Quantitative Measures of Physical Risk Factors Associated with Work-Related Musculoskeletal Disorders of the Elbow: A Systematic Review

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
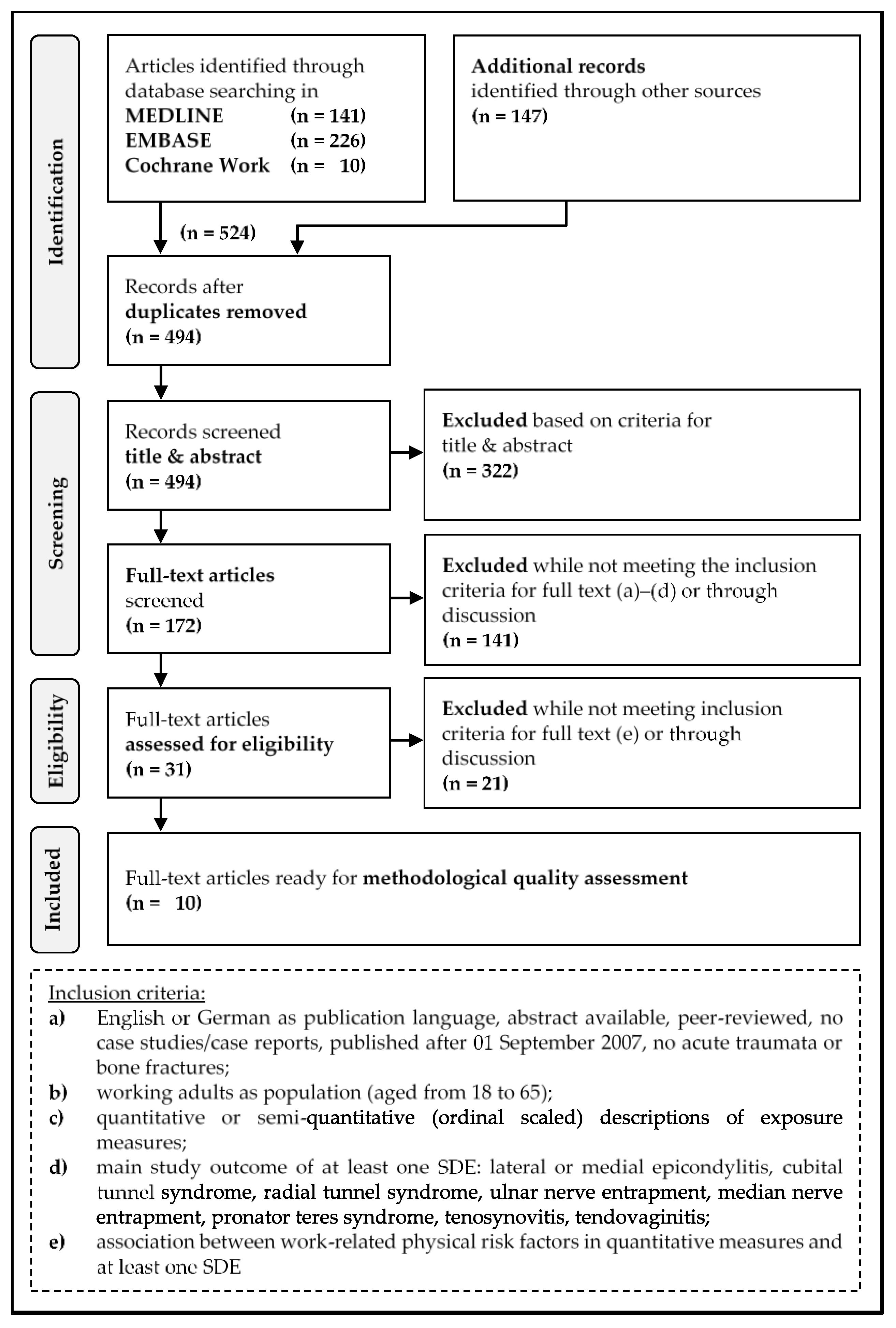
2.1. Literature Search and Selection Process
2.2. Inclusion Criteria
- (a)
- English or German as publication language, abstract available, peer-reviewed, no case studies/case reports, published after 01 September 2007, no acute traumata or bone fractures;
- (b)
- working adults as population (aged from 18 to 65);
- (c)
- quantitative or semi-quantitative (ordinal scaled) descriptions of exposure measures;
- (d)
- main study outcome of at least one SDE: LE or ME, cubital tunnel syndrome, radial tunnel syndrome, ulnar nerve entrapment, median nerve entrapment, pronator teres syndrome, tenosynovitis, tendovaginitis;
- (e)
- association between work-related physical risk factors in quantitative measures and at least one SDE.
2.3. Quality Assessment
- high (high frequency of positive values ‘+’ ≥67% corresponds to a score ≥12),
- medium (medium frequency of positive values ‘+’ 66% to 34% corresponds to a score 6 < 12), and
- low (low frequency of positive values ‘+’ ≤33% corresponds to a score ≤6).
2.4. Level of Evidence and Data Analysis
3. Results
3.1. Included Studies
3.2. Quality of the Included Studies
3.2.1. Methodological Quality
3.2.2. Quality of Exposure and Outcome Assessment
3.3. Physical Risk Factors Associated with SDEs
3.3.1. Force
3.3.2. Repetition
3.3.3. Posture/Movement
3.3.4. Vibration
3.3.5. Combined Exposures
3.3.6. Evidence of Sub-Categories of Exposure
- High evidence (n = 7): S2 (Forceful exertion), S4 (Manual load handling), S6 (Repetitiveness), S8 (Hand movements), S10 (Non-neutral posture), S13 (Force and repetition), S14 (Posture and force)
- Moderate evidence (n = 1): S16 (Posture and repetition and force)
- Low evidence (n = 3): S5 (High repetition), S9 (Forearm and elbow movements), S12 (Hand–arm vibration)
- Very low evidence (n = 5): S1 (Maximum force), S3 (Hand as tool), S7 (Overhead work), S11 (Body posture), S15 (Repetition and posture)
4. Discussion
4.1. Quality of the Included Studies
4.1.1. Study Design
4.1.2. Elbow Disorders and Outcome Assessment
4.1.3. Exposure Assessment
4.2. Significant and Non-Significant Risk Factors
4.2.1. Force
4.2.2. Repetition
4.2.3. Posture/Movement
4.2.4. Vibration
4.2.5. Combined Exposure
4.3. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| BMI | body mass index |
| CH | cohort study/studies |
| CIs | confidence intervals |
| CRS | case-referent study/studies |
| CSS | cross-sectional study/studies |
| EMG | electromyography |
| GRADE | Grading of Recommendations Assessment, Development and Evaluation |
| HAV | hand–arm vibrations |
| h/day | hours per day |
| HR | hazard ratio |
| IRR | incidence rate ratio |
| JEM | job exposure matrix |
| LE | lateral epicondylitis |
| ME | medial epicondylitis |
| MeSH | Medical Subject Headings |
| MVC | maximum voluntary contraction |
| MVE | maximal voluntary electric activity |
| OR | odds ratio |
| PICO | Population, Intervention, Comparison, Outcome |
| PR | prevalence ratios |
| PRISMA | Preferred Reporting Items for Systematic reviews and Meta-Analyses |
| Pronator | Pronator teres syndrome |
| Radial | Radial tunnel syndrome |
| S1 | exposure sub-category 1 |
| SDEs | specific disorders at the elbow |
| TCRS | triple case-referent study/studies |
| UN | ulnar neuropathy |
| WRULDs | work-related upper limb disorders |
References
- Health and Safety Executive (HSE). Work-Related Musculoskeletal Disorders (WRMSDs) Statistics in Great Britain 2017. Available online: www.hse.gov.uk/statistics/causdis/musculoskeletal/msd.pdf (accessed on 18 May 2018).
- European Agency for Safety and Health at Work (EU-OSHA). OSH in Figures: Work-Related Musculoskeletal Disorders in the EU-Facts and Figures; Publications Office of the European Union: Luxembourg, 2010; pp. 1–179. [Google Scholar]
- Bernard, B.P. Musculoskeletal Disorders and Work Place Factors—A Critical Review of Epidemiologic Evidence for Work-Related Musculoskeletal Disorders of the Neck, Upper Extremity and Low Back; U.S. Department of Health and Human Services, National Institute of Occupational Safety and Health (NIOSH): Cincinnati, OH, USA, 1997; pp. 1–590.
- Da Costa, B.R.; Vieira, E.R. Risk factors for work-related musculoskeletal disorders: A systematic review of recent longitudinal studies. Am. J. Ind. Med. 2010, 53, 285–323. [Google Scholar] [CrossRef] [PubMed]
- Descatha, A.; Albo, F.; Leclerc, A.; Carton, M.; Godeau, D.; Roquelaure, Y.; Petit, A.; Aublet-Cuvelier, A. Lateral epicondylitis and physical exposure at work? A review of prospective studies and meta-analysis. Arthritis Care Res. 2016, 68, 1681–1687. [Google Scholar] [CrossRef]
- Van Rijn, R.M.; Huisstede, B.M.; Koes, B.W.; Burdorf, A. Associations between work-related factors and specific disorders at the elbow: A systematic literature review. Rheumatology 2009, 48, 528–536. [Google Scholar] [CrossRef]
- Ellegast, R.; Hermanns, I.; Schiefer, C. Workload assessment in field using the ambulatory cuela system. In ICDHM 2009: Digital Human Modeling; Springer: Berlin/Heidelberg, Germany, 2009; pp. 221–226. [Google Scholar]
- Longo, A.; Meulenbroek, R.; Haid, T.; Federolf, P. Postural reconfiguration and cycle-to-cycle variability in patients with work-related musculoskeletal disorders compared to healthy controls and in relation to pain emerging during a repetitive movement task. Clin. Biomech. 2018, 54, 103–110. [Google Scholar] [CrossRef]
- Schiefer, C.; Kraus, T.; Ellegast, R.P.; Ochsmann, E. A technical support tool for joint range of motion determination in functional diagnostics—An inter-rater study. J. Occup. Med. Toxicol. 2015, 10, 16. [Google Scholar] [CrossRef]
- Wouda, F.J.; Giuberti, M.; Bellusci, G.; Veltink, P.H. Estimation of full-body poses using only five inertial sensors: An eager or lazy learning approach? Sensors 2016, 16, 2138. [Google Scholar] [CrossRef] [PubMed]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gotzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The prisma statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. J. Clin. Epidemiol. 2009, 62, e1–e34. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The prisma statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Mattioli, S.; Zanardi, F.; Baldasseroni, A.; Schaafsma, F.; Cooke, R.M.; Mancini, G.; Fierro, M.; Santangelo, C.; Farioli, A.; Fucksia, S.; et al. Search strings for the study of putative occupational determinants of disease. Occup. Environ. Med. 2010, 67, 436–443. [Google Scholar] [CrossRef] [PubMed]
- Melhorn, J.M.; Talmage, J.B.; Ackerman, W.E., III; Hyman, M.H. Ama Guides to the Evaluation of Disease and Injury Causation, 2nd ed.; American Medical Association: Chicago, IL, USA, 2014; pp. 1–792. [Google Scholar]
- PEROSH. Perosh—Osh Evidence Clearinghouse of Systematic Reviews: Partnership for European Research in Occupational Safety and Health. 2014. Available online: http://www.perosh.eu/wp-content/uploads/2013/06/PEROSH-Clearinghouse-Methods_Last-update-June-2014.pdf (accessed on 9 May 2016).
- Schaafsma, F.; Hulshof, C.; Verbeek, J.; Bos, J.; Dyserinck, H.; van Dijk, F. Developing search strategies in medline on the occupational origin of diseases. Am. J. Ind. Med. 2006, 49, 127–137. [Google Scholar] [CrossRef]
- Verbeek, J.; Salmi, J.; Pasternack, I.; Jauhiainen, M.; Laamanen, I.; Schaafsma, F.; Hulshof, C.; van Dijk, F. A search strategy for occupational health intervention studies. Occup. Environ. Med. 2005, 62, 682–687. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Tulder, M.; Furlan, A.; Bombardier, C.; Bouter, L. Updated method guidelines for systematic reviews in the cochrane collaboration back review group. Spine 2003, 28, 1290–1299. [Google Scholar] [CrossRef] [PubMed]
- Padula, R.S.; Comper, M.L.C.; Sparer, E.H.; Dennerlein, J.T. Job rotation designed to prevent musculoskeletal disorders and control risk in manufacturing industries: A systematic review. Appl. Ergon. 2017, 58, 386–397. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanderson, S.; Tatt, I.D.; Higgins, J.P. Tools for assessing quality and susceptibility to bias in observational studies in epidemiology: A systematic review and annotated bibliography. Int. J. Epidemiol. 2007, 36, 666–676. [Google Scholar] [CrossRef] [PubMed]
- Wong, W.C.; Cheung, C.S.; Hart, G.J. Development of a quality assessment tool for systematic reviews of observational studies (qatso) of hiv prevalence in men having sex with men and associated risk behaviours. Emerg. Themes Epidemiol. 2008, 5, 23. [Google Scholar] [CrossRef] [PubMed]
- Sulsky, S.I.; Carlton, L.; Bochmann, F.; Ellegast, R.; Glitsch, U.; Hartmann, B.; Pallapies, D.; Seidel, D.; Sun, Y. Epidemiological evidence for work load as a risk factor for osteoarthritis of the hip: A systematic review. PLoS ONE 2012, 7, e31521. [Google Scholar] [CrossRef] [PubMed]
- Boschman, J.S.; van der Molen, H.F.; Sluiter, J.K.; Frings-Dresen, M.H. Occupational demands and health effects for bricklayers and construction supervisors: A systematic review. Am. J. Ind. Med. 2011, 54, 55–77. [Google Scholar] [CrossRef]
- Du Prel, J.B.; Hommel, G.; Rohrig, B.; Blettner, M. Confidence interval or p-value?: Part 4 of a series on evaluation of scientific publications. Dtsch. Arztebl. Int. 2009, 106, 335–339. [Google Scholar] [CrossRef]
- Howard, J.; Piacentino, J.; MacMahon, K.; Schulte, P. Using systematic review in occupational safety and health. Am. J. Ind. Med. 2017, 60, 921–929. [Google Scholar] [CrossRef]
- Huguet, A.; Hayden, J.A.; Stinson, J.; McGrath, P.J.; Chambers, C.T.; Tougas, M.E.; Wozney, L. Judging the quality of evidence in reviews of prognostic factor research: Adapting the grade framework. Syst. Rev. 2013, 2, 71. [Google Scholar] [CrossRef]
- Van der Molen, H.F.; Foresti, C.; Daams, J.G.; Frings-Dresen, M.H.W.; Kuijer, P. Work-related risk factors for specific shoulder disorders: A systematic review and meta-analysis. Occup. Environ. Med. 2017, 74, 745–755. [Google Scholar] [CrossRef] [PubMed]
- Hayden, J.A.; Cote, P.; Bombardier, C. Evaluation of the quality of prognosis studies in systematic reviews. Ann. Intern. Med. 2006, 144, 427–437. [Google Scholar] [CrossRef]
- Hayden, J.A.; van der Windt, D.A.; Cartwright, J.L.; Cote, P.; Bombardier, C. Assessing bias in studies of prognostic factors. Ann. Intern. Med. 2013, 158, 280–286. [Google Scholar] [CrossRef] [PubMed]
- Viera, A.J.; Garrett, J.M. Understanding interobserver agreement: The kappa statistic. Fam. Med. 2005, 37, 360–363. [Google Scholar] [PubMed]
- Fan, Z.J.; Silverstein, B.A.; Bao, S.; Bonauto, D.K.; Howard, N.L.; Spielholz, P.O.; Smith, C.K.; Polissar, N.L.; Viikari-Juntura, E. Quantitative exposure-response relations between physical workload and prevalence of lateral epicondylitis in a working population. Am. J. Ind. Med. 2009, 52, 479–490. [Google Scholar] [CrossRef] [PubMed]
- Herquelot, E.; Bodin, J.; Roquelaure, Y.; Ha, C.; Leclerc, A.; Goldberg, M.; Zins, M.; Descatha, A. Work-related risk factors for lateral epicondylitis and other cause of elbow pain in the working population. Am. J. Ind. Med. 2013, 56, 400–409. [Google Scholar] [CrossRef] [PubMed]
- Nordander, C.; Ohlsson, K.; Akesson, I.; Arvidsson, I.; Balogh, I.; Hansson, G.A.; Stromberg, U.; Rittner, R.; Skerfving, S. Risk of musculoskeletal disorders among females and males in repetitive/constrained work. Ergonomics 2009, 52, 1226–1239. [Google Scholar] [CrossRef] [PubMed]
- Nordander, C.; Ohlsson, K.; Akesson, I.; Arvidsson, I.; Balogh, I.; Hansson, G.A.; Stromberg, U.; Rittner, R.; Skerfving, S. Exposure-response relationships in work-related musculoskeletal disorders in elbows and hands—A synthesis of group-level data on exposure and response obtained using uniform methods of data collection. Appl. Ergon. 2013, 44, 241–253. [Google Scholar] [CrossRef]
- Walker-Bone, K.; Palmer, K.T.; Reading, I.; Coggon, D.; Cooper, C. Occupation and epicondylitis: A population-based study. Rheumatology 2012, 51, 305–310. [Google Scholar] [CrossRef]
- Descatha, A.; Dale, A.M.; Jaegers, L.; Herquelot, E.; Evanoff, B. Self-reported physical exposure association with medial and lateral epicondylitis incidence in a large longitudinal study. Occup. Environ. Med. 2013, 70, 670–673. [Google Scholar] [CrossRef] [Green Version]
- Fan, Z.J.; Silverstein, B.A.; Bao, S.; Bonauto, D.K.; Howard, N.L.; Smith, C.K. The association between combination of hand force and forearm posture and incidence of lateral epicondylitis in a working population. Hum. Factors 2014, 56, 151–165. [Google Scholar] [CrossRef] [PubMed]
- Herquelot, E.; Gueguen, A.; Roquelaure, Y.; Bodin, J.; Serazin, C.; Ha, C.; Leclerc, A.; Goldberg, M.; Zins, M.; Descatha, A. Work-related risk factors for incidence of lateral epicondylitis in a large working population. Scand. J. Work Environ. Health 2013, 39, 578–588. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Svendsen, S.W.; Johnsen, B.; Fuglsang-Frederiksen, A.; Frost, P. Ulnar neuropathy and ulnar neuropathy-like symptoms in relation to biomechanical exposures assessed by a job exposure matrix: A triple case-referent study. Occup. Environ. Med. 2012, 69, 773–780. [Google Scholar] [CrossRef] [PubMed]
- Spahn, G.; Lipfert, J.-U.; Schmidt, A.; Maurer, C.; Dein, W.; Hartmann, B.; Hofmann, G.O.; Schiele, R. Risk factors for the lateral epicondylitis—Results from a case-control study. Arbeitsmed Sozialmed Umweltmed 2016, 51, 360–368. [Google Scholar]
- Moore, J.S.; Garg, A. The strain index: A proposed method to analyze jobs for risk of distal upper extremity disorders. Am. Ind. Hyg. Assoc. J. 1995, 56, 443–458. [Google Scholar] [CrossRef] [PubMed]
- Bao, S.; Howard, N.; Spielholz, P.; Silverstein, B. Quantifying repetitive hand activity for epidemiological research on musculoskeletal disorders—Part II: Comparison of different methods of measuring force level and repetitiveness. Ergonomics 2006, 49, 381–392. [Google Scholar] [CrossRef]
- Bao, S.; Silverstein, B. Estimation of hand force in ergonomic job evaluations. Ergonomics 2005, 48, 288–301. [Google Scholar] [CrossRef]
- Bao, S.; Spielholz, P.; Howard, N.; Silverstein, B. Quantifying repetitive hand activity for epidemiological research on musculoskeletal disorders—Part I: Individual exposure assessment. Ergonomics 2006, 49, 361–380. [Google Scholar] [CrossRef]
- McAtamney, L.; Nigel Corlett, E. Rula: A survey method for the investigation of work-related upper limb disorders. Appl. Ergon. 1993, 24, 91–99. [Google Scholar] [CrossRef]
- Thomsen, J.F.; Mikkelsen, S.; Andersen, J.H.; Fallentin, N.; Loft, I.P.; Frost, P.; Kaergaard, A.; Bonde, J.P.; Overgaard, E. Risk factors for hand-wrist disorders in repetitive work. Occup. Environ. Med. 2007, 64, 527–533. [Google Scholar] [CrossRef] [Green Version]
- Borg, G.A. Psychophysical bases of perceived exertion. Med. Sci. Sports Exerc. 1982, 14, 377–381. [Google Scholar] [CrossRef] [PubMed]
- Silverstein, B.A.; Fine, L.J.; Armstrong, T.J. Hand wrist cumulative trauma disorders in industry. Br. J. Ind. Med. 1986, 43, 779–784. [Google Scholar] [CrossRef] [PubMed]
- Latinovic, R.; Gulliford, M.C.; Hughes, R.A. Incidence of common compressive neuropathies in primary care. J. Neurol. Neurosurg. Psychiatry 2006, 77, 263–265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ranavolo, A.; Chini, G.; Silvetti, A.; Mari, S.; Serrao, M.; Draicchio, F. Myoelectric manifestation of muscle fatigue in repetitive work detected by means of miniaturized semg sensors. Int. J. Occup. Saf. Ergon. 2018, 24, 464–474. [Google Scholar] [CrossRef] [PubMed]
- Merletti, R.; Parker, P.J. Electromyography: Physiology, Engineering, and Non-Invasive Applications; Wiley-IEEE Press: New York, NY, USA, 2004. [Google Scholar]



{kind=link}
{kind=link}
| Criteria | Score | |
|---|---|---|
| Study population | ||
| 1 | Study groups are (exposed and unexposed) clearly defined | +/−/? |
| 2 | Participation ≥70% | +/−/? |
| 3 | Cases ≥50 | +/−/? |
| Assessment of exposure (adequate description) | ||
| 4 | Exposure definition | +/−/? |
| 5 | Assessment of exposure | +/−/? |
| 6 | Blind for outcome status | +/−/? |
| Assessment of outcome (specific disorder, adequate description) | ||
| 7 | Outcome definition | +/−/? |
| 8 | Assessment method | +/−/? |
| 9 | Blind for exposure status | +/−/? |
| Study design | ||
| 10 | Prospective design | +/−/? |
| 11 | Inclusion and exclusion criteria | +/−/? |
| 12 | Follow-up period ≥1 year | +/−/? |
| 13 | Information between completers vs. withdrawals | +/−/? |
| 14 | Research question * | +/−/? |
| Analysis and data presentation | ||
| 15 | Data presentation identifying confounders | +/−/? |
| 16 | Consideration of confounders | +/−/? |
| 17 | Control for confounding | +/−/? |
| 18 | Statistical methods * | +/−/? |
| Exposure Assessment | Score: Exposure * |
| Profession, job title, classification of occupation | 1 |
| Qualitative specification of exposure in different work activities (standing, sitting, static or dynamic movements) | 2 |
| Quantitative specification of exposure in different work activities/physical strains with information on intensity (e.g., repetition, force, load weight, awkward postures, or duration) | 3 |
| Quantitative specification of exposure (as above) with additional plausibility check (e.g., information on daily work output or special controls through video analysis) | 4 |
| Direct measurement or biomechanical model calculation of elbow strain with specification of quantitative information (e.g., repetition per time, force, load weight, awkward postures, holding time of awkward postures, amount/amplitudes, acceleration, velocity, torque) | 5 |
| Assessment of Outcome | Score: Diagnosis ** |
| Self-reported elbow pain without clinical check | 1 |
| Medical history/clinical questionnaire without clinical check or diagnosis | 2 |
| Clinically noticeable reduction of movement, clinical check, imaging procedure results and diagnosis | 3 |
| Reference | Study Design | Exposure Assessment Score * | Outcome Assessment Score * | General Methodological Quality Assessment (see Table 1 and chapter “Quality assessment” in ”Material and Methods” **) | |||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | 17 | 18 | Score | Quality | ||||
| Fan et al. (2009) [31] | CSS | 5 | 3 | + | + | − | + | + | + | + | + | − | + | + | + | − | + | + | + | + | − | 14 | high |
| Fan et al. (2014) [37] | CH | 5 | 3 | − | − | + | + | + | + | + | + | − | + | + | + | − | + | + | + | + | − | 13 | high |
| Herquelot et al. (2013b) [38] | CH | 3 | 3 | − | − | + | + | + | − | + | + | − | + | + | + | + | + | + | + | + | − | 13 | high |
| Descatha et al. (2013) [36] | CH | 3 | 3 | − | − | + | + | + | − | + | + | − | + | + | + | + | + | + | + | + | − | 13 | high |
| Svendsen et al. (2012) [39] | TCRS | 1 | 3 | − | − | + | + | + | − | + | + | − | − | + | − | + | + | + | + | + | + | 12 | high |
| Nordander et al. (2009) [33] | CSS | 3 | 3 | − | + | − | + | + | + | + | + | − | − | − | − | + | + | + | + | + | − | 11 | medium |
| Walker-Bone et al. (2012) [35] | CSS | 3 | 3 | − | − | + | + | + | − | + | + | − | − | + | − | − | + | + | + | + | − | 10 | medium |
| Herquelot et al. (2013a) [32] | CSS | 3 | 3 | − | − | + | + | + | − | + | + | − | − | + | − | − | + | + | + | + | − | 10 | medium |
| Nordander et al. (2013) [34] | CSS | 5 | 3 | − | + | − | + | + | + | + | + | − | − | − | − | − | + | + | + | + | − | 10 | medium |
| Spahn et al. (2016) [40] | CRS | 3 | 3 | + | + | + | − | − | − | + | + | − | − | + | − | − | + | + | + | + | − | 10 | medium |
| Total item score | 2 | 4 | 7 | 9 | 9 | 4 | 10 | 10 | 0 | 4 | 8 | 4 | 4 | 10 | 10 | 10 | 10 | 1 | 12 | high | |||
| Exposure (Main- and Sub-Category (S) *) | Significant Risk-Factor Specification | Reference | Outcome | Gender | Measure (95%-CI) | Adjustment | |||
|---|---|---|---|---|---|---|---|---|---|
| Force | S1 Maximum force | #1 | Maximum forceful efforts of the Hand >1 h/day | [40] | LE | Men | OR | 6.90 (2.70, 17.50) | (g) |
| LE | Women | OR | 9.60 (3.10, 30.40) | (g) | |||||
| S2 Forceful exertion | #2 | Hand in forceful grip on average ≥4 h/day | [36] | ME | - | OR | 3.80 (1.50, 9.60) | (a) | |
| LE/ME | - | OR | 2.80 (1.40, 5.80) | (a) | |||||
| #3 | <10% maximum voluntary contraction across a full working day | [39] | UN | - | OR | 2.73 (1.42, 5.25) | (h) | ||
| #4 | 10 to 29% maximum voluntary contraction across a full working day | [39] | UN | - | OR | 3.85 (2.04, 7.24) | (h) | ||
| S3 Hand as tool | #5 | Patting with the hand >1 h/day | [40] | LE | Men | OR | 13.80 (2.90, 66.10) | (g) | |
| S4 Manual load handling | #6 | Forceful lifting (≥4.5 kg) >0% of time | [31] | LE | - | OR | 2.65 (1.21, 5.83) | (i) | |
| #7 | Forceful lifting (≥4.5 kg) ≥2 times/min | [31] | LE | - | OR | 3.06 (1.28, 7.27) | (i) | ||
| Repetition | S5 High repetition | #8 | >3 motion sequences/sec or at least 10,000 times/h for >1 h/day | [40] | LE | Men | OR | 10.60 (4.00, 28.30) | (g) |
| LE | Women | OR | 11.00 (2.60, 45.10) | (g) | |||||
| S6 Repetitiveness | #9 | Doing repetitive tasks ≥4 h/day | [32] | LE | Women | OR | 2.46 (1.30, 4.65) | (a) | |
| [38] | LE | Men | IRR | 2.80 (1.20, 6.20) | (n) | ||||
| #10 | Wrist angular velocity (5°/s) in [%/(°/s)] | [34] | ME | - | PR | 0.10 (0.10, 0.20) | (g) | ||
| #11 | Repetitive elbow or wrist movements (≥4/min) ≥2.5 h/day | [39] | UN | - | OR | 2.22 (1.41, 3.51) | (j) | ||
| Posture/movement | S7 Overhead work | #12 | Overhead working >1 h/day | [40] | LE | Men | OR | 12.00 (3.20, 43.80) | (g) |
| S8 Hand movements | #13 | Frequent wrist bending or twisting on average 2 to 4 h/day | [36] | ME | - | OR | 4.90 (1.10, 20.70) | (a) | |
| LE/ME | - | OR | 3.90 (1.10, 13.80) | (a) | |||||
| #14 | Frequent wrist bending or twisting on average ≥4 h/day | [36] | LE | - | OR | 4.40 (1.50, 13.10) | (a) | ||
| ME | - | OR | 8.20 (2.40, 27.90) | (a) | |||||
| LE/ME | - | OR | 6.90 (2.40, 19.90) | (a) | |||||
| #15 | Frequent wrist bending ≥4 h/day and forearm rotating on average ≥2 h/day | [36] | LE | - | OR | 2.50 (1.10, 5.30) | (b) | ||
| ME | - | OR | 3.10 (1.40, 6.80) | (b) | |||||
| LE/ME | - | OR | 3.00 (1.60, 5.80) | (b) | |||||
| LE/ME | Men | OR | 2.80 (1.20, 6.20) | (b) | |||||
| LE/ME | Women | OR | 3.60 (1.20, 11.00) | (b) | |||||
| #16 | Wrist flexion (−40.0°) in [%/°] | [34] | LE | - | PR | 0.30 (0.04, 0.60) | (g) | ||
| #17 | Wrist flexion (−20.0°) in [%/°] | [34] | ME | - | PR | 0.08 (0.01, 0.10) | (g) | ||
| #18 | Wrist extension >1 h/day | [40] | LE | Men | OR | 12.00 (3.00, 47.90) | (g) | ||
| LE | Women | OR | 7.50 (1.80, 31.60) | (g) | |||||
| #19 | Wrist flexion >1 h/day | [40] | LE | Men | OR | 4.20 (1.20, 14.80) | (g) | ||
| #20 | Extreme wrist bending >2 h/day | [32] | LE | Men | OR | 2.27 (1.30, 3.97) | (a) | ||
| LE | Women | OR | 1.98 (1.04, 3.75) | (a) | |||||
| S9 Forearm and elbow movements | #21 | Elbow flexion/extension >2 h/day | [32] | LE | Men | OR | 2.41 (1.38, 4.22) | (a) | |
| LE | Women | OR | 2.65 (1.40, 5.02) | (a) | |||||
| #22 | Forearm rotating (also twisting, or screwing motion) ≥4 h/day | [36] | LE | - | OR | 2.70 (1.20, 6.20) | (a) | ||
| LE/ME | - | OR | 2.70 (1.30, 5.40) | (a) | |||||
| S10 Non-neutral posture | #23 | Non-neutral posture (elbow flexion >100°, or ≥near maximal pronation/supination; or wrist deviation (>5° radial, >10° ulnar) or >15° palmar/dorsal flexion) ≥2 h/day pronation/supination) | [39] | UN | - | OR | 1.82 (1.15, 2.89) | (j) | |
| #24 | Forearm rotation ≥45° for ≥45% time and duty cycle ≥10% of time | [37] | LE | - | HR | 3.10 (1.05, 9.15) | (a) | ||
| #25 | Forearm pronation ≥45° for ≥40% time and duty cycle ≥10% of time | [37] | LE | - | HR | 2.25 (1.09, 4.66) | (e) | ||
| #26 | Forearm supination ≥45° for ≥5% time | [31] | LE | - | OR | 2.25 (1.13, 4.50) | (i) | ||
| Vibration | S12 Hand-arm vibration | #27 | Hand-arm vibration: acceleration ≥3 m/s² ≥1 h/day | [39] | UN | - | OR | 2.19 (1.05, 4.56) | (j) |
| Combined Exposures | S13 Force and repetition | #28 | Maximum forceful efforts of the hand and repetition >1 h/day | [40] | LE | Men | OR | 14.70 (5.20, 41.50) | (g) |
| LE | Women | OR | 29.30 (3.40, 34.80) | (g) | |||||
| #29 | Frequency of forceful exertions (≥44.1 N or ≥4.5 kg) ≤1 to <5 times/min | [31] | LE | - | OR | 4.47 (1.57, 13.71) | (d) | ||
| #30 | Frequency of forceful exertions (≥44.1 N or ≥4.5 kg) ≥5 times/min | [31] | LE | - | OR | 5.17 (1.78, 15.02) | (d) | ||
| #31 | Duty cycle of forceful exertions (≥44.1 N or ≥4.5 kg) from ≤3 to <15% time | [31] | LE | - | OR | 3.36 (1.28, 8.84) | (i) | ||
| #32 | Duty cycle of forceful exertions (≥44.1 N or ≥4.5 kg) for ≥15% time | [31] | LE | - | OR | 3.00 (1.13, 7.96) | (i) | ||
| S14 Posture and force | #33 | Forearm supination ≥45° and forceful lifting (≥4.5 kg) in [% time] | [31] | LE | - | OR | 3.65 (1.47, 9.07) | (i) | |
| #34 | Forearm supination ≥45° ≥5% (duty cycle) and forceful lifting (≥4.5 kg) >0% of time | [31] | LE | - | OR | 2.98 (1.18, 7.55) | (d) | ||
| #35 | Forearm supination ≥45° for <5% time and lifting (≥4.5 kg) ≥3% of time | [37] | LE | - | HR | 2.09 (1.02, 4.27) | (a) | ||
| #36 | Forearm supination ≥45° for <5% time and any power grip (≥44.1 N) | [37] | LE | - | HR | 2.86 (1.41, 5.82) | (a) | ||
| #37 | Forearm rotation ≥45° for ≥45% time and any power grip (≥44.1 N) | [37] | LE | - | HR | 2.83 (1.16, 6.90) | (a) | ||
| #38 | Forearm pronation ≥45° for ≥40% time and any power grip (≥44.1 N) | [37] | LE | - | HR | 2.80 (1.35, 5.77) | (e) | ||
| #39 | Forearm pronation ≥45° for ≥40% time and lifting (≥4.5 kg) ≥3% of time | [37] | LE | - | HR | 2.50 (1.19, 5.24) | (e) | ||
| #40 | Forceful exertion (turning) >1 h/day | [40] | LE | Men | OR | 4.70 (1.40, 16.20) | (g) | ||
| #41 | Hard physical exertion (BORG Score 14 to 20) and 1 elbow movement | [32] | LE | Men | OR | 3.78 (1.85, 7.70) | (m) | ||
| #42 | Hard physical exertion (BORG Score 14 to 20) and 2 elbow movements | [32] | LE | Men | OR | 5.27 (1.93, 14.37) | (a) | ||
| (elbow movements = elbow flexion/extension >2 h/day and wrist bending >2 h/day | |||||||||
| High physical exertion with elbow flexion/extension >2 h/day and extreme wrist bending >2 h/day (at follow-up investigation) | [38] | LE | Men | IRR | 2.70 (1.10, 6.10) | (f) | |||
| High physical exertion with elbow flexion/extension >2 h/day and extreme | [38] | LE | Men | IRR | 3.20 (1.50, 6.40) | (f) | |||
| wrist bending >2 h/day (at baseline and at follow-up investigation) | LE | Women | IRR | 3.30 (1.40, 7.60) | (f) | ||||
| S15 Repetition and posture | #43 | Repetitive/constrained work with >30 s or >50% of cycle time (involved same | [33] | ME | Men | PR | 4.00 (1.10, 15.00) | (c) | |
| fundamental cycle) vs. >50% (working time) involved prolonged awkward postures | |||||||||
| #44 | Repetitive bending/straightening of the elbow >1 h/day | [35] | LE | - | OR | 2.50 (1.20, 5.30) | (k) | ||
| ME | - | OR | 5.30 (1.90, 14.90) | (k) | |||||
| Exposure (Main- and Sub-Category (S)) | Risk Factors | n | Number of Studies | Number of Cohorts | Outcome | Uni-/Multivariate Analyses | GRADE Factors (According to [26,27]) | GRADE Evidence | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| + | 0 | − | + | 0 | − | I | II * | III | IV | V | VI ** | VII | VIII | |||||||||
| Force | S1 | Maximum force | #1 | 197 | 1 [40] | 0 | LE | 2 | 0 | 0 | 1 | 2↓ | n. a. | 1↓ | 1↓ | ✔ | ↑ | † | Very low | |||
| S2 | Forceful exertion | #2 to #4, #46 to #49 | 8055 | 3 [34,36,39] | 1 | LE; ME LE/ME; UN | 2 | 7 | 0 | 2 | 1 | 2 | 2 | 2↓ | ✔ | ✔ | ✔ | 1↓ | ↑ | ↑ | High | |
| S3 | Hand as tool | #5 | 197 | 1 [40] | 0 | LE | 1 | 0 | 0 | 1 | 2↓ | n. a. | 1↓ | 1↓ | ✔ | ↑ | † | Very low | ||||
| S4 | Manual load handling | #6, #7, #50 to #53 | 930 | 3 [31,37,40] | 1 | LE | 0 | 1 | 0 | 2 | 3 | 0 | 3 | 1✔ | ✔ | ✔ | 1↓ | ✔ | ↑ | ↑ | High | |
| Rep-etition | S5 | High repetition | #8 | 197 | 1 [40] | 0 | LE | 2 | 0 | 0 | 1 | 2↓ | n. a. | ✔ | 1↓ | ✔ | ↑ | † | Low | |||
| S6 | Repetitiveness | #9 to #11, #54 to #57 | 11391 | 6 [31,32,34,37,38,39] | 2 | LE; ME; UN | 1 | 1 | 0 | 3 | 11 | 0 | 3 | 1✔ | 1↓ | ✔ | ✔ | ✔ | † | † | High | |
| Posture/Movement | S7 | Overhead work | #12 | 197 | 1 [40] | 0 | LE | 1 | 1 | 0 | 1 | 2↓ | n. a. | 1↓ | 1↓ | ✔ | ↑ | † | Very low | |||
| S8 | Hand movements | #13 to #20, #58 to 63 | 8399 | 6 [31,32,34,36,37,40] | 2 | LE; ME; LE/ME | 7 | 5 | 0 | 10 | 7 | 0 | 3 | 2↓ | ✔ | ✔ | 1↓ | 1↓ | ↑ | ↑ | High | |
| S9 | Forearm and elbow movements | #21, #22, #66 to #69 | 5014 | 3 [32,36,40] | 1 | LE; ME LE/ME | 4 | 7 | 0 | 0 | 4 | 0 | 2 | 2↓ | ✔ | ✔ | 1↓ | 1↓ | ↑ | † | Low | |
| S10 | Non-neutral posture | #23 to #26, #64, #65, #70 to #83 | 5029 | 3 [31,37,39] | 1 | LE; UN | 1 | 14 | 0 | 3 | 3 | 0 | 3 | 1✔ | ✔ | ✔ | 1↓ | ✔ | † | † | High | |
| S11 | Body posture | #84 to #86 | 197 | 1 [40] | 0 | LE | 0 | 6 | 0 | 1 | 2↓ | n. a. | 1↓ | 1↓ | ✔ | † | † | Very low | ||||
| Vibration | S12 | Hand–arm vibration | #27, #87 to #89 | 8203 | 3 [32,39,40] | 0 | LE; UN | 0 | 2 | 0 | 1 | 2 | 0 | 1 | 2↓ | ✔ | ✔ | ✔ | ✔ | † | † | Low |
| Combined exposure | S13 | Force and repetition | #28 to #32, #90 | 930 | 3 [31,37,40] | 1 | LE | 0 | 1 | 0 | 6 | 0 | 0 | 3 | 1✔ | ✔ | ✔ | 1↓ | ✔ | ↑ | ↑ | High |
| S14 | Posture and force | #33 to #42, #45, #91 to #118 | 4640 | 5 [31,32,37,38,40] | 2 | LE | 4 | 22 | 0 | 9 | 15 | 0 | 3 | 1✔ | 1↓ | ✔ | 1↓ | ✔ | ↑ | ↑ | High | |
| S15 | Repetition and posture | #43, #44 | 8690 | 2 [33,35] | 0 | LE; ME; Pronator; Radial | 3 | 6 | 0 | 1 | 2↓ | 1↓ | ✔ | 1↓ | ✔ | ↑ | † | Very low | ||||
| S16 | Posture and repetition and force | #119 to #133 | 611 | 1 [37] | 1 | LE | 0 | 15 | 0 | 3 | 1✔ | n. a. | ✔ | 1↓ | 1↓ | † | † | Moderate | ||||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Seidel, D.H.; Ditchen, D.M.; Hoehne-Hückstädt, U.M.; Rieger, M.A.; Steinhilber, B. Quantitative Measures of Physical Risk Factors Associated with Work-Related Musculoskeletal Disorders of the Elbow: A Systematic Review. Int. J. Environ. Res. Public Health 2019, 16, 130. https://doi.org/10.3390/ijerph16010130
Seidel DH, Ditchen DM, Hoehne-Hückstädt UM, Rieger MA, Steinhilber B. Quantitative Measures of Physical Risk Factors Associated with Work-Related Musculoskeletal Disorders of the Elbow: A Systematic Review. International Journal of Environmental Research and Public Health. 2019; 16(1):130. https://doi.org/10.3390/ijerph16010130
Chicago/Turabian StyleSeidel, David H., Dirk M. Ditchen, Ulrike M. Hoehne-Hückstädt, Monika A. Rieger, and Benjamin Steinhilber. 2019. "Quantitative Measures of Physical Risk Factors Associated with Work-Related Musculoskeletal Disorders of the Elbow: A Systematic Review" International Journal of Environmental Research and Public Health 16, no. 1: 130. https://doi.org/10.3390/ijerph16010130