Linking a History of Childhood Abuse to Adult Health among Canadians: A Structural Equation Modelling Analysis


Abstract
:1. Introduction
1.1. Sex Differences
1.2. Theoretical Models
2. Materials and Methods
2.1. Study Design
Data Source
2.2. Study Population
2.3. Study Measures
2.3.1. Child Abuse
2.3.2. Social Support
Stress
Physical Health
Mental Health
Sociodemographic Characteristics
2.4. Data Analysis
3. Results
3.1. Descriptive Statistics
3.2. Model Fit Testing in the Total Sample
3.3. Multiple-Group Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Leeb, R.T.; Paulozzi, L.J.; Melanson, C.; Simon, T.R.; Arias, I. Child Maltreatment Surveillance: Uniform Definitions for Public Health and Recommended Data Elements; Version 1.0; Centers for Disease Control and Prevention, National Center for Injury Prevention and Control: Atlanta, GA, USA, 2008.
- World Health Organization. Child Maltreatment Factsheet. Child Maltreatment. September 2016. Available online: https://www.who.int/en/news-room/fact-sheets/detail/child-maltreatment (accessed on 15 March 2019).
- World Health Organization. Child Maltreatment Infographic. Child Maltreatment: The Health Sector Responds. Available online: https://www.who.int/violence_injury_prevention/violence/child/en/ (accessed on 15 March 2019).
- Afifi, T.O.; MacMillan, H.L.; Boyle, M.; Taillieu, T.; Cheung, C.; Sareen, J. Child abuse and mental disorders in Canada. Can. Med. Assoc. J. 2014, 186, E324–E331. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; D’Arcy, C.; Meng, X. Maltreatment in childhood substantially increases the risk of adult depression and anxiety in prospective cohort studies: Systematic review, meta-analysis, and proportional attributable fractions. Psychol. Med. 2016, 46, 717–730. [Google Scholar] [CrossRef] [PubMed]
- Weber, S.; Jud, A.; Landolt, M.A. Quality of life in maltreated children and adult survivors of child maltreatment: A systematic review. Qual. Life Res. 2016, 25, 237–255. [Google Scholar] [CrossRef]
- Teicher, M.H.; Samson, J.A. Annual Research Review: Enduring neurobiological effects of childhood abuse and neglect. J. Child Psychol. Psychiatry 2016, 57, 241–266. [Google Scholar] [CrossRef] [PubMed]
- Guha, A.; Luebbers, S.; Papalia, N.; Ogloff, J. A follow-up study of mental health service utilisation in a cohort of 2433 sexually abused Australian children utilising five years of medical data. Child Abuse Negl. 2019, 90, 174–184. [Google Scholar] [CrossRef]
- Agnew-Blais, J.; Danese, A. Childhood maltreatment and unfavorable clinical outcomes in bipolar disorder: A systematic review and meta-analysis. Lancet Psychiatry 2016, 3, 342–349. [Google Scholar] [CrossRef]
- Aydin, B.; Akbas, S.; Turla, A.; Dundar, C. Depression and post-traumatic stress disorder in child victims of sexual abuse: Perceived social support as a protection factor. Nordic J. Psychiatry 2016, 70, 418–423. [Google Scholar] [CrossRef] [PubMed]
- Caslini, M.; Bartoli, F.; Crocamo, C.; Dakanalis, A.; Clerici, M.; Carrà, G. Disentangling the Association Between Child Abuse and Eating Disorders: A Systematic Review and Meta-Analysis. Psychosom. Med. 2016, 78, 79–90. [Google Scholar] [CrossRef]
- Dorahy, M.J.; Middleton, W.; Seager, L.; Williams, M.; Chambers, R. Child abuse and neglect in complex dissociative disorder, abuse-related chronic PTSD, and mixed psychiatric samples. J. Trauma Dissoc. 2016, 17, 223–236. [Google Scholar] [CrossRef] [PubMed]
- Infurna, M.R.; Reichl, C.; Parzer, P.; Schimmenti, A.; Bifulco, A.; Kaess, M. Associations between depression and specific childhood experiences of abuse and neglect: A meta-analysis. J. Affect. Disord. 2016, 190, 47–55. [Google Scholar] [CrossRef] [PubMed]
- Katz, L.F.; Stettler, N.; Gurtovenko, K. Traumatic Stress Symptoms in Children Exposed to Intimate Partner Violence: The Role of Parent Emotion Socialization and Children’s Emotion Regulation Abilities. Soc. Dev. 2016, 25, 47–65. [Google Scholar] [CrossRef]
- Kelly, D.L.; Rowland, L.M.; Patchan, K.M.; Sullivan, K.; Earl, A.; Raley, H.; Liu, F.; Feldman, S.; McMahon, R.P. Schizophrenia clinical symptom differences in women vs. men with and without a history of childhood physical abuse. Child Adolesc. Psychiatry Ment. Health 2016, 10, 5. [Google Scholar] [CrossRef] [Green Version]
- Klanecky, A.K.; McChargue, D.E.; Tuliao, A.P. Proposed pathways to problematic drinking via post-traumatic stress disorder symptoms, emotional dysregulation, and dissociative tendencies following child/adolescent sexual abuse. J. Addict. Dis. 2016, 35, 180–193. [Google Scholar] [CrossRef] [PubMed]
- Lauterbach, D.; Armour, C. Symptom Trajectories Among Child Survivors of Maltreatment: Findings from the Longitudinal Studies of Child Abuse and Neglect (LONGSCAN). J. Abnorm. Child Psychol. 2015, 44, 369–379. [Google Scholar] [CrossRef]
- Marwaha, S.; Gordon-Smith, K.; Broome, M.; Briley, P.M.; Perry, A.; Forty, L.; Craddock, N.; Jones, I.; Jones, L. Affective instability, childhood trauma and major affective disorders. J. Affect. Disord. 2016, 190, 764–771. [Google Scholar] [CrossRef]
- Pavlova, B.; Perroud, N.; Cordera, P.; Uher, R.; Dayer, A.; Aubry, J.M. Childhood maltreatment and comorbid anxiety in people with bipolar disorder. J. Affect. Disord. 2016, 192, 22–27. [Google Scholar] [CrossRef]
- Sellers, C.; McRoy, R.; O’Brien, K. Substance use and suicidal ideation among child welfare involved adolescents: A longitudinal examination. Addict. Behav. 2019, 93, 39–45. [Google Scholar] [CrossRef] [PubMed]
- Cascardi, M. From Violence in the Home to Physical Dating Violence Victimization: The Mediating Role of Psychological Distress in a Prospective Study of Female Adolescents. J. Youth Adolesc. 2016, 45, 777–792. [Google Scholar] [CrossRef] [PubMed]
- Hahn, A.M.; Simons, R.M.; Simons, J.S. Childhood Maltreatment and Sexual Risk Taking: The Mediating Role of Alexithymia. Arch. Sex. Behav. 2016, 45, 53–62. [Google Scholar] [CrossRef]
- Keene, A.C.; Epps, J. Childhood physical abuse and aggression: Shame and narcissistic vulnerability. Child Abuse Negl. 2016, 51, 276–283. [Google Scholar] [CrossRef]
- Meller, S.; Kuperman, K.L.; McCullough, C.; Shaffer, A. Adverse Effects of Childhood Emotional Maltreatment on Child Behavioral Outcomes. J. Aggress. Maltreat. Trauma 2016, 25, 127–144. [Google Scholar] [CrossRef]
- Vasilevski, V.; Tucker, A. Wide-Ranging Cognitive Deficits in Adolescents Following Early Life Management. Neuropsychology 2016, 30, 239–246. [Google Scholar] [CrossRef]
- Felitti, V.J.; Anda, R.F.; Nordenberg, D.; Williamson, D.F.; Spitz, A.M.; Edwards, V.; Marks, J.S. Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults: The Adverse Childhood Experiences (ACE) Study. Am. J. Prev. Med. 1998, 14, 245–258. [Google Scholar] [CrossRef]
- Brown, D.W.; Anda, R.F.; Felitti, V.J.; Edwards, V.J.; Malarcher, A.M.; Croft, J.B.; Giles, W.H. Adverse childhood experiences are associated with the risk of lung cancer: A prospective cohort study. BMC Public Health 2010, 10, 20. [Google Scholar] [CrossRef] [PubMed]
- Campbell, J.A.; Walker, R.J.; Egede, L.E. Associations Between Adverse Childhood Experiences, High-Risk Behaviors, and Morbidity in Adulthood. Am. J. Prev. Med. 2016, 50, 344–352. [Google Scholar] [CrossRef] [PubMed]
- Irish, L.; Kobayashi, I.; Delahanty, D.L. Long-term physical health consequences of childhood sexual abuse: A meta-analytic review. J. Pediatric Psychol. 2010, 35, 450–461. [Google Scholar] [CrossRef]
- Kamiya, Y.; Timonen, V.; Kenny, R.A. The impact of childhood sexual abuse on the mental and physical health, and healthcare utilization of older adults. Int. Psychogeriatr. 2016, 28, 415–422. [Google Scholar] [CrossRef]
- Mersky, J.P.; Topitzes, J.; Reynolds, A.J. Impact of adverse childhood experiences on health, mental health, and substance use in early childhood: A cohort study of urban, minority sample in the U.S. Child Abuse Negl. 2013, 37, 917–925. [Google Scholar] [CrossRef] [PubMed]
- Spitzer, C.; Wegert, S.; Wollenhaupt, J.; Wingenfeld, K.; Barnow, S.; Grabe, H.J. Gender-specific association between childhood trauma and rheumatoid arthritis: A case–control study. J. Psychosom. Res. 2013, 74, 296–300. [Google Scholar] [CrossRef]
- Oh, A.; Han, M.; Choi, Y.; Lau, S.; Shum, M. Exploring relationship among child maltreatment experience in childhood and behavior problems as young adults: Role of social support among college students in Hong Kong. Int. Soc. Work 2019, 62, 1011–1024. [Google Scholar] [CrossRef]
- Salazar, A.M.; Keller, T.E.; Courtney, M.E. Understanding social support’s role in the relationship between maltreatment and depression in youth with foster care experience. Child Maltreat. 2011, 16, 102–113. [Google Scholar] [CrossRef]
- Sokol, R.; Ennett, S.; Gottfredson, N.; Shanahan, M.; Poti, J.; Halpern, C.; Fisher, E. Child maltreatment and body mass index over time: The roles of social support and stress responses. Child. Youth Serv. Rev. 2019, 100, 214–220. [Google Scholar] [CrossRef]
- Sperry, D.M.; Widom, C.S. Child abuse and neglect, social support, and psychopathology in adulthood: A prospective investigation. Child Abuse Negl. 2013, 37, 415–425. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garami, J.; Valikhani, A.; Parkes, D.; Haber, P.; Mahlberg, J.; Misiak, B.; Frydecka, D.; Moustafa, A. Examining Perceived Stress, Childhood Trauma and Interpersonal Trauma in Individuals with Drug Addiction. Psychol. Rep. 2019, 122, 433–450. [Google Scholar] [CrossRef]
- Luecken, L.J.; Lemery, K.S. Early caregiving and physiological stress responses. Clin. Psychol. Rev. 2004, 24, 171–191. [Google Scholar] [CrossRef]
- Spinhoven, P.; Elzinga, B.M.; Van Hemert, A.M.; de Rooij, M.; Penninx, B.W. Childhood maltreatment, maladaptive personality types and level and course of psychological distress: A six-year longitudinal study. J. Af. Dis. 2016, 191, 100–108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cicchetti, D.; Toth, S.L. Child maltreatment. Ann. Rev. Clin. Psychol. 2005, 1, 409–438. [Google Scholar] [CrossRef] [PubMed]
- Fuller-Thompson, E.; Baird, S.L.; Dhrodia, R.; Brennenstuhl, S. The association between adverse childhood experiences and suicide attempts in a population-based study. Child Care Health Dev. 2016, 42, 725–734. [Google Scholar] [CrossRef] [PubMed]
- Fuller-Thomson, E.; Roane, J.L.; Brennenstuhl, S. Three Types of Adverse Childhood Experiences, and Alcohol and Drug Dependence Among Adults: An Investigation Using Population-Based Data. Subst. Use Misuse 2016, 51, 1451–1461. [Google Scholar] [CrossRef]
- Kristman-Valente, A.N.; Oesterle, S.; Hill, K.G.; Wells, E.A.; Epstein, M.; Jones, T.M.; Hawkins, J.D. The Relationship Between Interpersonal Violence Victimization and Smoking Behavior Across Time and by Gender. J. Soc. Work Pract. Addict. 2016, 16, 132–159. [Google Scholar] [CrossRef]
- Chen, G.; Gueta, K. Childhood Abuse and Mental Health Problems: Does Gender Matter? Psychiatr. Q. 2016, 87, 189–202. [Google Scholar] [CrossRef] [PubMed]
- Cronin, S.; Murphy, S.; Elklit, A. Investigating the relationship between childhood maltreatment and alcohol misuse in a sample of Danish young adults: Exploring gender differences. NAD Nordic Stud. Alcohol Drugs 2016, 33, 287–298. [Google Scholar] [CrossRef] [Green Version]
- Garcia, M.; Montalvo, I.; Creus, M.; Cabezas, Á.; Solé, M.; Algora, M.J.; Moreno, I.; Gutiérrez-Zotes, A.; Labad, J. Sex differences in the effect of childhood trauma on the clinical expression of early psychosis. Compr. Psychiatry 2016, 68, 86–96. [Google Scholar] [CrossRef]
- Soylu, N.; Ayaz, M.; Gökten, E.S.; Alpaslan, A.H.; Dönmez, Y.E.; Özcan, Ö.Ö.; Ayaz, A.B.; Tufan, A.E. Gender Differences in Sexually Abused Children and Adolescents: A Multicenter Study in Turkey. J. Child Sex. Abuse 2016, 25, 415–427. [Google Scholar] [CrossRef]
- Verona, E.; Murphy, B.; Javdari, S. Gendered pathways: Violent childhood maltreatment, sex exchange, and drug use. Psychol. Violence 2016, 6, 124–134. [Google Scholar] [CrossRef]
- Gokten, E.S.; Duman, N.S. Factors influencing the development of psychiatric disorders in the victims of sexual abuse: A study on Turkish children. Child. Youth Serv. Rev. 2016, 69, 49–55. [Google Scholar] [CrossRef]
- Bebbington, P.E.; Cooper, C.; Minot, S.; Brugha, T.S.; Traolach, S.; Jenkins, R.; Meltzer, H.; Dennis, M. Suicide attempts, gender, and sexual abuse: Data from the 2000 British psychiatric morbidity survey. Am. J. Psychiatry 2009, 166, 1135–1140. [Google Scholar] [CrossRef] [PubMed]
- Devries, K.M.; Mak, J.Y.T.; Child, J.C.; Falder, G.; Bacchus, L.J.; Astbury, J.; Watts, C.H. Childhood sexual abuse and suicidal behavior: A meta-analysis. Pediatrics 2014, 133, e1331–e1344. [Google Scholar] [CrossRef] [PubMed]
- Halfon, N.; Inkelas, M.; Hochstein, M. The Health Development Organization: An Organizational Approach to Achieving Child Health Development. Milbank Q. 2000, 78, 447–497. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Russ, S.A.; Larson, K.; Tullis, E.; Halfon, N. A Lifecourse Approach to Health Development: Implications for the Maternal and Child Health Research Agenda. Matern. Child Health J. 2014, 18, 497–510. [Google Scholar] [CrossRef]
- Statistics Canada. Statistics Canada. Canadian Community Health Survey (CCHS)—Mental Health Questionnaire, 30 November 2011; Ottawa, ON, Canada. Available online: www23.statcan.gc.ca/imdb-bmdi/instrument/5105_Q1_V3-eng.pdf (accessed on 15 December 2018).
- Brown, S.M.; Rienks, S.; McCrae, J.S.; Watamura, S.E. The co-occurrence of adverse childhood experiences among children investigated for child maltreatment: A latent class analysis. Child Abuse Negl. 2017, 87, 18–27. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.; Mennen, F.E.; Trickett, P.K. Patterns and correlates of co-occurrence among multiple types of child maltreatment. Child Fam. Soc. Work 2017, 22, 492–502. [Google Scholar] [CrossRef]
- Vachon, D.D.; Krueger, R.F.; Rogosch, F.A.; Cicchetti, D. Assessment of the harmful psychiatric and behavioral effects of different forms of child maltreatment. JAMA Psychiatry 2015, 72, 1135–1142. [Google Scholar] [CrossRef]
- Statistics Canada. Canadian Community Health Survey (CCHS)—Mental Health User Guide Microdata File; Statistics Canada: Ottawa, ON, Canada, 2013. [Google Scholar]
- Statistics Canada. Canadian Community Health Survey (CCHS)—Mental Health User Guide; Statistics Canada: Ottawa, ON, Canada, 2013. [Google Scholar]
- Cutrona, C.E.; Russell, D.W. The provisions of social relationships and adaptation to stress. Adv. Pers. Relatsh. 1987, 1, 37–67. [Google Scholar]
- Carol, J. A validation of the Social Provisions Scale: The SPS-10 items (Article in French: Une validation de la forme abrégée de l’Échelle de provisions sociales: l’ÉPS-10 items). St. Ment. Québec 2013, 38, 297–318. [Google Scholar]
- Kline, R.B. Principles and Practice of Structural Equation Modeling, 4th ed.; The Guilford Press: New York, NY, USA, 2015. [Google Scholar]
- DiStefano, C.; Morgan, G.B. A Comparison of Diagonal Weighted Least Squares Robust Estimation Techniques for Ordinal Data. Struct. Equ. Modeling A Multidiscip. J. 2014, 21, 425–438. [Google Scholar] [CrossRef]
- Bentler, P.M.; Bonett, D.G. Significance tests and goodness of fit in the analysis of covariance structures. Psychol. Bull. 1980, 88, 588–606. [Google Scholar] [CrossRef]
- Shah, R.; Goldstein, S.M. Use of structural equation modeling in operations management research: Looking back and forward. J. Oper. Manag. 2006, 24, 148–169. [Google Scholar] [CrossRef]
- Schreiber, J.B.; Stage, F.K.; King, J.; Nora, A.; Barlow, E. Reporting Structural Equation Modeling and Confirmatory Factor Analysis Results: A Review. J. Educ. Res. 2006, 99, 323–337. [Google Scholar] [CrossRef]
- Everaerd, D.; Klumpers, F.; Zwiers, M.; Guadalupe, T.; Franke, B.; van Oostrom, I.; Schene, A.; Fernández, G.; Tendolkar, I. Childhood abuse and deprivation are associated with distinct sex-dependent differences in brain morphology. Neuropsychopharmacology 2016, 41, 1716–1723. [Google Scholar] [CrossRef]
- Teicher, M.H.; Samson, J.A.; Anderson, C.M.; Ohashi, K. The effects of childhood maltreatment on brain structure, function and connectivity. Nat. Rev. Neurosci. 2016, 17, 652. [Google Scholar] [CrossRef] [PubMed]
- Edwards, V.J.; Anda, R.F.; Nordenberg, D.F.; Felitti, V.J.; Williamson, D.F.; Wright, J.A. Bias assessment for child abuse survey: Factors affecting probability of response to a survey about childhood abuse. Child Abuse Negl. 2001, 25, 307–312. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | N (%) | Variable | N (%) |
|---|---|---|---|
| SEX Male Female | 12,381 (49.3) 12,732 (50.7) | OCCUPATION Employed Unemployed | 15,822 (63.1) 8789 (34.9) |
| AGE GROUP | Unable to work | 502 (2.0) | |
| 15–34 35–54 55–74 ≥75 | 7936 (31.6) 8865 (35.3) 6580 (26.2) 1732 (6.9) | PERSONAL INCOME <$20,000 $20,000–$49,999 ≥$50,000 | 8238 (32.8) 9743 (38.8) 7132 (28.4) |
| MARITAL STATUS Married Common-law Widowed Divorced/Separated Single | 12,381 (49.3) 2712 (10.8) 1230 (4.9) 2009 (8.0) 6781 (27) | HOUSEHOLD INCOME <$20,000 $20,000–$79,999 ≥$80,000 | 1155 (4.6) 12,080 (48.1) 11,878 (47.3) |
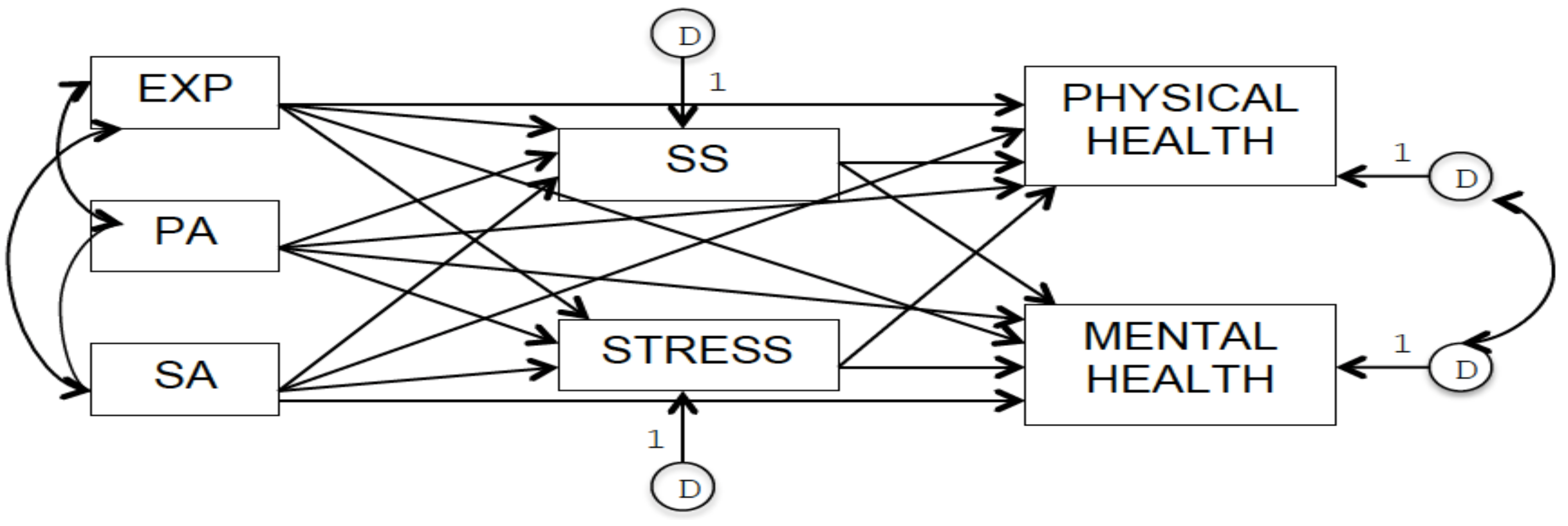
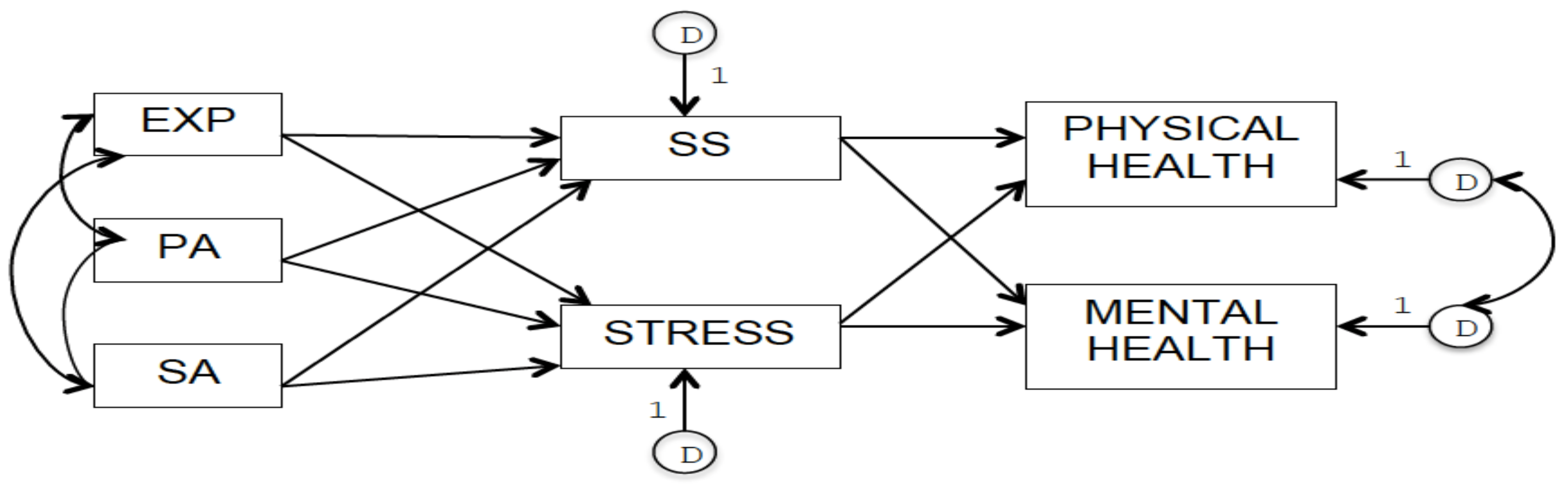
| Parameter | Model 1 | Model 2 | ||
|---|---|---|---|---|
| Unst. | Stand. | Unst. | Stand. | |
| EXP → PHYSIC_H EXP → MENTAL_H | −0.04 −0.09 | −0.01 −0.03 | - - | - - |
| PA → PHYSIC_H PA → MENTAL_H SA → PHYSIC_H SA → MENTAL_H | −0.14 −0.15 −0.24 −0.25 | −0.04 −0.04 −0.06 −0.07 | - - - - | - - - - |
| EXP → SS EXP → STRESS PA → SS PA → STRESS SA → SS SA → STRESS | −0.71 0.21 −1.16 0.19 −0.68 0.33 | −0.06 0.08 −0.07 0.05 −0.04 0.08 | −0.82 0.24 −1.44 0.24 −1.13 0.41 | −0.07 0.08 −0.09 0.06 −0.06 0.10 |
| SS → PHISIC_H SS → MENTAL_H STRESS → PHYSIC_H STRESS → MENTAL_H | 0.05 0.06 −0.17 −0.27 | 0.21 0.28 −0.17 −0.29 | 0.05 0.06 −0.19 −0.30 | 0.23 0.30 −0.19 −0.33 |
| CV EXPPA CV EXPSA CV PASA CVDPHYSIC_HDMENTAL_H | 0.04 0.02 0.02 0.32 | 0.39 0.23 0.28 0.34 | 0.04 0.02 0.02 0.31 | 0.39 0.23 0.28 0.33 |
| Indirect Path | Estimations | |
|---|---|---|
| Model 1 | Model 2 | |
| EXP → SS → PHYSIC_H | −0.715 (0.05) = −0.03 | −0.82 (0.05) = −0.04 |
| PA → SS → PHYSIC_H | −1.16 (0.05) = −0.06 | −1.44 (0.05) = −0.07 |
| SA → SS → PHYSIC_H | −0.68 (0.05) = −0.03 | −1.13 (0.05) = −0.06 |
| EXP → SS → MENTAL_H | −0.715 (0.06) = −0.04 | −0.82 (0.065) = −0.05 |
| PA → SS → MENTAL_H | −1.16 (0.06) = −0.07 | −1.44 (0.065) = −0.09 |
| SA → SS → MENTAL_H | −0.68 (0.06) = −0.04 | −1.13 (0.065) = −0.07 |
| EXP → STRESS → PHYSIC_H | 0.215 (−0.17) = 0.04 | 0.24 (−0.19) = −0.04 |
| PA → STRESS → PHYSIC_H | 0.19 (−0.17) = −0.03 | 0.24 (−0.19) = −0.04 |
| SA → STRESS → PHYSIC_H | 0.33 (−0.17) = −0.06 | 0.41 (−0.19) = −0.08 |
| EXP → STRESS → MENTAL_H | 0.215 (−0.27) = −0.06 | 0.24 (−0.30) = −0.07 |
| PA → STRESS → MENTAL_H | 0.19 (−0.27) = −0.05 | 0.24 (−0.30) = −0.07 |
| SA → STRESS → MENTAL_H | 0.33 (−0.27) = −0.09 | 0.41 (−0.30) = −0.12 |
| Fit Index | Male Subsample (nm = 11,340) | Female Subsample (nf = 13,773) |
|---|---|---|
| SRMR | 0.02 | 0.03 |
| GFI–AGFI | 0.99–0.98 | 0.99–0.97 |
| NFI | 0.97 | 0.96 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cameranesi, M.; Lix, L.M.; Piotrowski, C.C. Linking a History of Childhood Abuse to Adult Health among Canadians: A Structural Equation Modelling Analysis. Int. J. Environ. Res. Public Health 2019, 16, 1942. https://doi.org/10.3390/ijerph16111942
Cameranesi M, Lix LM, Piotrowski CC. Linking a History of Childhood Abuse to Adult Health among Canadians: A Structural Equation Modelling Analysis. International Journal of Environmental Research and Public Health. 2019; 16(11):1942. https://doi.org/10.3390/ijerph16111942
Chicago/Turabian StyleCameranesi, Margherita, Lisa M. Lix, and Caroline C. Piotrowski. 2019. "Linking a History of Childhood Abuse to Adult Health among Canadians: A Structural Equation Modelling Analysis" International Journal of Environmental Research and Public Health 16, no. 11: 1942. https://doi.org/10.3390/ijerph16111942