- Karcher, M.J. The study of mentoring in the learning environment (SMILE): A randomized evaluation of the effectiveness of school-based mentoring. Prev. Sci. 2008, 9, 99–113. [Google Scholar] [CrossRef] [PubMed]
- Kim, N.S. Designing youth mentoring for disadvantaged family. Korean J. Youth Stud. 2011, 18, 355–380. [Google Scholar]
- Rhodes, J.E. Stand by Me: The Risks and Rewards of Mentoring Today’s Youth; Harvard University Press: Cambridge, MA, USA, 2009. [Google Scholar]
- Yadav, V.; O’Reilly, M.; Karim, K. Secondary school transition: Does mentoring help ‘at-risk’ children? Community Pract. 2010, 83, 24–28. [Google Scholar] [PubMed]
- Duncan, M.J.; Clarke, N.D.; Birch, S.L.; Tallis, J.; Hankey, J.; Bryant, E.; Eyre, E.L. The effect of green exercise on blood pressure, heart rate and mood state in primary school children. Int. J. Environ. Res. Public Health 2014, 11, 3678–3688. [Google Scholar] [CrossRef] [PubMed]
- Sharma-Brymer, V.; Bland, D. Bringing nature to schools to promote children’s physical activity. Sports Med. 2016, 46, 955–962. [Google Scholar] [CrossRef] [PubMed]
- Lee, A.C.; Maheswaran, R. The health benefits of urban green spaces: A review of the evidence. J. Public Health 2011, 33, 212–222. [Google Scholar] [CrossRef] [PubMed]
- Barton, J.; Sandercock, G.; Pretty, J.; Wood, C. The effect of playground-and nature-based playtime interventions on physical activity and self-esteem in UK school children. Int. J. Environ. Health Res. 2015, 25, 196–206. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, L.; Murray, R. Forest School and its impacts on young children: Case studies in Britain. Urban For. Urban Green. 2007, 6, 249–265. [Google Scholar] [CrossRef]
- Louv, R. Last Child in the Woods: Saving Our Children from Nature-Deficit Disorder; Algonquin books of Chapel Hill: Chapel Hill, NC, USA, 2008. [Google Scholar]
- Tsunetsugu, Y.; Lee, J.; Park, B.-J.; Tyrväinen, L.; Kagawa, T.; Miyazaki, Y. Physiological and psychological effects of viewing urban forest landscapes assessed by multiple measurements. Landsc. Urban Plan. 2013, 113, 90–93. [Google Scholar] [CrossRef]
- Bang, K.-S.; Lee, I.; Kim, S.; Lim, C.S.; Joh, H.-K.; Park, B.-J.; Song, M.K. The Effects of a Campus Forest-Walking Program on Undergraduate and Graduate Students’ Physical and Psychological Health. Int. J. Environ. Res. Public Health 2017, 14, 728. [Google Scholar] [CrossRef] [PubMed]
- Park, B.J.; Tsunetsugu, Y.; Kasetani, T.; Kagawa, T.; Miyazaki, Y. The physiological effects of Shinrin-yoku (taking in the forest atmosphere or forest bathing): Evidence from field experiments in 24 forests across Japan. Environ. Health Prev. Med. 2009, 15, 18. [Google Scholar] [CrossRef] [PubMed]
- Lee, I.; Choi, H.; Bang, K.-S.; Kim, S.; Song, M.; Lee, B. Effects of forest therapy on depressive symptoms among adults: A systematic review. Int. J. Environ. Res. Public Health 2017, 14, 321. [Google Scholar] [CrossRef] [PubMed]
- Cho, Y.M.; Kim, D.J.; Lee, K.H.; Lee, H.E.; Lee, Y.J. A study on effect of forest related programs based on the meta-analysis. J. Korean Inst. For. Recreat. 2015, 19, 1–13. [Google Scholar]
- Akrimi, S.; Raynor, S.; Johnson, R.; Wylie, A. Evaluation of SHINE—Make every child count: A school-based community intervention programme. J. Public Ment. Health 2008, 7, 7–17. [Google Scholar] [CrossRef]
- Nursing and Midwifery Council. Standards for Competence for Registered Nurses. Available online: https://www.nmc.org.uk/globalassets/sitedocuments/standards/nmc-standards-for-competence-for-registered-nurses.pdf (accessed on 10 March 2017).
- Kim, S.; Bang, K.-S.; Kang, K.; Song, M.K. Mentoring experience of nursing students participating in a health promotion program for elementary school students. J. Korean Acad. Soc. Nurs. Educ. 2018, 24, 137–148. [Google Scholar]
- Leventhal, K.S.; DeMaria, L.M.; Gillham, J.E.; Andrew, G.; Peabody, J.; Leventhal, S.M. A psychosocial resilience curriculum provides the “missing piece” to boost adolescent physical health: A randomized controlled trial of Girls First in India. Soc. Sci. Med. 2016, 161, 37–46. [Google Scholar] [CrossRef] [PubMed]
- Rubenstein, L.M.; Hamilton, J.L.; Stange, J.P.; Flynn, M.; Abramson, L.Y.; Alloy, L.B. The cyclical nature of depressed mood and future risk: Depression, rumination, and deficits in emotional clarity in adolescent girls. J. Adolesc. 2015, 42, 68–76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Han, K.-T. The effect of nature and physical activity on emotions and attention while engaging in green exercise. Urban For. Urban Green. 2017, 24, 5–13. [Google Scholar] [CrossRef]


{kind=link}
| Session | Lecture | Forest Therapy | Program Duration (hours) |
|---|---|---|---|
| 1 | Program orientation Meeting with mentors Pre-test | 2 | |
| 2 | Understanding the relationship between physical and psychosocial health | Making a nickname for natural objects that resemble me Five senses experience in urban forest | 2 |
| 3 | Personal hygiene and eating habits | Physical activities in forest (I) -Forest walking and exercise | 2 |
| 4 | Internet overdependence | Playing with natural materials (I) -Making a paper fan with dry flowers and leaves | 2 |
| 5 | Forest day camp (I) | 4 | |
| 6 | Self-emotion awareness and expression | Playing with natural materials (II) -Rock-paper-scissors game with natural materials -Water carrying using leaves | 2 |
| 7 | Self-esteem | Self-expression activities with natural materials Making a bracelet of retinispora beads | 2 |
| 8 | Communication and peer relationships | Physical activities in forest (II) -Cloth volleyball -Traditional play | 2 |
| 9 | Forest day camp (II) | 4 | |
| 10 | Completion ceremony Discussion with mentors Post-test | 2 | |
| Characteristics/Variables | Categories | Exp. (n = 24) n (%) M ± SD | Cont. (n = 28) n (%) M ± SD | χ2/t/Z | p |
|---|---|---|---|---|---|
| Age (years) | 11.83 ± 0.82 | 11.75 ± 0.97 | 0.33 | 0.741 † | |
| Gender | Male | 8 (33.3) | 14 (50.0) | 1.47 | 0.225 ‡ |
| Female | 16 (66.7) | 14 (50.0) | |||
| Grade | 4th | 10 (41.7) | 11 (39.3) | 0.09 | 0.958 ‡ |
| 5th | 8 (33.3) | 9 (32.1) | |||
| 6th | 6 (25.0) | 8 (28.6) | |||
| Perceived health status | 4.04 ± 0.95 | 3.68 ± 1.12 | −1.31 | 0.191 § | |
| Self-esteem | 31.42 ± 5.48 | 31.86 ± 5.06 | −0.04 | 0.971 § | |
| Depression | 12.26 ± 7.99 | 9.39 ± 7.27 | −1.33 | 0.184 § | |
| Peer relationships | 79.27 ± 12.34 | 78.54 ± 13.77 | 0.20 | 0.845 † | |
| Attention deficit and hyperactivity | 15.09 ± 9.26 | 14.85 ± 11.57 | −0.66 | 0.507 § | |
| LF/HF ratio | 1.02 ± 0.58 | 1.67 ± 1.38 | −1.83 | 0.068 § | |
| Variables | Group | Pre-Test | Post-Test | Difference | t or Z | p | ES d/r |
|---|---|---|---|---|---|---|---|
| M ± SD | |||||||
| Perceived health status | Exp. | 4.04 ± 0.95 | 4.21 ± 0.83 | 0.17 ± 0.96 | 0.76 | 0.449 ‡ | 0.15 |
| Cont. | 3.48 ± 1.12 | 3.86 ± 0.97 | 0.18 ± 1.22 | 0.62 | 0.538 ‡ | 0.12 | |
| Self-esteem | Exp. | 31.42 ± 5.48 | 33.21 ± 4.35 | 1.79 ± 3.79 | 2.32 | 0.030 † | 0.47 |
| Cont. | 31.86 ± 5.06 | 30.43 ± 5.03 | −1.43 ± 4.73 | −1.12 | 0.265 ‡ | −0.21 | |
| Depression | Exp. | 12.26 ± 7.99 | 9.67 ± 6.44 | −2.74 ± 5.55 | −2.32 | 0.020 ‡ | −0.48 |
| Cont. | 9.39 ± 7.27 | 8.57 ± 6.86 | −0.82 ± 4.44 | −0.63 | 0.531 ‡ | −0.12 | |
| Peer relationships | Exp. | 79.27 ± 12.34 | 78.96 ± 11.11 | −0.43 ± 12.34 | −0.16 | 0.875 † | −0.03 |
| Cont. | 78.54 ± 13.77 | 80.36 ± 13.40 | 1.82 ± 9.10 | 1.19 | 0.236 ‡ | 0.22 | |
| Attention deficit and hyperactivity | Exp. | 15.09 ± 9.26 | 15.58 ± 11.99 | 0.22 ± 7.50 | 0.14 | 0.891 † | 0.03 |
| Cont. | 14.85 ± 11.57 | 14.14 ± 9.77 | −0.48 ± 9.85 | −0.25 | 0.802 † | −0.05 | |
| LF/HF ratio | Exp. | 1.02 ± 0.58 | 1.05 ± 0.61 | 0.03 ± 0.71 | 0.19 | 0.849 † | 0.04 |
| Cont. | 1.67 ± 1.38 | 1.45 ± 0.95 | −0.22 ± 0.98 | −1.20 | 0.241 † | −0.23 | |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bang, K.-S.; Kim, S.; Song, M.K.; Kang, K.I.; Jeong, Y. The Effects of a Health Promotion Program Using Urban Forests and Nursing Student Mentors on the Perceived and Psychological Health of Elementary School Children in Vulnerable Populations. Int. J. Environ. Res. Public Health 2018, 15, 1977. https://doi.org/10.3390/ijerph15091977
Bang K-S, Kim S, Song MK, Kang KI, Jeong Y. The Effects of a Health Promotion Program Using Urban Forests and Nursing Student Mentors on the Perceived and Psychological Health of Elementary School Children in Vulnerable Populations. International Journal of Environmental Research and Public Health. 2018; 15(9):1977. https://doi.org/10.3390/ijerph15091977
Chicago/Turabian StyleBang, Kyung-Sook, Sungjae Kim, Min Kyung Song, Kyung Im Kang, and Yeaseul Jeong. 2018. "The Effects of a Health Promotion Program Using Urban Forests and Nursing Student Mentors on the Perceived and Psychological Health of Elementary School Children in Vulnerable Populations" International Journal of Environmental Research and Public Health 15, no. 9: 1977. https://doi.org/10.3390/ijerph15091977