Effect of Stress on the Work Ability of Aging American Workers: Mediating Effects of Health


Abstract
:1. Introduction
2. Methods and Materials
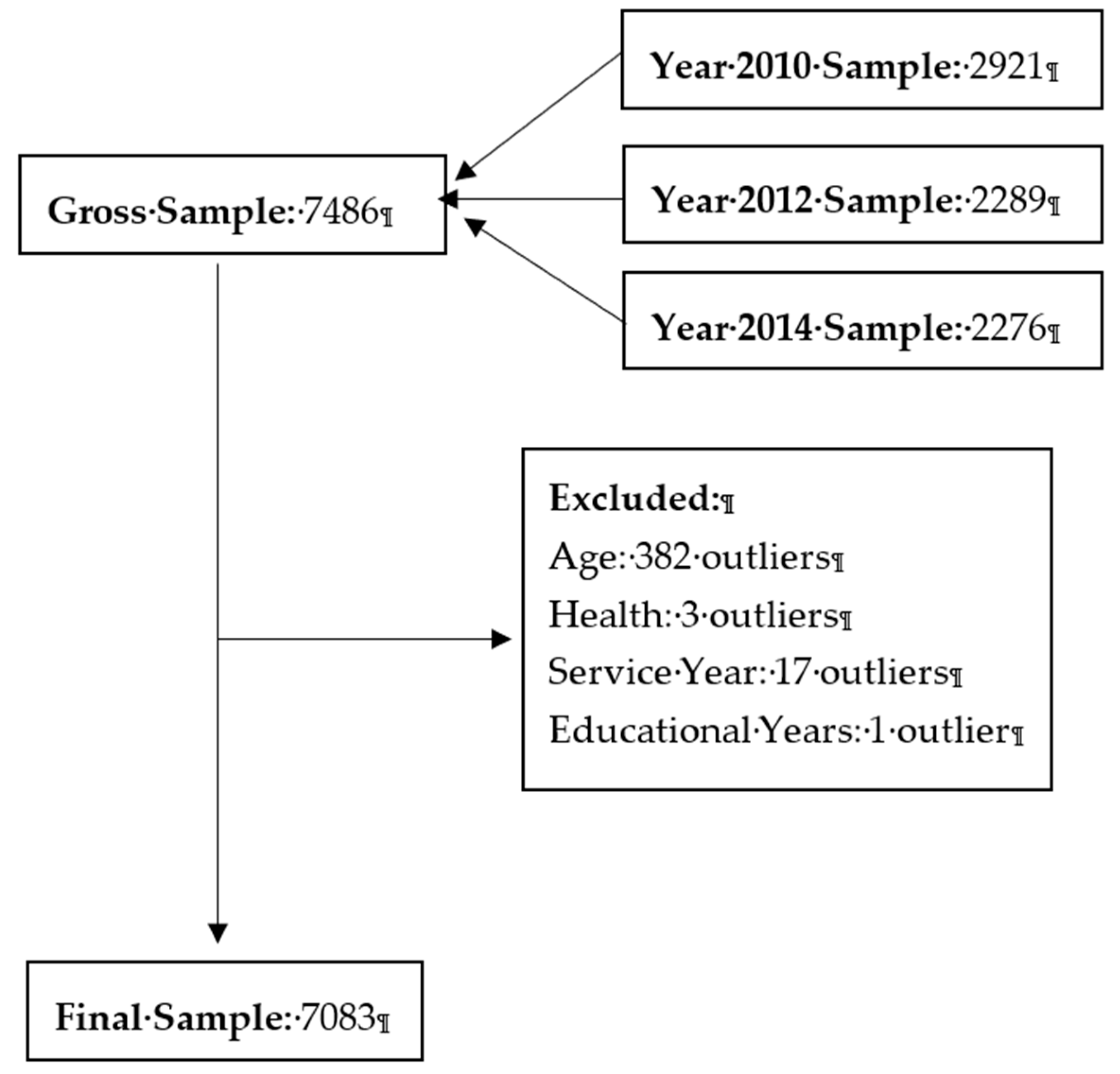
2.1. Sample
2.2. Data Manipulation
2.3. Definitions of Variables
2.4. Method
3. Empirical Results
3.1. Descriptive Statistics
3.2. Correlation Matrix
3.3. Regression Analysis
3.4. Mediation Analysis
3.5. Robustness Check
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Walker, A. Managing an Ageing Workforce: A Guide to Good Practice; European Foundation for the Improvement of Living and Working Conditions: Dublin, Ireland; Office for Official Publications of the European Communities: Luxembourg, 1999. [Google Scholar]
- Ilmarinen, J. The ageing workforce—Challenges for occupational health. Occup. Med. 2006, 56, 362–364. [Google Scholar] [CrossRef]
- OECD. Reforms for an Ageing Society; Sourceoecd Social Issues/Migration/Health; OECD: Paris, France, 2000; pp. 1–220. [Google Scholar]
- Redaymulvey, G. Working Beyond 60: Key Policies and Practices in Europe. Ind. Labor Relat. Rev. 2007, 60, 85. [Google Scholar]
- Ilmarinen, J.; Rantanen, J. Promotion of work ability during ageing. Am. J. Ind. Med. 1999, 36, 21–23. [Google Scholar] [CrossRef]
- Supporting the aging workforce: A review and recommendations for workplace intervention research. Annu. Rev. Organ. Psychol. Organ. Behav. 2015, 2, 351–381. [CrossRef]
- Maertens, J.A.; Putter, S.E.; Chen, P.Y.; Diehl, M.; Huang, Y.H. Physical Capabilities and Occupational Health of Older Workers. In The Oxford Handbook of Work and Aging; Oxford University Press: Oxford, UK, 2012. [Google Scholar] [CrossRef]
- Blok, M.; De Looze, M.P. What is the evidence for less shift work tolerance in older workers. Ergonomics 2011, 54, 221–232. [Google Scholar] [CrossRef]
- Hedge, J.W.; Borman, W.C. Work and aging. In The Oxford Handbook of Organizational Psychology; Oxford University Press: London, UK, 2012; pp. 1245–1283. [Google Scholar]
- Lichtman, S.M. The physiological aspects of aging. In Fourteen Steps in Managing an Aging Workforce; Dennis, H., Ed.; Lexington Books: Lexington, MA, USA, 1988; pp. 39–51. [Google Scholar]
- Soto, C.J.; John, O.P. Development of big five domains and facets in adulthood: Mean-level age trends and broadly versus narrowly acting mechanisms. J. Personal. 2012, 80, 881–914. [Google Scholar] [CrossRef]
- Soto, C.J.; John, O.P.; Gosling, S.D.; Jeff, P. Age differences in personality traits from 10 to 65: Big Five domains and facets in a large cross-sectional sample. J. Personal. Soc. Psychol. 2011, 100, 330–348. [Google Scholar] [CrossRef]
- Zwart, B.C.H.D.; Frings-Dresen, M.H.W.; Dijk, F.J.H.V. Physical workload and the ageing worker: A review of the literature. Int. Arch. Occup. Environ. Health 1996, 68, 1–12. [Google Scholar] [CrossRef]
- Topcic, M.; Baum, M.; Kabst, R. Are high-performance work practices related to individually perceived stress? A job demands-resources perspective. Int. J. Hum. Res. Manag. 2016, 27, 45–66. [Google Scholar] [CrossRef]
- Costa, G.; Sartori, S. Ageing, working hours and work ability. Ergonomics 2007, 50, 1914–1930. [Google Scholar] [CrossRef]
- Costanza, R.; Kubiszewski, I.; Giovannini, E.; Lovins, H.; Mcglade, J.; Pickett, K.E.; Ragnarsdóttir, K.; Roberts, D.; De, V.R.; Wilkinson, R. Development: Time to leave GDP behind. Nature 2014, 505, 283–285. [Google Scholar] [CrossRef] [Green Version]
- Goetzel, R.Z.; Long, S.R.; Ozminkowski, R.J.; Hawkins, K.; Wang, S.; Lynch, W.L. Health, Absence, Disability, and Presenteeism Cost Estimates of Certain Physical and Mental Health Conditions Affecting, U.S. Employers. J. Occup. Environ. Med. 2004, 46, 398–412. [Google Scholar] [CrossRef]
- Vänni, K.; Virtanen, P.; Luukkaala, T.; Nygård, C.-H. Relationship between perceived work ability and productivity loss. Int. J. Occup. Saf. Ergon. 2012, 18, 299–309. [Google Scholar] [CrossRef]
- Mcgonagle, A.K.; Fisher, G.G.; Barnes-Farrell, J.L.; Grosch, J.W. Individual and work factors related to perceived work ability and labor force outcomes. J. Appl. Psychol. 2015, 100, 376–398. [Google Scholar] [CrossRef]
- Koolhaas, W.; Klink, J.J.L.V.D.; Boer, M.R.D.; Groothoff, J.W.; Brouwer, S. Chronic health conditions and work ability in the ageing workforce: The impact of work conditions, psychosocial factors and perceived health. Int. Arch. Occup. Environ. Health 2014, 87, 433. [Google Scholar] [CrossRef]
- National institutes of Health U.S. Department of Health and Human Services. Growing Older in America: The Health and Retirement Study; Karp, F., Ed.; National Institutes of Health U.S. Department of Health and Human Services: Bethesda, MD, USA, 2007. [Google Scholar]
- Health and Retirement Study. Produced and Distributed by the University of Michigan with Funding from the National Institute on Aging (Grant Number NIA U01AG009740); ([2010 HRS core]); Health and Retirement Study, Ed.; Health and Retirement Study: Ann Arbor, MI, USA, 2010. [Google Scholar]
- Smith, J.; Fisher, G.; Ryan, L.; Clarke, P.; House, J.; Weir, D. Psychosocial and Lifestyle Questionnaire 2006–2010 Documentation Report Core Section LB; The HRS Psychosocial Working Group, Ed.; University of Michigan: Ann Arbor, MI, USA, 2013. [Google Scholar]
- Juster, F.T.; Suzman, R. An Overview of the Health and Retirement Study. J. Hum. Res. 2016, 30, S7–S56. [Google Scholar] [CrossRef]
- Troxel, W.M.; Matthews, K.A.; Bromberger, J.T.; Kim, S.T. Chronic stress burden, discrimination, and subclinical carotid artery disease in African American and Caucasian women. Health Psychol. Off. J. Divis. Health Psychol. Am. Psychol. Assoc. 2003, 22, 300–309. [Google Scholar] [CrossRef]
- Löve, J.; Holmgren, K.; Torén, K.; Hensing, G. Can work ability explain the social gradient in sickness absence: A study of a general population in Sweden. BMC Public Health 2012, 12, 163. [Google Scholar] [CrossRef]
- López, P. Aging and work ability from the gender perspective. Revista Cubana de Salud y Trabajo 2010, 11, 48–53. [Google Scholar]
- Padula, R.S.; da Silva Valente Ldo, S.; de Moraes, M.V.; Chiavegato, L.D.; Cabral, C.M. Gender and age do not influence the ability to work. Work 2012, 41, 4330–4332. [Google Scholar] [Green Version]
- Meer, L.V.D.; Leijten, F.R.M.; Heuvel, S.G.V.D.; Ybema, J.F.; Wind, A.D.; Burdorf, A.; Geuskens, G.A. Erratum to: Company Policies on Working Hours and Night Work in Relation to Older Workers’ Work Ability and Work Engagement: Results from a Dutch Longitudinal Study with 2 Year Follow-Up. J. Occup. Rehabil. 2016, 26, 182. [Google Scholar] [CrossRef]
- Chung, J.; Park, J.; Cho, M.; Park, Y.; Kim, D.; Yang, D.; Yang, Y. A study on the relationships between age, work experience, cognition, and work ability in older employees working in heavy industry. J. Phys. Ther. Sci. 2015, 27, 155–157. [Google Scholar] [CrossRef] [Green Version]
- Demakakos, P.; Nazroo, J.; Breeze, E.; Marmot, M. Socioeconomic status and health: The role of subjective social status. Soc. Sci. Med. 2008, 67, 330–340. [Google Scholar] [CrossRef] [Green Version]
- Archana, S.-M.; Marmot, M.G.; Adler, N.E. Does Subjective Social Status Predict Health and Change in Health Status Better Than Objective Status? Psychosom. Med. 2005, 67, 855–861. [Google Scholar]
- Ghaddar, A.; Ronda, E.; Nolasco, A. Work ability, psychosocial hazards and work experience in prison environments. Occup. Med. 2011, 61, 503–508. [Google Scholar] [CrossRef] [Green Version]
- Mirowsky, J.; Ross, C.E. Education, Social Status, and Health; Aldine Transaction: Plano, TX, USA, 2003; pp. 71–125. [Google Scholar]
- Jussi, I. Work ability-a comprehensive concept for occupational health research and prevention. Scand. J. Work Environ. Health 2009, 35, 1–5. [Google Scholar]
- Iacobucci, D. Mediation analysis and categorical variables: The final frontier. J. Consum. Psychol. 2012, 22, 582–594. [Google Scholar] [CrossRef]
- Bojana, K.; Milan, M.; Rajna, G.; Ljiljana, B.; Andrea, R.; Jadranka, M. Work-related stress and work ability among Croatian university hospital midwives. Midwifery 2011, 27, 146–153. [Google Scholar]
- Airila, A.; Hakanen, J.J.; Schaufeli, W.B.; Luukkonen, R.; Punakallio, A.; Lusa, S. Are job and personal resources associated with work ability 10 years later? The mediating role of work engagement. Work Stress 2014, 28, 87–105. [Google Scholar] [CrossRef]
- Williamson, D.L.; Carr, J. Health as a resource for everyday life: Advancing the conceptualization. Crit. Public Health 2009, 19, 107–122. [Google Scholar] [CrossRef]
- Bakker, A.B.; Demerouti, E. The Job Demands-Resources model: State of the art. J. Manag. Psychol. 2007, 22, 309–328. [Google Scholar] [CrossRef]
- Demerouti, E.; Bakker, A.B.; Nachreiner, F.; Schaufeli, W.B. The job demands-resources model of burnout. J. Appl. Psychol. 2001, 86, 499–512. [Google Scholar] [CrossRef]
- Dahl, E. Social mobility and health: Cause or effect? BMJ Clin. Res. 1996, 313, 435–436. [Google Scholar] [CrossRef]
- Simandan, D. Rethinking the health consequences of social class and social mobility. Soc. Sci. Med. 2018, 77, 258–261. [Google Scholar] [CrossRef]
- Tracey, E.R.; Katie, E.C.; Jared, A.L. The aging process and cognitive abilities. In The Oxford Handbook of Work and Aging; Oxford University Press: Oxford, UK, 2012; pp. 236–255. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Variable | Definition |
|---|---|
| WORK | The total score of 4 questions in the HRS measuring perceived work ability. Each question was scored from 0 to 10 with respect to a job’s separate general, physical, mental, and interpersonal demands. High scores indicate high work ability. |
| STRESS | The natural logarithm of the total score for 8 ongoing chronic stressors in the HRS survey. The score ranges from 1 to 4 for each question, and illustrates various stresses with respect to ongoing health issues of the respondent, physical or emotional problems in spouses or children, problems with alcohol or drug use in a family member, difficulties at work, financial strain, housing problems, relationship problems, and helping sick, limited, or frail family members or friends. High scores indicate high stress. |
| SOCIAL | Social status, as perceived by the individual. High scores indicate high self-perceived social status. |
| HEALTH | Health status of an individual in the survey year. The original score ranges from 1 to 5, with lower values indicating better health status. We subtracted the original values from 5, to make them more readable in the regression results. Higher scores thus indicate better health status. |
| GENDER | An indicator variable of the gender of an individual. Originally, 1 represented male and 2 represented female. We replaced the value of 2 with 0. Thus, 1 indicates male; other values indicate female. |
| AGE | The natural logarithm of the age of an individual. |
| WORKLOAD | An indicator variable that controls for differences in the workload of an individual. The classification process is as follows; if the original work hours per week is lower than 10, the value is 1; if 10 ≤ work hours ≤ 20, the value is 2; if 20 < work hours ≤ 30, the value is 3; if 30 < work hours ≤ 40, the value is 4; if work hours > 40, the value is 5. |
| EXPERIENCE | The natural logarithm of the respondent’s years of service in a job. Years of service was calculated as the natural logarithm of the difference between the year the respondent started the current job and the survey year. |
| EDUCATION | The total number of years of education an individual has received. |
| Variable * | N (%) | Mean | SD | Min | 25% | 75% | Max |
|---|---|---|---|---|---|---|---|
| GENDER | |||||||
| Women | 5880(83.0) | ||||||
| Men | 1203(17.0) | ||||||
| WORKLOAD | |||||||
| <10 h/week | 268(3.8) | ||||||
| 10–20 h/week | 490(6.9) | ||||||
| 20–30 h/week | 860(12.1) | ||||||
| 30–40 h/week | 3728(52.6) | ||||||
| >40 h/week | 1737(24.5) | ||||||
| WORK | 34.57 | 5.29 | 0.00 | 32.00 | 39.00 | 40.00 | |
| STRESS | 12.54 | 3.85 | 8.00 | 10.00 | 15.00 | 32.00 | |
| SOCIAL | 6.46 | 1.59 | 1.00 | 5.00 | 8.00 | 10.00 | |
| HEALTH | 2.51 | 0.95 | 0.00 | 2.00 | 3.00 | 4.00 | |
| AGE | 60.69 | 7.36 | 50.00 | 55.00 | 65.00 | 99.00 | |
| EXPERIENCE | 20.21 | 14.47 | 0.00 | 7.00 | 32.00 | 83.00 | |
| EDUYEARS | 13.65 | 2.76 | 0.00 | 12.00 | 16.00 | 17.00 |
| Variable | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 |
|---|---|---|---|---|---|---|---|---|---|
| 1. WORK | 1 | −0.288 ** | 0.248 *** | 0.343 *** | −0.051 *** | −0.102 *** | 0.133 *** | 0.020 * | 0.152 *** |
| 2. STRESS | −0.257 *** | 1 | −0.296 *** | −0.304 *** | −0.071 *** | −0.105 *** | 0.015 | −0.076 *** | −0.040 *** |
| 3. SOCIAL | 0.224 *** | −0.281 *** | 1 | 0.278 *** | 0.059 *** | 0.124 *** | 0.056 *** | 0.140 *** | 0.267 *** |
| 4. HEALTH | 0.320 *** | −0.300 *** | 0.269 *** | 1 | −0.013 | −0.027 ** | 0.062 *** | 0.032 *** | 0.275 *** |
| 5. GENDER | −0.076 *** | −0.066 *** | 0.062 *** | −0.012 | 1 | 0.208 *** | 0.031 *** | 0.105 *** | 0.013 |
| 6. AGE | 0.106 *** | −0.093 *** | 0.117 *** | −0.018 | −0.172 *** | 1 | −0.330 *** | 0.210 *** | −0.005 |
| 7. WORKLOAD | 0.119 *** | 0.013 | 0.079 *** | 0.072 *** | 0.035 *** | −0.281 *** | 1 | 0.084 *** | 0.063 *** |
| 8. EXPERIENCE | 0.009 | −0.066 *** | 0.130 *** | 0.040 *** | 0.088 *** | 0.150 *** | 0.114 *** | 1 | 0.045 *** |
| 9. EDUCATION | 0.129 *** | −0.038 *** | 0.301 *** | 0.256 *** | 0.019 | 0.000 | 0.095 *** | 0.057 *** | 1 |
| Variables | Pred. Sign | WORK | WORK | WORK | HEALTH |
|---|---|---|---|---|---|
| Coefficient (t Value) | Coefficient (t Value) | Coefficient (t Value) | Coefficient (t Value) | ||
| Intercept | +/− | 38.88 (14.78) *** | 50.83 (20.01) *** | 56.85 (21.88) *** | 4.75 (10.77) *** |
| STRESS | - | −3.42 (−14.53) *** | −4.53 (−19.05) *** | −0.88 (−22.17) *** | |
| SOCIAL | + | 0.42 (9.7) *** | 0.54 (11.86) *** | 0.088 (11.59) *** | |
| HEALTH | + | 1.27 (17.7) *** | |||
| GENDER | +/− | −0.80 (−4.78) *** | −0.87 (−5.64) *** | −0.98 (−6.23) *** | −0.09 (−3.19) *** |
| AGE | − | −2.50 (−4.03) *** | −3.97 (−6.91) *** | −4.51 (−7.64) *** | −0.43 (−4.26) *** |
| WORKLOAD | + | 0.55 (7.61) *** | 0.45 (6.87) *** | 0.48 (7.15) *** | 0.03 (2.4) ** |
| EXPERIENCE | + | 0.16 (2.43) ** | 0.02 (0.34) | 0.01 (0.23) | −0.01 (−0.49) |
| EDUCATION | + | 0.28 (11.49) *** | 0.08 (3.5) *** | 0.18 (7.73) *** | 0.08 (19.45) *** |
| YEAR EFFECTS | YES | YES | YES | YES | |
| N | 7083 | 7083 | 7083 | 7083 | |
| F Statistic | 50.22 *** | 170.31 *** | 140.47 *** | 182.82 *** | |
| Adj. R Square | 0.046 | 0.193 | 0.151 | 0.188 |
| Effect | Coefficient Value |
|---|---|
| Total Effect () | −4.53 |
| Direct Effect () | −3.42 |
| Indirect Effect () | −1.11 |
| Percent of total effect that is mediated | 24.50% |
| Variables | Pred. Sign | Low | Moderate | High |
|---|---|---|---|---|
| Coefficient (t Value) | Coefficient (t Value) | Coefficient (t Value) | ||
| Intercept | +/− | 49.38 (2.72) *** | 53.05 (16.5) *** | 52.14 (12.74) *** |
| STRESS | - | −6.11 (−4.31) *** | −3.72 (−13.34) *** | −2.90 (−6.79) *** |
| HEALTH | + | 2.47 (6.16) *** | 1.34 (15.1) *** | 0.96 (8.47) *** |
| GENDER | +/− | −1.19 (−1.05) | −0.89 (−4.37) *** | −0.87 (−3.75) |
| AGE | - | −1.87 (−0.45) | −3.93 (−5.4) *** | −3.48 (−3.81) *** |
| WORKLOAD | + | 0.50 (1.16) | 0.50 (5.93) *** | 0.41 (4.04) *** |
| EXPERIENCE | + | −0.05 (−0.15) | 0.06 (0.81) | −0.01 (−0.13) |
| EDUCATION | + | 0.08 (0.54) | 0.12 (4.13) *** | 0.08 (1.91) * |
| YEAR EFFECTS | YES | YES | YES | |
| N | 296 | 4768 | 2019 | |
| F Statistic | 10.29 *** | 98.83 *** | 36.44 *** | |
| Adj. R Square | 0.2208 | 0.1559 | 0.1365 |
| Effect | Low | Moderate | High |
|---|---|---|---|
| Coefficient Value | Coefficient Value | Coefficient Value | |
| Total Effect () | −8.73 | −4.95 | −3.79 |
| Direct Effect () | −6.11 | −3.72 | −2.90 |
| Indirect Effect () | −2.62 | −1.23 | −0.89 |
| Percent of total effect that is mediated | 30.01% | 24.85% | 23.50% |
| Variables | Pred. Sign | WORK | HEALTH |
|---|---|---|---|
| Coefficient (t Value) | Coefficient (t Value) | ||
| Intercept | +/− | 20.75 (3.10) *** | 2.24 (1.97) ** |
| LAGWORK | 0.49 (11.04) *** | ||
| LAGSTRESS | - | −0.12 (−3.06) *** | −0.07 (−10.59) *** |
| LAGSOCIAL | + | −0.02 (−0.22) | 0.07 (4.22) *** |
| LAGHEALTH | + | 0.53 (3.60) *** | |
| GENDER | +/− | −0.75 (−1.78) * | −0.15 (−1.86) * |
| AGE | - | −1.34 (−0.90) | −0.07 (−0.29) |
| WORKLOAD | + | 0.16 (1.25) | 0.04 (1.48) |
| EXPERIENCE | + | 0.13 (0.94) | 0.00 (0.16) |
| EDUCATION | + | 0.07 (1.46) | 0.07 (7.92) *** |
| YEAR EFFECTS | YES | YES | |
| N | 1462 | 1462 | |
| F Statistic | 60.05 *** | 44.77 *** | |
| Adj. R Square | 0.271 | 0.173 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, T.; Liu, T.; Lei, R.; Deng, J.; Xu, G. Effect of Stress on the Work Ability of Aging American Workers: Mediating Effects of Health. Int. J. Environ. Res. Public Health 2019, 16, 2273. https://doi.org/10.3390/ijerph16132273
Yang T, Liu T, Lei R, Deng J, Xu G. Effect of Stress on the Work Ability of Aging American Workers: Mediating Effects of Health. International Journal of Environmental Research and Public Health. 2019; 16(13):2273. https://doi.org/10.3390/ijerph16132273
Chicago/Turabian StyleYang, Tianan, Taoming Liu, Run Lei, Jianwei Deng, and Guoquan Xu. 2019. "Effect of Stress on the Work Ability of Aging American Workers: Mediating Effects of Health" International Journal of Environmental Research and Public Health 16, no. 13: 2273. https://doi.org/10.3390/ijerph16132273